

Abstract
Background:
Although research has demonstrated that depression and anxiety are associated with problematic executive function (EF), results are often inconsistent and underspecified. Delineating specific EF impairments in depression and anxiety has the potential to provide a mechanistic account of symptom presentation and course in these highly co-occurring disorders. The present study evaluated associations between components of EF and symptom dimensions of depression (depressed mood) and anxiety (anxious apprehension, anxious arousal) using factor analyses and structural equation modeling.
Methods:
Undergraduates (N = 1,123) completed self-report measures of EF in everyday life and of psychopathology. Based on a three-factor model (Miyake et al., 2000), item-level exploratory (n = 561) and confirmatory (n = 562) factor analyses were conducted on inhibition, shifting, and working memory scales chosen from the EF measure. Structural equation modeling tested the relationship of EF factors to dimensions of psychopathology using the total sample.
Results:
A three-factor model of EF best fit the data and was replicated via confirmatory factor analysis. Depressed mood and anxious arousal evidenced broad deficits across all EF domains, whereas anxious apprehension evidenced shifting disruptions.
Limitations:
Perceived EF may not index the same constructs as performance-based EF tests. Further, the present study was restricted to college students, warranting replication in other samples.
Conclusions:
Findings suggest that depressed mood and anxious arousal are characterized by a general disruption in the ability to maintain task goals, whereas anxious apprehension is characterized by cognitive inflexibility. EF impairments are likely contributory factors in the maintenance of affective disorders.
Keywords: executive function, affect, psychopathology, arousal, factor analysis, latent class analysis
Introduction
Depression and anxiety are the most prevalent and burdensome forms of psychopathology worldwide, costing between $47 and $210 billion per year in care and lost time (Greenberg et al., 2015; Kessler et al., 2015). Individuals with co-occurring depression and anxiety are more likely to experience severe and persistent symptoms and greater treatment resistance (Jakubovski & Bloch, 2014; Kessler et al., 2015; Saveanu et al., 2015). Their high comorbidity (up to 70%; Kessler et al., 2005) and recurrence rates suggest that there are specific factors that increase people’s risk for repeated episodes.
One probable but poorly understood domain of cognitive vulnerability is executive function (EF) and its relationship to symptom development, presentation, and course in depression and anxiety. Executive function refers to processes that regulate non-executive cognitive processes (e.g., motor responses) to flexibly guide behavior toward a goal, especially in novel situations (Banich, 2009). It is likely that the cognitive difficulties in attention and memory that are associated with depression and anxiety (e.g., difficulty concentrating and indecisiveness; APA, 2013) are driven in part by EF deficits (Snyder et al., 2015b). Supporting this view, research has demonstrated that depression is associated with impaired performance in specific domains of EF such as inhibition or termination of a pre-potent response (Bredemeier, Warren, Berenbaum, Miller, & Heller, 2016; Joormann & Gotlib, 2010) as well as shifting or alternating attention between tasks or mental sets (Austin et al., 2001; Bredemeier et al., 2016). Others have concluded that depression is associated with broad impairments in EF (for reviews, see Rock et al., 2014; Snyder, 2013). Research on anxiety-related EF impairment is less well developed. Evidence suggests deficits in working memory capacity (e.g., Eysenck, Payne, & Derakshan, 2005; Hayes, Hirsch, & Mathews, 2008; Moran, 2016), updating working memory (e.g., Snyder et al., 2015a), and shifting attention (Airaksinen, Larsson, & Forsell, 2005), though these findings are inconsistent (e.g., Castaneda et al., 2010; Snyder et al., 2015b).
Cognitive models of depression posit that deficits in controlling information in working memory maintain mood symptoms (see LeMoult & Gotlib, 2019, for a review). Specifically, difficulties inhibiting and updating negative information in working memory are thought to contribute to cognitive biases and maladaptive emotion regulation strategies (e.g., excessive rumination). A prominent theory in cognitive research proposes that anxiety impairs performance because it reduces attentional control in the presence of salient distracters (Berggren & Derakshan, 2012; Eysenck, Derakshan, Santos, & Calvo, 2007). According to Attentional Control Theory, anxiety is hypothesized to affect inhibition of task-irrelevant stimuli and shifting attention. Although Attentional Control Theory represented significant progress in that it targets specific EF components (unlike cognitive theories of depression), this theory does not distinguish among dimensions of anxiety. Anxiety is a heterogeneous construct, and it has been proposed that it is composed of anxious apprehension, or a propensity to engage in worry, and anxious arousal, a tendency to experience enduring patterns of hypervigilance and symptoms of intense fear and/or panic in response to relatively mild stressors (Sharp, Miller, & Heller, 2015). As anxious apprehension and anxious arousal are psychologically and physiologically distinct dimensions of anxiety that are associated with distinct neural mechanisms (see Sharp, Miller, & Heller, 2015, for a review), they should be characterized by different executive dysfunction profiles. The present study investigated EFs associated with specific dimensions of depression and anxiety by drawing upon an empirically supported theory of EF and utilizing a statistical framework that fosters systematic examination of executive impairment.
An Executive Function Framework
A significant problem in the study of EF has been conceptual in nature (Stuss & Alexander, 2000). EF is often difficult to define and is frequently framed or operationalized imprecisely (Martin & Failows, 2010). Despite these limitations, neuropsychological research supports distinguishing EFs (Miyake et al., 2000), although the exact decomposition remains a matter of debate. Given the variable definitions of EF, it is not surprising that inconsistent findings of EF integrity/impairment in psychopathology have emerged.
In an influential contribution, Miyake et al. (2000) used latent variable analysis to demonstrate that EF is multi-dimensional, parsing it into three separable but related fundamental domains: 1) shifting or alternating attention between tasks/mental sets, 2) updating of working memory representations, and 3) inhibition of dominant or prepotent responses (the latter reconceptualized as subsumed by a more general ability to maintain task goals; Miyake & Friedman, 2012). Although the component processes of shifting, updating, and inhibition are not intended to be an exhaustive list of executive processes, they are frequently identified in the literature as important EFs and are more circumscribed than some other executive processes (e.g., “planning”).
Shifting, updating, and inhibition are considered to act as control functions for working memory. Working memory is defined variously in the literature, with a common view that it covers both the focus of attention and the active representation and manipulation of context-specific information (Baddeley, 2003). Accordingly, the concept refers both to the contents of a particular type of memory and certain EF operations that work with that content. Working memory is a limited capacity system (Engle, Kane, & Tuholski, 1999) that relies on EF processes to effectively update and manage its contents (Friedman & Miyake, 2004). EFs allow relevant information to enter, block entrance of intrusive irrelevant material, and discard information that is no longer relevant (Engle et al., 1999). Given that the experience of negative mood states and negative life events activates mood-congruent representations in working memory (Siemer, 2005), the ability to control the contents of working memory could be crucial in understanding why some individuals more easily recover from negative affect, whereas others initiate and persist in using maladaptive emotion-regulation strategies that promote and maintain negative affect. Identifying specific EF impairments in specific dimensions of depression and anxiety has the potential to provide a novel, mechanistic account of such maladaptive patterns of behavior, as well as understanding emotion-regulation proclivities.
The Present Study
The present study drew upon on the Miyake et al. (2000) model to test contrasting hypotheses and findings regarding the nature of EF disruptions in depression and anxiety. We tested whether depression is best characterized by deficits that are specific to inhibition and updating (as suggested by cognitive and neurobiological frameworks; e.g., De Raedt & Koster, 2019; Joormann & Gotlib, 2010; LeMoult & Gotlib, 2010) and/or to shifting (as suggested by Austin et al., 2001), or that reflect a general EF deficit manifested across inhibition, shifting, and updating (Snyder, 2013). Similarly, we evaluated whether anxious apprehension and anxious arousal would result in inhibition and shifting deficits as predicted by Attentional Control Theory (Eysenck et al., 2007) or in updating deficits (e.g., Snyder et al., 2015a). It was hypothesized that depression would be associated with broad EF impairments, as affective neuroscience studies have demonstrated functional abnormalities across several prefrontal cortical regions associated with multiple EFs (e.g., Davidson, Pizzagalli, Nitschke, & Putnam, 2002; Zilverstand, Parvaz, & Goldstein, 2017). Based on neuroimaging evidence supporting distinct patterns of brain activity associated with individual differences in anxious apprehension and anxious arousal during an EF task (Engels et al., 2007; 2010; Warren et al., 2013; for a review, see Sharp et al., 2015), it was hypothesized that anxious apprehension (i.e., worry) would be associated with problems in shifting and that anxious arousal would be associated with broad EF impairments.
