

The authors review the timelines, and probabilities, of recent vaccines progressing from phase 2 clinical trials to licensure within 10 years.
Visual Abstract. Probability of Success and Timelines of Vaccines for Viral Infectious Diseases.
The authors review the timelines, and probabilities, of recent vaccines progressing from phase 2 clinical trials to licensure within 10 years.
Abstract
Background:
Anticipated success rates and timelines for COVID-19 vaccine development vary. Recent experience with developing and testing viral vaccine candidates can inform expectations regarding the development of safe and effective vaccines.
Objective:
To estimate timelines and probabilities of success for recent vaccine candidates.
Design:
ClinicalTrials.gov was searched to identify trials testing viral vaccines that had not advanced to phase 2 before 2005, and the progress of each vaccine from phase 1 through to U.S. Food and Drug Administration (FDA) licensure was tracked. Trial characteristics were double-coded. (Registration: Open Science Framework [https://osf.io/dmuzx/]).
Setting:
Trials launched between January 2005 and March 2020.
Participants:
Preventive viral vaccine candidates for 23 emerging or reemerged viral infectious diseases.
Measurements:
The primary end point was the probability of vaccines advancing from launch of phase 2 to FDA licensure within 10 years.
Results:
In total, 606 clinical trials forming 220 distinct development trajectories (267 343 enrolled participants) were identified. The probability of vaccines progressing from phase 2 to licensure within 10 years was 10.0% (95% CI, 2.6% to 16.9%), with most approvals representing H1N1 or H5N1 vaccines. The average timeline from phase 2 to approval was 4.4 years (range, 6.4 weeks to 13.9 years). The probabilities of advancing from phase 1 to 2, phase 2 to 3, and phase 3 to licensure within the total available follow-up time were 38.2% (CI, 30.7% to 45.0%), 38.3% (CI, 23.1% to 50.5%), and 61.1% (CI, 3.7% to 84.3%), respectively.
Limitations:
The study did not account for preclinical development and relied primarily on ClinicalTrials.gov and FDA resources. Success probabilities do not capture the varied reasons why vaccines fail to advance to regulatory approval.
Conclusion:
Success probabilities and timelines varied widely across different vaccine types and diseases. If a SARS-CoV-2 vaccine is licensed within 18 months of the start of the pandemic, it will mark an unprecedented achievement for noninfluenza viral vaccine development.
Primary Funding Source:
McGill Interdisciplinary Initiative in Infection and Immunity (MI4) Emergency COVID-19 Research Funding program.
Development of a safe and effective vaccine for the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is widely regarded as a crucial public and global health goal. As of 7 October 2020, at least 48 vaccine development efforts have launched trials across 6 continents, with 30 candidates having advanced to phase 2 or phase 3 testing (1). It remains unclear how many of these candidates will withstand rigorous evaluation in field trials and when effective vaccines will be ready for deployment.
At the outset of the coronavirus disease 2019 (COVID-19) pandemic, numerous public health authorities and political leaders projected that a SARS-CoV-2 vaccine could be delivered within 12 to 18 months of laboratory testing (2, 3). However, projections of vaccine timelines as well as certainty of success have varied widely. Whereas some commentators anticipate that a vaccine can be easily developed within 1 year owing to immunologic characteristics of the virus, others are less sanguine (4). Moreover, vaccine development for viral diseases has occasionally encountered unexpected setbacks, including vaccine-dependent enhancement (5–7), which some commentators have suggested may play a role in the development of a SARS-CoV-2 vaccine (8, 9).
Although the current pandemic is unprecedented both in terms of the biological properties of SARS-CoV-2 and the strong political will and financial support being funneled into vaccine development, looking at recent vaccine development efforts may elucidate some of the factors that could affect the pace of SARS-CoV-2 vaccine development. Previous studies have used proprietary databases to estimate that 2% to 39% of vaccine candidates introduced into phase 1 trials progress to regulatory licensure (10–16). However, such studies primarily evaluated trials that predate 2009; since then, new techniques, such as next-generation sequencing and atomic-level structural biology approaches, have emerged that may speed the pace of viral vaccine development (17, 18). Many such studies have included seasonal influenza vaccines or nonviral vaccines, the development of which may differ from that anticipated for COVID-19. In this study, we estimate timelines and probabilities of success (POSs) for a recent cohort of viral vaccine candidates.
Methods
We performed a retrospective cohort study of vaccines for emerging and reemerged viral infectious diseases (EVIDs). Our primary objective was to determine the POS of vaccine development efforts, defined as the probability of a vaccine candidate advancing from the start of phase 2 to U.S. Food and Drug Administration (FDA) approval within 10 years. The start of each phase was defined as the date of first enrollment of the first trial as listed on ClinicalTrials.gov.
