

Abstract
Amidst the coronavirus disease 2019 (COVID‐19) pandemic, there is uncertainty regarding potential lasting impacts on children's health and educational outcomes. Play, a fundamental part of childhood, may be integral to children's health during crises. We undertook a rapid review of the impact of quarantine, isolation and other restrictive environments on play and whether play mitigates adverse effects of such restrictions. Fifteen peer‐reviewed studies were identified, spanning hospitals, juvenile and immigration detention and refugee camps. We found evidence of changes in children's access to play in crises and quarantine. These studies indicated how play might support children enduring isolation but lacked robust investigations of play as an intervention in mitigating impacts of restriction. Studies pertaining to children in isolation due to infectious disease outbreaks were notably absent. It is important that the potential effects of changes to such a crucial aspect of childhood are better understood to support children in this and future crises.
Keywords: children, disease outbreak, isolation, mental health, play, restriction
Key messages.
Children have a fundamental right to play, yet access to play can be considerably altered in circumstances of quarantine, isolation or restriction.
Evidence from this review suggests that quarantine and restriction do change children's access to play and play opportunities.
Play provides children with a means for expressiveness and coping, skill promotion, and activity and social connectivity, but there is limited research on whether play can mitigate the risks that quarantine can have on children's physical and mental health.
There is a clear need for more research that evaluates children's play, particularly from children's perspectives, in social isolation during a pandemic or disease outbreak.
As we learn how to support children living in and emerging from a pandemic‐related lockdown, play may be one of the most important areas of focus to promote children's health and well‐being.
1. INTRODUCTION
The ongoing coronavirus disease 2019 (COVID‐19) pandemic is a health crisis that is uniquely affecting members of the global community. In such moments, it is often vulnerable populations that are acutely affected, not only medically but also socio‐economically and psychologically (Berkman, 2008; Hutchins, Truman, Merlin, & Redd, 2009). For children, this vulnerability may be reflected in their general disease susceptibility, access to education, nutrition, socio‐economic status and physical and psychological safety (Armitage & Nellums, 2020; Landrigan, 2005). There is concern that health crises like COVID‐19 can have hidden, yet potentially profound and long‐lasting, impacts on children's health and education (Ramchandani, 2020).
As a universal crisis, virtually, all children in all countries are being impacted by COVID‐19 (United Nations, 2020). Social distancing and nation‐wide lockdowns were instated beginning in January 2020 to slow the transmission of the virus among populations after the declaration of COVID‐19 as a pandemic (Ren, 2020; World Health Organization, 2020). In April 2020, UNICEF reported that 2.34 billion children lived in one of the 186 countries with movement restrictions in place due to COVID‐19, and 60% of children lived in one of the 82 countries that experienced a full (7%) or partial (53%) lockdown (Fore, 2020). Such restrictions include school closures, playground and public park closures, gathering restrictions and quarantine requirements. More recently, as regulations continue to change (varying markedly by location), researchers and health care professionals have warned that though children are less clinically impacted by this virus, they are still deeply affected (Dong et al., 2020; Sinha, Bennett, & Taylor‐Robinson, 2020). Children are specifically at risk due to reduced access to food, nutrition, essential social and health services, preventative care measures and the detrimental possible effects of prolonged school closures such as a widening learning gap and socio‐economic disparity (Andrew et al., 2020; Clark et al., 2020; Roberton et al., 2020). By consequence of these disruptions to typical life and childhood, there has been an unprecedented and global shift in where, when, how and with whom play occurs.
There is good reason to take changes to children's play seriously. Emerging evidence suggests that prolonged school closure, home confinement and social restrictions during disease outbreak could have serious consequences for children's physical and mental health, highlighting the need for preventative support and early intervention for children facing social restrictions (Brooks et al., 2020; Guan et al., 2020; Holmes et al., 2020; Loades et al., 2020; Xie et al., 2020). For children living within these severe safety restrictions, play may be one of the most essential ways to attend to their health, development and learning. Play is a fundamental right of all children (United Nations Committee on the Rights of the Child [UNCRC], 2013), and its importance for encouraging psychological and physical health has been highlighted in academic and advocacy contexts (Cohen & Gadassi, 2018; International Play Association, 2020; Nijhof et al., 2018; Yogman et al., 2018). In crisis situations, play helps children to cope with stress, anxiety and trauma (Chatterjee, 2018) and provides stability, normalcy and enjoyment (International Play Association, 2017). It is of concern, therefore, that at a time of increased stress and worry, children are also faced with shifts in or reduced access to play and the affordances it offers for their development and coping. Thus, it is important in this critical moment to better understand the connections between physical or environmental restrictions, children's play and their health, development and well‐being.
2. RATIONALE FOR THIS REVIEW
This review aimed to collate the available evidence on the impact of quarantine and isolation on children's play and to investigate whether play might mitigate any adverse effects of quarantine or isolation on children's health and educational outcomes. We endeavoured to identify gaps in the research literature and inform the foundations of policies that affect children during moments of crisis.
3. RESEARCH QUESTIONS
Based on a review of research:
How might quarantine and related restricted environments affect play in children and young people?
In what ways might play and related activities mitigate the impact of quarantine and restriction on children/young people's health and education?
4. SEARCH STRATEGY AND SELECTION CRITERIA
We conducted a rapid review to synthesize evidence on children's play under restrictive circumstances. We defined quarantine and related restricted environments as an extended state of living where children have limited movement (e.g. from home or hospital) because of restrictions imposed by the government or medical advice, or other factors beyond their own control. Our definition of play and related activities was drawn from language put forth by the UNCRC, General Comment No. 17 (Article 31), which states the rights of all children to ‘… rest and leisure, to engage in play and recreational activities appropriate to the age of the child and to participate freely in cultural life and the arts’. Further detail of what constitutes play behaviours can be found in General Comment No. 17 (UNCRC, 2013, pp. 5–7).
