

Abstract
Background:
Hospice care confers well-documented benefits to patients and their families, but it is underutilized. One potential reason for this is inadequate family support to make end-of-life decisions and care for older adults on hospice at home. We assessed the association between amount of family support and hospice use among a population of decedents and among specific illness types.
Design:
Prospective cohort study using the National Health and Aging Trends Study (NHATS) waves 2011–2017, linked to Medicare claims data.
Setting:
Contiguous United States
Participants:
1,868 NHATS decedents.
Measurements:
Outcome variable was ≥1 day of hospice. Family caregiving intensity was measured by self-reported hours of care per week and number of caregivers. Covariates included probable dementia status and other demographic, clinical and functional characteristics.
Results:
At the end of life, hours of family caregiving and numbers of helpers vary widely with individuals with dementia receiving the most hours of unpaid care (mean =64.5 hours per week) and having 2.4 unpaid caregivers on average. In an adjusted analysis, older adults with cancer receiving ≥ 40 hours of unpaid care/week as compared to < 6 hours/week were twice as likely to receive hospice care at the end of life (OR 2.0, 95% CI 1.0 – 4.1). This association was not seen among those with dementia or among decedents in general. There was no significant association between number of caregivers and hospice use at the end of life.
Conclusion:
Older adults at the end of life receive a high number of hours of help at the end of life, many from more than one caregiver, and this may shape hospice access. Better understanding of disparities in hospice use can facilitate timely access to care for older adults with serious illness.
Keywords: Hospice, family caregiving, dementia, cancer, end of life
Introduction
Families and other unpaid caregivers provide the bulk of needed care to older adults in the United States (US).1, 2 This is particularly true at the end of life,1, 3 when care intensifies in nature, new needs arise, medical decision-making is required, and caregiver burden increases.4–6 Yet population-based research on caregiving at the end of life in the population is limited7 and often focused on the caregiver-patient dyad, which may not capture the breadth of unpaid caregiving. During the end of life, care decisions (such as the decision to enter hospice care) commonly involve multiple family members, rather than a lone, primary caregiver.8, 9 There is a high degree of heterogeneity in end-of-life caregiver networks– although nearly half (44%) of caregivers report they receive no assistance from other caregivers (paid or unpaid),10 most people at the end of life are cared for by more than one unpaid caregiver (almost always a family member),1 and most decisions around healthcare are made by three or more people.8 The caregiver networks of patients also vary based on illness type and associated care needs. For example, dementia care networks are more likely to be composed of caregivers who help with multiple domains of care, rather than caregivers who help in a single area of need.11 While the size of a caregiving network expands at the end of life overall,1 it is unknown how the intensity of unpaid caregiving influences end-of-life decision-making.
A critical element of high-quality end-of-life care is access to hospice care. Hospice provides supportive care to terminally ill patients and services to families, during the patient’s last months and after their death.12 Hospice use is associated with more advance care planning, which in turn is associated with improved communication with families.13, 14 Hospice care is also associated with better pain management15 and greater family satisfaction with care, common indicators of quality end of life care.16, 17 Hospice consistently is found to improve caregiver mental health, family adjustment to bereavement, and reduce rehospitalization risk.18, 19 While hospice use is rising overall in the U.S., it remains underused among key populations.20, 21 For example, racial and ethnic minority groups use hospice at lower rates than non-Hispanic white patients.22, 23 Access to hospice care also varies by primary diagnosis. Cancer is consistently the most common principal diagnosis (30% of diagnoses),24 while dementia makes up only 15% of hospice principal diagnoses. Given the less-predictable, more gradual clinical decline of advanced dementia, individuals with dementia may not qualify for hospice until the very end of life.25–27
While the consequences of race and diagnosis on hospice enrollment are well-documented, the effect of social factors, such as family size and caregiving intensity, on hospice use are under-studied. This is a gap in research, given that vast majority of hospice care occurs at home, and caregiver support may be crucial to facilitating access.10 Previous research has demonstrated that presence of a paid caregiver significantly improves access to hospice, whereas presence of a family caregiver does not increase the likelihood of enrollment.28 However, most studies lack data on the family caregiver network, both in terms of number of family caregivers and total hours of caregiving. Measures that capture both the intensity and size of the caregiving network may better reflect the quality of care received.29–32 Characteristics of care networks have implications for patient outcomes. For instance, larger care networks are associated with worse psychological outcomes in patients with multiple comorbidities.30 On the other hand, smaller care networks may restrict access to services. While it is illegal to deny any person hospice based on lack of caregivers at home, in practice many hospice organizations still have policies in place that restrict services to those with additional home support.28,33 Additionally, home hospice provides only a median of 80.2 minutes of paid home health aide caregiving per week.34 It is critical to understand if hospice availability is limited to those with significant family caregiving resources. It is also important to understand the role of family help, when present, in facilitating hospice enrollment. These factors are likely to vary significantly by disease type due to variation in disease trajectories and caregiving needs at the end of life. The goal of this study was to examine the association between family caregiving intensity (total family caregiver hours of care and number of caregivers) and subsequent hospice use among decedents. We examined this association among all individuals at the end of life as well as for subpopulations with cancer and dementia.
Methods
Sample
This is a prospective cohort study using the National Health and Aging Trends Study (NHATS).35 NHATS is a longitudinal, nationally-representative, population-based survey of late-life disability trends and trajectories that draws from a random sample of individuals ages 65 years and older living in the contiguous U.S. We drew on the 2011–2017 NHATS survey waves which contained 8,500 persons and had a response rate for new respondents of 70.9% in the initial 2010 cohort and 63% in the 2015 replenishment cohort, with annual response rates for those already enrolled in NHATS ranging from 86% to 96%.36,37
Our cohort included community dwelling (i.e., not in a nursing home) NHATS respondents who died within twelve months of completing the NHATS interview.1, 3 Date of death was derived from the Medicare Master Beneficiary Summary File as well as from the NHATS surveys. The cohort was further limited to those who reported having any unpaid caregiver in their last NHATS interview prior to death, who helped with an activity of daily living (ADL; or eating, bathing, using the toilet, dressing, getting around inside, and getting in and out of bed) or an instrumental activity of daily living (IADL; or preparing light meals, managing money, shopping, performing housework, doing laundry, and using a telephone). This left a sample of 1,868 older adults. The Johns Hopkins University Institutional Review Board approved the NHATS protocol, and all participants provided written informed consent. The Icahn School of Medicine at Mount Sinai’s Institutional Review Board and the Centers for Medicare & Medicaid Services Privacy Board approved the study.