Our sample was created in 3 steps. First, we established a list of EVIDs. Second, we identified all prelicensure vaccine trials for each EVID registered on ClinicalTrials.gov from 1 January 2005 to 22 March 2020. Third, we organized vaccine trials into “trajectories,” defined as the collection of trials testing a given vaccine candidate or regimen for a specific EVID; an example of this is shown in Appendix Figure 1 (available at Annals.org). Using FDA approval documents, we categorized trajectories as “successful” if the vaccine candidate received FDA approval at any time after 2005. We calculated the POS by using time-to-event analysis methods to account for censored data and estimated the time required to progress from early-phase testing to approval.
Appendix Figure 1. Vaccine trajectories for Dengvaxia and Ervebo.

Each line represents a trial and spans the duration from trial start to primary completion date. Completed phase 1/2 and phase 2/3 trials are indicated by using both colors, with the first phase spanning a third of the total trial duration and the second phase spanning the remainder of the trial duration. The vertical black line indicates the U.S. Food and Drug Administration approval date.
Data Sources
We established a list of EVIDs by using the World Health Organization (WHO) list of epidemic and pandemic diseases (19), supplemented with EVIDs from a recent review (18). We excluded seasonal influenza because such vaccines rely on well-established platforms (20) but included pandemic (H1N1 and avian flu) and universal flu vaccine development efforts. Universal influenza vaccines often use innovative approaches with some similarities to COVID-19 vaccine development efforts (21).
To identify vaccine development trajectories for our EVIDs of interest, we searched ClinicalTrials.gov for all prelicensure clinical trials of any phase from 2005 to present by using PubMed Medical Subject Heading synonyms for each EVID and vaccine keywords; detailed search methods are provided in the Supplement (available at Annals.org). We focused on 2005 onward because new vaccine development approaches emerged in this period (17). Trials were double-screened according to the following inclusion criteria: 1) phase 1, 2, or 3 trial; 2) preventive vaccine targeting an EVID of interest; 3) prelicensure trial based on trial enrollment start date; 4) testing safety, immunogenicity, or protection; and 5) monovalent vaccine candidate, for nonuniversal influenza vaccines. We excluded trials that exclusively enrolled subpopulations with comorbid conditions (such as individuals with HIV), enrolled persons who had previously participated in a trial of the same vaccine, had a pre-2005 phase 2 or 3 trial of the same vaccine candidate, or were withdrawn before recruiting any participants (Figure 1). The Supplement provides further details.
Figure 1. Study flow diagram.
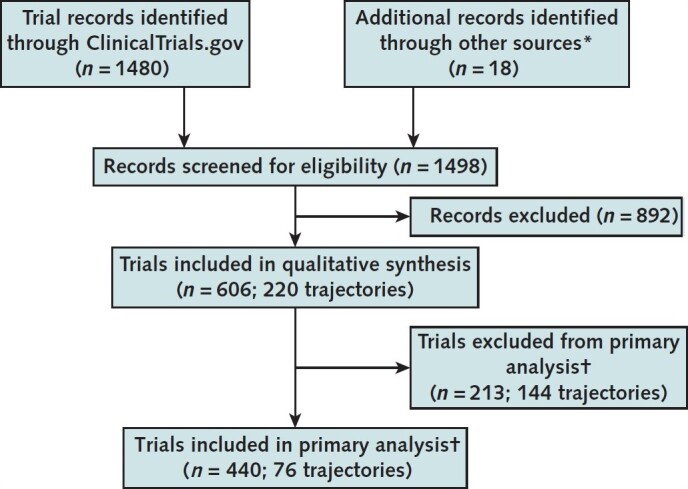
* PubMed, World Health Organization, and U.S. Food and Drug Administration resources; these were only searched to supplement the trajectories of approved vaccine candidates or vaccines with incomplete trajectories based on ClinicalTrials.gov.
† Trajectories (and the trials they contained) were excluded from the primary analysis if they did not advance beyond phase 1. Some trials tested multiple vaccine candidates and were thus included in multiple trajectories, so the sum of the trials included in and excluded from the primary analysis exceeds the total number of trials included in the quantitative synthesis.
Trials were assigned to trajectories by 2 independent coders on the basis of vaccine name, type, and sponsor, and any discrepancies were adjudicated to produce the final data set. Where multiple vaccines were tested in combination, we combined vaccines into a single trajectory based on the trial that was furthest along in development (Supplement). Once trajectories had been established, we further searched PubMed, WHO, and FDA resources to supplement our trial sample; the Supplement shows detailed search methods.
Data Extraction
Data available on ClinicalTrials.gov, including trial recruitment status, phase, enrollment, trial start and primary completion dates, were downloaded automatically. These data were manually double-extracted for trials identified through PubMed, WHO, and FDA resources (Supplement). Data not available on ClinicalTrials.gov, including vaccine type, FDA approval status, and sponsor type, were independently double-coded.
Vaccine type, approval status, and sponsor type were coded at the trajectory level. Vaccines were classified as whole-pathogen, subunit, or nucleic acid vaccines on the basis of the National Institute of Allergy and Infectious Diseases categorization (22). Split virus vaccines in influenza were classified separately (23), and trajectories that combined multiple vaccine candidates of different types were labelled as “multiple.” When trial records provided insufficient information to determine the trajectory or vaccine type, we consulted pipeline reviews and press releases to resolve uncertainties. The FDA approval status was determined on the basis of the date of first approval for each vaccine. Trajectory sponsorship was based on trial records for the earliest 2 trials per trajectory; the Supplement provides details on sponsor classification.