We limited the databases searched and abbreviated the data extraction and synthesis strategies according to accepted parameters for streamlining traditional review methodologies (Ganann, Ciliska, & Thomas, 2010). Search terms relating to (A) the population of interest (children and young people, henceforth referred to as ‘children’), (B) quarantine and restricted environments and (C) play and related activities (henceforth referred to as ‘play’) were included. Appendix A details the search syntax.
The review protocol was registered with the Open Science Framework (OSF) on 16 April 2020, and we engaged the academic community in an open consultation process, soliciting feedback from leading experts and organizations (www.osf.io/vqjnk). Feedback predominantly centred upon search term inclusion and clarity, with suggestions for additional terms or aspects to consider. The authorship team carefully considered all feedback and adapted the final search strategy. We searched key databases indexing psychological, educational and medical research (PsycInfo, ERIC and PubMed) using the same syntax (Appendix A) between 21 April and 25 April 2020, filtering for English‐language articles.
Inclusion criteria consisted of peer‐reviewed research reports, involving participants under age 18, participants experiencing quarantine or related restricted environments, assessment of (or collected data on) educational, developmental or health‐related outcomes and referencing play in relation to study concept. All articles were title and abstract screened for eligibility. After initial screening, any papers where there was uncertainty about whether they met inclusion criteria were flagged and discussed by the authors to reach consensus. The articles selected for inclusion were then also screened by at least one other author to ensure adherence to criteria.
5. RESULTS
Our search yielded 5897 papers, of which 12 met the inclusion criteria (see Figure 1). Handsearching provided an additional three papers, totalling 15 studies. Study characteristics were extracted, and key themes were identified via narrative synthesis. See Table 1 for study characteristics and corresponding reference numbers.
FIGURE 1.
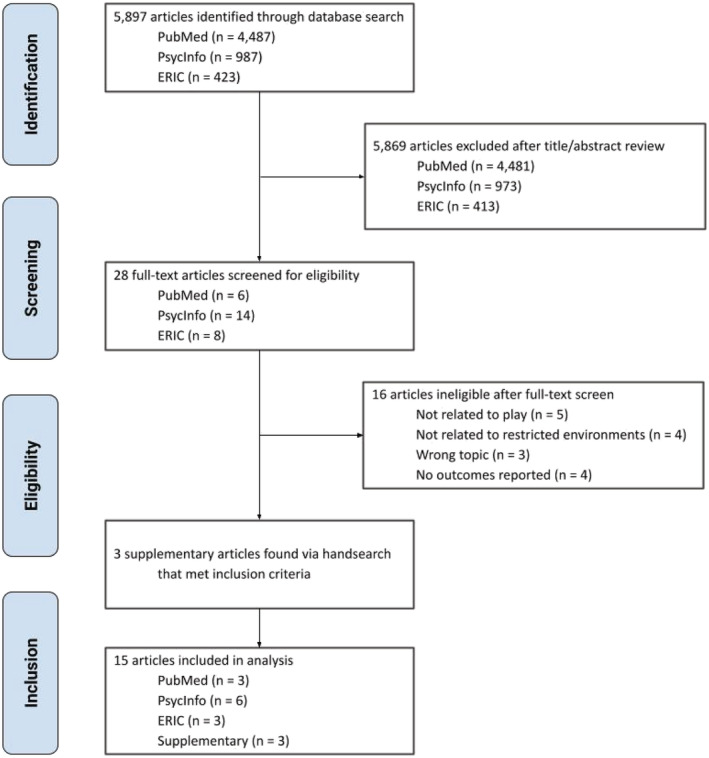
PRISMA flowchart [Colour figure can be viewed at wileyonlinelibrary.com]
TABLE 1.
Study characteristics
| Study | Country | Design | Measures | Participant age | Sample size | Restriction setting | Type of play | |
|---|---|---|---|---|---|---|---|---|
| (1) | Brodsky (1989) a | Israel | Qualitative | NA | 4–10 years | 4 | Hospital | Music |
| (2) | Hollenbeck et al. (1980) | USA | Quantitative | Observation | 18 months to 4 years | 4 | Hospital | Undefined |
| (3) | Kronick, Rousseau, and Cleveland (2015) a | Canada | Qualitative | Ethnographic observation, interviews | 6–18 years | 20 families | Immigration detention | Undefined |
| (4) | Kronick, Rousseau, and Cleveland (2018) | Canada | Qualitative | Interviews and observations | 3–13 years | 10 | Immigration detention | Sand play |
| (5) | Kuntz et al. (1996) a | USA | Qualitative | Case studies | 0–7 years | 2 | Hospital | Toy play |
| (6) | Lambert, Coad, Hicks, and Glacken (2014) | Ireland | Qualitative | Semi‐structured interviews and art activities | 5–8 years | 55 | Hospital | Art, discussion |
| (7) | Linn, Beardslee, and Patenaude (1996) | USA | Qualitative | Puppet play | 4–6 years | 1 | Hospital | Puppet play |
| (8) | Mares, Newman, Dudley, and Gale (2002) | Australia | Qualitative | NA | 5 months to 21 years | 2 families | Immigration detention | Undefined |
| (9) | Pytash (2013) | USA | Qualitative | Case study, observations and interviews | 17 years | 1 | Juvenile detention | Reading, writing |
| (10) | Robb (2000) | USA | Quantitative | Observation, Affective Face Scale | 4–11 years | 10 | Hospital | Music, varied |
| (11) | Shea and Siu (2016) | USA | Mixed methods | Study‐specific survey, observation, analysis of worksheet/craft | 14–18 years | 295 | Juvenile detention | Varied |
| (12) | Susman et al. (1981) | USA | Quantitative | Observation | 18 months to 21 years | 23 | Hospital | Varied |
| (13) | Venable (2005) | USA | Qualitative | Exit survey | 16 years (mean age) | Not specified | Juvenile detention | Art |
| (14) | Veronese, Cavazzoni, and Antenucci (2018) | Occupied Palestinian Territories | Qualitative | Thematic analysis of children's art/writing | 6–15 years | 122 | Refugee camps | Art, writing |
| (15) | Winn (2012) | USA | Qualitative | Thematic analysis of adolescent girls' writing | 14–17 years | Not specified | Juvenile detention | Writing |
Note. All studies met inclusion criteria for involving children ≤18 years, though in two studies (2 and 12), the maximum age of participants was 21 years.