Measures
The primary dependent variable was utilization of hospice, defined as receiving one or more days of hospice services, as reflected by Medicare billing data.
We examined family caregiving intensity using two approaches: the total number of unpaid caregiving hours per week in the last interview before death (median =15.0 hours), and the number of individual unpaid caregivers. The number of unpaid caregiver hours/week was categorized as <6 hours/week, 6–19.9, 20–39.9, and 40 or more to approximate quartiles. The number of unpaid caregivers was categorized as 1, 2, and 3 or more.
The following covariates were included to capture key functional and demographic characteristics: age, sex, race, education, marital status, income, living arrangements, the number of ADLs and IADLs for which the individual received help, as well as whether they received help from a paid caregiver in the last interview before death. Primary caregiver was defined as the person providing the most hours of help to the decedent. If number of hours were equal between a son and a daughter, we designated the daughter as the primary caregiver (less than one percent of cases). Although we did not have a measure of cause of death, we identified two subpopulations with dementia and cancer. Dementia was measured through a “probable dementia” indicator on the NHATS survey, which was determined by cognitive testing and other reporting during the NHATS survey.38 Participants were asked if they had ever had cancer in their initial interview and each year they were queried to report new cancers. Other self-reported medical conditions included heart attack, heart disease (including angina and congestive heart failure), high blood pressure, arthritis, osteoporosis, diabetes, lung disease, stroke, depression, anxiety, and broken or fractured hip. Based on these conditions, we developed a count of total medical conditions. Self-reported health was dichotomized as fair/poor vs. good, very good, and excellent.39
Analysis
We first described the characteristics and caregiving patterns of our cohort of older adults receiving family help at the end of life as well as those with cancer and dementia. Next, we conducted multivariable logistic regression modeling the association between total caregiving hours and number of caregivers and hospice use at the end of life, adjusting for multiple demographic and clinical characteristics as well as receipt of paid care. The association was assessed for the entire cohort, for only those reporting cancer diagnoses, and for only those with probable dementia. Because short hospice stays are not considered high quality end-of-life care,40 we also ran our model with 2 additional hospice length of stay outcomes: 3 or more days and 15 or more days. Finally, we ran a sensitivity analysis limiting the cancer subpopulation to those with new cancers only. All analyses used survey weights to account for differential nonresponse and the complex sampling design.41 All analyses were completed using Stata Statistical Software: Release 16. College Station, TX.
Results
Sample characteristics
We identified 1,868 community-dwelling individuals who died within 1 year and received any family help with ADLs or IADLs according to their last NHATS interview prior to death (Table 1). The average age in our sample population was 82.5 and 54% of participants were female. The majority (78%) of the participants were White, 10% were Black, and 7% were Hispanic. Forty percent of participants were married, 35% lived alone, and, on average, participants had 3 living children. Fifty-five percent of participants needed help with one or more ADLs and 66% required help with one or more IADLs. Of 1,868 older adults in the sample, 822 had dementia and 686 had cancer (not mutually exclusive). Fourteen percent of decedents had both cancer and dementia. Fifty-two percent of decedents used hospice, 62% of patients with dementia used hospice, and 61% of patients with cancer used hospice. Median length of stay for those who had any hospice use was 16 days for the full sample, 21 days for the dementia subgroup, and 18 days for the cancer subgroup. Over half of hospice stays were 15 days or longer.
Table 1:
Characteristics of community-dwelling older adults in the last 12 months of life
| All (1,868) | Dementiaa (822) | Cancera (686) | |
|---|---|---|---|
| Demographic and social characteristics: | |||
| Age, years, mean (SD) | 82.45 (8.37) | 85.23 (8.19) | 81.97 (8.14) |
| Female, % | 53.69 | 56.68 | 49.58 |
| White Non-Hispanic race, % | 78.21 | 73.80 | 83.92 |
| Black Non-Hispanic race, % | 9.51 | 10.24 | 6.59 |
| Hispanic race, % | 6.94 | 8.89 | 4.10 |
| Other race, % | 3.59 | 4.74 | 3.56 |
| Completed high school, % | 70.57 | 64.84 | 77.59 |
| Enrolled in Medicaid, % | 19.75 | 22.80 | 15.07 |
| Northeastern region, % | 20.33 | 17.72 | 15.39 |
| Midwestern region, % | 24.16 | 20.82 | 27.51 |
| Southern region, % | 34.09 | 35.24 | 35.12 |
| Married, % | 40.27 | 34.76 | 45.79 |
| Lives alone, % | 35.38 | 33.62 | 33.30 |
| Residential care, % | 17.27 | 24.79 | 17.48 |
| Number of living children, mean (SD) | 2.95 (2.03) | 2.99 (2.12) | 2.99(1.97) |
| Health and function characteristics: | |||
| Cancer, % | 36.72 | 32.56 | - |
| Dementia, % | 44.00 | - | 38.83 |
| Count of medical conditions, mean (SD)b | 4.44(2.15) | 5.06(2.23) | 5.16 (2.08) |
| Help with ≥1 ADL, %c | 55.03 | 84.18 | 54.34 |
| Average number of ADLs, mean (SD) | 1.86 (2.19) | 3.40(2.23) | 1.76 (2.12) |
| Help with ≥1 IADL, %d | 65.69 | 91.15 | 63.82 |
| Average number of IADLs, mean (SD) | 2.02 (1.92) | 3.26 (1.77) | 1.92 (1.89) |
| Self reported health fair/poor, %e | 55.57 | 63.56 | 60.94 |
| Hospice Use: | |||
| Any hospice use, % | 51.55 | 61.97 | 60.86 |
| Median length of stay (IQR), days | 16 (5 – 50) | 21 (6 – 91) | 18 (5 – 48) |
| Length of stay 1–2 days, % | 10.74 | 9.76 | 9.25 |
| Length of stay 3 – 14 days, % | 37.68 | 33.70 | 35.53 |
| Length of stay ≥ 15 days, % | 51.58 | 56.54 | 55.22 |
Analyses were weighted to produce nationally representative estimates.
