
Fig. 7.
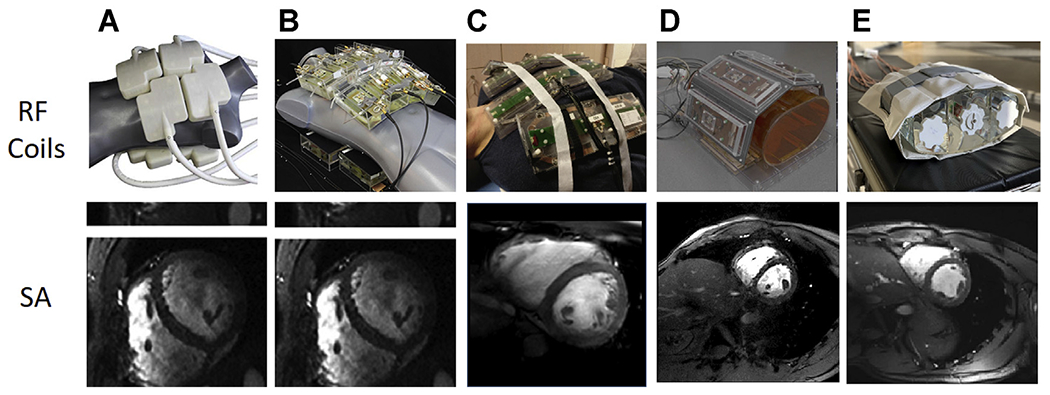
Single frames from short-axis (SA) cardiac cines acquired with 5 different 7 T body imaging arrays. (A) A 32-channel transceiver array consisting of 8 building blocks composed of 4 shielded loops in a 2 × 2 configuration per block. (B) An array composed of 16 building blocks each containing a bow tie-shaped λ/2-dipole antenna in a 4 × 2 configuration anterior and posterior. (A) and (B) used a universal RF shim solution based on EM simulations implemented through a splitter to produce a uniform field in the 4-chamber view. Images for (A) and (B) are acquired with resolutions of 1.1 × 1.1 × 2.5 mm3 and GRAPPA = 2 with acoustic cardiac triggering. (C) An 8 block array where each block is composed of a fractionated dipole transceiver and 2 receive only loops (ie, 8Tx/32Rx). The anterior elements are bent in the middle to better conform to the chest wall. Images were acquired with a resolution of 1.3 × 1.3 × 8 mm3 with subject-dependent phase-based RF shimming and VCG gating. (D) An 8-block array where each block is composed of a meander transceiver and 3 receive-only loop elements (ie, 8Tx/32Rx). RF shimming consisted of a universal phase-only RF shim and gating was performed with a finger pulse oximeter. Acquisition resolution was 1.5 × 1.5 × 3 mm3 with GRAPPA = 2 acceleration. (E) A 16-channel transceiver array with 4 loop-dipole blocks both anterior and posterior driven by a 16-channel pTx system using subject-specific static RF shim optimized for homogeneity over the heart. Acquisition parameters were 1 2 × 1.2 × 4 mm3 with GRAPPA = 2 and acquired with VCG gating. VCG, vectorcardiogram. (Courtesy of: Neindorf and Ozerdem (A, B); Steensma (C); Reitsch (D).)