Data Synthesis
The primary outcome was the POS from launch of phase 2 within 10 years. We anchored our primary outcome at phase 2 rather than phase 1 because sponsors are not legally required to register phase 1 trials on ClinicalTrials.gov (24) and publication bias would make it almost impossible to reliably identify all vaccine candidates that produced negative results in phase 1 trials (25). Trajectories that did not advance beyond phase 1 were not included in the primary analysis. The follow-up time of 10 years from the enrollment start date was selected because it is in line with prior estimates of vaccine development time (15, 16).
To evaluate the POS, we used time-to-event analysis, which accounts for the fact that newer vaccine development efforts have less follow-up time than older ones. We report the Kaplan–Meier estimate at 10 years, along with 95% CIs based on the log-transformation of survival.
As a secondary outcome, we looked at the probabilities of phase transition events from the enrollment start date of each phase to the enrollment start date of the subsequent phase. The probabilities of transitioning from one phase to the next were calculated for phase 1 to phase 2, phase 2 to phase 3, phase 3 to approval by using the time-to-event analysis method described above (Supplement). We report the transition probabilities at the total available follow-up time of 15.5 years, 15.0 years, and 14.1 years from phase 1, phase 2, and phase 3, respectively. We also looked at the POS from initiation of phase 1 within 12 years to include more of our data set; this can be interpreted as an upper limit on the POS from phase 1, given that our search may not have captured all vaccine candidates that did not advance past phase 1.
As a sensitivity analysis to account for the fact that vaccine candidates may fail to advance to regulatory approval owing to an outbreak quelling (which would impede trial accrual and lower vaccine demand), we reanalyzed our primary outcome of POS from phase 2 to approval, including only those vaccine candidates for which termination of trial activity did not coincide with outbreak quelling. We defined a quelling as a 12-month period without active cases listed in the WHO Outbreak Archive, with the exception of endemic diseases, including HIV, hepatitis C, and universal influenza, and excluded vaccines from the sensitivity analysis if a quelling followed the primary completion date of the last active trial in the trajectory. In addition, we report the total proportion of “unsuccessful” vaccines whose terminations coincided with a quelling and the proportion of trajectories that persisted despite a quelling.