Dementia status was determined using the NHATS dementia classification variable. Cancer status was from self-report. Dementia and cancer populations were not mutually exclusive.
Based on self-report of heart disease, hypertension, arthritis, osteoporosis, diabetes, lung disease, stroke, dementia or Alzheimer disease, cancer, depression, anxiety, and broken hip.
Activities of daily living (ADLs) include bathing, eating, dressing, toileting, getting around inside, getting out of bed.
Instrumental activities of daily living (IADLs) include preparing meals, managing money, shopping for groceries or personal items, performing housework, doing laundry, and using a telephone.
As opposed to good, very good, or excellent.
Caregiving patterns at the end of life
Decedents with dementia reported the largest family care networks (average of 2.4 helpers, compared to 2.2 helpers for those with cancer and 2.2 for the total cohort) and the most hours of family care (64.5 hours per week compared to 39.3 hours per week for those with cancer and 41.0 for the total cohort) (Table 2). In fact, 47% of decedents with dementia received more than 40 hours of family help, and 40% of them had 3 or more unpaid caregivers in their care networks. The dementia subgroup, in addition to having the highest ADL needs, was most likely to receive paid help.
Table 2.
Caregiving patterns at the end of life for community-dwelling older adults.
| All (N= 1,868) | Dementiaa (N= 822) | Cancera (N= 686) | |
|---|---|---|---|
| Unpaid caregivers: | |||
| Number of unpaid caregivers reported, mean (SD) | 2.19 (1.29) | 2.43 (1.36) | 2.20 (1.28) |
| Average hours of unpaid care per week, mean (SD) | 41.03 (58.67) | 64.45 (72.16) | 39.29 (55.81) |
| < 6 hours unpaid care per week, % | 28.10 | 18.99 | 25.51 |
| 6 – 19 hours of unpaid care per week, % | 26.48 | 19.57 | 28.55 |
| 20 – 39 hours of unpaid care per week, % | 16.74 | 14.83 | 18.70 |
| ≥ 40 hours of unpaid care per week, % | 28.68 | 46.61 | 27.23 |
| 1 unpaid caregiver, % | 35.63 | 26.83 | 35.26 |
| 2 unpaid caregivers, % | 32.40 | 32.90 | 32.79 |
| ≥ 3 unpaid caregivers, % | 31.97 | 40.28 | 31.95 |
| Paid caregivers: | |||
| Received help from ≥1 paid caregiver, % | 18.63 | 24.09 | 19.74 |
| 0 hours paid care per week, % | 82.36 | 76.05 | 81.14 |
| <20 hours paid care per week, % | 10.92 | 11.92 | 11.07 |
| 20–39 hours paid care per week, % | 2.43 | 3.65 | 3.31 |
| 40+ hours paid care per week, % | 4.29 | 8.39 | 4.48 |
| Both paid and unpaid caregivers: | |||
| Number of paid and unpaid caregivers reported, mean (SD) | 2.43(1.44) | 2.75 (1.50) | 2.44 (1.42) |
| Primary caregiverb, %: | |||
| Spouse/Partner | 34.14 | 27.55 | 38.44 |
| Daughter | 26.75 | 31.11 | 26.17 |
| Son | 12.23 | 13.62 | 9.73 |
| Other unpaid caregiver | 19.43 | 17.91 | 18.15 |
| Paid caregiver | 7.39 | 9.82 | 7.51 |
Analyses were weighted to produce nationally representative estimates.
Dementia status was determined using the NHATS dementia classification variable. Cancer status was from self-report. Dementia and cancer populations were not mutually exclusive.
Primary caregiver was defined as the person providing the most hours of help to decedent. In the case of a tie between son and daughter, the daughter was designated the primary caregiver.
Association between care networks and hospice use
