

Abstract
Background
In COPD patients it is very important to assess the activities of daily living (ADL) due to an impairment of independence and quality of life. There is a lack of retrievable data regarding the cardio-pulmonary response to Londrina ADL protocol in patients with COPD. The aim of the present study was to assess the cardio-pulmonary response to Londrina ADL protocol in patients with COPD and to compare this with responses to the Glittre ADL test.
Methods
This cross-sectional study was done on 30 COPD subjects. Each subject was taken to perform the Londrina ADL protocol, Glittre ADL test, twice each, on subsequent days. The Londrina ADL protocol comprises 5 activities representing ADL, involving upper limbs, lower limbs, and trunk movements. The Glittre ADL test consists of completing a circuit while carrying a weighted backpack (2.5 kg for women, 5.0 kg for men). The better value of the two was taken into consideration. For the Londrina ADL protocol and Glittre ADL test the outcome of primary interest was time and for the six-minute walk test was the distance walked. The secondary outcomes for all tests were heart rate, systolic blood pressure, diastolic blood pressure, respiratory rate, saturation of oxygen in blood and dyspnea.
Results
The COPD subjects of age group 63.27±11.07 years took 5.94±0.36 min to complete trial 2 of the Londrina ADL protocol. Significant physiological increases in heart rate (p≤0.01), respiratory rate (p≤0.01), blood pressure (p≤0.01) and severity of dyspnea (p≤0.01) were observed, whereas saturation of oxygen in blood (p≤0.01) was reduced at the end of the Londrina ADL protocol and Glittre ADL test. There was a positive, non-significant correlation between the six-minute walk test distance and the Londrina ADL protocol time (r=0.236) (p=0.209). A positive, not significant correlation was observed between the Glittre ADL test (time) and the Londrina ADL protocol (time) (r=0.194) (p=0.304) and a negative but not significant correlation between the six-minute walk test (distance) and the Glittre ADL test (time) (r= -0.184) (p=0.330).
Conclusion
The Londrina ADL protocol can be used as an assessment tool for the evaluation of functional performance and activities of daily living in COPD along with other test protocols in pulmonary rehabilitation.
Key words: Activities of daily living (ADL), cardiopulmonary response, Londrina ADL protocol, Glittre ADL test, functional performance, COPD
Introduction
Chronic obstructive pulmonary disease is a preventable and treatable disease characterized by thelimitation in airflow and persistent respiratory symptoms [1]. People with chronic obstructive disease also present extra- pulmonary features such as systemic inflammation, increased oxidative stress, nutritional impairments and skeletal muscle dysfunction [2], leading to a reduction in the exercise capacity and physical activity [3]. As a result of these pulmonary and extrapulmonary manifestations, symptoms like dyspnea and fatigue are common. These symptoms make people with COPD feel uncomfortable and they are often discouraged to perform their daily physical activities [1,3].
The activities of daily living (ADL) are affected in COPD patients due to the weakness of skeletal muscles. The six-minute walk test (6MWT) is routinely used to assess exercise intolerance, which may not be a true indicator of limitation of activities of daily living. The assessment of activities of daily living and the study of the cardiopulmonary responses during the assessment, may help in planning an appropriate rehabilitation program for the COPD patients. Exercise intolerance is commonly observed in patients with chronic obstructive pulmonary disease, which hampers the capacity to perform day-to-day activities and contributes to reduction in functional capacity [4]. The reduction in exercise capacity can be due to many factors such as inefficient gas exchange, airflow limitation, changes in metabolism and the composition of peripheral musculature, peripheral muscle weakness, and abnormal oxygen transport in the exercising muscle [5].
Limitations in ADLs and functional capacity are better predicted by clinical field tests, instead of tests which focus on isolated components of function [4]. The ability to perform activities of daily living (ADL), is better predicted by an integrative test rather than by tests focused on a single component of functional activities [3]. The 6MWT has been widely used for evaluating an individual’s functional capacity [5]. However, the limitation is that it takes into consideration only the walking function and does not include other activities involving the upper limbs [6].
