
Figure 1.
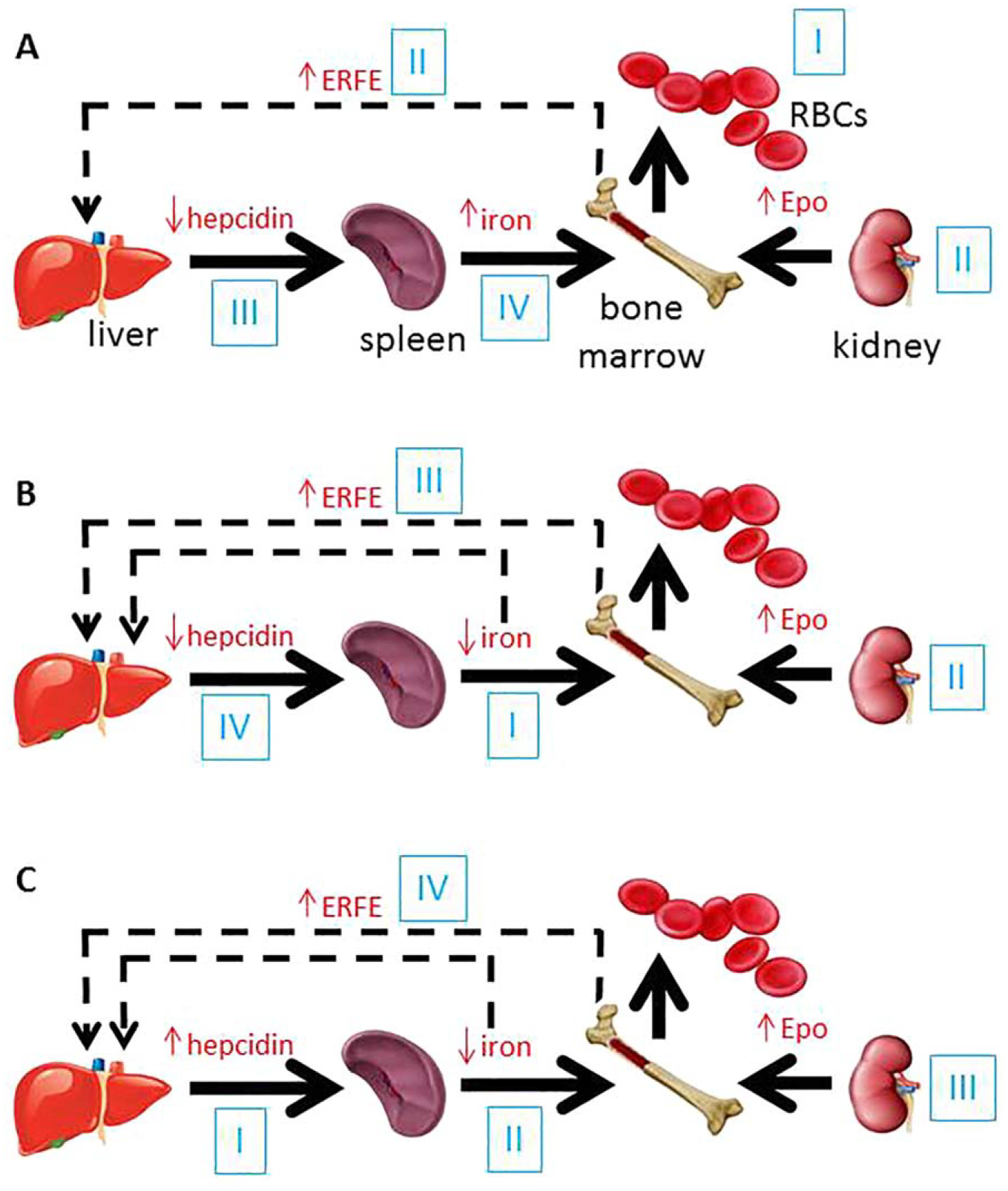
Proposed steps in the cross-talk between erythropoiesis and iron metabolism in conditions associated with iron dysregulation. (A) In acute blood loss (I), resultant hypoxia leads to increased erythropoietin (II) and consequent increase in erythroferrone (II) which suppresses hepcidin (III) and enables an increase in iron absorption and iron recycling, resulting in increased circulating iron (IV) available for erythropoiesis. (B) In iron deficiency anemia, decreased circulation iron concentration (I) leads to anemia and resultant hypoxia which results in increased erythropoietin (II) and subsequently increased erythroferrone (III), suppressing hepcidin (IV) to increase iron absorption and recycling. (C) In anemia of chronic inflammation, IL-6 driven increase in hepcidin (I) results in the sequestration of iron in macrophages, enterocytes, and hepatocytes, decreasing iron release into the circulation (II). As a consequence, iron restricted erythropoiesis and anemia result in compensatory increase in erythropoietin (III) and erythroferrone (IV), the later providing negative feedback to suppress hepcidin (RBCs = red blood cells; Epo = erythropoietin; ERFE = erythroferrone).