As depicted in Figure 1, increased unpaid caregiving hours was associated with increased hospice use overall. This trend was particularly evident among those with cancer.
Figure 1:
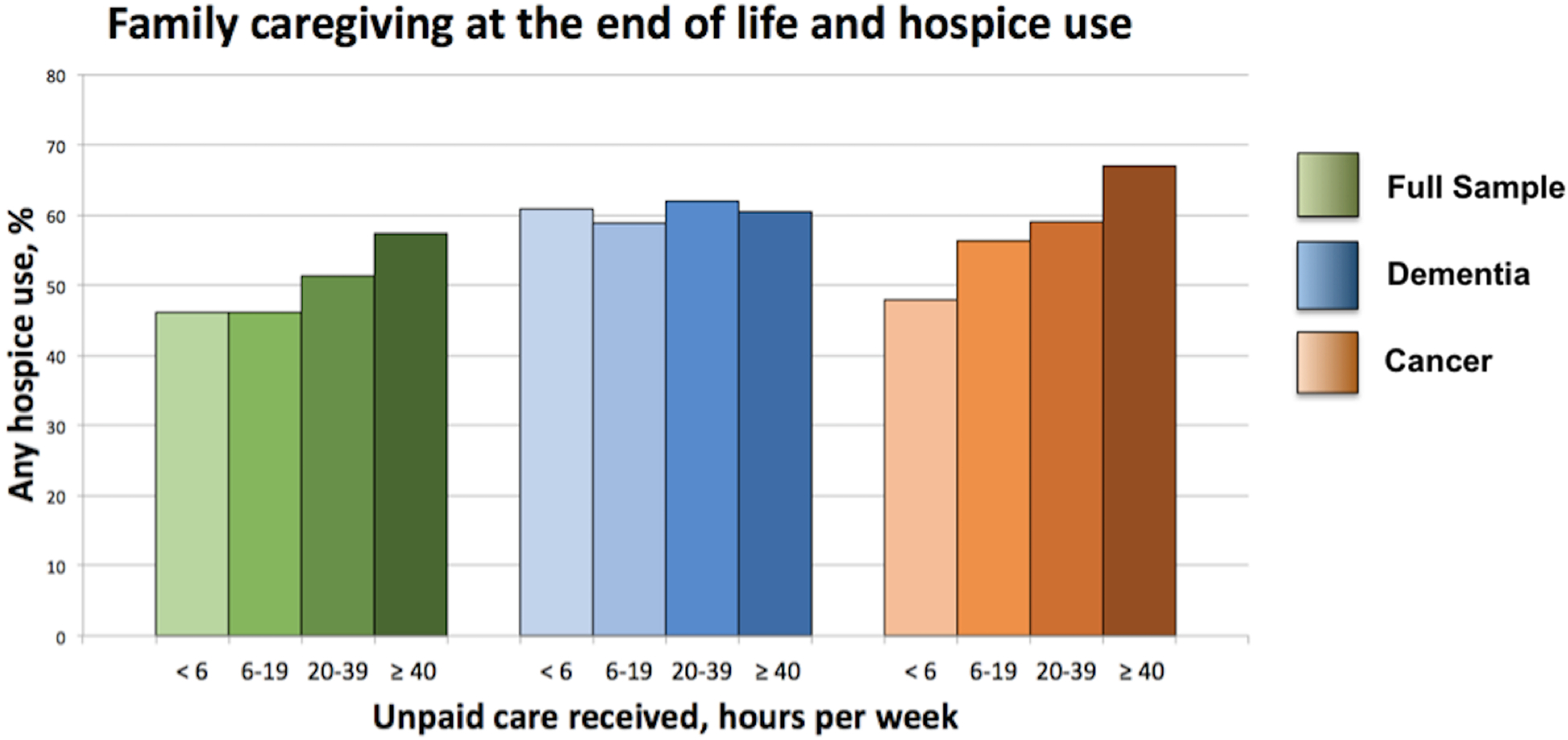
Hospice use increases with increasing hours of family care in cancer patients
In adjusted models (Table 3), there was no association between caregiving hours and hospice use for the full sample and the subset of those with dementia. For those with cancer, those receiving ≥ 40 hours of help per week had more than double the odds of receiving hospice compared to those receiving less than 6 hours of family caregiving per week (odds ratio, OR, 2.03, 95% confidence interval, CI, 1.01–4.08). In the dementia subgroup and the full sample, those receiving ≥ 40 hours of help per week had a higher likelihood of receiving hospice compared to those receiving less than 6 hours of family caregiving per week, but this effect was not statistically significant. As shown in Table 4, there was no association between number of caregivers and hospice use in the full sample or either subgroup.
Table 3:
Adjusted Association between unpaid caregiving hours and hospice use at the end of life
| Full Sample | Dementiaa | Cancera | |
|---|---|---|---|
| OR (CI) | OR (CI) | OR (CI) | |
| Unpaid caregiving hours: | |||
| < 6 hours/week | Reference | Reference | Reference |
| 6 – 19 hours/week | 1.04 (0.80 – 1.36) | 1.10 (0.66 – 1.82) | 1.25 (0.69 – 2.25) |
| 20 – 39 hours/week | 0.94 (0.65 – 1.34) | 1.38 (0.68 – 2.79) | 1.06 (0.62 – 1.84) |
| ≥ 40 hours/week | 1.21 (0.84 – 1.74) | 1.12 (0.73 – 1.73) | 2.03 (1.01 – 4.08)* |
| Any paid caregiver | 1.01 (0.72 – 1.42) | 1.10 (0.70 – 1.73) | 1.40 (0.79 – 2.47) |
| Age | 1.01 (1.00 – 1.03) | 1.01 (0.99 – 1.04) | 0.97 (0.94 – 1.00) |
| Female | 1.16 (0.84 – 1.60) | 1.03 (0.65 – 1.63) | 1.75 (1.06 – 2.88)* |
| Black Non-Hispanic | 0.56 (0.39 – 0.80)** | 0.75 (0.47 – 1.20) | 0.41 (0.24 – 0.68)** |
| Other race/ethnicity | 0.63 (0.25 – 1.56) | 1.39 (0.48 – 4.04) | 0.17 (0.05 – 0.61)** |
| Hispanic | 0.62 (0.41 – 0.93)* | 0.93 (0.49 – 1.79) | 1.12 (0.35 – 3.56) |
| Education: High School+ | 1.00 (0.76 – 1.33) | 1.48(1.00 – 2.18)* | 0.83 (0.50 – 1.36) |
| Married | 1.06 (0.80 – 1.40) | 0.81 (0.50 – 1.30) | 0.94 (0.56 – 1.58) |
| Northeast | 0.52 (0.35 – 0.76)** | 0.48(0.31 – 0.76)** | 0.36 (0.20 – 0.62)** |
| South | 0.82 (0.60 – 1.13) | 0.79 (0.46 – 1.35) | 0.57 (0.31 – 1.05) |
| Midwest | 0.92 (0.64 – 1.30) | 1.05 (0.61 – 1.81) | 0.80 (0.46 – 1.39) |
| Medicaid | 0.87 (0.60 – 1.25) | 0.80 (0.49 – 1.31) | 0.75 (0.39 – 1.48) |
| Dementiaa | 1.52 (1.15 – 2.02)** | 1.68 (1.04 – 2.71)* | |
| Cancera | 1.72 (1.34 – 2.21)** | 1.52(1.07 – 2.16)* | |
| Count of Medical Conditionsb | 1.06 (0.98 – 1.13) | 1.07 (0.98 – 1.18) | 1.00 (0.89 – 1.12) |
| Help with ≥1 ADLc | 1.408 (0.99 – 1.99) | 1.84(1.10 – 3.07)* | 1.73 (1.01 – 2.94)* |
| Help with ≥1 IADLd | 0.93 (0.66 – 1.32) | 1.16 (0.65 – 2.07) | 0.64 (0.38 – 1.08) |
| Self reported health fair/poore | 1.12 (0.84 – 1.49) | 1.06 (0.64 – 1.77) | 1.64 (1.11 – 2.43)* |
| Number living children | 1.04 (0.97 – 1.11) | 1.00 (0.92 – 1.08) | 1.01 (0.92 – 1.11) |
Analyses were weighted to produce nationally representative estimates.
indicates p-value < 0.05;
indicates p-value < 0.005.
