
Figure 3.
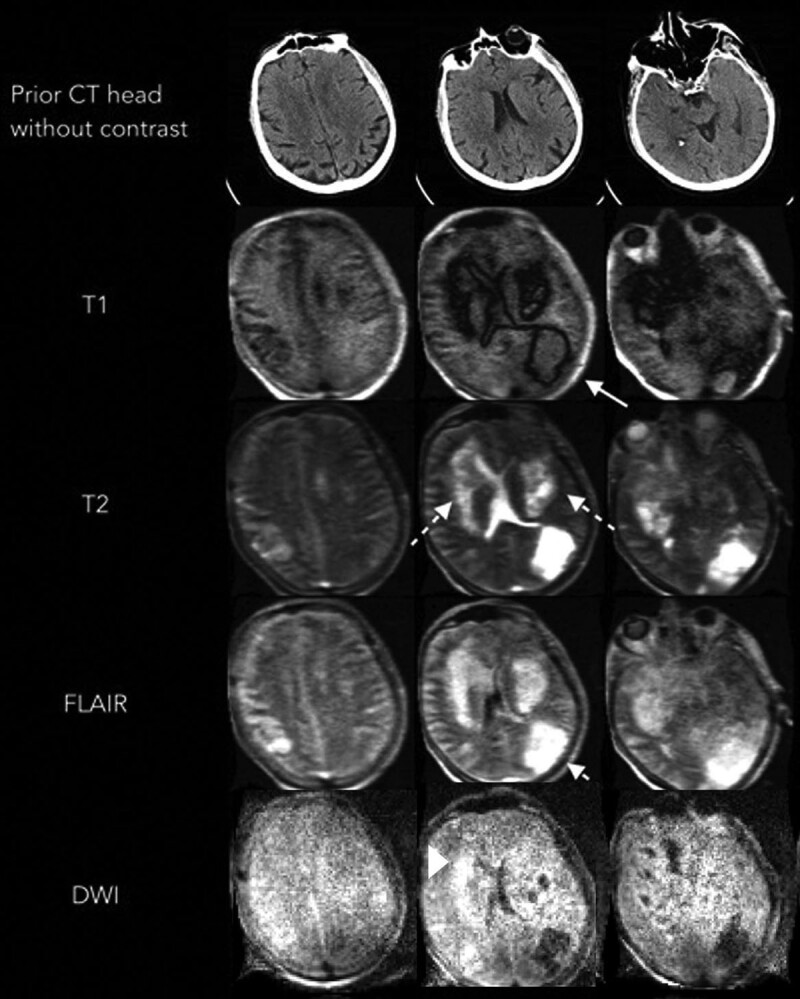
Portable MRI of a critically ill patient with coronavirus disease 2019 (patient illustration 2). A 60-year-old male with a history of coronary artery disease, prior coronary artery bypass grafting on antiplatelet medication, hypertension, and obesity presented with severe hypoxia and was subsequently diagnosed with severe acute respiratory syndrome coronavirus 2. The patient had a prolonged ICU course complicated by seizure, acute respiratory distress syndrome, cardiac arrhythmias requiring anticoagulation, and acute kidney injury requiring hemodialysis. A head CT performed for a poor neurologic examination despite being off sedation revealed no acute findings. Nine days later, a portable MRI demonstrated new areas of low T1 weighted signal surrounding isointense changes in the left parietal occipital region (solid arrow). Extensive high signal was noted on T2 weighted and fluid attenuated inversion recovery (FLAIR) sequences (solid arrow) in the bilateral basal ganglia and left parietal lobe. A concurrent area of restricted diffusion is seen in the basal ganglia on diffusion weighted imaging (DWI). Local mass effect was noted on the left lateral ventricle.