
FIGURE 3.
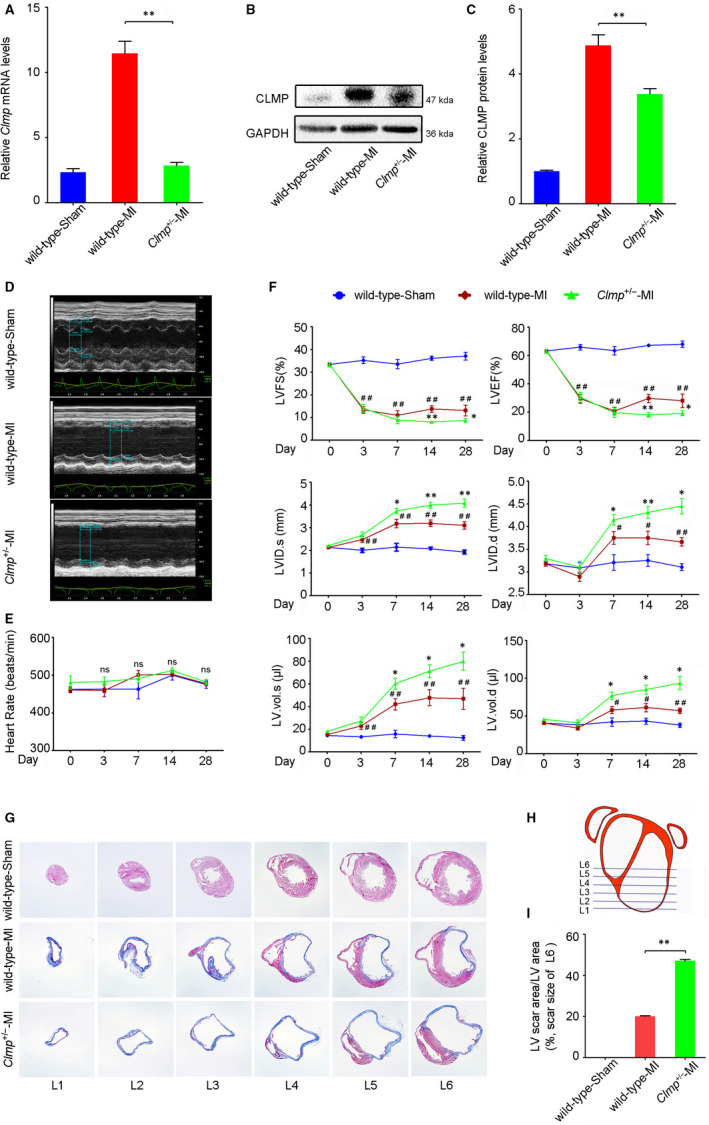
Clmp deficiency further deteriorates the ventricular function after MI injury. A, B, Compared with the wild‐type MI LV, Clmp +/− MI LV showed decreased Clmp mRNA and protein levels detected by qRT‐PCR and Western blot, respectively. C, The relative densitometric quantification of panel B. D, The representative M‐mode echocardiographic images at week 4 after MI (n = 15 per group) indicated more severe cardiac dysfunction in the Clmp +/− MI mice. E, The heart rates among three groups on days 0, 3, 7, 14 and 28 post‐MI. F, The transthoracic echocardiographic analyses were performed on days 0, 3, 7, 14 and 28 post‐MI. LVFS: left ventricular fractional shortening; LVEF: left ventricular ejection fraction; LVID.s: left ventricular internal dimension at end systole; LVID.d: left ventricular internal dimension at end diastole; LV.vol.s: left ventricular volume at end systole; LV.vol.d: left ventricular volume at end diastole. Two‐way repeated‐measures ANOVA; *P < .05 and **P < .01 (wild‐type MI vsClmp +/−‐MI); # P < .05 and ## P < .01 (wild‐type MI vs wild type). G, The representative images of Masson's trichrome in mouse hearts. H, The schematic diagram of serial transverse heart sections for Masson's trichrome staining. I, The quantification of L6 showed a significant increase in fibrosis areas in the Clmp +/− MI heart. All data are presented as the mean ± SEM. One‐way ANOVA; *P < .05; **P < .01