Among the tests which were proposed to evaluate ADL activities was the Glittre ADL test. It involves activities other than walking, such as ascending and descending steps, sitting and rising from a chair, and arm movements while carrying weights. Thus, it appears to be a better and more appropriate option than the 6MWT for evaluating an individual’s functional capacity [4]. However, the activities included in the Glittre ADL test do not mimic the actual functional tasks performed in day-to-day life, which may be affected in people with COPD [7]. Another option to assess functional capacity is to use questionnaires. A few questionnaires like the Modified Pulmonary Functional Status and Dyspnea Questionnaire (PFSDQM) and the London chest activity of daily living questionnaire (LCADL) are commonly used in clinical settings and report the degree of symptoms and the perception of ADL performance of the patients [7]. However, psychological or cognitive factors might play a vital role in an individual’s response to such questionnaires [8]. Considering the limitations of the available tools used to assess ADL, a new protocol named the Londrina ADL was developed by a research group from the State University of Londrina, Brazil and represents the subject’s real life and performance of day-to-day ADL activities. A few studies have attempted to assess the ADL’s objectively by using functional tests. However, they do not include a range of specific ADL like tasks that would represent life. So, there has been a growing interest in the objective assessment of the ADL performance through performance-based protocols which encompass activities that people perform daily [9,10].
There is a lack of retrievable data regarding the cardio-pulmonary response to Londrina activities daily of living protocol in patients with chronic obstructive pulmonary disease. The study of cardiopulmonary response during the ADL assessment tests was not studied earlier. It is not well known whether these ADL tests can lead to accelerated cardiopulmonary responses in COPD patients during the test procedure. The aim of the study is to investigate the cardiopulmonary response induced by the Londrina activities of daily living protocol in patients with chronic obstructive pulmonary disease and compare it with the response elicited by the 6MWT and Glittre ADL test.
Methods
Study population
Patients with mild and moderate chronic obstructive pulmonary disease, according to the GOLD criteria, 2019 and referred by a physician or pulmonologist [1].
Sample size
The sample size was calculated based on a pilot study consisting of Londrina activities of daily living (15 subjects) with an anticipated increase in heart rate of 90% after the protocol, using the following formula:
| n = 4pq/d2 |
where p=0.9; q=1-p; d=15% of 90, with 15% relative precision, 95% CI, and adding 20% non-response error. Sample size = 30.
Inclusion criteria
Patients with mild and moderate chronic obstructive pulmonary disease according to the GOLD criteria, 2019 and referred by a physician.
Exclusion criteria
Criteria for exclusion were: long term oxygen therapy; patients with acute exacerbation of chronic obstructive pulmonary disease; patients with unstable hemodynamic parameters: systolic blood pressure< 100 mmHg, <60 mmHg for diastolic blood pressure and mean arterial pressure (MAP) <80mmHg); any condition other than COPD that could compromise the patient’s ability to perform the tests.
Materials
Londrina activities of daily living protocol: Table (120 cm ×60 cm); objects: (4 objects of 250 g, 4 objects of 500 g, 2 objects of 1 kg and 2 objects of 2 kg); basket, 10 items of clothing (80-442 g), 2 bags with 10% of the subject’s body weight i.e. 5 % in each bag.
Glittre activities of daily living test: Stepper (17 cm high×27 cm deep each step); bag pack (2.5 kg for female, 5 kg for male).
Study procedure
The study protocol was submitted for approval to the scientific committee and research- ethics committee. The study was approved by the Kasturba medical college Mangalore, Institutional Ethics Committee (IEC KMC MLR 11-17/229). The subjects were then recruited between August 2018 to September 2019. The study was explained to the subjects (patients) with mild and moderate COPD, who were referred to the Department of Physiotherapy, and after signing a written consent form, willing participants were screened for the inclusion and exclusion criteria.
Pulmonary function and anthropometric parameters were assessed for all subjects. Before starting with the protocols, each protocol was demonstrated. All the subjects underwent three tests, twice each on subsequent days [11]. The tests included the Londrina activities of daily living protocol, the Glittre activities of daily living test and the 6MWT. The clinical trial registration number assigned was CTRI/2018/ 12/016738 (http://ctri.nic.in/Clinicaltrials/pdf_generate. php?trialid= 29941&EncHid=89791.92680&modid=1&compid=19%27,%27 29941det%27).
Description of Londrina activities of daily living protocol
Five activities are included in the Londrina ADL protocol, activities that involve the upper limbs, lower limbs, and trunk flexion/inclination/ rotation, which can be fully and realistically performed, without pretending or simulating. Also, all the activities included are relatively simple to organize from the logistical point of view [7].
Activities of daily living: The Londrina protocol is composed of 5 activities organized at 5 stations inside a room (6.5×5.1 m).
Objects on the table: The subject sits on a chair in front of a table (120 cm × 60 cm), with a line separating it into 2 halves. The table has 10 objects on it (4 of 250 g, 4 of 500 g, 2 of 1 kg), all on the left side. The subject takes the objects one by one, with both hands and puts them all on the right side and then again on the left side of the table [8,11]. There is no standardized order for object positioning and this activity represents activities that involve upper-limb movements in the sitting position [7].