We assessed whether there were differences in trajectory success probabilities stratified by vaccine type and indication (influenza versus noninfluenza). All analyses were descriptive. Analyses were performed with R, version 3.5.0, and time-to-event analyses were performed by using the survival package on 22 June 2020 (26). Outcomes were prespecified before extraction, and the study was prospectively registered on Open Science Framework (https://osf.io/dmuzx/); the Supplement provides an explanation of differences from the registration record. The full data set and statistical code is available on Open Science Framework (https://osf.io/ed6ar/).
Role of the Funding Source
The study was funded by the McGill Interdisciplinary Initiative in Infection and Immunity (MI4) Emergency COVID-19 Research Funding program. The funding source had no role in the design or execution of this study or in the decision to submit the manuscript for publication.
Results
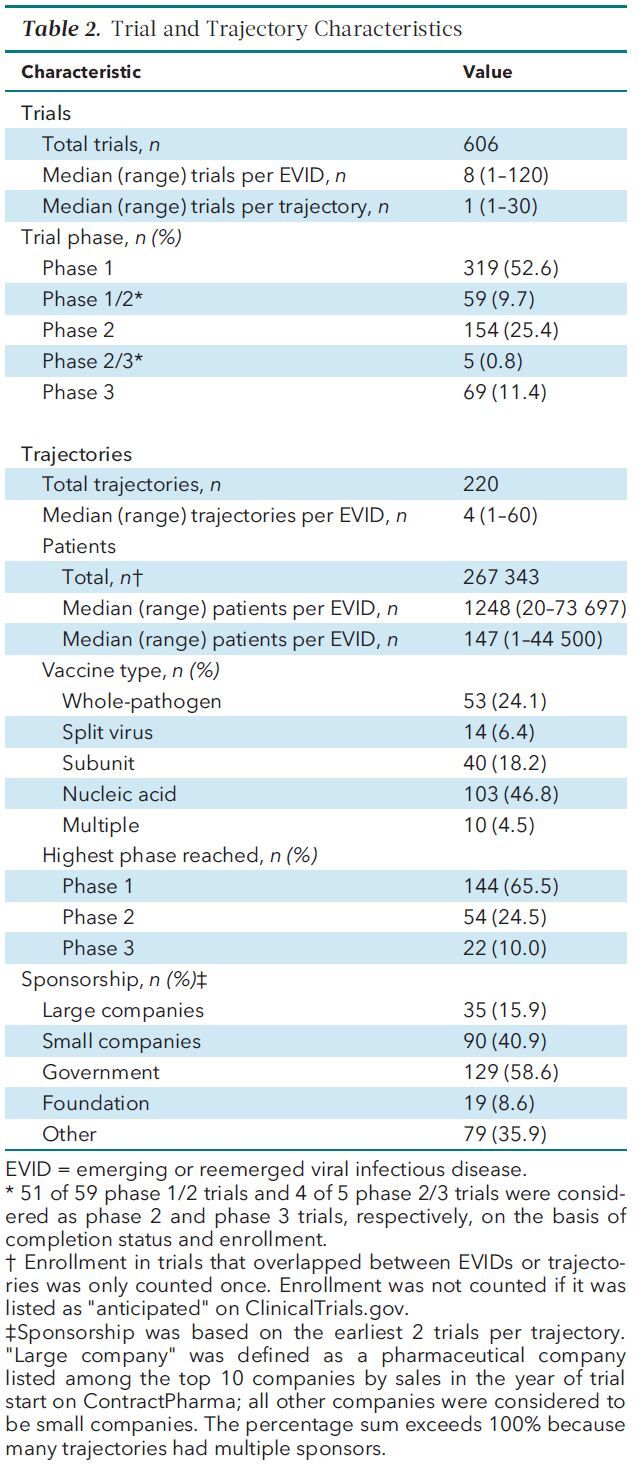
Of the 27 EVIDs included in our initial search, we identified at least 1 eligible trial on ClinicalTrials.gov for 23 (Table 1). Our trial search captured 606 eligible trials forming 220 trajectories and enrolling 267 343 volunteers (Table 2). Of the 220 vaccine trajectories, 9 advanced to FDA approval, 7 of which were approved within 10 years of phase 2 start, and 76 advanced beyond phase 1 and were included in the primary analysis.
Table 1. Characteristics of EVIDs Included in the Study*.

Table 2. Trial and Trajectory Characteristics.
The timeline from the launch of the first phase 2 trial to FDA approval ranged from 6.4 weeks (Influenza A [H1N1] 2009 Monovalent Vaccine [Sanofi Pasteur, Inc.] and Influenza A [H1N1] 2009 Monovalent Vaccine [Novartis Vaccines and Diagnostics Ltd.]) to 13.9 years (Audenz Influenza A [H5N1] Monovalent Vaccine, Adjuvanted [Seqirus Inc.]), with an average of 4.4 years (Table 3).
Table 3. Characteristics of Approved Vaccines.

Vaccine Development POS
The POS from phase 2 launch was 10.0% (95% CI, 2.6% to 16.9%) within 10 years (Figure 2). The 7 vaccines that received approval within 10 years were Ervebo (Ebola Zaire Vaccine, Live [Merck Sharp & Dohme Corp.]) and 6 pandemic influenza vaccines. Dengvaxia (Dengue Tetravalent Vaccine, Live [Sanofi Pasteur Inc.]) and Audenz were approved 12.7 and 13.9 years from initiation of phase 2, respectively. The POS from phase 1 was 7.1% (CI, 1.3% to 12.5%) within 12 years.
Figure 2. Kaplan–Meier curve for probability of FDA approval from the time of launch of the phase 2 trial.
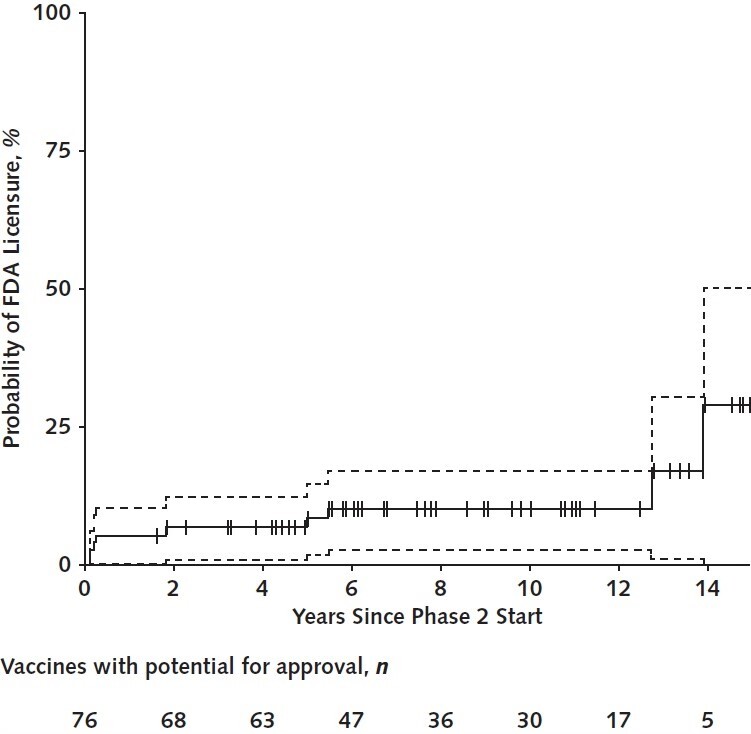
Vertical tick marks indicate censored vaccine trajectories. Dotted lines indicate 95% CIs. FDA = U.S. Food and Drug Administration.