Dementia status was determined using the NHATS dementia classification variable. Cancer status was from self-report. Dementia and cancer populations were not mutually exclusive.
Based on self-report of heart disease, hypertension, arthritis, osteoporosis, diabetes, lung disease, stroke, dementia or Alzheimer disease, cancer, depression, anxiety, and broken hip.
Activities of daily living (ADLs) include bathing, eating, dressing, toileting, getting around inside, getting out of bed.
Instrumental activities of daily living (IADLs) include preparing meals, managing money, shopping for groceries or personal items, performing housework, doing laundry, and using a telephone.
As opposed to good, very good, or excellent.
Table 4:
Adjusted Association between unpaid caregivers and hospice use at the end of life
| Full Sample | Dementiaa | Cancera | |
|---|---|---|---|
| OR (CI) | OR (CI) | OR (CI) | |
| Number unpaid caregivers: | |||
| 1 unpaid caregiver | Reference | Reference | Reference |
| 2 unpaid caregivers | 0.92 (0.69 – 1.24) | 1.03 (0.62 – 1.71) | 0.67 (0.42 – 1.09) |
| ≥ 3 unpaid caregivers | 1.16 (0.84 – 1.59) | 1.45 (0.78 – 2.68) | 0.98 (0.57 – 1.69) |
| Any paid caregiver | 0.99 (0.70 – 1.40) | 1.11 (0.70 – 1.76) | 1.27 (0.71 – 2.28) |
| Age | 1.01(1.00 – 1.03) | 1.01 (1.00 – 1.04) | 0.97 (0.94 – 1.00) |
| Female | 1.14 (0.83 – 1.57) | 1.05 (0.66 – 1.68) | 1.66 (1.02 – 2.69)* |
| Black, Non-Hispanic | 0.57(0.40 – 0.80)** | 0.73 (0.45 – 1.18) | 0.44 (0.27–0.72)** |
| Other race/ethnicity | 0.65 (0.26 – 1.60) | 1.37 (0.49 – 3.85) | 0.19 (0.05 – 0.69)* |
| Hispanic | 0.63 (0.41 – 0.95)* | 0.90 (0.47 – 1.75) | 1.03 (0.31 – 3.39) |
| Education: High School+ | 0.99 (0.75 – 1.30) | 1.48 (0.99 – 2.22) | 0.78 (0.46 – 1.32) |
| Married | 1.07 (0.83 – 1.38) | 0.83 (0.52 – 1.33) | 0.95 (0.58 – 1.56) |
| Northeast | 0.52 (0.35 – 0.75)** | 0.47 (0.30 – 0.72)** | 0.36 (0.20–0.64)** |
| South | 0.83 (0.60 – 1.14) | 0.79 (0.46 – 1.39) | 0.59 (0.32 – 1.10) |
| Midwest | 0.92 (0.68 – 1.32) | 1.02 (0.61 – 1.73) | 0.83 (0.47 – 1.49) |
| Medicaid | 0.87 (0.61 – 1.24) | 0.80 (0.49 – 1.29) | 0.70 (0.37 – 1.35) |
| Dementiaa | 1.55 (1.17 – 2.05)** | 1.65 (1.03 – 2.65)* | |
| Cancera | 1.71 (1.33 – 2.21)** | 1.49 (1.05 – 2.12)* | |
| Count medical conditionsb | 1.06 (0.99 – 1.14) | 1.08 (0.98 – 1.19) | 1.01 (0.90 – 1.13) |
| Help with ≥1 ADLc | 1.47 (1.06 – 2.04)* | 1.73 (1.03 – 2.91)* | 1.98 (1.17 – 3.33)* |
| Help with ≥1 IADLd | 0.92 (0.64 – 1.32) | 1.11 (0.63 – 1.95) | 0.74 (0.43 – 1.27) |
| Self reported health fair/poore | 1.11 (0.84 – 1.48) | 1.05 (0.63 – 1.73) | 1.68 (1.13 – 2.51)* |
| Number of living children | 1.03 (0.97 – 1.10) | 0.98 (0.89 – 1.07) | 1.02 (0.92 – 1.12) |
Analyses were weighted to produce nationally representative estimates.
indicates p-value < 0.05;
indicates p-value < 0.005.
Dementia status was determined using the NHATS dementia classification variable. Cancer status was from self-report. Dementia and cancer populations were not mutually exclusive.
Based on self-report of heart disease, hypertension, arthritis, osteoporosis, diabetes, lung disease, stroke, dementia or Alzheimer disease, cancer, depression, anxiety, and broken hip.
Activities of daily living (ADLs) include bathing, eating, dressing, toileting, getting around inside, getting out of bed.
Instrumental activities of daily living (IADLs) include preparing meals, managing money, shopping for groceries or personal items, performing housework, doing laundry, and using a telephone.
As opposed to good, very good, or excellent.
Sensitivity analyses
As a sensitivity analysis, we considered two alternative definitions of hospice use. First, we defined hospice use as 3 or more days of hospice care. We found similar patterns using this definition of hospice use: in the full sample and dementia sample, there was no association between increased hours of family caregiving, but in the cancer sample there was a trend of increased hospice use among patients who received greater than or equal 40 hours of family care (OR = 1.6, 95% CI 0.8–3.3). Similarly, when we examined hospice use defined as 15 or more days, we found a positive association between caregiving hours and hospice use among the cancer subpopulation (Supplemental Table 1). We also ran a sensitivity analysis restricting our cancer subgroup to those with a new cancer diagnosed in the year of interview. Results did not substantially differ in direction or magnitude.
Discussion
In this nationally representative, prospective study, we found significant heterogeneity in caregiving resources at the end of life with key implications for hospice use. Decedents with cancer who had family caregivers providing more than 40 hours of unpaid help per week at the end of life compared to those with less than 6 hours of unpaid help were more likely to subsequently enroll in hospice. This finding suggests that hospice access may be limited for those with less caregiver resources, at least among the cancer population.