Walking with bags: The subject walks over a 6 m line, 3 consecutive times carrying 2 bags (of 10% body weight with 5% in each bag), one in each hand [8,11]. This activity represents activities that involve carrying loads while walking, inside home or in the street [7].
Shelves: The subject stands in front of 4 shelves, one above the other (distance between the floor and first shelf, 42 cm; distance between one shelf and the next, 45 cm), with a table next to them. On the table there are 12 objects (4 of 250 g, 4 of 500 g, 2 of 1 kg, 2 of 2 kg). The subject takes the objects, one at a time, and puts them on the shelves (without a predetermined order). The subject organizes the objects on the shelves in such a way that there are 3 objects on each shelf. When all the objects are placed on the shelves, the subject returns them in the same way to the table [8,11]. This activity represents the unsupported upper-limb activities associated with trunk movement in the standing position [7].
Clothesline: The subject stands in front of a clothesline positioned at eye-level. A basket containing 10 items of clothing (80-442 kg) is kept on the ground, next to the subject. The subject picks up each item one by one and hangs it on the clothesline. After hanging all the items, the subject puts them back in the basket, one at a time [8,11]. Small variations in the clothes weight are allowed. This activity represents unsupported upper-limb activities in the standing position, with more intense trunk movements and, eventually, squatting [7].
Walking: The subject then walks back and forth again on the same 6m line described above. At the end of the test, the time taken to complete it is calculated using a stopwatch [8,11].
The instructions given to the subjects were: “Perform these activities as if you were doing them at home, at your usual day-by-day pace. You are allowed to stop to rest if you feel it is necessary.” After completing one activity, the subject was reminded of the next one; however, no encouragement was given during the protocol [7].
Before beginning the protocol, the evaluator demonstrated the activities one by one. BP (blood pressure), HR (heart rate), RR (respiratory rate), oxygen saturation (SPO2) and sensation of dyspnea (Mod Borg scale) were measured at the beginning and immediately after the test. The Londrina protocol was performed twice on subsequent days and the best value was taken [8,11].
Description of the Glittre activities of daily living test
The Glittre test is a protocol developed to assess functional status in patients with COPD [7]. It consists of a 10m circuit where the subject is instructed to perform the following activities: the individual is instructed to stand up from a sitting position with a backpack (2.5 kg for a female and 5 kg for a male), walk along a flat 10 m long course, in the middle of which at 5 m, is a 2-step stepper to be traversed. The subject then stands facing 3 shelves containing 3 objects on the first shelf. The subject moves each object one by one from the first shelf (at shoulder height) to the bottom shelf (waist height) and then back to the floor. The objects are then returned one by one to the bottom shelf and the top shelf, afterwards the subject walks back along the circuit, climbing and descending the stairs, until he/she reaches the starting point. The subject wears a weighted backpack, throughout the test [10].
Subjects were instructed to complete 5 laps ‘as fast as’ possible. At the end of the test the time taken to complete the test was calculated using a stopwatch. Subjects were instructed to perform the activities at their usual pace. Before beginning the protocol, the evaluator demonstrated the activities one by one. BP (blood pressure), RR (respiratory rate), HR (heart rate), sensation of dyspnea (Mod Borg scale) and SpO2 (oxygen saturation) were measured at the beginning and immediately after the test. The Glittre ADL test was performed twice each, on subsequent days [10,11]. No verbal incentive was offered during the test [4].
Description of six-minute walk test
The six-minute walk test is a test that reflects ADL using only horizontal displacement on a level surface [4]. It was performed according to the guidelines of the American Thoracic Society. Subjects were instructed to walk ‘as far as’ possible along a 30-meter corridor for 6 min, with the aim of achieving their maximum possible walking distance in 6 min. Standardized instructions were provided each minute. Subjects were permitted to stop and rest if required but were encouraged to continue walking as soon as they were able to. Blood pressure (BP), heart rate (HR), respiratory rate (RR), oxygen saturation (SpO2) and sensation of dyspnea (Mod Borg scale) were measured at the beginning and immediately after the test. The outcome of the test was the covered distance. The 6MWT was performed twice, on subsequent days [5,11].
Statistical analysis
Data was analyzed using IBM SPSS Statistics for Windows, ver. 25.0. Armonk, IBM Corp. The Shapiro-Wilk test was used for testing the normality of the data. Differences in the cardio-pulmonary response before and after the performance of each test were compared using paired sample t-test. The cardio-pulmonary response elicited by one test was compared with the other two, using the ANOVA test. The Karl Pearson coefficient was used to correlate variables of the Londrina activities of daily living protocol and those between the tests.