Phase Transition Probabilities
The probabilities that development trajectories would advance from phase 1 to 2, phase 2 to 3, and phase 3 to approval within the total follow-up time were 38.2% (CI, 30.7% to 45.0%), 38.3% (CI, 23.1% to 50.5%), and 61.1% (CI, 3.7% to 84.3%), respectively (Appendix Table 1, available at Annals.org). Appendix Figure 2 (available at Annals.org) shows Kaplan–Meier curves.
Appendix Table 1. Phase Transition Probabilities.

Appendix Figure 2. Kaplan–Meier curves for the probability of transitioning from phase 1 to 2 ( A ), phase 2 to phase 3 ( B ), and phase 3 to FDA licensure ( C ) over time from trial launch.

Vertical tick marks indicate censored vaccine trajectories. Dotted lines indicate 95% CIs. FDA = U.S. Food and Drug Administration.
Variation in POS by Indication and Vaccine Type
Excluding pandemic influenza trajectories, which largely build on an established vaccine development platform, the POS from phase 2 to approval was 3.2% (CI, 0.0% to 9.2%) within 10 years. Of all vaccine types, the only categories that had an FDA approval within 10 years were split virus and nucleic acid vaccines, with 56.4% (CI, 12.6% to 78.2%) of split virus vaccines and 5.9% (CI, 0.0% to 16.4%) of nucleic acid vaccines progressing from phase 2 to FDA licensure within 10 years (Appendix Table 2, available at Annals.org).
Appendix Table 2. POS, by Vaccine Type, Sponsor Type, and Indication.

Sensitivity Analyses
Of the 211 trajectories that did not advance to FDA approval and of the 67 of these included in our primary analysis, 23.2% (49 of 211) and 29.9% (20 of 67), respectively, terminated during a quelling of WHO-reported outbreak activity. After excluding these 20 trajectories, the POS from phase 2 was 13.5% (CI, 3.6% to 22.5%) overall and 5.0% (CI, 0.0% to 14.1%) for noninfluenza vaccines. Vaccine development efforts often persevered in spite of outbreak quelling. There were 77 vaccine development trajectories with at least 1 quelling of disease activity from trajectory start to within 1 year after trajectory end. Of these, 54 (70.1%) continued with further development through at least 1 quelling, 3 of which were approved (Dengvaxia, Ervebo, and Audenz).
Discussion
To our knowledge, this analysis provides the first estimate of preventive EVID vaccine development success rates from phase 2 to licensure by using publicly available data (27, 28). Our findings suggest that approximately 1 in 10 EVID vaccines that reached phase 2 since 2005 advanced to FDA licensure within 10 years, whereas 1 in 30 advanced when influenza vaccines were excluded. Of the 23 EVIDs in our sample, 4 diseases had at least 1 vaccine candidate that obtained an approval (dengue, Ebola, H1N1, and H5N1). However, FDA approval is an imperfect proxy for successful vaccine development and may not equate with public health impact. For instance, Dengvaxia is only 61% efficacious in endemic settings and is associated with enhanced disease (6, 29). In addition, the effect of an approval may be limited by the quelling of the initial epidemic, as in the 2014–2016 Ebola epidemic in West Africa (30).
Our results also highlight wide variation in timelines, development activities, and success rates in vaccine development across different EVIDs (Figure 3). H1N1 and H5N1 influenza vaccines accounted for most approved vaccines in our sample and also had the shortest clinical development times (with the exception of Audenz, which took 13.9 years). However, the rapid development of H1N1 and H5N1 vaccines is probably attributable to existing seasonal influenza research and platforms (20). Vaccine development efforts for SARS-CoV-2 are building on a much more limited base of research and vaccine candidates, including those developed using less well-established platforms. In addition, increased trial or trajectory volume was not necessarily associated with successful licensure. Vaccines designed to prevent HIV accounted for 20% of trials and almost 30% of trajectories but had only 1 vaccine regimen that reached phase 3 since 2005 and no approvals. In our sample, the most rapid successful noninfluenza vaccine development timeline was for the Ebola recombinant vector vaccine, Ervebo (5.0 years overall from phase 2 to approval), which also is the only approval of a nucleic acid vaccine to date.
Figure 3. Vaccine trajectories for EVIDs.