A challenge in assessing EF performance in the context of professional and laboratory settings (typically one-at-a-time tasks administered in a quiet environment) is its poor ecological validity, which can overestimate or otherwise misrepresent real-world performance (Chaytor, & Schmitter-Edgecombe, 2003). Some have argued that traditional EF tests are based on hypothetical constructs that have little predictive value for EF in the real world (Burgess et al., 2006; Parsons, Carlew, Magtoto, & Stonecipher, 2017). A psychometric concern is that EF tests frequently employed in clinical and experimental settings that are reliable at the group level may not translate well to individual differences contexts because they minimize between-subject variability. As a result, some EF tests may not consistently distinguish between individuals (Hedge, Powell, & Sumner, 2018). Some work has indicated that EF self-report measures are more predictive of functional impairment and psychopathology symptoms than EF tests of overt performance (e.g., Barkley & Fischer, 2011; Barkley & Murphy, 2010; Knouse, Barkley, & Murphy, 2013), suggesting that EF rating scales index typical performance, whereas EF tests index optimal performance (Toplak, West, & Stanovich, 2013). The present study used the Behavior Rating Inventory of Executive Function – Self-Report (BRIEF-SR; Guy, Isquith, & Gioia, 2004) to improve ecological and predictive validity relative to most standard EF tests.
The items comprising the BRIEF-SR’s shifting, updating of working memory, and inhibition scales were used to evaluate the utility of Miyake et al.’s (2000) three-factor model in differentiating dimensions of depression and anxiety. As the development of the BRIEF-SR was informed by clinical interactions and the broader EF literature (Guy et al., 2004) not specific to Miyake et al.’s (2000) three-factor model, an Exploratory Factor Analysis (EFA) was implemented to evaluate and maximize inter-item correlations between indicators and construct variance. The latent factors that emerged from the EFA were used to define EF constructs. The measurement model resulting from EFA was subsequently tested via confirmatory factor analysis (CFA) in a non-overlapping sample of participants. Pooling the samples, structural equation modeling (SEM) was then used to estimate relationships between the EF latent variables and dimensional measures of psychopathology symptoms, specifically anxious apprehension, anxious arousal, and depressed mood.
Methods
Participants
Participants were undergraduates (n =1,140) who provided informed consent prior to completing a series of questionnaires for credit in a psychology course. The questionnaires assessed symptoms associated with anxiety and depression: the Penn State Worry Questionnaire (PSWQ; Meyer, Miller, Metzger, & Borkovec, 1990) and the Anxious Arousal and Anhedonic Depression scales of the Mood and Anxiety Symptom Questionnaire (MASQ; Watson, Clark, et al., 1995; Watson, Weber, et al., 1995). Participants filled out the BRIEF-SR during the same questionnaire session. Data from 17 participants were excluded from analyses if questionnaire data had missing or illegible values or unusual response patterns or did not meet tests of multivariate normality (Mahalanobis, 1936). The final sample consisted of 635 females and 451 males1 (mean age2 = 18.7 years, SD = 1.1). The final sample (N = 1,123) was divided in half as observations were randomly selected for exploratory (n =561) and confirmatory (n =562) factor analyses. The total sample (N = 1,123) was used for SEM. As the present sample served as a recruitment pool for a neuroimaging study on affective and cognitive risk factors for psychopathology, all participants were right-handed, native speakers of English with self-reported normal hearing and color vision. Using cutoff scores established by receiver-operating characteristic analyses of the PSWQ (Behar, Alcaine, Zuellig & Borkovec, 2003; Fresco, Mennin, Heimberg, & Turk, 2003) and the depressed mood scale of the MASQ (Bredemeier et al., 2010), degree of psychopathology in the present sample was estimated as follows: between 13.5% and 18.9% of the sample met the clinical cutoff for generalized anxiety disorder, between 15.6% and 23.6% of the sample met the clinical cutoff for major depressive disorder, and between 4.1% and 7.3% of the sample met the clinical cutoffs for both disorders. Rates of depression and anxiety in the present sample are consistent with national estimates in college samples (Duffy, Twenge, & Joiner, 2019). Subsets of participants from the present sample with clinically diagnosed anxiety and mood disorders are published elsewhere (e.g., Bredemeier et al., 2016; Madian et al., 2019; Sadeh, Spielberg, Warren, Miller & Heller, 2014; Warren et al., 2013). The study was approved by the University of Illinois at Urbana-Champaign Institutional Review Board.
Questionnaires and Procedures
Participants completed the BRIEF-SR questionnaire (Guy, Isquith, & Gioia, 2004), involving 80 items assessing EF problems in daily life during the last six months on a three–point scale (1 = never; 2 = sometimes; 3=often). Research indicates that the BRIEF-SR has good clinical utility (e.g., Niendam, Horwitz, Bearden & Cannon, 2007) and internal consistency in normative and clinical samples (Cronbach’s alpha ≥ .82 for shifting, updating of working memory, and inhibition scales; Guy et al., 2004). Only items from the shifting, updating, and inhibition scales (n=35) were subjected to EFA as the goal of the present study was to test specific executive dysfunction hypotheses characterizing depression and anxiety dimensions based on Miyake et al.’s (2000) three-factor model.
The 16-item PSWQ was used to assess anxious apprehension (i.e., the tendency to engage in worry). Participants responded to questions such as “My worries overwhelm me,” by rating how characteristic (1 = not at all to 5 = very typical) each statement was of them. The Anxious Arousal scale of the MASQ (MASQAA) consists of 17 items in which participants responded to statements such as “Startled easily.” An eight-item subscale of the MASQ Anhedonic Depression (MASQAD8) was used to measure depressed mood (Nitschke et al., 2001), given its utility in predicting current depressive disorders (Bredemeier, Spielberg, Silton, Berenbaum, Heller, & Miller, 2010). The MASQAD8 scale consists of items such as “Felt like nothing was very enjoyable.” For both MASQ scales, participants rated how much they experienced each item during the previous week (1 = not at all, 5 = extremely). Research has shown that the PSWQ and MASQ have excellent test-retest reliability and good convergent and discriminant validity in undergraduate and clinical samples (Meyer, et al., 1990; Nitschke et al. 2001; Watson et al., 1995). Internal consistencies for the present sample were .93, .84, and .75, respectively. Dimensional measures of anxiety and depression were selected because they have been shown to effectively distinguish these highly co-occurring constructs, which share many overlapping symptoms (Nitschke et al., 2001).
Data Analysis
The distributions of the observed responses to the BRIEF-SR items did not have a multivariate-normal distribution. Research has indicated that using normal-theory estimation (e.g., Pearson product-moment correlations) factor analytic techniques for ordered, categorical responses to Likert-type scales could result in biased model fit statistics, negatively biased parameter estimates, inflated error variances, and extraction of illegitimate factors (Flora, Finkel, & Foshee, 2003). Thus, polychoric correlations were used for EFA and CFA (Olsson, 1979). Additionally, robust maximum likelihood estimation mean- and variance-adjusted weighted least squares (WLSMV; Muthén, du Toit, & Spisic, 1997) were implemented, as this method has been shown to perform well when modeling categorical data (Brown, 2006; Flora & Curran, 2004).