Results
A total of 35 subjects who matched the inclusion criteria of the study were selected, out of which 30 subjects were included and 5 excluded. The reasons for exclusion were as follows: 2 had a fear of falling, 2 had giddiness during the performance of the test and 1 was discharged after performing the 6MWT. Table 1 summarizes the anthropometric measures and baseline data of the 30 COPD subjects, while Table 2 shows the post-cardiopulmonary response of trial 1 and 2 of the Londrina Activities of daily living protocol in patients with COPD and a statistically significant difference was seen in between the two trials for time (p=0.04). The cardio-pulmonary response to Londrina ADL protocol during both the trials did not differ in respiratory rate, systolic blood pressure, diastolic blood pressure, SpO2 and Borg dyspnea (all p≥0.05) but showed a statistically significant difference in the time taken to complete both the trials (p≤0.05) and in the heart rate (p=0.02), across the two trials. On average, subjects spent 6.03±0.32 s and 5.94±0.36 s to perform the first and second Londrina ADL protocols, respectively (p≤0.05). There was a reduction of 0.08 s in the second trial of Londrina ADL protocol. Table 3 shows the postcardiopulmonary response to trials 1 and 2 of Glittre ADL test in COPD subjects and no significant difference was seen between them. Table 4 shows the post-cardiopulmonary response to trials 1 and 2 of 6MWT in patients with COPD and the subjects showed a significant and highly significant difference in the heart rate (p=0.03) and distance (p≤0.01) respectively, across the two trials.
Figure 1 shows a moderate positive correlation between trial 1 (time) and trial 2 (time) of Londrina ADL protocol (r=0.789; p≤0.01). Table 5 summarizes the pre-post physiological response to the 6MWT, the Glittre ADL test and the Londrina ADL protocol in COPD subjects. The COPD subjects took 5.13±0.32 s to complete Glittre ADL test, 5.94±0.36 s to complete Londrina ADL protocol and walked a distance of 288.57±23.23 meters during the 6MWT. Heart rate behavior was similar during the 6MWT (p≤0.01), Glittre ADL test (p≤0.01) and Londrina ADL protocol (p≤0.01), demonstrating a physiological increase. There was a significant increase in RR during the 6MWT (p≤0.01), Glittre ADL test (p≤0.01) and Londrina ADL protocol (p≤0.01). The COPD subjects showed a significant decrease in SpO2 during the 6MWT (p≤0.01), Glittre ADL test (p≤0.01) and Londrina ADL protocol (p≤0.01). The subjects also showed a significant increase in diastolic blood pressure during the 6MWT (p≤0.01), Glittre ADL test (p≤0.01) and Londrina ADL protocol (p<0.01). A significant physiological increase in systolic blood pressure and Borg dyspnea was seen during the Glittre ADL test (p≤0.01) and Londrina ADL protocol (p≤0.01), except during the 6MWT (p=0.16, p=1.00). Figure 2 shows no significant correlation between the 6MWT distance and the Londrina ADL protocol time (r=0.236, p=0.209). Figure 3 shows no significant correlation between the Glittre ADL (time) and the Londrina ADL protocol (time) (r=0.194, p=0.304). Figure 4 shows no significant correlation between the 6MWT (distance) and the Glittre ADL test (time) (r= -0.184, p=0.330).
Table 1.
Demographic characteristics of COPD subjects.
| Characteristics | COPD (n=30) (mean ± SD) |
|---|---|
| Age (years) | 63.27±11.07 |
| Gender (n) M:F | 19:11 |
| Height (meters) | 1.57±0.08 |
| Weigh t(kg) | 59.56±7.42 |
| BMI (kg/m2) | 23.81±3.33 |
| Pulmonary function test | |
| Forced expiratory volume/forced vital capacity | 61.37±5.76 |
| Forced expiratory volume (L) | 1.25±0.64 |
| Forced vital capacity (L) | 1.99±0.40 |
| Heart rate | 86.26±10.48 |
| Respiratory rate | 16.83±5.25 |
| Systolic blood pressure | 127.73±8.25 |
| Diastolic blood pressure | 84.47±8.13 |
| Saturation of oxygen | 94.73±1.74 |
| Borg dyspnea | 0.03±0.18 |
| COPD severity | |
| Mild | 10 |
| Moderate | 20 |
Table 2.
