
FIGURE 3.
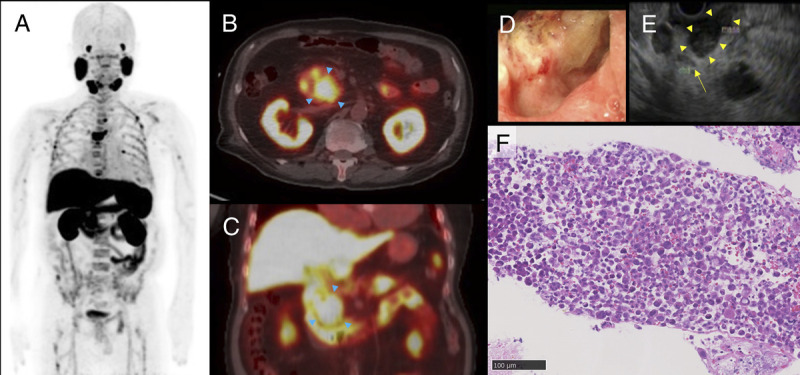
Six weeks later, to evaluate the state of metastatic castration-resistant prostate carcinoma and the duodenal tumor (PSA 0.02 ng/mL), he underwent 18F-PSMA-1007 PET/CT followed by endoscopic ultrasound (EUS)–guided fine-needle aspiration. Maximum intensity projection image (A), the axial and coronal fused PET/CT images (B, C), the endoscopic image (D), and the EUS image (E) are shown. 18F-PSMA-1007 PET/CT revealed abnormal uptake in the T5 bone metastasis (SUVmax, 33.55) and the duodenal tumor (SUVmax, 16.55), as well as physiological uptake in the hepatobiliary and intestinal tract. According to the EUS findings (E), the common bile duct (arrow) was located away from the duodenal tumor (arrowheads), indicating that the latter did not originate from the bile duct or pancreas. Histological examination revealed duodenal adenocarcinoma (F: hematoxylin-eosin stain microphotograph) negative for PSA on immunohistochemistry (not shown). As previously reported, some tumors other than prostate cancer can be positive on PSMA PET, such as brain metastases from breast cancer, glioblastoma recurrence, thyroid adenoma, and other benign lesions.10–13 When we find high uptake of 18F-PSMA-1007 in an isolated rapidly growing tumor, we should pay attention to the possibility of mimicking metastasis from prostate cancer.