
Figure 15.
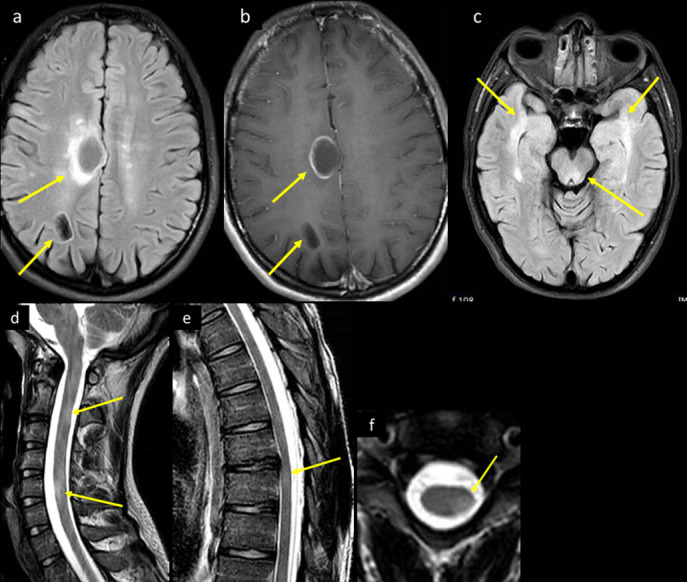
A 25-year-old male with recent history of flu-like illness before 3 weeks presented to the ED with increasing generalized body aches and upper and lower limb weakness. On examination, he had cerebellar signs and ataxia, and mildly decreased power in all 4 limbs of 4/5, with otherwise no focal neurological deficits. His COVID-19 PCR was confirmed positive. Brain CT (not shown) showed bilateral white matter cystic lesions, with surrounding mild vasogenic edema. His CSF analysis showed mildly elevated WBCs with lymphocytic predominance, mildly elevated glucose and protein. CSF culture, viral serology panel, TB PCR and autoimmune work-up were all negative. MRI brain axial (a) FLAIR image at the supraventricular level shows right frontal parasagittal and parietooccipital white matter cystic lesions, with bright intensity marginal changes. (b) Corresponding axial T1 post-i.v. contrast image shows incomplete ring enhancement of the more anterior lesion, and (c) axial FLAIR T2 image at the level of the midbrain shows posterior midbrain and bilateral anterior temporal lobes ill-defined bright signal intensity changes. MRI of the spinal cord sagittal T2 (d) cervical spine and (e) dorsal spine demonstrates multilevel short segment abnormal bright signal intensity (arrows in d and e). (f) Axial T2 image at mid-cervical level demonstrates eccentric localization of the intramedullary lesion (arrow in f). CSF, cerebrospinal fluid; ED, emergency department;FLAIR, fluid attenuated inversion recovery; PCR, polymerasechain reaction; TB, tuberculosis.