
Figure 1:
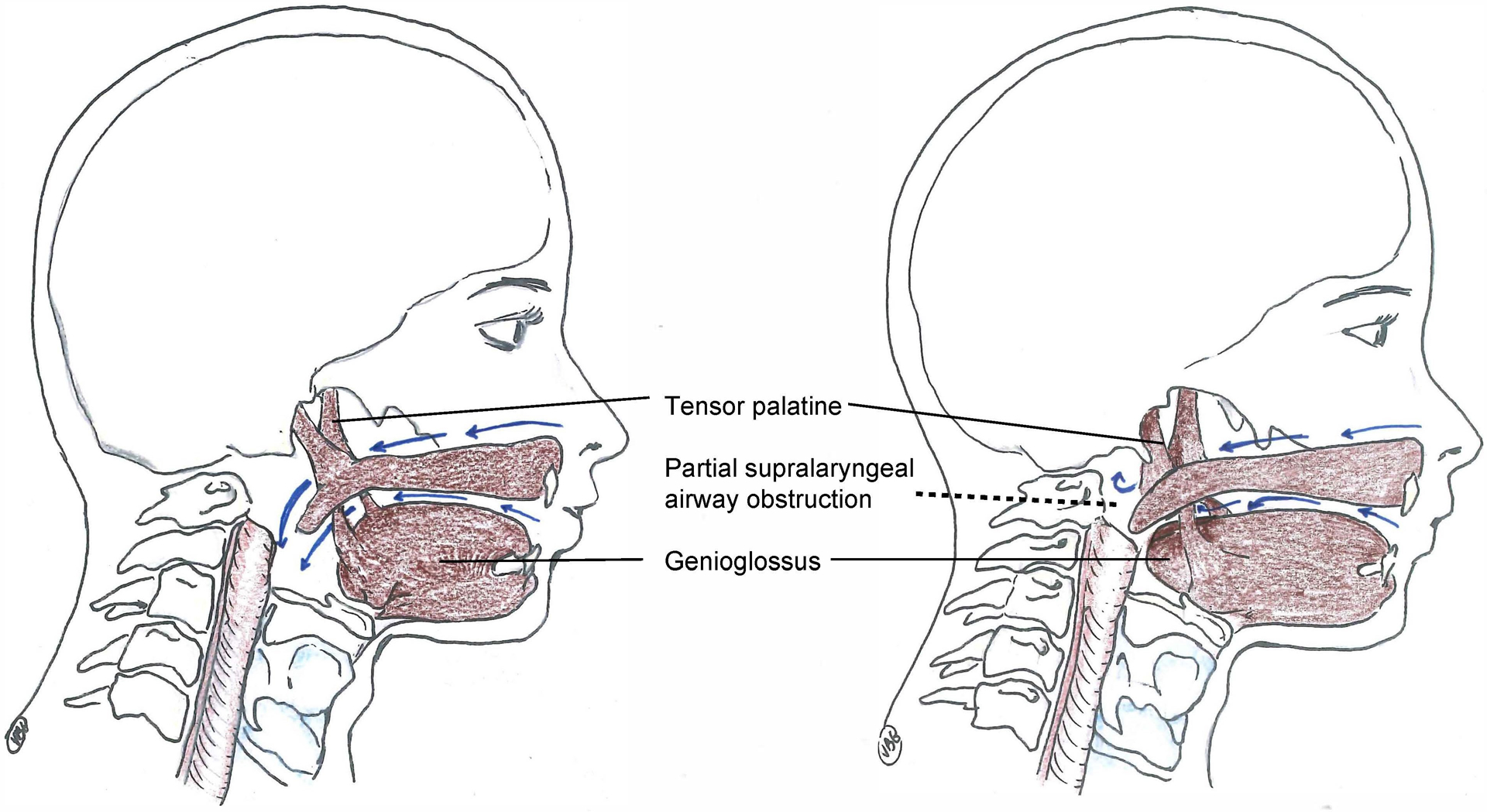
Pharmaco-physiology of upper airway failure during residual neuromuscular blockade.
Minimal residual neuromuscular blockade (train-of-four ratio 0.5–0.95) affects upper airway dilator muscle function which increases the vulnerability of the supralaryngeal airway to collapse during inspiration. The left panel shows a patient with full recovery of neuromuscular transmission. During inspiration, physiological coactivation of the tensor palatine and genioglossus muscles, which occur about 100 milliseconds before the contraction of the respiratory pump muscle (diaphragm), prevent negative inspiratory pressure related upper airway collapse. The right panel demonstrates the pharmaco-physiology during minimal neuromuscular blockade: the negative pressure generated by the diaphragm leads to a complete or partial collapse of the retronasal or retroglossal airway. These effects of residual neuromuscular transmission blockade can be treated with the application of non-invasive ventilation.