Post-cardiopulmonary response to trials 1 and 2 of Londrina activities of daily living protocol in patients with COPD.
| Variables | Londrina ADL Trial 1 | Londrina ADL Trial 2 | R | Mean diff (i-j) | p |
|---|---|---|---|---|---|
| (mean± SD) (i) | (mean± SD) (j) | ||||
| Heart rate | 99.47±12.71 | 97.23±12.32 | 0.916 | +2.24 | 0.02 |
| Respiratory rate | 24.33±4.4 | 24.90±4.17 | 0.859 | +0.57 | 0.18 |
| Systolic blood pressure | 133.47±8.3 | 131.60±7.21 | 0.738 | -1.87 | 0.08 |
| Diastolic blood pressure | 90.20±9.58 | 88.77±9.43 | 0.791 | -1.43 | 0.21 |
| SpO2 | 89.03±2.94 | 89.40±2.68 | 0.792 | +0.37 | 0.28 |
| Borg dyspnea | 1.60±0.55 | 1.60±0.56 | 1.000 | 0.00 | 0.97 |
| Time | 6.03±0.32 | 5.94±0.36 | 0.789 | 0.08 | 0.04 |
Table 3.
Post-cardiopulmonary response to trials 1 and 2 of Glittre activities of daily living protocol in patients with COPD.
| Variables | Glittre ADL test Trial 1 | Glittre ADL test Trial 2 | Mean difference (i-j) | p |
|---|---|---|---|---|
| mean±SD (i) | mean±SD (j) | |||
| Heart rate | 96.60±12.96 | 96.13±12.11 | -0.46 | 0.63 |
| Respiratory rate | 27.10±11.69 | 24.17±4.25 | -2.93 | 0.17 |
| Systolic blood pressure | 134.33±7.93 | 133.33±6.44 | -1.00 | 0.29 |
| Diastolic blood pressure | 90.00±9.81 | 90.00±10.03 | 0.00 | 1.00 |
| SpO2 | 89.27±3.59 | 89.83±3.20 | 0.56 | 0.12 |
| Borg dyspnea | 1.83±0.53 | 1.80±0.55 | 0.03 | 0.83 |
| Time | 5.22±0.10 | 5.13±0.32 | 0.09 | 0.05 |
Table 4.
Post-cardiopulmonary response to trials 1 and 2 in six-minute walk test in patients with COPD.
| Variables | Six-minute walk test Trial 1 | Six-minute walk test Trial 2 | Mean difference (i-j) | p |
|---|---|---|---|---|
| mean±SD (i) | mean±SD (j) | |||
| Heart rate | 89.17±11.11 | 91.63±9.51 | 2.46 | 0.03 |
| Respiratory rate | 20.10±4.56 | 21.86±3.71 | -0.76 | 0.55 |
| Systolic blood pressure | 130.60±7.79 | 130.07±9.28 | 0.53 | 0.83 |
| Diastolic blood pressure | 88.03±7.56 | 88.56±7.75 | -0.53 | 0.18 |
| SpO2 | 90.33±1.86 | 90.83±2.12 | 0.50 | 0.81 |
| Borg dyspnea | 0.03±0.20 | 0.03±0.19 | 0.00 | 1.00 |
| Distance | 317.67±62.73 | 288.57±23.23 | 29.10 | <0.01 |
Table 5.
Pre- and post-cardiopulmonary response to six-minute walk test, Glittre ADL test and Londrina ADL protocol in patients with COPD.
| Variables | Pre- six-minute walk test (mean SD) |
Post- six-minute walk test (mean±SD) |
p | Pre- Glittre ADL (mean±SD) |
Post- Glittre ADL (mean±SD) |
p | Pre-Londrina ADL (mean±SD) |
Post-Londrina ADL (mean±SD) |
p |
|---|---|---|---|---|---|---|---|---|---|
| Heart rate | 86.26±10.48 | 91.63±9.51 | <0.01 | 85.00±13.37 | 96.13±12.11 | <0.01 | 86.57±13.37 | 97.23±12.32 | <0.01 |
| Respiratory rate | 16.83±5.25 | 21.86±3.71 | <0.01 | 16.70±5.10 | 24.17±4.25 | <0.01 | 15.93±4.47 | 24.90±4.17 | <0.01 |
| SpO2 | 94.73±1.74 | 90.83±2.12 | <0.01 | 94.93±2.52 | 89.83±3.20 | <0.01 | 94.67±1.63 | 89.40±2.68 | <0.01 |
| Systolic blood pressure | 127.73±8.25 | 130.07±9.28 | 0.16 | 125.60±7.23 | 133.33±6.44 | <0.01 | 124.27±7.87 | 131.60±7.21 | <0.01 |
| Diastolic blood pressure | 84.47±8.13 | 88.56±7.75 | <0.01 | 82.47± 9.81 | 90.00±10.03 | <0.01 | 82.93±8.28 | 88.77±9.43 | <0.01 |
| Borg dyspnea | 0.03±0.18 | 0.03±0.19 | 1.00 | 0.07±0.25 | 1.80±0.55 | <0.01 | 0.07±0.25 | 1.60±0.56 | <0.01 |
| Time (minutes) | - | - | 5.13±0.32 | 5.94±0.36 | |||||
| Distance (meters) | - | 288.57±23.23 | - | - |
Figure 1.