Indicates article found via handsearching.
Most studies employed a qualitative methodology (n = 11), with few quantitative (n = 3) and one mixed methods study. Studies were conducted in the United States (n = 9) and Canada (n = 2) and one study each from Australia, Ireland, Israel and Palestine. Participants' ages ranged from 5 months to 21 years, and sample sizes ranged from 1 to 295. Eleven studies conducted their research with children (N = 527 individuals), two studies conducted research with families (N = 22 families) and two studies did not provide information regarding sample size.
Studies were conducted in various types of restricted environments, including hospitals (n = 7), juvenile (n = 4) and immigration (n = 3) detention centres and a refugee camp (n = 1). Our search did not identify studies investigating restricted environment due to a disease outbreak. Of the studies that reported on duration (n = 7), the length of time participants spent in restricted environments ranged from 48 h to 330 days.
5.1. Play amidst restrictions
The 15 included studies covered various play‐related activities, including sand play (4), puppet play (7), toy play (5), rule‐based games (11), art (6, 13 and 14), reading (9), writing (9, 14 and 15) and music (1 and 10). Three studies discussed children's play opportunities but lacked specific information about particular play activities (2, 3 and 8).
The role of play differed across studies: in some studies, play was used as a tool (10, 11, 13 and 14) (e.g. using play‐related activities, such as music, creative writing and painting, as a method of study engagement or behavioural intervention), whereas in others, play was the outcome of interest (2, 8, 9 and 12) (e.g. considering how play‐related behaviours are affected by restrictions). In many papers, play featured as both a tool and outcome (1, 3–7 and 14) whereby play‐based methods such as art (6 and 14) or puppet play (7) were implemented, and the resulting playful performance or creation was studied as the outcome.
The following themes relating to play amidst restrictive conditions were identified: access to play, frequency of play, play as a means of expression, play and social connectivity, play to promote coping and play for skill development. These themes are explored within the context of our research questions.
5.2. How might quarantine or restricted environments affect play in children and young people?
Overall, nine studies addressed how restricted environments may affect children's play experiences. The included literature described the impact of restrictions on children's access to and frequency of engaging in play, as well as on expressiveness and social connectedness through play. These studies spanned various settings: hospital (2, 6 and 12), immigration detention (3, 4 and 8), juvenile detention (9 and 15) and refugee camps (14).
The impact on children's access to play was illustrated in the context of those living in immigration detention centres (3 and 8) or refugee camps (14). These environments were described as lacking appropriate play spaces and resources: children lived in barren areas scattered with stones and razor wire, with minimal access to toys (14) or toys that were not age appropriate (8). There were reports that children experienced poor living conditions, remained idle, lacked social interaction for long periods and could not play outdoors due to lack of weather‐appropriate clothing (3). Some parents expressed how children were exposed to violence during confinement (8 and 14), diminishing younger children's inclination to play and creating an additional source of trauma. Disrupted access to play was also apparent in a hospital‐based study (6) where children reported wanting more play spaces and resources during long‐term hospitalization. Through drawings and interviews, children indicated what was important to them while required to stay in hospital including increased diversity of activities, more shared spaces and more resources for play, games and entertainment.
We identified two studies that included an examination of frequency of play behaviour, both of which centred upon hospitalized children undergoing chemotherapy (2 and 12). One study found that play behaviours remained constant across 6 weeks of observation (2); however, another found that play fluctuated during medical isolation, with younger participants being less likely to experience these changes (12). In the latter study, play encompassed a variety of behaviours across the broad age range of participants (18 months to 21 years), including reading, writing, crafts, watching television and completing schoolwork. Via hospital observations, the authors reported that 8 of 18 participants showed changes in play frequency during their hospitalization and periods of isolation.
Four studies emphasized play as a means of expression to gain insight into effects upon children's experiences of restriction or isolation (4, 9, 14 and 15). In a study based in an immigration detention centre (4), researchers engaged children in play as an age‐appropriate means of sharing lived experiences. Their play behaviours contained themes of confinement, surveillance, violence and loss of protection and notably lacked concepts of school or friends, which are usually associated with children's play. In another study of people within a refugee camp (14), children's drawings and written creations featured concepts such as political resistance and violence, reflecting the unique experience of living within that constrained environment. Two studies based in juvenile detention centres investigated engagement in reading and writing activities. The content of the expressive activities reflected participants' experiences of being detained, desires for freedom and hopes for a future outside of detention (9 and 15).
Two studies highlighted ways that restrictive circumstances can affect children's play related to their social connectivity (6 and 9). Hospitalized children conveyed a desire for more social connection and interaction, evidenced by interviews and children's drawings depicting people together and shared spaces. Children confined to their hospital rooms reported that they had few opportunities for socializing and that they wanted access to technology for communication (e.g. a computer with a camera) (6). In a case study of a young girl in juvenile detention, reading and letter‐writing activities with others in the centre reflected her longing for social connection and allowed her to form and foster relationships amidst isolation (9).
5.3. In what ways might play and related activities mitigate the impact of quarantine and restriction on children's health and education?