Our assessment of both the total caregiving hours and number of caregivers at the end of life revealed high caregiver reliance, especially among those with dementia. More than one quarter of older adults at the end of life required more than 40 hours of unpaid help a week, representing a full-time unpaid caregiving job. For those with dementia, this number rose to over 45%. Patients with dementia had larger family care networks, with an average size of 2.4 people versus 2.2 in the full sample, highlighting the importance of including all caregivers in analyses rather than one primary caregiver.
There are several likely reasons why decedents with cancer who have more hours of caregiver support at the end of life are more likely to access hospice. Cancer, a terminal illness, has a unique trajectory of sudden decline and escalating care needs at the end of life.42 This relatively predictable disease course makes the clinical decision to recommend hospice easier for doctors, especially compared to prognostication in dementia.43,44 However, our results show that there is an additional effect of the number of unpaid care hours as well that contributes to hospice use among cancer patients. The suddenly escalated care needs at the end of life may prompt family members of those with cancer to seek out support via hospice services.
Those with dementia, by contrast, likely have had years of high-level care needs45 and may already have care supports in place prior to the end-of-life, including paid caregiver support. Individuals with dementia who are able to stay at home at the end of life have actively engaged caregiving support.46 Additionally, 25% of persons with dementia lived in residential care settings, which may also reflect more engaged paid caregiver support in this population.47 Given that those with dementia had higher total caregiver use and hours of care, and that hospice provides few caregiving hours, it is possible these individuals opt for non-hospice care at the end of life such as skilled nursing or rehabilitation care. Additionally, increased caregiving hours for dementia patients are more likely to reflect worsening cognitive and behavioral problems,48 a less clear indicator of need for hospice care. Because our study focused on individuals living in the community, we are unable to examine how hospice use may be impacted by caregiving support among individuals living in nursing homes.
We separately tested the association between two measures of caregiver intensity and hospice use. Although we did not find that number of caregivers was associated with hospice use, we did see that total caregiving hours resulted in a two-fold increase in hospice enrollment for those with cancer. While larger care networks generally provide more hours of care,33 the relationship between the two may not be linear. A patient may have many people providing small amounts of care to them, while a patient who receives more hours from fewer people is likely receiving more involved care that may influence care decisions. Alternatively, our metric of caregiving resources may not have adequately represented caregiver involvement in the hospice decision-making process. It is possible that patients with high care hours and larger networks may still not have had the active family involvement in care decisions that is generally associated with transitioning to hospice care. Future research will require larger datasets to simultaneously examine hours of care and care network size as well as other caregiving factors, e.g., relationship quality, on end-of-life decision-making.
There are limitations in this study. It is possible that caregiving hours is capturing acuity of illness as opposed to caregiver resources. However, all patients in the sample died within one year and we adjust for level of disability as well as several other measures of illness, including self-reported health and number of comorbidities. Several of our measures rely on self-report including function and hours of care received. Our measure of cancer was also based on self-report of cancer diagnosis and, although used by others,1, 49 includes all cancers the respondent has and is not necessarily the cause of death, which is not available in NHATS. When limiting our cancer subpopulation to those with new cancers in the period before death in sensitivity analyses, we continued to find an association between caregiver support and hospice use. We are also unable to differentiate cancer type and stage, which may have consequences for hospice use. Furthermore, cancer and dementia in our subpopulations were not necessarily the principal diagnosis or cause of death in these decedents. They are also not mutually exclusive diagnoses. Our focus was on receipt of unpaid caregiving hours, and while we adjusted for receipt of paid care in our models, further research on the quantity and quality of paid caregiving support and its role in hospice care is warranted. While this study is representative of the Medicare population, it does not include younger decedents. Our model only incorporated decedents who had unpaid help in their last year of life, excluding those who did not have access to any family help. Additionally, our inclusion criteria used a 12 month period to delineate the end of life. This period, often in end of life care studies,1, 3, 48, 50 may not capture illnesses of longer duration.
Our main indicator of hospice use was one day or more. We did not examine hospice disenrollment or examine different lengths of hospice stay, some of which may have been very short, given hospice use statistics.40 In sensitivity analyses we tested alternative definitions of hospice use and found similar results. Across all lengths of stay, increased unpaid help for decedents with cancer was associated with increased hospice use. While our work expands on prior work by including all family caregivers, our measure of hours of care received captures only one dimension of a complex care system. Care networks may also be described by network composition and quality of care. Network analysis often studies nuanced elements of care networks, such as density, the degree to which network members spend time with each other. Such measures of care network analysis were out of reach in this large-scale, population-based study. Understanding the most useful measures of caregiver networks is critical to move forward with work to assess the link between caregiving and quality of end-of-life care.
This work is the first we are aware of to consider the association between caregiver intensity – hours of care and numbers of caregivers – and hospice use, a measure of quality of end-of-life care. By considering the entirety of the care network we were able to more completely assess the extent and breadth of care needs of older adults at the end of life. Our findings demonstrate the importance of assessing entire family and household resources to plan care. Our finding that increased caregiving hours are associated with increased hospice use for cancer patients (who remain the largest population of hospice users) indicates a potential driver of disparities in hospice use. Given that the Medicare hospice benefit pays for limited caregiving hours and that institutional care is financially burdensome for individuals who do not qualify for Medicaid but still have limited resources, patients who might otherwise use hospice may be prohibited from this benefit due to low family support. It is critical that hospice programs provide adequate in-home assistance to all patients, regardless of family member availability. Failure to do so may further perpetuate socioeconomic disparities in access to hospice,22, 23 both in terms of an individual’s family composition and the economic ability of their family to take time off of work to provide unpaid care. Researchers and policy makers must ensure that Medicare beneficiaries are not foregoing hospice care because they do not have adequate caregiving resources. Furthermore, it is important that researchers and hospice agencies study what interventions, such as increased home health aide support, might facilitate greater hospice access for those with less family support. Attending to these disparities can make hospice and quality end-of-life care more accessible to all older adults.