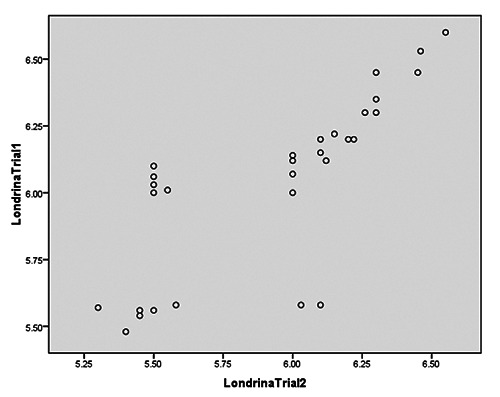
Correlation between Trial 1 (time) and Trial 2 (time) of Londrina ADL protocol.
Figure 2.

Correlation between six-minute walk test (distance) and Londrina ADL protocol (time).
Figure 3.
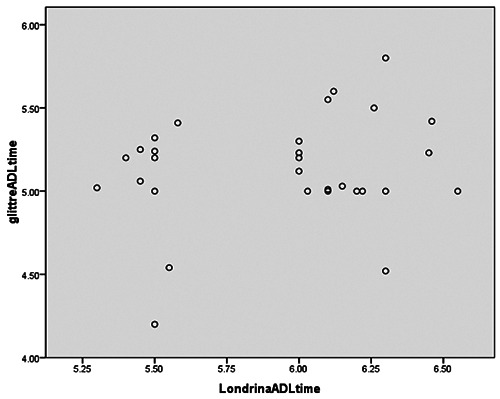
Correlation between Glitter ADL test and Londrina ADL protocol (time).
Figure 4.

Correlation between six-minute-walk test (distance) and Glittre ADL test (time).
Discussion
We investigated the cardiopulmonary response to the Londrina ADL protocol in 30 COPD subjects and compared the same with the response to the 6MWT and the Glittre ADL test. In our study, the COPD subjects took 6.03±0.32 min to complete trial 1 and 5.94±0.36 min to complete trial 2 of the Londrina ADL protocol with a difference of 0.08 s between the two trials. A similar study by Sant’Anna et al. on COPD subjects showed that the subjects spent 6.3 min to perform the first trial and 6.2 min to perform the second trial of the Londrina ADL protocol (a difference of 0.1 min) [7]. This result can be attributed to a learning effect seen with the second attempt. In another study done by Paes et al. on a healthy population, subjects in the age group ranging from 50-59 years spent 5.06±0.85 min and subjects in the age group 60-69 years spent 5.53±0.93 min to complete trial 2 [8].The possible reasons for the longer duration taken by COPD subjects could be the higher rate of work and the fatigue of the respiratory muscles due to progressive airflow limitation and loading of upper extremity muscles which compromise blood flow to postural and gait musculature. This in turn contributes to an increase in metabolic demand and slows down the gait speed [6]. The Londrina ADL protocol includes activities that involve both the upper and lower limbs (walking, sitting and standing, walking with bags, turning around) requiring abilities such as balance, mobility and muscle strength [8]. It has been observed that 20% of the variability of the time spent to perform the Londrina ADL protocol is explained by age, as with aging a decrease is seen in the muscle strength, mobility and balance, which contributes to the impairment of performance of ADL [8]. Extrapulmonary features such as the abnormalities of skeletal muscles caused by inflammation, alterations in exchange of gases, electrolyte imbalance, inactivity in addition to respiratory tract involvement, negatively affect the performance [12].
