
Figure 2.
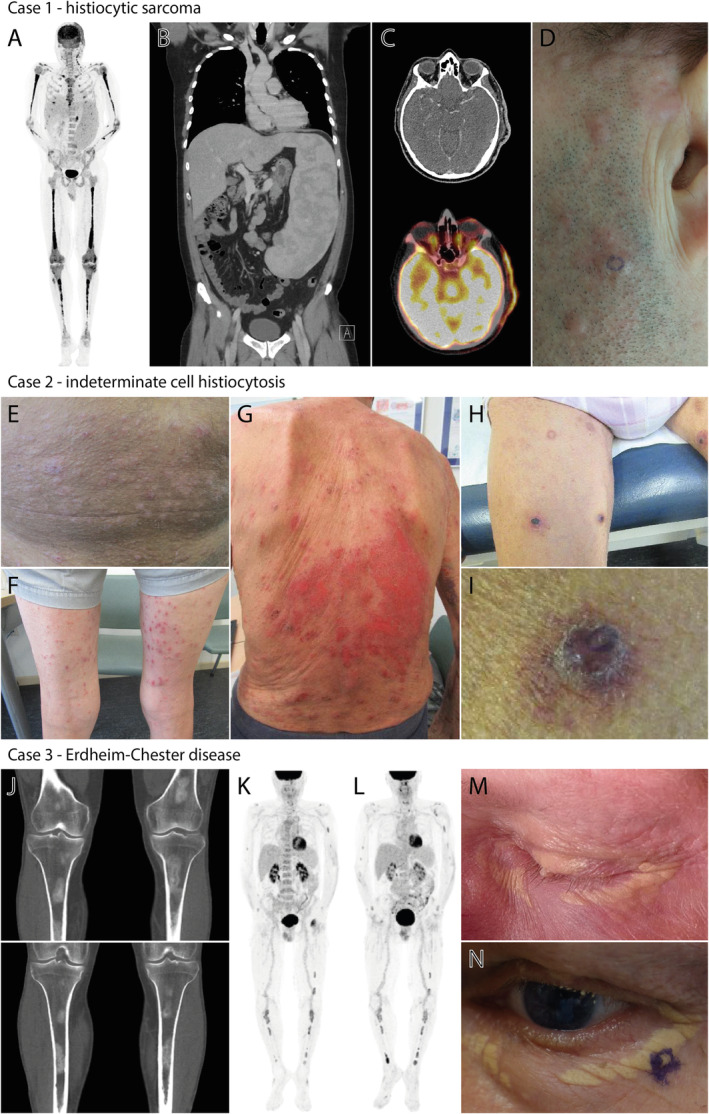
Clinical and radiological features of the patients described in this study. (A,B) Images of the PET‐CT scan made at diagnosis, showing FDG‐avid bone lesions and enlarged cervical lymph nodes, as well as extreme splenomegaly (29.5 cm) with diffuse moderately increased metabolism. (C,D) PET‐CT and clinical images of the pre‐auricular skin lesions. The localisation of the skin biopsy confirming the involvement of HS is encircled in panel (D). (E,F) Skin lesions on the abdomen and lower extremities at diagnosis. (G) Evidently progressed skin lesions at 7 months after initial diagnosis. (H–I) Recurrent skin lesions after treatment with topical corticosteroids and UV‐B phototherapy, with an altered phenotype of typical purple‐red papules. The localisation of the biopsy of one of these papules on the left upper leg is shown in panel (I). (J) Images of the CT‐scan performed at diagnosis, showing bilateral sclerotic femur and tibia lesions. (K) PET‐CT scan showing FDG uptake of ECD‐associated bone lesions after chemotherapy for the patient's multiple myeloma. (L) PET‐CT scan showing slightly increased FDG uptake of existing ECD bone lesions at diagnosis of acute myeloid leukaemia. (M) Peri‐orbital xanthelasma‐like lesions before myeloma‐directed chemotherapy. (N) Peri‐orbital xanthelasma‐like lesions after myeloma‐directed chemotherapy and autologous haematopoietic stem cell transplantation. The localisation of the skin biopsy confirming involvement of ECD is encircled.