Mplus 8 software (Muthén & Muthén, 2017) was used to conduct factor analyses and SEM. Resulting items from EFA using a first sample were used as indicators in CFA of a second, independent sample. CFA served as an objective test of the statistical fit against the EF factor model established using EFA. Model fit (CFA and SEM) was evaluated using the mean- and variance-adjusted chi-square goodness-of-fit statistic (χ2; Muthén et al., 1997), the comparative fit index (CFI; Bentler, 1990), the Tucker-Lewis index (TLI; Tucker & Lewis, 1973), and root-mean-square error of approximation (RMSEA; Steiger, 1990). Simulation studies in Yu and Muthén (2001) suggested the following goodness-of-fit values for categorical outcomes: CFI>.95, TLI>.95, and RMSEA<06, which are consistent with Hu and Bentler’s (1999) recommendations. The error variances of two inhibition items were allowed to co-vary to account for similarity in question structure.
Scores on the dimensional measures of anxiety and depression were added as manifest variables. SEM was used to test the relationships between the latent EF variables and the three psychopathology scores, as this method allows for these relationships to be estimated simultaneously and (unlike regression) explicitly accounts for measurement error in predictor variables. Additional structural tests of this model were conducted in order to evaluate potentially distinct relationships between EF latent variables and psychopathology scores. A series of nested models was created in which pairs of standardized psychopathology regression weights leading to one of the latent variables were constrained to be equal and were subsequently compared to a model in which all regression weights were allowed to be freely estimated. All difference tests of the nested models were performed using a chi-square difference procedure described by Asparouhov and Muthén (2006). Model χ2 values and degrees of freedom are not reported for these nested model tests, as they are not interpretable when using WLSMV (only p-values are interpretable; Muthén, 2008).
Results
Exploratory Factor Analysis
Thirty-five items from the BRIEF-SR shifting (n=10), updating of working memory (n=12), and inhibition (n=13) scales were subjected to EFA. Given theoretical and empirical support for moderate correlations among shifting, updating, and inhibition EF processes (e.g., Miyake et al. 2000), an oblique rotation, the Promax method, was applied. In order to obtain simple factor structure, items were retained if their primary loading was ≥.45 and cross-loading was ≤.2. Following procedures outlined by Brown (2006), factor retention was determined using multiple methods: examination of a scree plot of the eigenvalues, goodness of model fit statistics (χ2, RMSEA), and evaluation of the meaningfulness and interpretability of the factors that emerged. Poorly defined factors (e.g., a one-item loading) were eliminated.
Nineteen items (shifting n=4; updating n=5; inhibition n=10) were retained that met the above outlined criteria. Examination of the scree plot (Figure 1), model fit statistics, and interpretability of factors indicated that a three-factor solution best explained the relationships among the items (RMSEA values for one- and two-factor solutions ≥ 0.1; χ2 ps<.001). The complete three-factor solution and model fit statistics are presented in Table 1. Correlations among the three EF latent factors were small to moderate, ranging from .23 to .46 (p<.001; see Table 1).
Figure 1:
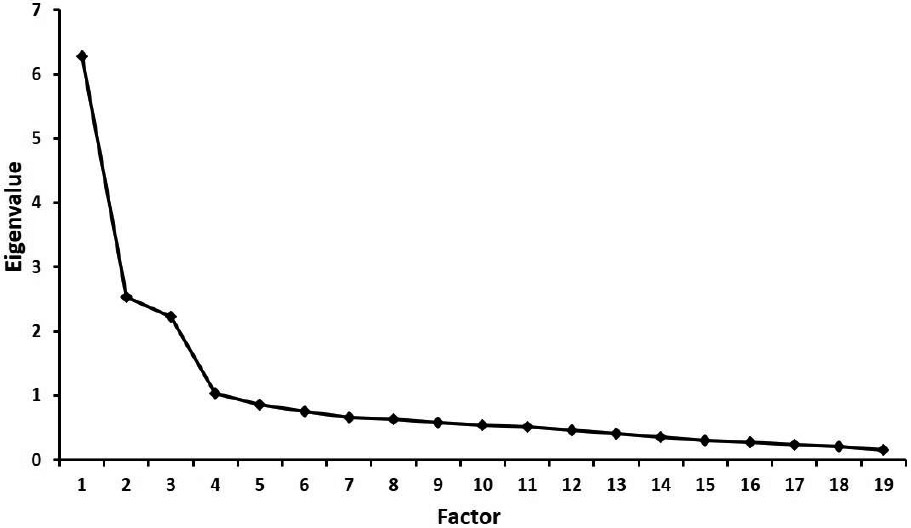
Scree plot from the Exploratory Factory Analysis model indicating that three factors should be extracted. N=561.
Table 1.
Exploratory Factor Analysis: Three-Factor Solution
| Factor |
|||
|---|---|---|---|
| 1 | 2 | 3 | |
| Promax-Rotated Pattern Coefficient | |||
| Item | |||
| I71 | 0.93 | −0.02 | −0.17 |
| I54 | 0.80 | 0.09 | −0.10 |
| I79 | 0.65 | −0.04 | 0.19 |
| I66 | 0.62 | 0.00 | 0.02 |
| I61 | 0.61 | −0.06 | 0.15 |
| I19 | 0.57 | 0.17 | −0.04 |
| I10 | 0.56 | 0.01 | −0.10 |
| I80 | 0.56 | −0.02 | 0.11 |
| I37 | 0.53 | −0.15 | 0.08 |
| I28 | 0.52 | 0.04 | 0.13 |
| S27 | −0.03 | 0.87 | 0.02 |
| S9 | 0.03 | 0.86 | −0.04 |
| S18 | 0.01 | 0.80 | 0.02 |
| S36 | 0.03 | 0.58 | 0.12 |
| WM73 | 0.01 | 0.01 | 0.83 |
| WM63 | −0.07 | 0.09 | 0.80 |
| WM48 | 0.00 | −0.05 | 0.76 |
| WM3 | −0.14 | −0.01 | 0.69 |
| WM39 | 0.19 | −0.03 | 0.57 |
| Interfactor Correlations | |||
| Factor | |||
| 2 | 0.23 | ||
| 3 | 0.46 | 0.23 | |
Note. N= 561. χ2117=258, p<.001. RMSEA = 0.046. Interfactor correlations were significant at p<.001. Entries in bold are the highest loading per item. I=Inhibition; S= Shifting; WM=Working Memory. The number indicates the item number on the BRIEF-SR.
Confirmatory Factor Analysis
Although the chi-square goodness-of-fit statistic (χ2) is typically used to test the fit of CFA models, several fit statistics are reported here, given this statistic’s sensitivity to large sample sizes and consequently excessive Type I error rates (Kline, 2010). The three-factor model was successfully estimated and associated with a χ261 value of 315, p<.001 (Figure 2). Fit indices indicated that this three-factor model provided an excellent fit to the data (CFI=.968; TLI=.963; RMSEA=.045, 90% confidence interval = .038 to .052). Measurement weights for each BRIEF item were significant at p<.001 (see Table 2 for standardized estimates). Correlations among the three EF latent factors were moderate, ranging from .32 to .44 (p<.001; see Figure 2 and Table 2).