Our study showed a statistically significant physiological change in heart rate, respiratory rate, systolic blood pressure, diastolic blood pressure, saturation of oxygen and Borg scale after the 6MWT, the Glittre ADL test and the Londrina ADL protocol. The possible explanation behind a significant physiological response to the Glittre ADL test and the Londrina ADL protocol; and milder response to the 6MWT is probably due to involvement of upper extremity activities during both ADL tests, whereas 6MWT involves only lower limb performance. This is because unsupported arm work leads to active contribution of the accessory respiratory muscles for postural support of the arms and torso which may decrease their effective contribution to ventilation, which may in turn place a great burden on the diaphragm leading to early fatigue. This leads to dyssynchronous-thoracoabdominal breathing movements which are associated with the onset of severe dyspnea leading to early termination of exercise at low work levels [13].
A study carried out by Cavalheri et al. [14] on COPD subjects using the Glittre ADL test showed that ADL activities like climbing up and down stairs generate a higher energy expenditure than walking does, causing more dyspnea and fatigue. Activities like shifting objects on and off a shelf without the arms supported, require the lowest energy expenditure [14]. However, a pilot study done by Karloh et al. showed that nearly 50-65% of one lap of the Glittre ADL test was spent in moving objects on and off the shelf without support to the hands, due to which the metabolic demand increased [6]. A previous study by Velloso et al. demonstrated that a huge portion of the ventilatory reserve in patients with chronic obstructive pulmonary disease is used during ADLs, causing ventilatory limitation in their functional and exercise capacity [15]. Another study done by Gulrat et al. [16] measured the physiological responses of multiple tasks which are included in the Glittre ADL test and found out that Glittre walking and Glittre shelf exercises resulted in similar workloads.
There was no significant correlation observed between the 6MWT (distance) and the Glittre ADL test (time), Londrina ADL protocol (time) and the 6MWT (distance). However, COPD subjects took more time to complete the Glittre ADL test and walked a shorter distance during the 6MWT than the healthy subjects. In these patients, ventilatory capacity and oxygen uptake dominate as exercise limiting factors and restrain most of the activities of daily living. Hyperinflation gives a lower inspiratory capacity, an increased work of ventilation and a dependency upon accessory respiratory muscles [16]. There is an increased risk of fall due to affected balance and poor coordination because of deconditioning and deteriorating muscle strength. The large variability in ADL time seen in COPD patients could be attributed to the above factors [17]. The findings of a study done by Corrȇa et al. on COPD subjects also showed a moderate negative correlation between the 6MWT (distance) and the Glittre ADL test (time) [4]. The Londrina ADL protocol and the Glittre ADL test, both involve more upper and lower limb activity whereas the 6MWT represents functional capacity and involves more of lower-limb activity. The Glittre ADL test stimulates the subjects to walk ‘as fast as’ possible (instructions given to the subjects) and the 6MWT instructs subjects to walk ‘as far as’ possible in six minutes, at the usual walking pace [8]. There is no significant correlation observed between the Glittre ADL test (time) and Londrina ADL protocol (time) which may be because the COPD subjects took more time than the healthy subjects to complete Glittre ADL test as well as Londrina ADL test. The possible reason could be the design of the tests and the fact that functional capacity is only one of the components necessary to perform ADLs. The Londrina ADL protocol is more representative of ADL performance than the Glittre ADL test and the 6MWT and can be more informative for clinical management than functional capacity alone [7].
Our study found a similar response between the Glittre ADL test, the 6MWT and the Londrina ADL protocol, thus the Londrina ADL protocol can be used as an assessment tool besides the Glittre ADL and the 6MWT for evaluation of functional performance and activities of daily living in subjects with chronic obstructive pulmonary disease.
Limitation of the study
COPD subjects who participated had a mild and moderate severity of the disease. The objects used in the protocols were not easily available in clinical settings and a large physical space was required to carry out the protocols. The Londrina ADL protocol took 5 min to be performed on an average, which was slightly longer than was required to perform other functional tests.
Conclusions
The Londrina ADL protocol induced a cardio- pulmonary response like that induced by the Glittre ADL test, whereas the responses were comparatively less with 6MWT in patients with chronic obstructive pulmonary disease. Both the tests used in ADL assessment caused a similar and significant increase in cardiopulmonary responses compared to the 6MWT, thus the Londrina ADL protocol may be used along with other test protocols, for a comprehensive assessment of COPD patients in pulmonary rehabilitation.
Abbreviations
- ADL
activities of daily living
- COPD
chronic obstructive pulmonary disease
- 6MWT
six-minute walk test.
Funding Statement
Funding: This study did not receive any grant from any external funding agency.