In total, we identified 10 studies relevant to the question of how play might mitigate the effects of quarantine or restriction on children's outcomes. Five papers considered play as a means of expression and play to promote coping (1, 7, 10, 14 and 15), highlighting ways in which play may help children express themselves and endure challenges when facing restrictive situations. In a study that described the use of therapeutic puppet play with a young bone marrow transplant patient in medical isolation, play sessions were described as helping the child to share concerns and fears about his confinement and abandonment and cope with some of the challenging aspects of his medical restrictions (7). Two studies investigated the use of music to help children to cope with the stress of prolonged hospitalization (1 and 10). Brodsky (1) reported that when given the opportunity to engage with musical outlets, children wrote lyrics and sang about their personal circumstances. The author suggested that children need to talk about their hospital experiences to cope with them and that musical play enables patients to express feelings, feel a sense of control and find moments of solace or hope. Similarly, Robb (10) conducted an observational study exploring the use of music to enhance children's coping. This study reported that engagement in music therapy helped create a supportive environment within which children could be in control and expressive, proposing that such playful contexts allowed children to better cope with the stressors of the hospital setting.
A qualitative study conducted in a refugee camp used writing and drawing as playful methods to explore children's experiences (14). The authors contended that this type of play offered children a sense of agency, competence and control over their restrictive environment. Through their creations, participants also shared ideas of hope for their futures and considered outcomes beyond their current circumstances. Furthermore, research regarding the content of detainees' playscripts in juvenile detention reported that girls were able to express their thoughts and desires for the future through playwriting, inferring that the creative process was used as an outlet for problem solving and perseverance (15).
One hospital‐based study implemented an intervention to improve children's access to play through the installation of play cabinets to combat a lack of play materials for children who had undergone bone marrow transplantation (5). These young patients must be kept in a sterile, isolated environment for extended periods. The knowledge required for selection of age‐appropriate toys and the time needed to sterilize toys and engage the child in playful experiences were identified as potential barriers to children freely accessing play during hospital isolation. According to two described cases of children's experiences with play cabinet materials, increasing access to play during isolation allowed for more physical and mental activity, reduced boredom and loneliness and engaged children in sharing feelings and decision‐making regarding their environment and routine.
Three papers considered ways in which play for skill development might assuage difficult aspects of restricted environments (5, 11 and 13). One study used play as part of an occupational therapy programme for youth in juvenile detention centres (11). The study aimed to promote the acquisition of life skills through playful methods including group games and discussions, worksheets and craft activities. Play activities were selected based on the belief that limited opportunities to play faced by incarcerated youth may increase feelings of isolation and hamper development. Some participants communicated that the play activities allowed them to express their feelings, hear about others' situations and gain a better understanding of self and encouraged them to think about making changes in their lives to improve their own outcomes. The authors suggested that these play activities promoted self‐awareness and positive personal reflections (11). Another study conducted in a juvenile detention facility focused on a programme to create an art mural (13): art teachers noted developments in skills that were taught as part of the programme, and the author suggested that fostering a creative skill set could facilitate learning in other academic areas, although this was not explicitly studied. In the study on the use of play cabinets in hospital (5), toys were selected for promoting social, fine motor, language and gross motor skills, with the purpose of helping children achieve developmental milestones despite restriction.
Four studies examined possible support stemming from play and social connectivity in restricted environments (5, 6, 9 and 13). Two studies provided information about children's social behaviours in juvenile detention, as they engaged in reading and letter‐writing (9) and art activities (13). In a case study of an adolescent girl, engaging in reading and writing activities was associated with perceived increases in social opportunities and connections (9). In the study of young detainees participating in an art mural project, that activity reportedly provided them with opportunities for socialization and developing positive relationships with peers (13). In a hospital setting, Kuntz et al. (5) stressed the importance of play for developing and maintaining children's social skills and for preparing them for later discharge and return to a typical, non‐restrictive setting. Similarly, Lambert et al. (6) recognized that children not only sought social connection outside of the hospital but were also eager for playful social interaction within the hospital community.
6. DISCUSSION
This rapid review is the first to map literature on the impact of restrictive environments on children's play experiences and on ways in which play may mitigate the adverse effects of such restrictions. Fifteen published, peer‐reviewed studies were included, spanning various conditions and environments under which children faced restriction. None were related to home confinement.
The first research question addressed how restrictive environments affect children's play. The included literature provides evidence that children's access to play can be impacted by quarantine or isolation. Barriers to play were identified, such as unsafe spaces, scarcity of toys, lack of interaction with other children and lack of time outdoors, and reports indicated that diminishing opportunities for play were associated with inactivity and boredom among children (Kuntz et al., 1996 [5]; Mares, Newman, Dudley, & Gale, 2002 [8]; Veronese, Cavazzoni, & Antenucci, 2018 [14]). Though frequency of play behaviours was recognized as potentially variable due to restricted conditions, only two studies examined this (Hollenbeck et al., 1980 [2]; Susman et al., 1981 [12]). Both studies were conducted in the context of hospitalization, without a baseline measurement of play frequency. Findings were contradictory, possibly due to different definitions of play and different age ranges of participants—variables that can considerably affect children's particular interests and capabilities.
Overall, relatively few studies characterized changes in the nature of children's play in restrictive environments. Most included studies were qualitative and varied greatly in terms of sample size, methodology and the type of play referenced. At present, the field lacks a detailed understanding of how play may be changed in response to restrictive circumstances and how children engage with such alterations. This gap emphasizes the pressing need to collect data from specific vulnerable populations, including children, during the current pandemic (Holmes et al., 2020).
The second research question considered how children's engagement in play behaviours may mitigate negative impacts of restriction. Although some studies alluded to mechanisms through which play might support children during quarantine or isolation (e.g. via coping, social connectivity and self‐expression), these mechanisms were not explicitly evaluated. Most studies were qualitative, providing valuable insights on the perceived benefits of play in restrictive conditions, especially from the perspectives of children. These findings suggest that play may have a role in attenuating the negative effects of restrictive environments, yet underscore the need for further research to test this hypothesis robustly.
