
Figure 14.
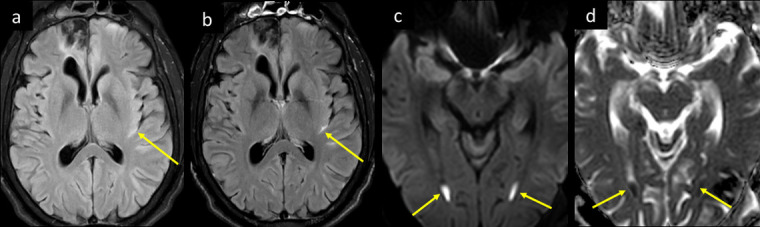
A 27-year-male patient with known post-traumatic seizures on antiepileptic mediations presented to ED with status epilepticus. He was found to be febrile and desaturated, the seizures were aborted, and he was intubated, and tested positive for COVID-19. Plain CT head (not shown) showed right anterior frontal old trauma changes and was otherwise unremarkable. His CSF analysis proved positive for Gram positive Streptococcus pneumonia. MRI head axial images at mid-ventricular level (a) T2-FLAIR before and (b) after i.v. contrast shows bright signal intensity in sylvian fissure, with post-contrast enhancement (long arrows in a and b), consistent with meningitis. Note the post-traumatic right anterior frontal encephalomalacia and gliotic changes (short arrow in a and b). Axial images at lower ventricular level (c) DWI b 1000 and (d) ADC map shows dependent pus with diffusion restriction within the occipital horns of the lateral ventricles bilaterally, representing ventriculitis. ADC, apparent diffusion coefficient; CSF, cerebrospinal fluid; DWI, diffusion-weighted image; ED,emergency department; FLAIR, fluid attenuated inversion recovery.