Figure 2:
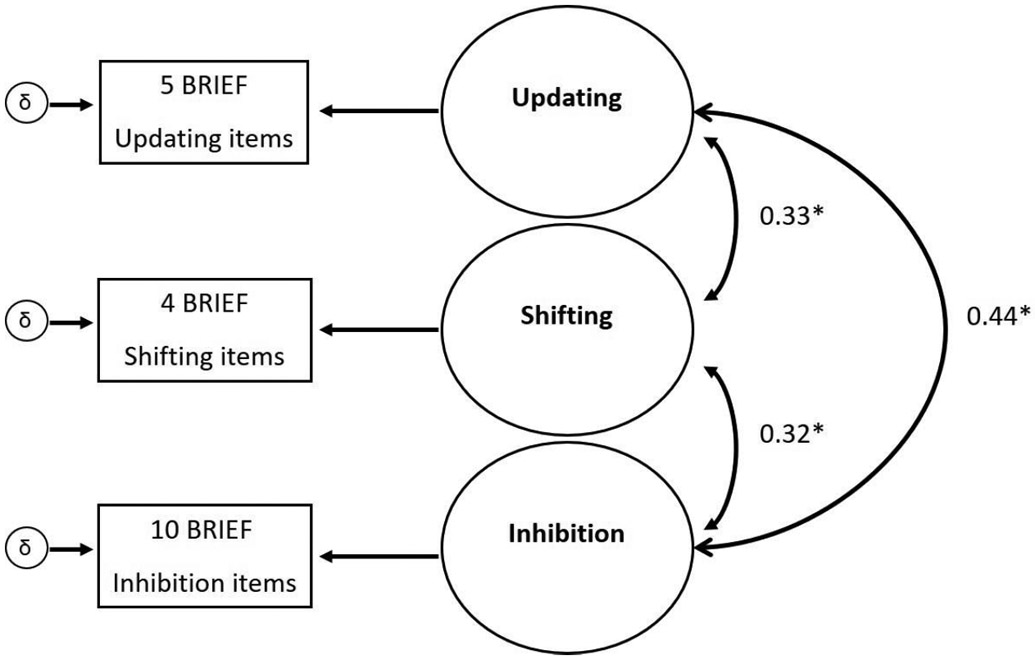
Confirmatory Factor Analysis model for N=562. Updating, Shifting, and Inhibition are latent factors. BRIEF = Behavior Rating Inventory of Executive Function. δ is a measurement error term for the observed latent factor indicators. The individual BRIEF items and covariances between error terms are not pictured for conciseness. *p<.001
Table 2.
Confirmatory Factor Analysis: Standardized Regression Coefficients
| Factor |
|||
|---|---|---|---|
| Inhibit | Shift | Update | |
| Item | |||
| I79 | 0.82 | - | - |
| I61 | 0.72 | - | - |
| I80 | 0.68 | - | - |
| I28 | 0.64 | - | - |
| I54 | 0.62 | - | - |
| I66 | 0.61 | - | - |
| I71 | 0.59 | - | - |
| I19 | 0.59 | - | - |
| I37 | 0.58 | - | - |
| I10 | 0.47 | - | - |
| S18 | - | 0.88 | - |
| S27 | - | 0.87 | - |
| S9 | - | 0.77 | - |
| S36 | - | 0.59 | - |
| WM73 | - | - | 0.90 |
| WM48 | - | - | 0.79 |
| WM63 | - | - | 0.74 |
| WM39 | - | - | 0.73 |
| WM3 | - | - | 0.67 |
| Interfactor Correlations | |||
| Factor | |||
| Shift | 0.32 | ||
| Update | 0.44 | 0.33 | |
Note. N=562. χ261=315, p<.001. CFI=.968; TLI=.963; RMSEA=.045. All measurement weights and interfactor correlations were significant at p<.001. I=Inhibition; S=Shifting; WM=Working Memory. The number indicates the item number on the BRIEF-SR.
Structural Equation Modeling
Descriptive statistics of the psychopathology measures for the total sample are presented in Table 3. Criteria for evaluating model fit were identical to those for the CFA procedure. The model was successfully estimated and associated with a χ2196 value of 578, p<.001. Fit indices indicated that this model provided adequate to good fit to the data (CFI=.954; TLI=.946; RMSEA=.042, 90% confidence interval = .038 to .046)3. Measurement weights for each BRIEF item were significant at p<.001 and were virtually identical to the measurement weights determined by the CFA procedure. Similarly, the correlations among the EF latent factors were small to moderate, ranging from .21 to .38 (p<.001; see Figure 3). The proportion of variance explained by each latent factor was the following: inhibition, 13.6%, shifting 26%, and updating 15.3%.
Table 3.
Self-Report Psychopathology Scores (N=1,123)
| Questionnaire | Mean | SD | Min | Max |
|---|---|---|---|---|
| PSWQ (Anxious Apprehension) | 48.69 | 13.45 | 16 | 80 |
| MASQAA (Anxious Arousal) | 28.31 | 8.55 | 17 | 80 |
| MASQAD8(Depressed Mood) | 17.15 | 5.19 | 8 | 39 |
Note. PSWQ = Penn State Worry Questionnaire. MASQAA = Mood and Anxiety Symptom Questionnaire Anxious Arousal scale. MASQAD8 = Mood and Anxiety Symptom Questionnaire Anhedonic Depression 8-item subscale for depressed mood.
Figure 3:
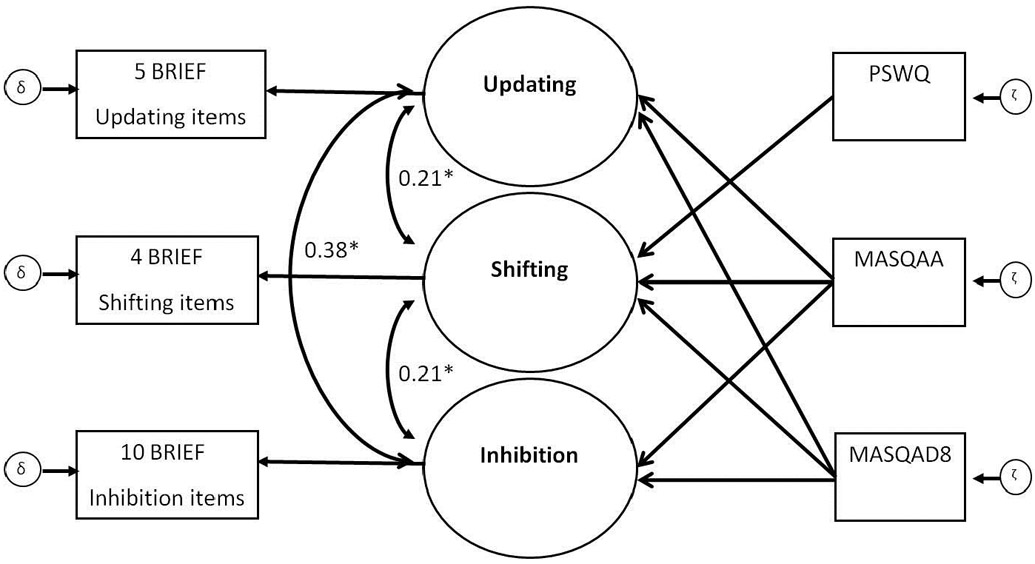
Structural equation model for N=1,123. Psychopathology measures predicting latent executive function variables updating, shifting, and inhibition. PSWQ = Penn State Worry Questionnaire. MASQAA = Mood and Anxiety Symptom Questionnaire Anxious Arousal scale. MASQAD8 = Mood and Anxiety Symptom Questionnaire Anhedonic Depression 8-item subscale for depressed mood. BRIEF = Behavior Rating Inventory of Executive Function. δ is a measurement error term for the observed exogenous (dependent) variables. ζ is a structural (regression) error term for the variance in updating, shifting, and inhibition that is unexplained by PSWQ, MASQAA, and MASQAD8. The regression paths from PSWQ, MASQAA, and MASQAD8 to the EF latent factors are referred to as γ (see Table 4 for values). The covariances between error terms, the individual BRIEF items, and the standardized regression coefficients for the psychopathology exogenous variables (see Table 4) are not pictured for conciseness. *p<.001
The psychopathology manifest variables (PSWQ, MASQAA, and MASQAD8) were modeled as exogenous (independent) variables predicting endogenous (dependent) EF latent variables. Increased levels of anxiety and depression were differentially associated with worse EF (see Figure 3). As shown in Table 4, PSWQ positively predicted problems with shifting, whereas MASQAA and MASQAD8 positively predicted problems with all three domains of EF. Additional structural tests between psychopathology domains determined that the magnitude of the γ (path from depression or anxiety independent variables to EF dependent variables) for PSWQ predicting shifting was larger than the γ’s for MASQAA (p<.001) and MASQAD8 (p<.001). The γ for MASQAD8 predicting shifting was larger than the γ for MASQAA (p<.04). For updating, the γ for MASQAA was larger than the γ’s for PSWQ (p<.001) and MASQAD8 (p=.02); MASQAD8 γ was larger than PSWQ γ (p<.01). Finally, the γ for MASQAA predicting inhibition was larger than the γ’s for PSWQ (p<.001) and MASQAD8 (p<.001). The γs for MASQAD8 and PSWQ predicting inhibition were not statistically different (p=.08).