We identified key themes pertaining to the ways in which play may benefit or protect child outcomes during times of restriction, including providing opportunities for socialization. In the studies involving adolescents in juvenile detention centres, engagement in creative, expressive activities afforded opportunities for social connectivity and development of social skills, which is particularly important during early adolescence (Waldrip, Malcolm, & Jensen‐Campbell, 2008). Children restricted to hospital environments also expressed a desire for more social connectivity via drawings depicting play areas, friends, shared spaces and technological activities for play and communication (Lambert, Coad, Hicks, & Glacken, 2014 [6]). Sociability is related to stress resilience in children (Zolkoski & Bullock, 2012), and using play to promote socialization may serve as a protective factor for children in isolation. In the midst of school closures, home quarantine, closed play areas and gathering restrictions throughout the COVID‐19 pandemic, children may welcome the advantages that technology provides for social connectivity in the absence of face‐to‐face interaction (Goldschmidt, 2020).
Play also affords opportunities for self‐expression. Creative and arts‐based activities were prominent in studies addressing our second research question. Evidence from the wider literature suggests that creative or expressive activities used in therapeutic and classroom settings provide children with opportunities to communicate personal accounts, interact with others and express emotion (Schaefer, 1993; Tyrer & Fazel, 2014). A systematic review conducted with refugee and asylum‐seeking children suggests that creative arts‐based interventions may help to reduce emotional and relational problems as well as post‐traumatic stress and depression symptoms and improve well‐being and self‐esteem (Tyrer & Fazel, 2014). In certain studies, such expressive play and creativity‐based activities were used as a method to engage children in research about their functioning and well‐being amidst restrictions. For example, Kronick et al. (2018 [4]) used sand play as a narrative enquiry methodology to capture the experiences of migrant children living in detention. Play‐based methods of data collection (e.g. draw and talk methods, vignettes and creative writing) may serve as an effective, age‐appropriate means of helping children share their perspectives on their lived experiences and express their feelings about it. Playful engagement in research can be particularly appropriate for younger children for whom play is a natural way to communicate and engage with their worlds (Thomas & O'Kane, 1998).
This rapid review is not without limitations. The review was conducted in a short timeframe to reflect the rapidity of the current pandemic and its associated effects, which limited the scope of the search strategy. Additional keywords may have yielded further relevant research, such as terms targeting particular infectious diseases and pandemics, or online play and games (likely relevant to adolescents' play and to children's current at‐home play behaviours). Notably, none of the included studies directly examined the impact of social or gathering restrictions on play due to infectious disease outbreak. A possible explanation for this is that global infectious and respiratory diseases disproportionately affect populations in developing countries, with places of widespread poverty and low‐income countries more often facing a higher disease burden (Dupas, 2011; Griffiths, 2012; Gupta & Guin, 2010). Expanding the search to include grey literature may have identified more relevant studies. For example, the views and voices of children affected by the Ebola crisis have been summarized in organizational reports by Save the Children (Kostelny et al., 2016; Risso‐Gill & Finnegan, 2015). Children in Sierra Leone affected by Ebola and who experienced restrictions as a result of that crisis, such as school closure, social distancing and household quarantine, reported that they missed playing, seeing their friends and that they felt unhappy, lonely and trapped. Such information is pertinent to understanding how play might be important in alleviating negative aspects of virus‐related isolation on children's well‐being. Finally, there may have been additional factors in the studies identified, relating to the reasons that children were facing restrictions, which impacted on their play experiences (e.g. drug toxicity in children isolated for cancer treatment, or history drug use and violence of those held in juvenile detention; Susman et al., 1981 [12]; Winn, 2012 [15]). This may limit the generalizability of findings to the current pandemic.
7. CONCLUSIONS AND NEXT STEPS
This rapid review describes literature regarding the impact of quarantine or other isolating circumstances on children's play behaviours and how play might mitigate resulting adverse effects on children's health outcomes. There remain significant gaps in understanding how play is affected by restrictive circumstances and the subsequent influence on children's health and education, especially during lockdown conditions due to an infectious disease outbreak. Findings indicated that children's access to play can be impacted by restrictive situations, though in the context of the current health crisis, children are not explicitly prevented from playing; rather, it is likely that play behaviours have needed to alter and adapt in light of lockdowns, necessary quarantines or requisite distancing. Although there are strong reasons to believe that the frequency of children's play behaviours would change as a result of lockdown, the dearth of available research does not allow for a substantial claim to be made in this regard. The papers included in this review alluded to potential pathways through which play may support children during isolation; however, none directly examined these relationships. To improve our collective understanding of how to appropriately care for children during this, and future, health crises, it is vital that we prioritize high‐quality research that directly investigates play during restrictive and lockdown conditions.
Notably absent from this literature search was research that investigated play and quarantine in long‐term, disease‐outbreak‐related situations that could provide insights regarding the integrity of play amidst the current pandemic. This gap emphasizes the pressing need to collect data from children directly in the context of other restrictive situations. It is imperative that children are given a voice and, critically, that their voices are listened to and valued. Future research that could guide both policy and practice could include studies that
engage children directly, soliciting their perceptions, opinions and priorities about their play experiences during lockdown restrictions;
compare contexts where restrictions to play are lifted at different times (e.g. access to schools, playgrounds and eased social distancing regulations) and/or examine the impact of policies that allow changes to play opportunities (e.g. where families can isolate together);
identify families' expressed priorities and needs regarding play and evaluate strategies or interventions to achieve this; and
identify the impact of recent large‐scale initiatives to support play in crisis situations (e.g. BRAC Play Labs; PlayMatters).
Acknowledging the importance of play in moments of crisis is critical for understanding how children's worlds are affected by quarantine, isolation and other environmental restrictions. Empirical evidence is needed to guide policymakers as they navigate decision‐making around the imminent post‐lockdown state, future restrictions and new outbreaks.
CONFLICT OF INTERESTS
There are no conflicts of interest to declare.
FUNDING INFORMATION
All authors work at the PEDAL Research Centre at the University of Cambridge, which receives philanthropic funding from the LEGO Foundation. The funder played no part in the direction or execution of this research.