Supplementary Material
Supplemental Table 1: Hospice length of stay by disease type
Acknowledgments
Conflict of interest: Vedika Kumar was funded by the Patricia S. Levinson Summer Research Award. Dr. Ornstein was funded by grant number NIA K01AG047923. National Health and Aging Trends Study (NHATS) is sponsored by the National Institute on Aging (grant number NIA U01AG32947) and was conducted by the Johns Hopkins University.
Footnotes
Sponsor’s Role: Funders played no role in the study’s design, methods, subject recruitment, data collection, analysis, and preparation of the paper.
References
- 1.Ornstein KA, Kelley AS, Bollens-Lund E and Wolff JL, A national profile of end-of-life caregiving in the United States. Health Affairs, 2017. 36(7): p. 1184–1192. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Wolff JL, Spillman BC, Freedman VA and Kasper JD, A national profile of family and unpaid caregivers who assist older adults with health care activities. JAMA Internal Medicine, 2016. 176(3): p. 372–379. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Wolff JL, Dy SM, Frick KD and Kasper JD, End-of-life care: findings from a national survey of informal caregivers. Archives of Internal Medicine, 2007. 167(1): p. 40–46. [DOI] [PubMed] [Google Scholar]
- 4.Kehl KA, Kirchhoff KT, Kramer BJ and Hovland-Scafe C, Challenges facing families at the end of life in three settings. Journal of social work in end-of-life & palliative care, 2009. 5(3–4): p. 144–168. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.McMillan SC, Interventions to facilitate family caregiving at the end of life. Journal of Palliative Medicine, 2005. 8(supplement 1): p. s-132–s-139. [DOI] [PubMed] [Google Scholar]
- 6.Emanuel EJ, Fairclough DL, Slutsman J and Emanuel LL, Understanding economic and other burdens of terminal illness: the experience of patients and their caregivers. Annals of internal medicine, 2000. 132(6): p. 451–459. [DOI] [PubMed] [Google Scholar]
- 7.Stajduhar KI, Funk L, Toye C, Grande GE, Aoun S and Todd CJ, Part 1: Home-based family caregiving at the end of life: a comprehensive review of published quantitative research (1998–2008). Palliative medicine, 2010. 24(6): p. 573–593. [DOI] [PubMed] [Google Scholar]
- 8.Haley WE, Allen RS, Reynolds S, Chen H, Burton A and Gallagher-Thompson D, Family issues in end-of-life decision making and end-of-life care. American Behavioral Scientist, 2002. 46(2): p. 284–298. [Google Scholar]
- 9.Rutherford A and Bowes A, Networks of informal caring: a mixed-methods approach. Canadian Journal on Aging/La Revue canadienne du vieillissement, 2014. 33(4): p. 473–487. [DOI] [PubMed] [Google Scholar]
- 10.National H and Palliative Care O, NHPCO facts and figures: Hospice care in America. 2012, National Hospice and Palliative Care Organization; Alexandria, VA. [Google Scholar]
- 11.Spillman BC, Freedman VA, Kasper JD and Wolff JL, Change over time in caregiving networks for older adults with and without dementia. The Journals of Gerontology: Series B, 2019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Ornstein KA, Aldridge MD, Mair CA, Gorges R, Siu AL and Kelley AS, Spousal characteristics and older adults’ hospice use: Understanding disparities in end-of-life care. Journal of palliative medicine, 2016. 19(5): p. 509–515. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Teno JM, Gruneir A, Schwartz Z, Nanda A and Wetle T, Association between advance directives and quality of end‐of‐life care: A national study. Journal of the American Geriatrics Society, 2007. 55(2): p. 189–194. [DOI] [PubMed] [Google Scholar]
- 14.Garrido MM, Balboni TA, Maciejewski PK, Bao Y and Prigerson HG, Quality of life and cost of care at the end of life: the role of advance directives. Journal of pain and symptom management, 2015. 49(5): p. 828–835. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Miller SC, Mor V, Wu N, Gozalo P and Lapane K , Does receipt of hospice care in nursing homes improve the management of pain at the end of life? Journal of the American Geriatrics Society, 2002. 50(3): p. 507–515. [DOI] [PubMed] [Google Scholar]
- 16.Earle CC, Park ER, Lai B, Weeks JC, Ayanian JZ and Block S, Identifying potential indicators of the quality of end-of-life cancer care from administrative data. Journal of Clinical Oncology, 2003. 21(6): p. 1133–1138. [DOI] [PubMed] [Google Scholar]
- 17.Wachterman MW, Pilver C, Smith D, Ersek M, Lipsitz SR and Keating NL, Quality of end-of-life care provided to patients with different serious illnesses. JAMA internal medicine, 2016. 176(8): p. 1095–1102. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Holden TR, Smith MA, Bartels CM, Campbell TC, Yu M and Kind AJH, Hospice enrollment, local hospice utilization patterns, and rehospitalization in medicare patients. Journal of palliative medicine, 2015. 18(7): p. 601–612. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Teno JM, Clarridge BR, Casey V, et al. , Family perspectives on end-of-life care at the last place of care. Jama, 2004. 291(1): p. 88–93. [DOI] [PubMed] [Google Scholar]
- 20.Aldridge MD, Canavan M, Cherlin E and Bradley EH, Has hospice use changed? 2000–2010 utilization patterns. Medical care, 2015. 53(1): p. 95. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Garcia MJ, Systematic Review of the Literature on Why There is Hospice Underutilization. 2018.