Table 4.
Structural Equation Modeling: Standardized Regression Coefficients
| Variable | λ | P |
|---|---|---|
| Exogenous variable: PSWQ | ||
| Updating | <.01 | 0.98 |
| Shifting | 0.45 | <.01 |
| Inhibition | <.01 | 0.91 |
| Exogenous variable: MASQAA | ||
| Updating | 0.32 | <.01 |
| Shifting | 0.08 | 0.04 |
| Inhibition | 0.34 | <.01 |
| Exogenous variable: MASQAD8 | ||
| Updating | 0.17 | <.01 |
| Shifting | 0.22 | <.01 |
| Inhibition | 0.11 | <.01 |
Note. N=1123. χ2196=578, p<.001. CFI=.954; TLI=.946; RMSEA=.042. PSWQ = Penn State Worry Questionnaire. MASQAA = Mood and Anxiety Symptom Questionnaire Anxious Arousal scale. MASQAD8 = Mood and Anxiety Symptom Questionnaire Anhedonic Depression 8-item subscale for depressed mood. Updating, shifting, and inhibition represent latent variables derived from EFA and CFA.
Discussion
Although research has demonstrated that anxiety and depression are associated with disruptions in EF, the specific effects observed have been mixed. The present study tested the statistical effects of dimensions of depressed mood and anxiety (operationalized as anxious apprehension and anxious arousal) on EF. As expected, an EFA applied to an ecologically-sensitive, self-report measure of EF in everyday life yielded a three-factor structure representing shifting, updating, and inhibition domains and was replicated via CFA in an independent sample. Also consistent with hypotheses, SEM indicated that depression and anxious arousal demonstrated broad deficits in EF, whereas anxious apprehension was associated with deficits in shifting. As there are few studies that compare prominent mood and anxiety dimensions in terms of their relationships with specific EF domains, present findings can help explain inconsistencies in previous research and provide novel insights into the nature of EF deficits in depression, apprehension, and arousal.
The fact that depressed mood and anxious arousal evidenced reductions across all EF domains indicates that these dimensions may be better characterized by a general disruption in the ability to maintain task goals, also referred to as “common EF” or what is shared among EF domains (Miyake & Friedman, 2012). Common EF represents stability (via goal maintenance) and demonstrates an opposing relationship with shifting (or mental flexibility; for a review, see Snyder et al., 2015b). Delineating how common and specific EF deficits predict clinically relevant phenomena has the potential to advance understanding of EF contributions to psychopathology development, comorbidity, and heterogeneity in symptom presentation. For example, present results indicate that deficits in common EF represent a transdiagnostic feature of depression and anxiety. Indeed, recent work suggests that disruptions in common EF coupled with elevated repetitive negative thought (an element common to worry and rumination; Hur, Heller, Kern, & Berenbaum, 2017) is an important pathway to the development of psychopathology (Madian, Bredemeier, Heller, Miller, & Warren, 2019). Although depressed mood and anxious arousal share common EF reductions, their behavioral phenotypes demonstrate opposing presentations – depressed mood as a lack of arousal and anxious arousal as a pattern of enduring hypervigilance. Future research on depression and anxiety would benefit from exploring how EF deficits predict and interact with other symptom dimensions (e.g., positive and negative affect) that give rise to pathways of disorder co-occurrence and symptom heterogeneity (e.g., Hur et al., 2015; Madian et al., 2019).
Present findings might also have important theoretical implications. Attentional Control Theory (Eysenck et al., 2007) asserts that (undifferentiated) “anxiety” is related to shifting and inhibition impairments. As evidenced here, the nature of executive dysfunction depended on carefully differentiating anxiety dimensions, as well as measuring multiple components of EF. Anxious apprehension was associated with shifting impairments only, whereas anxious arousal demonstrated impairments across all three EF domains. In the context of Attentional Control Theory, results suggest that alterations in shifting have an important influence on cognition and emotion regulation associated with anxious apprehension or excessive worry, but that common EF disruptions, rather than inhibition per se, play a prominent role in anxious arousal. Results also suggest that anxious arousal, rather than anxious apprehension or worry, is the dominant component of anxiety’s effect on cognition and perhaps processing efficiency, although this remains to be empirically tested.
As hypothesized, anxious apprehension predicted impairment in shifting, suggesting that individuals who experience elevated levels of worry have difficulties making necessary cognitive adjustments for switching task sets, resulting in cognitive inflexibility. Impaired shifting could prevent appropriate selection of working memory contents that are pertinent to the task at hand, and could cause difficulty making transitions, problem-solving inflexibility (e.g., approaching a different problem with the same strategy), and difficulty changing focus from one mindset or topic to another. Individuals with elevated anxious apprehension may have difficulty switching attention from a particular set of thoughts to new thoughts or task-relevant thoughts, consequently maintaining dysfunctional worry. Present results have implications for understanding psychological factors maintaining and perhaps contributing to Generalized Anxiety Disorder (GAD). Although excessive and stable patterns of worry are defining criteria of GAD, approaching the development and maintenance of GAD as an emergent property of component interactions - anxious apprehension (the propensity to engage in worry), shifting impairment (cognitive inflexibility), and other relevant components (e.g., negative affect, avoidance motivation) - may help to identify treatment mechanisms and refine treatment approaches to better target those mechanisms.
Although the present study provides new insights into alterations of EF affected by specific dimensions of psychopathology, there are some limitations. First, the study was restricted to an undergraduate sample, and results may not generalize to more cognitively diverse samples. For example, the degree of EF domain separability may be less pronounced in general community samples (e.g., Legree, Pifer, & Grafton, 1996) and may vary across the lifespan. To the degree that distinct brain regions implement these executive processes, neuroimaging evidence suggests that older adults recruit additional bilateral prefrontal regions (for a review, see Reuter-Lorenz & Lustig, 2005). Thus, generalizability to different samples remains to be established. Nonetheless, present findings could serve as a baseline of executive dysfunction in early development of depression and anxiety.
Second, although executive dysfunctions are often viewed as sequelae of psychopathology, it is possible that specific EF deficits confer vulnerability to the development and maintenance of psychopathology, or that there is a bidirectional relationship. The present study was not designed to elucidate causal direction. Prospective studies are needed to draw firm conclusions about the temporal precedence of EF impairment and the development of psychopathology. Indeed, emerging prospective work suggests that executive dysfunction is not merely a reaction to depression and anxiety but may carry its own consequences for emotion regulation and the development of psychopathology (Kertz, Belden, Tilman, & Luby, 2015; Letkiewicz et al., 2014). Experimental studies that directly test causal associations between EF and affective symptoms are needed to explicate these relationships.
Third, as the present study used self-report measures of EF and psychopathology, it is unclear to what extent self-report measures of cognition accurately index cognition in daily life versus perceptions of cognition seen through the lens of current mood. Self-report cognition scales and performance-based measures of cognitive processes correlate relatively poorly (e.g., McAuley, Chen, Goos, Schachar, & Crosbie, 2010; Quigley, Wright, Dobson, & Sears, 2017; Toplak et al., 2013), indicating that they are likely not measuring the same construct. Some work suggests that discrepancies between these two classes of assessment are a result of measuring different aspects of cognitive and behavioral functioning that contribute independently to clinical phenomena. Specifically, EF performance-based tests assess cognitive efficiency within an optimal setting (e.g., distraction-free environment, one test given at a time) and measure broadly defined constructs narrowly (e.g., inhibition measured via a Stroop task does not translate to all areas of inhibition in an individual’s life). On the other hand, EF rating scales index goal pursuit and behaviors related to achieving those goals in everyday life (Toplak et al., 2010), which may improve ecological validity but may carry interpretation limitations (e.g., personality, mood state, or motivation may influence perception and overt behavior rather than EF per se; Buchanan, 2016). Nonetheless, EF rating scales predict meaningful outcomes such as academic performance, and in at least one study good agreement was found between informant and self-report (for review, see Letkiewitz et al., 2014). Further research is needed to test the extent to which performance-based neuropsychological tests replicate present findings, as well as how present findings can augment standardized testing. As both performance-based tests and EF scales provide clinically useful information but are not necessarily interchangeable measures, an integrative framework may advance the development of standardized testing measures that predict everyday behavior.