AUTHOR CONTRIBUTIONS
Professor Ramchandani conceived of the idea for this rapid review. All authors contributed to the conceptualization and planning of the protocol and search strategy. Kelsey Graber was responsible for the overall team, time and data management. She, along with Dr. Byrne, Emily Goodacre, Natalie Kirby and Krishna Kulkarni, conducted the database searches, article screening and data extraction. Kelsey Graber took the lead in writing the manuscript alongside Dr. Byrne; Emily Goodacre, Natalie Kirby and Krishna Kulkarni contributed significantly to writing and editing the text. Dr. Byrne, Dr. O'Farrelly and Professor Ramchandani provided critical input, feedback and consultation throughout the writing process, in addition to contributing sections of independent writing. All authors reviewed and provided feedback for the final manuscript.
APPENDIX A. SEARCH SYNTAX
| (A) Population of interest: | (child* OR adolescen* OR teenage* OR [paediatric OR pediatric] OR youth OR ‘young people’ OR infan* OR toddler OR preschool OR ‘school age’) |
| AND | |
| (B) Quarantine and restricted environments: | (quarantine OR ‘social distancing’ OR ‘social restriction’ OR ‘patient isolation’ OR confine* OR [lockdown OR ‘lock‐down’ OR curfew] OR ‘deprivation‐isolation’ OR ‘protect* environment’ OR detention OR incarceration) |
| AND | |
| (C) Play and related activities: | (play* OR [art OR arts OR ‘arts‐based’] OR sport* OR exercise OR ‘outdoor activities’ OR ‘outdoor spaces’ OR exploration OR discovery OR toys OR games OR ‘social media’ OR [‘free play’ OR ‘free‐play’] OR ‘adult‐directed activities’ OR drawing OR crafts OR reading OR ‘book sharing’ OR [danc* OR sing* OR fun] OR drama* OR imagin*) |
Optional terms included in iterative search process are as follows:
OR (famil* OR student* OR kindergarten*)
AND (epidemic OR outbreak OR crisis OR pandemic OR separation OR ‘social isolation’ OR ‘extreme weather’ OR flood OR ice storm OR pandemic OR disaster OR ‘natural disaster’ OR war OR ‘war zone’ OR ‘conflict area’ OR [refuge* OR immigra*] OR [SARS OR ‘severe acute respiratory syndrome’] OR [H1N1 OR ‘swine flu’ OR ‘swine influenza’] OR [MERS OR ‘Middle East respiratory syndrome’ OR ‘Middle East Respiratory Syndrome Coronavirus’ OR ‘MERS‐CoV’] OR ‘influenza pandemic’ OR ‘equine influenza’ OR ‘infectious disease’ OR virus OR ‘viral infection’ OR ‘contagious disease’ OR [coronavirus* OR coronavirus infections OR COVID‐19 OR SARS‐Cov‐2]).
Graber KM, Byrne EM, Goodacre EJ, et al. A rapid review of the impact of quarantine and restricted environments on children's play and the role of play in children's health. Child Care Health Dev. 2021;47:143–153. 10.1111/cch.12832
DATA AVAILABILITY STATEMENT
Data sharing is not applicable to this article as no new data were created or analysed in this study.
REFERENCES
- Andrew, A. , Cattan, S. , Costa‐Dias, M. , Farquharson, C. , Kraftman, L. , Krutikova, S. , … Sevilla, A. (2020). Learning during the lockdown: Real‐time data on children's experiences during home learning. [DOI] [PMC free article] [PubMed]
- Armitage, R. , & Nellums, L. B. (2020). Considering inequalities in the school closure response to COVID‐19. The Lancet Global Health, 8(5), e644. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7195275/pdf/main.pdf, 10.1016/S2214-109X(20)30116-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Berkman, B. E. (2008). Mitigating pandemic influenza: The ethics of implementing a school closure policy. Journal of Public Health Management and Practice, 14(4), 372–378. Retrieved from <Go to ISI>://WOS:000256855500010 [DOI] [PubMed] [Google Scholar]
- Brodsky, W. (1989). Music therapy as an intervention for children with cancer in isolation rooms. Music Therapy, 8(1), 17–34. 10.1093/mt/8.1.17 [DOI] [Google Scholar]
- Brooks, S. K. , Webster, R. K. , Smith, L. E. , Woodland, L. , Wessely, S. , Greenberg, N. , & Rubin, G. J. (2020). The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet, 395(10227), 912–920. 10.1016/S0140-6736(20)30460-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chatterjee, S. (2018). Children's coping, adaptation and resilience through play in situations of crisis. Children, Youth and Environments, 28(2), 119–145. 10.7721/chilyoutenvi.28.2.0119 [DOI] [Google Scholar]
- Clark, H. , Coll‐Seck, A. M. , Banerjee, A. , Peterson, S. , Dalglish, S. L. , Ameratunga, S. , … Costello, A. (2020). After COVID‐19, a future for the world's children? The Lancet, 396(10247), 298–300. 10.1016/S0140-6736(20)31481-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cohen, E. , & Gadassi, R. (2018). The function of play for coping and therapy with children exposed to disasters and political violence. Current Psychiatry Reports, 20(5), 31. 10.1007/s11920-018-0895-x [DOI] [PubMed] [Google Scholar]
- Dong, Y. , Mo, X. , Hu, Y. , Qi, X. , Jiang, F. , Jiang, Z. , & Tong, S. (2020). Epidemiology of COVID‐19 among children in China. Pediatrics, 145(6), e20200702. 10.1542/peds.2020-0702 [DOI] [PubMed] [Google Scholar]
- Dupas, P. (2011). Health behavior in developing countries. Annual Review of Economics, 3(1), 425–449. 10.1146/annurev-economics-111809-125029 [DOI] [Google Scholar]
- Fore, H . (2020). Don't let children be the hidden victims of COVID‐19 pandemic [Press release]. Retrieved from https://www.unicef.org/press-releases/dont-let-children-be-hidden-victims-covid-19-pandemic
- Ganann, R. , Ciliska, D. , & Thomas, H. (2010). Expediting systematic reviews: Methods and implications of rapid reviews. Implementation Science, 5, 10–19. Artn 56. 10.1186/1748-5908-5-56 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Goldschmidt, K. (2020). The COVID‐19 pandemic: Technology use to support the wellbeing of children. Journal of Pediatric Nursing, 53, 88–90. 10.1016/j.pedn.2020.04.013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Griffiths, S. (2012). Chapter 1: Why research infectious diseases of poverty. Global report for research on infectious diseases of poverty, 1–34.
