
Figure 4.
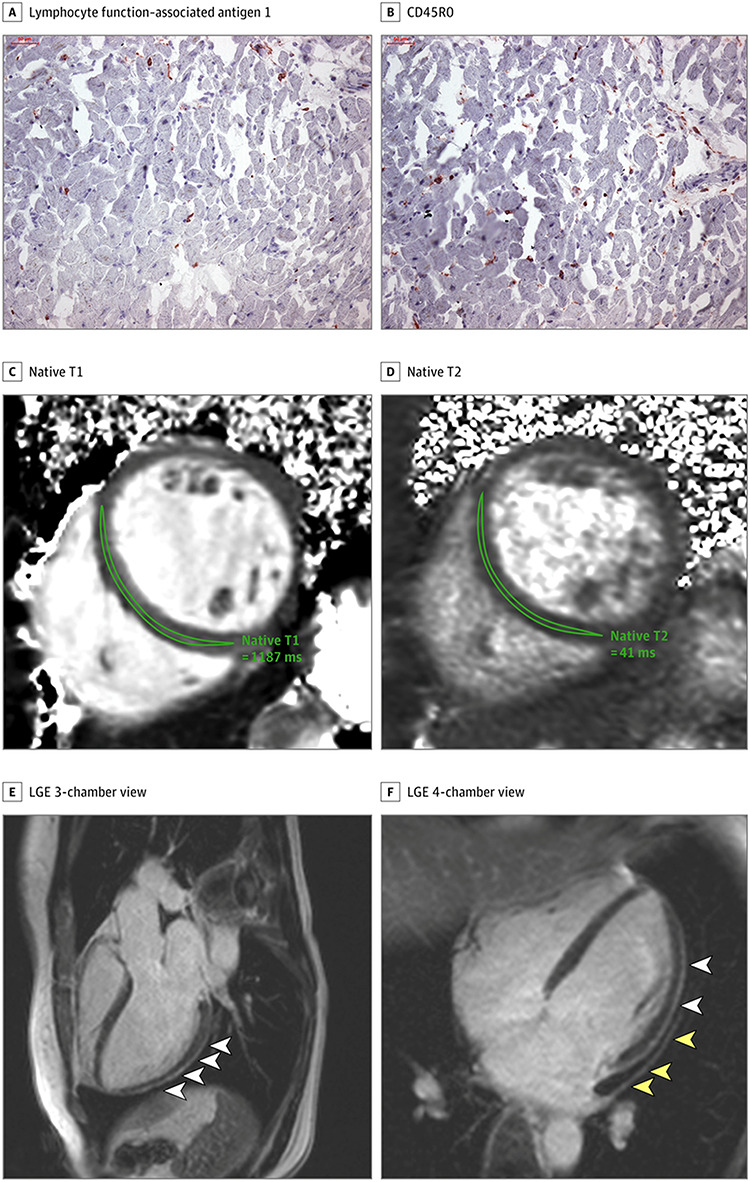
A and B, Histologic findings in an adult man with severe CMR imaging abnormalities 67 days after COVID-19 diagnosis. High-sensitivity troponin T level on the day of CMR imaging was 16.7 pg/ml. The patient recovered at home from COVID-19 illness with minimal symptoms, which included loss of smell and taste and only mildly increased temperature lasting 2 days. There were no known previous conditions or regular medication use. Histology revealed intracellular oedema as enlarged cardiomyocytes with no evidence of interstitial or replacement fibrosis. Panels A and B show immunohistochemical staining, which revealed acute lymphocytic infiltration (lymphocyte function–associated antigen 1 and activated lymphocyte T antigen CD45R0) as well as activated intercellular adhesion molecule 1. C–F, Representative CMR images of an adult woman with COVID-19–related perimyocarditis. Panels C and D show significantly raised native T1 and native T2 in myocardial mapping acquisitions. Panels E and F show pericardial effusion and enhancement (yellow arrowheads) and epicardial and intramyocardial enhancement (white arrowheads) in LGE acquisition. Image reproduced from Puntmann et al. [10] under the terms of the CC-BY License