Despite these limitations, the present research provides novel insights into domain-specific EF impairments that are likely to be important factors in the maintenance, and possibly the development, of distinct dimensions of depression and anxiety. More specifically, present findings implicate EF mechanisms of maladaptive emotion-regulation processes associated with aspects of depression and anxiety. EF deficits may impair an individual’s ability to evaluate, initiate, or engage in pleasurable activities or stimuli that promote pleasant emotional states. Importantly, the present study highlights typically occurring self-reported executive dysfunction in everyday living that is associated with depression and anxiety, extending previous EF research obtained in formal (and typically artificial) evaluation settings. Indeed, the cognitive processes that formal tests of EF purport to measure are still not well known, and the range of behaviors and activities in an individual’s everyday environment that require these same processes remains to be established (Burgess, Alderman, Volle, Benoit, & Gilbert, 2009). Finally, this is the only within-subjects study to date that explicitly assesses specific EF impairments, at the level of latent variables, among anxious apprehension, anxious arousal, and depressed mood, so replication is needed.
In summary, the present study tested the effects of depressed mood, anxious arousal, and anxious apprehension on multiple dimensions of EF. Depression and anxious arousal demonstrated broad deficits in EF, whereas anxious apprehension was associated with deficits in shifting. As evidenced here, executive dysfunction associated with depression and anxious arousal could not be accurately accounted for by examining one aspect of EF. Furthermore, if the focus is on just one dimension of EF, as has often been the case in the literature, it is possible that what appears to be a primary EF deficit in depression or anxiety is actually the result of another correlated, yet separable EF component (e.g., inhibition vs. shifting for depression). Comprehensive approaches in the measurement of EF domains will likely yield fruitful avenues for psychopathology research.
Supplementary Material
Highlights:
Executive function (EF) disruptions in depression and anxiety are underspecified
Factor analyses supported and replicated an EF model using a self-report measure
SEM tested types of EF difficulties related to affective symptoms
Depressed mood and anxious arousal evidenced broad EF deficits
Anxious apprehension (worry) evidenced a deficit in cognitive shifting
ACKNOWLEDGEMENTS
S.L. Warren developed the study concept and design and executed all data analyses under the primary mentorship of W. Heller and G.A. Miller. Warren drafted the initial version of the manuscript, which was revised by all the authors. All authors approved the final version of the manuscript for submission.
This study was submitted in partial fulfillment of dissertation requirements at the University of Illinois at Urbana-Champaign for Stacie L. Warren.
This research was supported by the National Institutes of Mental Health (P50 MH079485, R01 MH61358, T32 MH19554), the University of Illinois Department of Psychology, and the Palo Alto University Department of Psychology.
Role of funding sources: data collection, analysis, and manuscript preparation for this study was supported in part by the National Institutes of Mental Health (P50 MH079485, R01 MH61358, T32 MH19554); and the University of Illinois Department of Psychology. Additional data analysis and manuscript preparation was supported in part by the Palo Alto University Department of Psychology.
Footnotes
Declaration of interests
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Thirty-seven individuals did not specify their gender
Forty individuals did not specify their age
As there are known gender differences in the prevalence of mood and anxiety disorders, the present SEM was repeated adding gender as a covariate. Model fit statistics were nearly identical (χ2260 value of 629, p<.001; CFI=.953; TLI=.945; RMSEA=.036, 90% confidence interval = .033 to .040). Shifting impairment was greater for females than males (γ=−0.082,p<.01). The effect of depressed mood on shifting was greater for females than males (γ=−0.066, p<.05). Lastly, the effect of anxious apprehension on shifting was greater for males than females (γ=0.069, p<.038). No other gender effects were observed.
References
- Airaksinen E, Larsson M, & Forsell Y (2005). Neuropsychological functions in anxiety disorders in population-based samples: evidence of episodic memory dysfunction. Journal of Psychiatric Research, 39, 207–214. doi: 10.1016/j.jpsychires.2004.06.001 [DOI] [PubMed] [Google Scholar]
- Altamirano LJ, Miyake A, & Whitmer AJ (2010). When mental inflexibility facilitates executive control: Beneficial side effects of ruminative tendencies on goal maintenance. Psychological Science, 21, 1377–1382. doi: 10.1177/0956797610381505. [DOI] [PMC free article] [PubMed] [Google Scholar]
- American Psychiatric Association [APA], (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Arlington, VA: American Psychiatric Publishing. [Google Scholar]
- Asparouhov T, & Muthén B (2006). Robust Chi Square Difference Testing with mean and variance adjusted test statistics. Retrieved from http://www.statmodel.com/download/webnotes/webnote10.
- Austin MP, Mitchell P, & Goodwin GM (2001). Cognitive deficits in depression: Possible implications for functional neuropathology. The British Journal of Psychiatry, 178, 200–206. doi: 10.1192/bjp.178.3.200 [DOI] [PubMed] [Google Scholar]
- Baddeley A (2003). Working memory: Looking back and looking forward. Nature Reviews Neuroscience, 4(10), 829–839. doi: 10.1038/nrn1201 [DOI] [PubMed] [Google Scholar]
- Barkley RA, & Fischer M (2011). Predicting impairment in major life activities and occupational functioning in hyperactive children as adults: Self-reported executive function (EF) deficits versus EF tests. Developmental Neuropsychology, 36(2), 137–161 doi: 10.1080/87565641.2010.549877 [DOI] [PubMed] [Google Scholar]
- Barkley RA, & Murphy KR (2010). Impairment in occupational functioning and adult ADHD: the predictive utility of executive function (EF) ratings versus EF tests. Archives of Clinical Neuropsychology, 25(3), 157–173. doi: 10.1093/arclin/acq014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bentler PM (1990). Comparative fit indexes in structural models. Psychological Bulletin, 107, 238–246. doi: 10.1037/0033-2909.107.2.238 [DOI] [PubMed] [Google Scholar]
- Berggren N, & Derakshan N (2012) Attentional control deficits in trait anxiety: Why you see them and why you don’t. Biological Psychology. Advance online publication. doi: 10.1016/j.biopsycho.2012.03.007 [DOI] [PubMed] [Google Scholar]
- Bredemeier K, Spielberg JM, Silton RL, Berenbaum H, Heller W, & Miller GA (2010). Screening for depressive disorders using the Mood Anxiety Symptoms Questionnaire Anhedonic Depression Scale: A receiver-operating characteristic analysis. Psychological Assessment, 22, 702–710. doi: 10.1037/a0019915 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bredemeier K, Warren SL, Berenbaum H, Miller GA, & Heller W (2016). Executive function deficits associated with current and past major depressive symptoms. Journal of Affective Disorders, 204, 226–233. doi: 10.1016/j.jad.2016.03.070 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brown TA (2006). Confirmatory factor analysis for applied research. New York: Guilford Press. [Google Scholar]
- Buchanan T (2016). Self-report measures of executive function problems correlate with personality, not performance-based executive function measures, in nonclinical samples. Psychological Assessment, 28(4), 372. doi: 10.1037/pas0000192 [DOI] [PubMed] [Google Scholar]
- Burgess PW, Alderman N, Forbes C, Costello A, Laure MC, Dawson DR, … Channon S (2006). The case for the development and use of “ecologically valid” measures of executive function in experimental and clinical neuropsychology. Journal of the International Neuropsychological Society, 12, 194–209. doi: 10.1017/S1355617706060310 [DOI] [PubMed] [Google Scholar]
- Burgess PW, Alderman N, Volle E, Benoit RG, & Gilbert SJ (2009). Mesulam’s frontal lobe mystery re-examined. Restorative Neurology and Neuroscience, 27, 493–506. doi: 10.3233/RNN-2009-0511 [DOI] [PubMed] [Google Scholar]
- Castaneda AE, Suvisaari J, Marttunen M, Perala J, Saarni SI, Aalto-Setälä T, … Tuulio-Henriksson A (2010). Cognitive functioning in a population-based sample of young adults with anxiety disorders. European Psychiatry, doi: 10.1016/j.eurpsy.2009.11.006 [DOI] [PubMed] [Google Scholar]