Each horizontal bar represents a single trajectory composed of 1 or more trials, beginning at the start date of the earliest trial of any phase since 2005 and ending at the primary completion date of the latest trial or the date of U.S. Food and Drug Administration (FDA) approval. If the latest primary completion date was marked as “anticipated” on ClinicalTrials.gov or the trial status was not marked as “completed,” “active, not recruiting,” or “terminated,” the confirmed trajectory duration is indicated by a solid bar, and the interval between the latest confirmed date and the latest possible date is indicated by a segmented bar. Lines are censored at 2021 for trials with anticipated completion dates later than 2021. Only EVIDs with more than 5 trajectories are shown. Trajectories are ordered by start date within each EVID. Open diamonds indicate vaccine candidates that received FDA approval; X's indicate the latest confirmed primary completion date for a trajectory that coincides with a quelling in World Health Organization–reported outbreak activity. Question marks indicate trajectories for which the end date could not be confirmed. Gray shading indicates periods of 1 year or more between 2005 and 2020 where there was no World Health Organization–reported outbreak activity in the preceding year. EVID = emerging and reemerged viral infectious disease.
If COVID-19 vaccine development were to follow historic timelines, progress would be insufficient, given the urgency of controlling the pandemic (31). Our results should be viewed as a systematic assessment of historically observed success rates and timelines of viral vaccine development rather than necessarily foreshadowing the outcome of COVID-19 efforts. Nevertheless, our findings point to challenges that SARS-CoV-2 vaccine development will need to overcome and highlight the need for new paradigms that can facilitate the development of vaccines “at pandemic speed” (31).
As of 7 October 2020, at least 48 SARS-CoV-2 vaccine candidates had entered clinical testing, 19 of which are in phase 2 clinical trials and 11 of which are in phase 3 (1). Current SARS-CoV-2 vaccine development efforts differ from those for the EVIDs in our study in several ways. First, many outbreaks of EVIDs in our sample, such as SARS, ended before vaccines were developed, which is less likely to be the case for COVID-19. On the other hand, for some EVIDs in our sample (such as HIV and universal influenza), disease activity and public interest remained high throughout the study period. In addition, our sensitivity analysis indicated that the overall success probability does not change substantially after vaccines for which trajectory discontinuation coincided with a quelling in WHO-reported outbreak activity are excluded. Second, many SARS-CoV-2 vaccine candidates have condensed or truncated the usual basic science research and preclinical steps and are conducting traditionally distinct clinical trial phases in parallel. This could accelerate timelines, though careful attention will be needed to ensure that sufficient evidence is generated for advancement of candidates to further testing and licensure. Third, the global collaboration facilitated by private–public partnerships and organizations, such as the Coalition for Epidemic Preparedness Innovations, to expedite development timelines is unprecedented (32, 33). Finally, with almost 50 COVID-19 vaccine candidates in the clinical pipeline, the volume of candidates is already similar to the volume of experimental vaccine platforms that HIV vaccine efforts produced over the past 15 years.
The above dynamics nevertheless contend with uncertainty regarding the biology of SARS-CoV-2. SARS-CoV-2 is the world's third encounter with a novel coronavirus that has pandemic potential. Although research on SARS-CoV and MERS-CoV provided a springboard for SARS-CoV-2 (34, 35), no coronavirus vaccines have yet been evaluated in large field studies, and the possibility of vaccine-dependent enhancement or other adverse safety events provide grounds for caution (8, 9). In addition, some companies are pursuing novel approaches, such as recombinant vectors and proteins and mRNA and DNA vaccines (31, 36). No mRNA or DNA vaccines have previously been licensed. However, many other SARS-CoV-2 vaccine candidates are being developed by using previously successful technologies, such as inactivated vaccines. Our findings underscore the importance of pursuing both conventional and novel platforms to maximize chances of success, especially given that for sufficient doses to be available to vaccinate various at-risk populations, multiple vaccines are likely to be needed worldwide.
Our study has limitations. First, we did not account for time invested in preclinical development or manufacturing and distribution, which represent substantial portions of the development timeline for new vaccines (3). Second, we relied primarily on ClinicalTrials.gov and FDA resources to create our trial sample and identify approvals. We may be missing phase 1 trials, which are not required to be registered on ClinicalTrials.gov (24); for this reason, we anchored our primary outcome at phase 2. Also, our analysis only captured approvals by the FDA. At least 4 non-U.S. approvals of vaccines in our data set were not captured in our analysis (2 enterovirus 71 approvals in China and 1 H1N1 influenza approval each in South Korea and India) (37, 38), in addition to H5N1 influenza vaccines licensed by the European Medicines Agency (39). Third, our estimates were heavily influenced by influenza and HIV vaccine development efforts. Finally, our analysis did not enable assessment of whether trajectories failed owing to safety, efficacy, decline in disease activity, or commercial reasons. Disentangling explanations for vaccine development failure is likely to be challenging given the many contributing factors. For example, low efficacy may render safety concerns more salient. In addition, while we looked at quelling of disease activity as a possible explanation for trajectory discontinuation, this is only one of many possible causes, and we are not aware of any systematic attempts to assess reasons for vaccine development failure. Future studies are needed to elucidate the factors contributing to the failure of vaccine candidates, as well as to probe the concordance between the outcomes of early and late phase trials.