- Guan, H. , Okely, A. D. , Aguilar‐Farias, N. , del Pozo Cruz, B. , Draper, C. E. , el Hamdouchi, A. , … Veldman, S. L. C. (2020). Promoting healthy movement behaviours among children during the COVID‐19 pandemic. The Lancet Child & Adolescent Health, 4, 416–418. 10.1016/S2352-4642(20)30131-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gupta, I. , & Guin, P. (2010). Communicable diseases in the South‐East Asia Region of the World Health Organization: Towards a more effective response. Bulletin of the World Health Organization, 88, 199–205. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2828785/pdf/09-065540.pdf, 10.2471/BLT.09.065540 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hollenbeck, A. R. , Susman, E. J. , Nannis, E. D. , Strope, B. E. , Hersh, S. P. , Levine, A. S. , & Pizzo, P. A. (1980). Children with serious illness: Behavioural correlates of separation and isolation. Child Psychiatry and Human Development, 11(1), 3–11. 10.1007/BF00705865 [DOI] [PubMed] [Google Scholar]
- Holmes, E. A. , O'Connor, R. C. , Perry, V. H. , Tracey, I. , Wessely, S. , Arseneault, L. , … Bullmore, E. (2020). Multidisciplinary research priorities for the COVID‐19 pandemic: A call for action for mental health science. The Lancet Psychiatry, 7, 547–560. 10.1016/S2215-0366(20)30168-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hutchins, S. S. , Truman, B. I. , Merlin, T. L. , & Redd, S. C. (2009). Protecting vulnerable populations from pandemic influenza in the United States: A strategic imperative. American Journal of Public Health, 99, S243–S248. 10.2105/Ajph.2009.164814 [DOI] [PMC free article] [PubMed] [Google Scholar]
- International Play Association (2017). Access to play for children in situations of crisis. Retrieved from http://ipaworld.org/wp-content/uploads/2017/07/IPA-A4-ACCESS-TO-PLAY-IN-SITUATIONS-OF-CRISIS-TOOLKIT-LR.pdf
- International Play Association (2020). The importance of playing during a crisis. Retrieved from http://ipaworld.org/wp-content/uploads/2020/04/APC1-The-importance-of-playing-during-a-crisis.pdf
- Kostelny, K. , Lamin, D. , Manyeh, M. , Ondoro, K. , Stark, L. , Lilley, S. , & Wessells, M. (2016). ‘Worse than the war’: An ethnographic study of the impact of the Ebola crisis on life, sex, teenage pregnancy, and a community‐driven intervention in rural Sierra Leone. London: Save the Children. [Google Scholar]
- Kronick, R. , Rousseau, C. , & Cleveland, J. (2015). Asylum‐seeking children's experiences of detention in Canada: A qualitative study. The American Journal of Orthopsychiatry, 85(3), 287–294. 10.1037/ort0000061 [DOI] [PubMed] [Google Scholar]
- Kronick, R. , Rousseau, C. , & Cleveland, J. (2018). Refugee children's sandplay narratives in immigration detention in Canada. European Child & Adolescent Psychiatry, 27(4), 423–437. 10.1007/s00787-017-1012-0 [DOI] [PubMed] [Google Scholar]
- Kuntz, N. , Adams, J. A. , Zahr, L. , Killen, R. , Cameron, K. , & Wasson, H. (1996). Therapeutic play and bone marrow transplantation. Journal of Pediatric Nursing, 11(6), 359–367. 10.1016/S0882-5963(96)80080-7 [DOI] [PubMed] [Google Scholar]
- Lambert, V. , Coad, J. , Hicks, P. , & Glacken, M. (2014). Social spaces for young children in hospital. Child: Care, Health and Development, 40(2), 195–204. 10.1111/cch.12016 [DOI] [PubMed] [Google Scholar]
- Landrigan, P. J. (2005). Children as a vulnerable population (reprinted from the European Journal of Oncology Library, vol 2, 2003). Human and Ecological Risk Assessment, 11(1), 235–247. 10.1080/10807030590920051 [DOI] [Google Scholar]
- Linn, S. , Beardslee, W. , & Patenaude, A. F. (1996). Puppet therapy with pediatric bone marrow transplant patients. Journal of Pediatric Psychiatry, 11(1), 37–46. [DOI] [PubMed] [Google Scholar]
- Loades, M. E. , Chatburn, E. , Higson‐Sweeney, N. , Reynolds, S. , Shafran, R. , Brigden, A. , … Crawley, E. (2020). Rapid Review: The impact of social isolation and loneliness on the mental health of children and adolescents in the context of COVID‐19. Retrieved from osf.io/p8q3d [DOI] [PMC free article] [PubMed]
- Mares, S. , Newman, L. , Dudley, M. , & Gale, F. (2002). Seeking refuge, losing hope: Parents and children in immigration detention. Australasian Psychiatry, 10(2), 91–96. 10.1046/j.1440-1665.2002.00414.x [DOI] [Google Scholar]
- Nijhof, S. L. , Vinkers, C. H. , van Geelen, S. M. , Duijff, S. N. , Achterberg, E. J. M. , van der Net, J. , … Lesscher, H. M. B. (2018). Healthy play, better coping: The importance of play for the development of children in health and disease. Neuroscience and Biobehavioral Reviews, 95, 421–429. 10.1016/j.neubiorev.2018.09.024 [DOI] [PubMed] [Google Scholar]
- Pytash, K. E. (2013). “I'm a reader”: Transforming incarcerated girls' lives in the English classroom. English Journal, 67–73.24902395 [Google Scholar]
- Ramchandani, P. (2020). Covid‐19: We can ward off some of the negative impacts on children. NewScientist (3277). Retrieved from https://institutions.newscientist.com/article/mg24532773-000-covid-19-we-can-ward-off-some-of-the-negative-impacts-on-children/ [Google Scholar]