- Chaytor N, & Schmitter-Edgecombe M (2003). The ecological validity of neuropsychological tests: A review of the literature on everyday cognitive skills. Neuropsychology Review, 13(4), 181–197. doi: 10.1023/B:NERV.0000009483.91468.fb [DOI] [PubMed] [Google Scholar]
- Davidson RJ, Pizzagalli D, Nitschke JB, & Putnam K (2002). Depression: perspectives from affective neuroscience. Annual Review of Psychology, 53(1), 545–574. doi: 10.1146/annurev.psych.53.100901.135148 [DOI] [PubMed] [Google Scholar]
- De Raedt R, & Koster EH (2010). Understanding vulnerability for depression from a cognitive neuroscience perspective: A reappraisal of attentional factors and a new conceptual framework. Cognitive, Affective, & Behavioral Neuroscience, 10(1), 50–70. doi: 10.3758/CABN.10.1.50 [DOI] [PubMed] [Google Scholar]
- Duffy ME, Twenge JM, & Joiner TE (2019). Trends in mood and anxiety symptoms and suicide-related outcomes among US undergraduates, 2007–2018: Evidence from two national surveys. Journal of Adolescent Health, 65(5), 590–598.doi 10.1016/j.jadohealth.2019.04.033 [DOI] [PubMed] [Google Scholar]
- Engels A, Heller W, Mohanty A, Herrington J, Banich M, Webb A, & Miller GA (2007). Specificity of regional brain activity in anxiety types during emotion processing. Psychophysiology, 44, 352–363. doi: 10.1111/j.1469-8986.2007.00518.x [DOI] [PubMed] [Google Scholar]
- Engels AS, Heller W, Spielberg JM, Warren SL, Sutton BP, Banich MT, & Miller GA (2010). Co-occurring anxiety influences patterns of brain activity in depression. Cognitive, Affective & Behavioral Neuroscience, 10, 141–156. doi: 10.3758/CABN.10.1.141 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Engle R, Kane MJ, & Tuholski SW (1999). Individual differences in working memory capacity and what they tell us about controlled attention, general fluid intelligence, and functions of the prefrontal cortex In Miyake A & Shah P (Eds.), Models of working memory: Mechanisms of active maintenance and executive control (pp. 102–134). New York, NY: Cambridge University Press. [Google Scholar]
- Eysenck MW, Payne S, & Derakshan N (2005). Trait anxiety, visuospatial processing, and working memory. Cognition and Emotion, 19, 1214–1228. doi: 10.1080/02699930500260245 [DOI] [Google Scholar]
- Eysenck MW, Derakshan N, Santos R, & Calvo MG (2007). Anxiety and cognitive performance: Attentional control theory. Emotion, 7, 336–353. doi: 10.1037/1528-3542.7.2.336 [DOI] [PubMed] [Google Scholar]
- Flora DB, Curran PJ (2004). An empirical evaluation of alternative methods of estimation for confirmatory factor analysis with ordinal data. Psychological Methods, 9, 466–491. doi: 10.1037/1082-989X.9.4.466 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Flora DB, Finkel EJ, & Foshee VA (2003). Higher order factor structure of a self-control test: Evidence from confirmatory factor analysis with polychoric correlations. Educational and Psychological Measurement, 63(1), 112–127. doi: 10.1177/0013164402239320 [DOI] [Google Scholar]
- Friedman NP, & Miyake A (2004). The relations among inhibition and interference control functions: A latent-variable analysis. Journal of experimental psychology. General, 133(1), 101–135. doi: 10.1037/0096-3445.133.1.101 [DOI] [PubMed] [Google Scholar]
- Guy SC, Isquith PK, & Gioia GA (2004). Behavior rating inventory of executive function – self-report version. Lutz, FL: Psychological Assessment Resources. [Google Scholar]
- Hayes S, Hirsch C, & Mathews A (2008). Restriction of working memory capacity during worry. Journal of Abnormal Psychology, 117, 712–717. doi: 10.1037/a0012908 [DOI] [PubMed] [Google Scholar]
- Hedge C, Powell G, & Sumner P (2018). The reliability paradox: Why robust cognitive tasks do not produce reliable individual differences. Behavior Research Methods, 50(3), 1166–1186. doi: 10.3758/s13428-017-0935-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hu L, & Bentler PM (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling, 6, 1–55. doi: 10.1080/10705519909540118 [DOI] [Google Scholar]
- Hur J, Heller W, Kern JL, & Berenbaum H (2017). A bi-factor approach to modeling the structure of worry and rumination. Journal of Experimental Psychopathology, 8(3), 252–264. doi: 10.5127/jep.057116 [DOI] [Google Scholar]
- Hur J, Miller GA, McDavitt J, Spielberg JM, Crocker LC, Infantolino ZP, Towers DN, Warren SL, & Heller W (2015). Interactive effects of trait and state affect on top-down control of attention. Social, Cognitive, and Affective Neuroscience, 10(8), 1128–1136. doi: 10.1093/scan/nsu163. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Joormann J, & Gotlib IH (2010). Emotion regulation in depression: Relation to cognitive inhibition. Cognition and Emotion, 24(2), 281–298. doi: 10.1080/02699930903407948 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kertz SJ, Belden AC, Tillman R, & Luby J (2016). Cognitive control deficits in shifting and inhibition in preschool age children are associated with increased depression and anxiety over 7.5 years of development. Journal of Abnormal Child Psychology, 44(6), 1185–1196. doi: 10.1007/s10802-015-0101-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Knouse LE, Barkley RA, & Murphy KR (2013). Does executive functioning (EF) predict depression in clinic-referred adults?: EF tests vs. rating scales. Journal of Affective Disorders, 145(2), 270–275. doi: 10.1016/j.jad.2012.05.064 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kline RB (2011). Principles and practice of structural equation modeling (3rd ed.). New York: Guilford. [Google Scholar]
- Legree PJ, Pifer ME, & Grafton FC (1996). Correlations among cognitive abilities are lower for higher ability groups. Intelligence, 23, 45–57. doi: 10.1016/S0160-2896(96)80005-5 [DOI] [Google Scholar]
- LeMoult J, & Gotlib IH (2019). Depression: a cognitive perspective. Clinical Psychology Review, 69, 51–66. doi: 10.1016/j.cpr.2018.06.008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Letkiewicz AM, Miller GA, Crocker LD, Warren SL, Infantolino ZP, Mimnaugh KJ, & Heller W (2014). Executive function deficits in daily life prospectively predict increases in depressive symptoms. Cognitive Therapy and Research, 38(6), 612–620. doi: 10.1007/s10608-014-9629-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Madian N, Bredemeier K, Heller W, Miller GA, & Warren SL (2019). Repetitive negative thought and executive dysfunction: An interactive pathway to emotional distress. Cognitive Therapy and Research, 43(2), 464–480. doi: 10.1007/s10608-018-9966-x [DOI] [Google Scholar]
- Mahalanobis PC (1936). On the generalized distance in statistics. Proceedings of the National Institute of Science of India, 2(1), 49–55. [Google Scholar]
- Martin J, & Failows L (2010). Executive function: Theoretical concerns In Sokol B, Muller U, Carpendale J, Young A, & Iarocci G (Eds.), Self and social regulation: Social interaction and the development of social understanding and executive functions (pp. 35–55). Oxford, UK: Oxford University Press. [Google Scholar]
- McAuley T, Chen S, Goos L, Schachar R, & Crosbie J (2010). Is the behavior rating inventory of executive function more strongly associated with measures of impairment or executive function?. Journal of the International Neuropsychological Society, 16(3), 495–505. doi: 10.1017/S1355617710000093 [DOI] [PubMed] [Google Scholar]
- Meyer TJ, Miller ML, Metzger RL, & Borkovec TD (1990). Development and validation of the Penn State Worry Questionnaire. Behaviour Research and Therapy, 28, 487–495. doi: 10.1016/0005-7967(90)90135-6 [DOI] [PubMed] [Google Scholar]
- Miyake A, & Friedman NP (2012). The nature and organization of individual differences in executive functions: Four General conclusions. Current Directions in Psychological Science, 21, 8–14. doi: 10.1177/0963721411429458 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miyake A, Friedman NP, Emerson MJ, Witzki AH , Howerter A, & Wager TD (2000). The unity and diversity of executive functions and their contributions to complex “frontal lobe” tasks: A latent variable analysis. Cognitive Psychology, 41, 49–100. doi: 10.1006/cogp.1999.0734 [DOI] [PubMed] [Google Scholar]
- Moran TP (2016). Anxiety and working memory capacity: A meta-analysis and narrative review. doi: 10.1037/bul0000051 [DOI] [PubMed] [Google Scholar]
- Muthén LK (2008, March 30). Temporal invariance [Msg 6]. Message posted to http://www.statmodel.com/discussion/messages/9/3012.html?1207672749. [Google Scholar]
- Muthén B, du Toit SHC & Spisic D (1997). Robust inference using weighted least squares and quadratic estimating equations in latent variable modeling with categorical and continuous outcomes. Unpublished technical report.