Low success rates and long timelines for recent viral vaccine development underscore the extensive challenges of developing a safe and effective SARS-CoV-2 vaccine within 18 months of its emergence. Nevertheless, new collaborative paradigms of vaccine development and an unprecedented number and diversity of development efforts offer some prospect that such challenges may be overcome. Although it is difficult to predict which platforms or strategies will prove most efficient from a timeline perspective, maintaining active research programs on various emerging infectious diseases and developing platforms that can be easily mobilized for emerging threats are likely to be critical to reducing vaccine development timelines in the future.
Supplementary Material
Footnotes
This article was published at Annals.org on 24 November 2020
References
- 1. McGill COVID19 Vaccine Tracker Team. COVID19 vaccine tracker. October 2020. Accessed at http://covid19.trackvaccines.org on 14 October 2020.
- 2. Cohen J. Unveiling ‘Warp Speed,’ the White House's America-first push for a coronavirus vaccine. Science. 12 May 2020. Accessed at www.sciencemag.org/news/2020/05/unveiling-warp-speed-white-house-s-america-first-push-coronavirus-vaccine on 13 May 2020.
- 3. Thompson SA. How long will a vaccine really take? New York Times. 30 April 2020. Accessed at www.nytimes.com/interactive/2020/04/30/opinion/coronavirus-covid-vaccine.html on 30 April 2020.
- 4. Kane PB , Moyer H , MacPherson A , et al. Expert forecasts of COVID-19 vaccine development timelines [Letter]. J Gen Intern Med. 2020. [PMID: ] doi: 10.1007/s11606-020-06244-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Sekaly RP . The failed HIV Merck vaccine study: a step back or a launching point for future vaccine development. J Exp Med. 2008;205:7-12. [PMID: ] doi: 10.1084/jem.20072681 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Halstead SB . Dengvaxia sensitizes seronegatives to vaccine enhanced disease regardless of age. Vaccine. 2017;35:6355-6358. [PMID: ] doi: 10.1016/j.vaccine.2017.09.089 [DOI] [PubMed] [Google Scholar]
- 7. Acosta PL , Caballero MT , Polack FP . Brief history and characterization of enhanced respiratory syncytial virus disease. Clin Vaccine Immunol. 2015;23:189-95. [PMID: ] doi: 10.1128/CVI.00609-15 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Iwasaki A , Yang Y . The potential danger of suboptimal antibody responses in COVID-19. Nat Rev Immunol. 2020;20:339-341. [PMID: ] doi: 10.1038/s41577-020-0321-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Lambert PH , Ambrosino DM , Andersen SR , et al. Consensus summary report for CEPI/BC March 12-13, 2020 meeting: assessment of risk of disease enhancement with COVID-19 vaccines. Vaccine. 2020;38:4783-4791. [PMID: ] doi: 10.1016/j.vaccine.2020.05.064 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Wong CH , Siah KW , Lo AW . Estimation of clinical trial success rates and related parameters. Biostatistics. 2019;20:273-286. [PMID: ] doi: 10.1093/biostatistics/kxx069 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Hay M , Thomas DW , Craighead JL , et al. Clinical development success rates for investigational drugs. Nat Biotechnol. 2014;32:40-51. [PMID: ] doi: 10.1038/nbt.2786 [DOI] [PubMed] [Google Scholar]
- 12. Thomas D, Burns J, Audette J, et al. Clinical development success rates 2006-2015. BIO, BioMedTracker, and Amplion. June 2016. Accessed at www.bio.org/sites/default/files/legacy/bioorg/docs/Clinical%20Development%20Success%20Rates%202006-2015%20-%20BIO,%20Biomedtracker,%20Amplion%202016.pdf on 17 June 2020.
- 13. Davis MM , Butchart AT , Wheeler JR , et al. Failure-to-success ratios, transition probabilities and phase lengths for prophylactic vaccines versus other pharmaceuticals in the development pipeline. Vaccine. 2011;29:9414-6. [PMID: ] doi: 10.1016/j.vaccine.2011.09.128 [DOI] [PubMed] [Google Scholar]
- 14. World Health Organization; Norwegian Institute of Public Health. An R&D blueprint for action to prevent epidemics: funding & coordination models for preparedness and response. World Health Organization; May 2016.
- 15. Struck MM . Vaccine R&D success rates and development times. Nat Biotechnol. 1996;14:591-3. [PMID: ] [DOI] [PubMed] [Google Scholar]
- 16. Pronker ES , Weenen TC , Commandeur H , et al. Risk in vaccine research and development quantified. PLoS One. 2013;8:e57755. [PMID: ] doi: 10.1371/journal.pone.0057755 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Graham BS , Sullivan NJ . Emerging viral diseases from a vaccinology perspective: preparing for the next pandemic. Nat Immunol. 2018;19:20-28. [PMID: ] doi: 10.1038/s41590-017-0007-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Marston HD , Folkers GK , Morens DM , et al. Emerging viral diseases: confronting threats with new technologies. Sci Transl Med. 2014;6:253ps10. [PMID: ] doi: 10.1126/scitranslmed.3009872 [DOI] [PubMed] [Google Scholar]
- 19. World Health Organization. Pandemic & epidemic diseases. 2014. Accessed at www.who.int/csr/disease/WHO_PED_flyer_2014.PDF?ua=1 on 8 May 2020.