- Ren, X. (2020). Pandemic and lockdown: A territorial approach to COVID‐19 in China, Italy and the United States. Eurasian Geography and Economics, 1–12. 10.1080/15387216.2020.1762103 [DOI] [Google Scholar]
- Risso‐Gill, I. , & Finnegan, F. (2015). Children's Ebola recovery assessment. Sierra Leone: Save the Children Fund. World Vision International, Plan International, UNICEF. [Google Scholar]
- Robb, S. L. (2000). The effect of therapeutic music interventions on the behavior of hospitalized children in isolation: Developing a contextual support model of music therapy. Journal of Music Therapy, 37(2), 118–146. Retrieved from https://pubmed.ncbi.nlm.nih.gov/10932125/, 10.1093/jmt/37.2.118 [DOI] [PubMed] [Google Scholar]
- Roberton, T. , Carter, E. D. , Chou, V. B. , Stegmuller, A. R. , Jackson, B. D. , Tam, Y. , … Walker, N. (2020). Early estimates of the indirect effects of the COVID‐19 pandemic on maternal and child mortality in low‐income and middle‐income countries: A modelling study. The Lancet Global Health, 8, e901–e908. 10.1016/S2214-109X(20)30229-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schaefer, C. E. (1993). The therapeutic powers of play. Lanham, Maryland, USA: Jason Aronson. [Google Scholar]
- Shea, C.‐K. , & Siu, A. M. H. (2016). Engagement in play activities as a means for youth in detention to acquire life skills. Occupational Therapy International, 23(3), 276–286. 10.1002/oti.1432 [DOI] [PubMed] [Google Scholar]
- Sinha, I. , Bennett, D. , & Taylor‐Robinson, D. C. (2020). Children are being sidelined by covid‐19. British Medical Journal, 369. 10.1136/bmj.m2061 [DOI] [PubMed] [Google Scholar]
- Susman, E. J. , Hollenbeck, A. R. , Nannis, E. D. , Strope, B. E. , Hersh, S. P. , Levine, A. S. , & Pizzo, P. A. (1981). A prospective naturalistic study of the impact of an intensive medical treatment on the social behavior of child and adolescent cancer patients. Journal of Applied Developmental Psychology, 2, 29–47. 10.1016/0193-3973(81)90028-9 [DOI] [Google Scholar]
- Thomas, N. , & O'Kane, C. (1998). The ethics of participatory research with children. Children & Society, 12(5), 336–348. 10.1111/j.1099-0860.1998.tb00090.x [DOI] [Google Scholar]
- Tyrer, R. A. , & Fazel, M. (2014). School and community‐based interventions for refugee and asylum seeking children: A systematic review (vol 9, e89359, 2014). PLoS ONE, 9(5), e97977. 10.1371/journal.pone.0097977 [DOI] [PMC free article] [PubMed] [Google Scholar]
- United Nations . (2020). Policy brief: The impact of COVID‐19 on children. Retrieved from https://unsdg.un.org/sites/default/files/2020-04/160420_Covid_Children_Policy_Brief.pdf
- United Nations Committee on the Rights of the Child (UNCRC) (2013). General comment No. 17 on the right of the child to rest, leisure, play, recreational activities, cultural life and the arts (art. 31). Retrieved from https://www.refworld.org/docid/51ef9bcc4.html
- Venable, B. B. (2005). At‐risk and in‐need: Reaching juvenile offenders through art. Art Education, 58(4), 48–53. 10.1080/00043125.2005.11651552 [DOI] [Google Scholar]
- Veronese, G. , Cavazzoni, F. , & Antenucci, S. (2018). Narrating hope and resistance: A critical analysis of sources of agency among Palestinian children living under military violence. Child: Care, Health and Development, 44(6), 863–870. 10.1111/cch.12608 [DOI] [PubMed] [Google Scholar]
- Waldrip, A. M. , Malcolm, K. T. , & Jensen‐Campbell, L. A. (2008). With a little help from your friends: The importance of high‐quality friendships on early adolescent adjustment. Social Development, 17(4), 832–852. 10.1111/j.1467-9507.2008.00476.x [DOI] [Google Scholar]
- Winn, M. T. (2012). The politics of desire and possibility in urban playwriting: (Re)reading and (re)writing the script. Pedagogies: An International Journal, 7(4), 317–332. 10.1080/1554480X.2012.715737 [DOI] [Google Scholar]
- World Health Organization (2020). Coronavirus disease (COVID‐2019) situation reports. Retrieved from https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports
- Xie, X. , Xue, Q. , Zhou, Y. , Zhu, K. , Liu, Q. , Zhang, J. , & Song, R. (2020). Mental health status among children in home confinement during the coronavirus disease 2019 outbreak in Hubei Province, China. JAMA Pediatrics, 174, 898–900. 10.1001/jamapediatrics.2020.1619 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yogman, M. , Garner, A. , Hutchinson, J. , Hirsh‐Pasek, K. , Golinkoff, R. M. , Committee On Psychosocial Aspects Of, C , & Council On Communications And Media (2018). The power of play: A pediatric role in enhancing development in young children. Pediatrics, 142(3), e20182058. 10.1542/peds.2018-2058 [DOI] [PubMed] [Google Scholar]
- Zolkoski, S. M. , & Bullock, L. M. (2012). Resilience in children and youth: A review. Children and Youth Services Review, 34(12), 2295–2303. 10.1016/j.childyouth.2012.08.009 [DOI] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Data sharing is not applicable to this article as no new data were created or analysed in this study.