- 22.Cohen LL, Racial/ethnic disparities in hospice care: a systematic review. Journal of palliative medicine, 2008. 11(5): p. 763–768. [DOI] [PubMed] [Google Scholar]
- 23.Jarosek S, Shippee TP and Virnig B. RACIAL DISPARITIES IN THE USE OF THE MEDICARE HOSPICE BENEFIT OVER TIME in Gerontologist. 2015. OXFORD UNIV PRESS INC JOURNALS DEPT, 2001 EVANS RD, CARY, NC 27513 USA. [Google Scholar]
- 24.Alexandria V, NHPCO Facts and Figures: Hospice Care in America. 2018, National Hospice and Palliative Care Organization. [Google Scholar]
- 25.Sachs GA, Shega JW and Cox-Hayley D, Barriers to excellent end-of-life care for patients with dementia. Journal of general internal medicine, 2004. 19(10): p. 1057–1063. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Mitchell SL, Teno JM, Kiely DK, et al. , The clinical course of advanced dementia. New England Journal of Medicine, 2009. 361(16): p. 1529–1538. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Shega JW, Hougham GW, Stocking CB, Cox-Hayley D and Sachs GA, Patients dying with dementia: experience at the end of life and impact of hospice care. Journal of pain and symptom management, 2008. 35(5): p. 499–507. [DOI] [PubMed] [Google Scholar]
- 28.Van Houtven CH, Taylor DH Jr, Steinhauser K and Tulsky JA, Is a home-care network necessary to access the Medicare hospice benefit? Journal of palliative medicine, 2009. 12(8): p. 687–694. [DOI] [PubMed] [Google Scholar]
- 29.Keating N, Otfinowski P, Wenger C, Fast J and Derksen L, Understanding the caring capacity of informal networks of frail seniors: a case for care networks. Ageing & Society, 2003. 23(1): p. 115–127. [Google Scholar]
- 30.Andersson MA and Monin JK, Informal Care Networks in the Context of Multimorbidity: Size, Composition, and Associations With Recipient Psychological Well-Being. Journal of aging and health, 2018. 30(4): p. 641–664. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Fast J, Keating N, Otfinowski P and Derksen L, Characteristics of family/friend care networks of frail seniors. Canadian Journal on Aging/La Revue Canadienne du Vieillissement, 2004. 23(1): p. 5–19. [DOI] [PubMed] [Google Scholar]
- 32.Koehly LM, Ashida S, Schafer EJ and Ludden A, Caregiving networks—Using a network approach to identify missed opportunities. Journals of Gerontology Series B: Psychological Sciences and Social Sciences, 2014. 70(1): p. 143–154. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Aldridge Carlson MD, Barry CL, Cherlin EJ, McCorkle R and Bradley EH, Hospices’ enrollment policies may contribute to underuse of hospice care in the United States. Health Affairs, 2012. 31(12): p. 2690–2698. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Unroe KT, Bernard B, Stump TE, Tu W and Callahan CM, Variation in hospice services by location of care: nursing home versus assisted living facility versus home. Journal of the American Geriatrics Society, 2017. 65(7): p. 1490–1496. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Kasper JD and Freedman VA, National Health and Aging Trends Study (NHATS) User Guide Rounds 1 & 2. 2013. 2014.
- 36.DeMatteis J, Freedman VA and Kasper JD, National Health and Aging Trends Study Round 5 Sample Design and Selection. NHATS Technical Paper# 16. Baltimore: Johns Hopkins University School of Public Health; 2016.
- 37.Kasper JD and Freedman VA, National Health and Aging Trends Study (NHATS) user guide: rounds 1–7. 2018.
- 38.Kasper JD, Freedman VA and Spillman BC, Classification of persons by dementia status in the National Health and Aging Trends Study. Technical Paper, 2013. 5. [Google Scholar]
- 39.DeSalvo KB, Bloser N, Reynolds K, He J and Muntner P, Mortality prediction with a single general self-rated health question. Journal of general internal medicine, 2006. 21(3): p. 267. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Teno JM, Shu JE, Casarett D, Spence C, Rhodes R and Connor S, Timing of referral to hospice and quality of care: length of stay and bereaved family members’ perceptions of the timing of hospice referral. Journal of pain and symptom management, 2007. 34(2): p. 120–125. [DOI] [PubMed] [Google Scholar]
- 41.Montaquila J, Freedman VA, Spillman B and Kasper JD, National Health and Aging Trends Study development of round 1 survey weights. NHATS technical paper, 2012. 2. [Google Scholar]
- 42.Waldrop DP and Meeker MA, Hospice decision making: Diagnosis makes a difference. The Gerontologist, 2012. 52(5): p. 686–697. [DOI] [PubMed] [Google Scholar]
- 43.Mitchell SL, Kiely DK, Miller SC, Connor SR, Spence C and Teno JM, Hospice care for patients with dementia. Journal of pain and symptom management, 2007. 34(1): p. 7–16. [DOI] [PubMed] [Google Scholar]
- 44.Mitchell SL, Kiely DK, Hamel MB, Park PS, Morris JN and Fries BE, Estimating prognosis for nursing home residents with advanced dementia. Jama, 2004. 291(22): p. 2734–2740. [DOI] [PubMed] [Google Scholar]
- 45.Van der Steen JT, Radbruch L, Hertogh CMPM, et al. , White paper defining optimal palliative care in older people with dementia: a Delphi study and recommendations from the European Association for Palliative Care. Palliative medicine, 2014. 28(3): p. 197–209. [DOI] [PubMed] [Google Scholar]
- 46.Harrison KL, Ritchie CS, Patel K, et al. , Care settings and clinical characteristics of older adults with moderately severe dementia. Journal of the American Geriatrics Society, 2019. 67(9): p. 1907–1912. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Reckrey JM, Morrison RS, Boerner K, et al. , Living in the Community With Dementia: Who Receives Paid Care? Journal of the American Geriatrics Society, 2020. 68(1): p. 186–191. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Schulz R, Mendelsohn AB, Haley WE, et al. , End-of-life care and the effects of bereavement on family caregivers of persons with dementia. New England Journal of Medicine, 2003. 349(20): p. 1936–1942. [DOI] [PubMed] [Google Scholar]
- 49.Patel KV, Guralnik JM, Dansie EJ and Turk DC, Prevalence and impact of pain among older adults in the United States: findings from the 2011 National Health and Aging Trends Study. Pain®, 2013. 154(12): p. 2649–2657. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Singer AE, Meeker D, Teno JM, Lynn J, Lunney JR and Lorenz KA, Symptom trends in the last year of life from 1998 to 2010: a cohort study. Annals of internal medicine, 2015. 162(3): p. 175–183. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplemental Table 1: Hospice length of stay by disease type