
Figure 3. Sodium‐glucose cotransporter type 2 (SGLT2) inhibition and adenosine in healthy patients and those with diabetes mellitus.
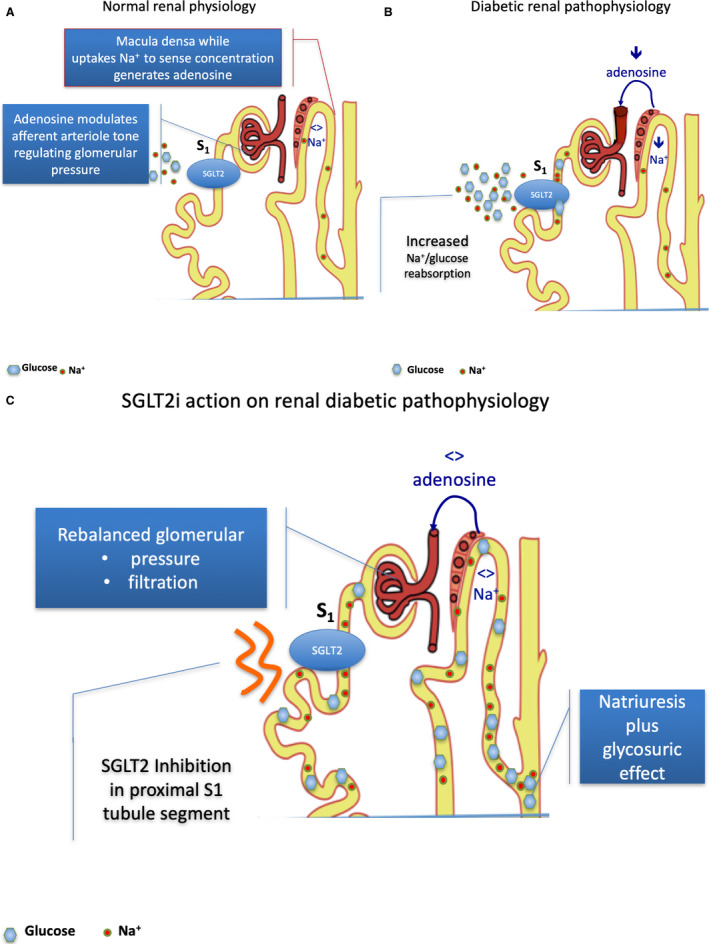
A, Normal renal physiology. The NaCl uptake by dense macula cells (juxtaglomerular apparatus) occurs largely via the Na/K/2Cl cotransporter. It is an energy‐requiring process leading to a breakdown of ATP to adenosine, which has a vasoconstrictive effect. In normal physiology, regular NaCl concentration in urine transit across dense macula (juxtaglomerular apparatus) cells balancing the amount of ATP release and the breakdown to adenosine. Adenosine acts modulating the afferent arteriole tone in relation to normal physiology occurrence. The mechanism is defined as tubular‐glomerular feedback (TGF). Afferent arteriole has a slightly larger diameter in comparison to efferent. The difference assures the intraglomerular pressure gradient to generate urine. Therefore, any vasodilating or vasoconstrictive action in the glomerular vasculature generates a disproportioned relative or absolute decrease in efferent vessel section with a corresponding increase in intraglomerular pressure. B, Diabetic renal pathophysiology. In diabetic renal pathophysiology, a lower urine NaCl concentration is driven by SGLT2‐increased Na+/glucose reabsorption, and therefore a decreased NaCl concentration transit across the dense macula (juxtaglomerular apparatus). The low NaCl concentration is sensed by the dense macula as a low volume, low perfusion state, leading to low adenosine production that induces vasodilating action prevailing on the afferent vessel and causing glomerular hypertension and glomerular hyperfiltration. 57 , 58 Decreased Na+ delivery to the dense macula entails decreased adenosine production with vasodilating effect on afferent glomerular arteriole, enhancing relative disproportion with efferent arteriole section and leading to intraglomerular hypertension and glomerular hyperfiltration. 59 , 60 C, SGLT2 inhibition and glomerular hyperphyltration correction. Selective SGLT2 inhibition by promoting glucose and NaCl. urination increases distal renal NaCl delivery, leading to adenosine production and afferent arteriole tone restoration, thus decreasing intraglomerular pressure and positively affecting hyperfiltration. Restoration of Na+ delivery to the dense macula normalizes adenosine production, reestablishing afferent glomerular arteriole tone and abolishing intraglomerular hypertension and glomerular hyperfiltration.