References
- 1.Vogelmeier C, Criner GJ, Martinez FJ, Anzueto A, Barnes PJ, Bourbeau J, et al. Global strategy for the diagnosis, management and prevention of chronic obstructive pulmonary disease 2017 Report: GOLD Executive Summary. Eur Respir J 2017;49:1700214. [DOI] [PubMed] [Google Scholar]
- 2.Maltais F, Decramer M, Casaburi R, Barreiro S, Burelle Y, Debigare R, et al. An official American Thoracic Society/European Respiratory Society statement: update on limb muscle dysfunction in chronic obstructive pulmonary disease. Am J Respir Crit Care Med 2014;189:15-62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Pitta F, Troosters T, Spruit MA, Probst VS, Decramer M, Gosselink R. Characteristics of physical activities of daily life in chronic obstructive pulmonary disease. Am J Respir Crit Care Med 2005;171:972-7. [DOI] [PubMed] [Google Scholar]
- 4.Corrȇa KS, Karloh M, Martins LQ, dos Santos K, Mayer AF. Can the Glittre ADL test differentiate the functional capacity of COPD patients from that of healthy subjects? Braz J Phys Ther 2011;15:467-73. [DOI] [PubMed] [Google Scholar]
- 5.ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: Guidelines for the six-minute walk test. Am J Respir Crit Care Med 2002;166:111–7. Erratum in: ATS Statement: Guidelines for the Six-Minute Walk Test. [No authors listed] Am J Respir Crit Care Med 2016;193: 1185. [DOI] [PubMed] [Google Scholar]
- 6.Karloh M, Karsten M, Pissaia FV, de Araujo CLP, Mayer AM. Physiological responses to the Glittre-ADL test in patients with chronic obstructive pulmonary disease. J Rehabil Med 2014;46:88-94. [DOI] [PubMed] [Google Scholar]
- 7.Sant'Anna T, Donaria L, Furlanetto KC, Morakami F, Rodrigues A, Grosskreutz T, et al. Development, validity and reliability of the Londrina activities of daily living protocol for subjects with COPD. Respir Care 2017;62:288-97. [DOI] [PubMed] [Google Scholar]
- 8.Paes T, Belo LF, da Silva DR, Morita AA, et al. Londrina activities of daily living protocol: reproducibility, validity, and reference values in physically independent adults age 50 years and older. Respir Care 2017;62(3):298-306. [DOI] [PubMed] [Google Scholar]
- 9.Paes T, Machado FV, Cavalheri V, Donaria L, Furlanetto KC, Sant'Anna T, et al. Multitask protocols to evaluate activities of daily living performance in people with COPD: a systematic review. Expert Rev Respir Med 2017;11(7):581-90. [DOI] [PubMed] [Google Scholar]
- 10.Jose A, Dal Corso S. Reproducibility of the six-minute walk test and Glittre ADL-test in patients hospitalized for acute and exacerbated chronic lung disease. Braz J Phys Ther 2015;19: 235-42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Hernandes NA, Wouters EFM, Meijer K, Annegarn J, Pitta F, Spruit MA. Reproducibility of 6-minute walking test in patients with COPD. Eur Respir J 2011;38:261-7. [DOI] [PubMed] [Google Scholar]
- 12.Ravoori H, Alaparthi GK, Krishnan KS, Anand R, Acharya V, Acharya P. Cardiorespiratory responses to Glittre ADL test in bronchiectasis: A cross- sectional study. Can Respir J 2018;2018:7470387. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Celli BR, Rassulo J, Make BJ. Dyssynchronous breathing during arm but not leg exercise in patients with chronic airflow obstruction. N Engl J Med 1986;314:1485-90. [DOI] [PubMed] [Google Scholar]
- 14.Cavalheri V, Donaria L, Ferreira T, Finatti M, Camillo CA, Ramos EMC, et al. Energy expenditure during daily activities as measured by two motion sensors in patients with COPD. Respir Med 2011;105:922-9. [DOI] [PubMed] [Google Scholar]
- 15.Velloso M, Stella SG, Cendon S, Silva AC, Jardim JR. Metabolic and ventilatory parameters of four activities of daily living accomplished with arms in COPD patients. Chest 2003;123:1047-53. [DOI] [PubMed] [Google Scholar]
- 16.Gulart AA, Munari AB, Tressoldi C, Dos Santos K, Karloh M, Flieg Mayer A. Glittre-ADL multiple tasks induce similar dynamic hyperinflation with different metabolic and ventilatory demands in patients with COPD. J Cardiopulm Rehabil Prev 2017;37:450-3. [DOI] [PubMed] [Google Scholar]
- 17.Skumlien S, Hagelund T, Bjortuft O, SkredeRyg M. A field test of functional status as performance of activities of daily living in COPD patients. Respir Med 2006;100:316-23. [DOI] [PubMed] [Google Scholar]