- 20. Weir JP , Gruber MF . An overview of the regulation of influenza vaccines in the United States. Influenza Other Respir Viruses. 2016;10:354-60. [PMID: ] doi: 10.1111/irv.12383 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Wei CJ , Crank MC , Shiver J , et al. Next-generation influenza vaccines: opportunities and challenges. Nat Rev Drug Discov. 2020;19:239-252. [PMID: ] doi: 10.1038/s41573-019-0056-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. National Institute of Allergy and Infectious Diseases; National Institutes of Health. Vaccine types. 1 July 2019. Accessed at www.niaid.nih.gov/research/vaccine-types on 21 March 2020.
- 23. World Health Organization. Influenza vaccines. 19 June 2019. Accessed at www.who.int/biologicals/vaccines/influenza/en on 25 June 2020.
- 24. ClinicalTrials.gov. FDAAA 801 and the Final Rule. August 2020. Accessed at https://clinicaltrials.gov/ct2/manage-recs/fdaaa on 14 October 2020.
- 25. Manzoli L , Flacco ME , D’Addario M , et al. Non-publication and delayed publication of randomized trials on vaccines: survey. BMJ. 2014;348:g3058. [PMID: ] doi: 10.1136/bmj.g3058 [DOI] [PubMed] [Google Scholar]
- 26. Therneau T. A package for survival analysis in R. 2020. R Project. Accessed at https://CRAN.R-project.org/package=survival on 16 June 2020.
- 27. Pronker ES , Weenen TC , Commandeur HR , et al. The gold industry standard for risk and cost of drug and vaccine development revisited. Vaccine. 2011;29:5846-9. [PMID: ] doi: 10.1016/j.vaccine.2011.06.051 [DOI] [PubMed] [Google Scholar]
- 28. Chit A , Parker J , Halperin SA , et al. Toward more specific and transparent research and development costs: the case of seasonal influenza vaccines. Vaccine. 2014;32:3336-40. [PMID: ] doi: 10.1016/j.vaccine.2013.06.055 [DOI] [PubMed] [Google Scholar]
- 29. Villar L , Dayan GH , Arredondo-García JL , et al; CYD15 Study Group. Efficacy of a tetravalent dengue vaccine in children in Latin America. N Engl J Med. 2015;372:113-23. [PMID: ] doi: 10.1056/NEJMoa1411037 [DOI] [PubMed] [Google Scholar]
- 30. Venkatraman N , Silman D , Folegatti PM , et al. Vaccines against Ebola virus. Vaccine. 2018;36:5454-5459. [PMID: ] doi: 10.1016/j.vaccine.2017.07.054 [DOI] [PubMed] [Google Scholar]
- 31. Lurie N , Saville M , Hatchett R , et al. Developing covid-19 vaccines at pandemic speed. N Engl J Med. 2020;382:1969-1973. [PMID: ] doi: 10.1056/NEJMp2005630 [DOI] [PubMed] [Google Scholar]
- 32. Corey L , Mascola JR , Fauci AS , et al. A strategic approach to COVID-19 vaccine R&D. Science. 2020;368:948-950. [PMID: ] doi: 10.1126/science.abc5312 [DOI] [PubMed] [Google Scholar]
- 33. Apuzzo M, Kirkpatrick DD. Covid-19 changed how the world does science, together. New York Times. 1 April 2020. Accessed at www.nytimes.com/2020/04/01/world/europe/coronavirus-science-research-cooperation.html on 17 June 2020.
- 34. Ahmed SF , Quadeer AA , McKay MR . Preliminary identification of potential vaccine targets for the COVID-19 coronavirus (SARS-CoV-2) based on SARS-CoV immunological studies. Viruses. 2020;12. [PMID: ] doi: 10.3390/v12030254 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Padron-Regalado E . Vaccines for SARS-CoV-2: lessons from other coronavirus strains. Infect Dis Ther. 2020:1-20. [PMID: ] doi: 10.1007/s40121-020-00300-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Le TT, Andreadakis Z, Kumar A, et al. The COVID-19 vaccine development landscape. Nat Rev Drug Discov. 2020;19:305-6. doi:10.1038/d41573-020-00073-5 [DOI] [PubMed]
- 37. Reed Z , Cardosa MJ . Status of research and development of vaccines for enterovirus 71. Vaccine. 2016;34:2967-2970. [PMID: ] doi: 10.1016/j.vaccine.2016.02.077 [DOI] [PubMed] [Google Scholar]
- 38. World Health Organization. WHO prequalified vaccines. 11 September 2020. Accessed at https://extranet.who.int/gavi/PQ_Web on 11 September 2020.
- 39. European Medicines Agency. Vaccines for pandemic influenza. 2018. Accessed at www.ema.europa.eu/en/human-regulatory/overview/public-health-threats/pandemic-influenza/vaccines-pandemic-influenza on 4 June 2020.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.