- Muthén LK, & Muthén B,O (2017). Mplus (Version 8). Los Angeles, CA: Author. [Google Scholar]
- Niendam TA, Horwitz J, Bearden CE, & Cannon TD (2007). Ecological assessment of executive dysfunction in the psychosis prodrome: A pilot study. Schizophrenia Research, 93, 350–354. doi: 10.1016/j.schres.2007.03.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nitschke JB, Heller W, Imig JC, McDonald RP, & Miller GA (2001). Distinguishing dimensions of anxiety and depression. Cognitive Therapy and Research, 25, 1–22. doi: 10.1023/A:1026485530405. [DOI] [Google Scholar]
- Nolen-Hoeksema S, Wisco BE, & Lyubomirsky S (2008). Rethinking rumination. Perspectives on Psychological Science, 3400–424. doi: 10.1111/j.1745-6924.2008.00088.x [DOI] [PubMed] [Google Scholar]
- Olsson U (1979). Maximun likelihood estimation of the polychoric correlation coefficient. Psychometrika, 44, 443–460. doi: 10.1007/BF02296207 [DOI] [Google Scholar]
- Parsons TD, Carlew AR, Magtoto J, & Stonecipher K (2017). The potential of function-led virtual environments for ecologically valid measures of executive function in experimental and clinical neuropsychology. Neuropsychological Rehabilitation, 27(5), 777–807. doi: 10.1080/09602011.2015.1109524 [DOI] [PubMed] [Google Scholar]
- Quigley L, Wright CA, Dobson KS, & Sears CR (2017). Measuring attentional control ability or beliefs? Evaluation of the factor structure and convergent validity of the attentional control scale. Journal of Psychopathology and Behavioral Assessment, 39(4), 742–754. doi: 10.1007/s10862-017-9617-7 [DOI] [Google Scholar]
- Reuter-Lorenz PA, & Cappell KA (2008). Neurocognitive aging and the compensation hypothesis. Current Directions in Psychological Science, 17, 177–182. doi: 10.1111/j.1467-8721.2008.00570.x [DOI] [Google Scholar]
- Rock PL, Roiser JP, Riedel WJ, & Blackwell AD (2013). Cognitive impairment in depression: A systematic review and meta-analysis. Psychological Medicine, 29, 1–12. doi: 10.1017/S0033291713002535 [DOI] [PubMed] [Google Scholar]
- Sadeh NS, Spielberg JM, Warren SL, Miller GA, & Heller H (2014). Aberrant neural connectivity during emotional processing associated with posttraumatic stress. Clinical Psychological Science, 2, 748–755. doi: 10.1177/2167702614530113 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Saveanu R, Etkin A, Duchemin AM, Goldstein-Piekarski A, Gyurak A, Debattista C, … Rekshan WR (2015). The International Study to Predict Optimized Treatment in Depression (iSPOT-D): outcomes from the acute phase of antidepressant treatment. Journal of Psychiatric Research, 61, 1–12. doi: 10.1016/j.jpsychires.2014.12.018 [DOI] [PubMed] [Google Scholar]
- Sharp PB, Miller GA, & Heller W (2015). Transdiagnostic dimensions of anxiety: neural mechanisms, executive functions, and new directions. International Journal of Psychophysiology, 98(2), 365–377. doi: 10.1016/j.ijpsycho.2015.07.001 [DOI] [PubMed] [Google Scholar]
- Siemer M (2005). Mood congruent cognitions constitute mood experience. Emotion, 5, 296–308. doi: 10.1037/1528-3542.5.3.296 [DOI] [PubMed] [Google Scholar]
- Snyder HR (2013). Major depressive disorder is associated with broad impairments on neuropsychological measures of executive function: A meta-analysis and review. Psychological Bulletin. Advance online publication. doi: 10.1037/a0028727 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Snyder HR, Kaiser RK, Warren SL, & Heller W (2015)a. Obsessive compulsive disorder is associated with broad impairments in executive function: A meta-analysis. Clinical Psychological Science, 3, 301–330. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Snyder HR, Miyake A, & Hankin BL (2015)b. Advancing understanding of executive function impairments and psychopathology: bridging the gap between clinical and cognitive approaches. Frontiers in Psychology, 6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Steiger JH (1990). Structural model evaluation and modification: An interval estimation approach. Multivariate Behavioral Research, 25, 173–180. doi: 10.1207/s15327906mbr2502_4 [DOI] [PubMed] [Google Scholar]
- Stuss DT, & Alexander MP (2000). Executive functions and the frontal lobes: A conceptual view. Psychological Research, 63, 289–298. doi: 10.1007/s004269900007 [DOI] [PubMed] [Google Scholar]
- Toplak ME, West RF, & Stanovich KE (2013). Practitioner review: Do performance-based measures and ratings of executive function assess the same construct?. Journal of Child Psychology and Psychiatry, 54(2), 131–143. doi: 10.1111/jcpp.12001 [DOI] [PubMed] [Google Scholar]
- Tucker LR, & Lewis C (1973). A reliability coefficient for maximum likelihood factor analysis. Psychometrika, 38, 1–10. doi: 10.1007/BF02291170 [DOI] [Google Scholar]
- Warren SL, Crocker LD, Spielberg JM, Engels AS, Banich MT, Sutton BP, … Heller W (2013). Cortical organization of inhibition-related functions and modulation by psychopathology. Frontiers in Human Neuroscience, 7, 271 10.3389/fnhum.2013.00271. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Watson D, Weber K, Assenheimer JS, Clark LA, Strauss ME, & McCormick RA (1995). Testing a tripartite model: I. Evaluating the convergent and discriminant validity of anxiety and depression symptom scales. Journal of Abnormal Psychology, 104, 3–14. doi: 10.1037/0021-843X.104.1.3. [DOI] [PubMed] [Google Scholar]
- Watson D, Clark LA, Weber K, Assenheimer JS, Strauss ME, & McCormick RA (1995). Testing a tripartite model: II. Exploring the symptom structure of anxiety and depression in student, adult, and patient samples. Journal of Abnormal Psychology, 104, 15–25. doi: 10.1037/0021-843X.104.1.15 [DOI] [PubMed] [Google Scholar]
- Yu CY, & Muthén BO (2001). Evaluation of model fit indices for latent variable models with categorical and continuous outcomes (Technical report). Los Angeles: University of California, Los Angeles, Graduate School of Education and Information Studies. [Google Scholar]
- Zilverstand A, Parvaz MA, & Goldstein RZ (2017). Neuroimaging cognitive reappraisal in clinical populations to define neural targets for enhancing emotion regulation. A systematic review. Neuroimage, 151, 105–116. doi: 10.1016/j.neuroimage.2016.06.009 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.