
Figure 1.
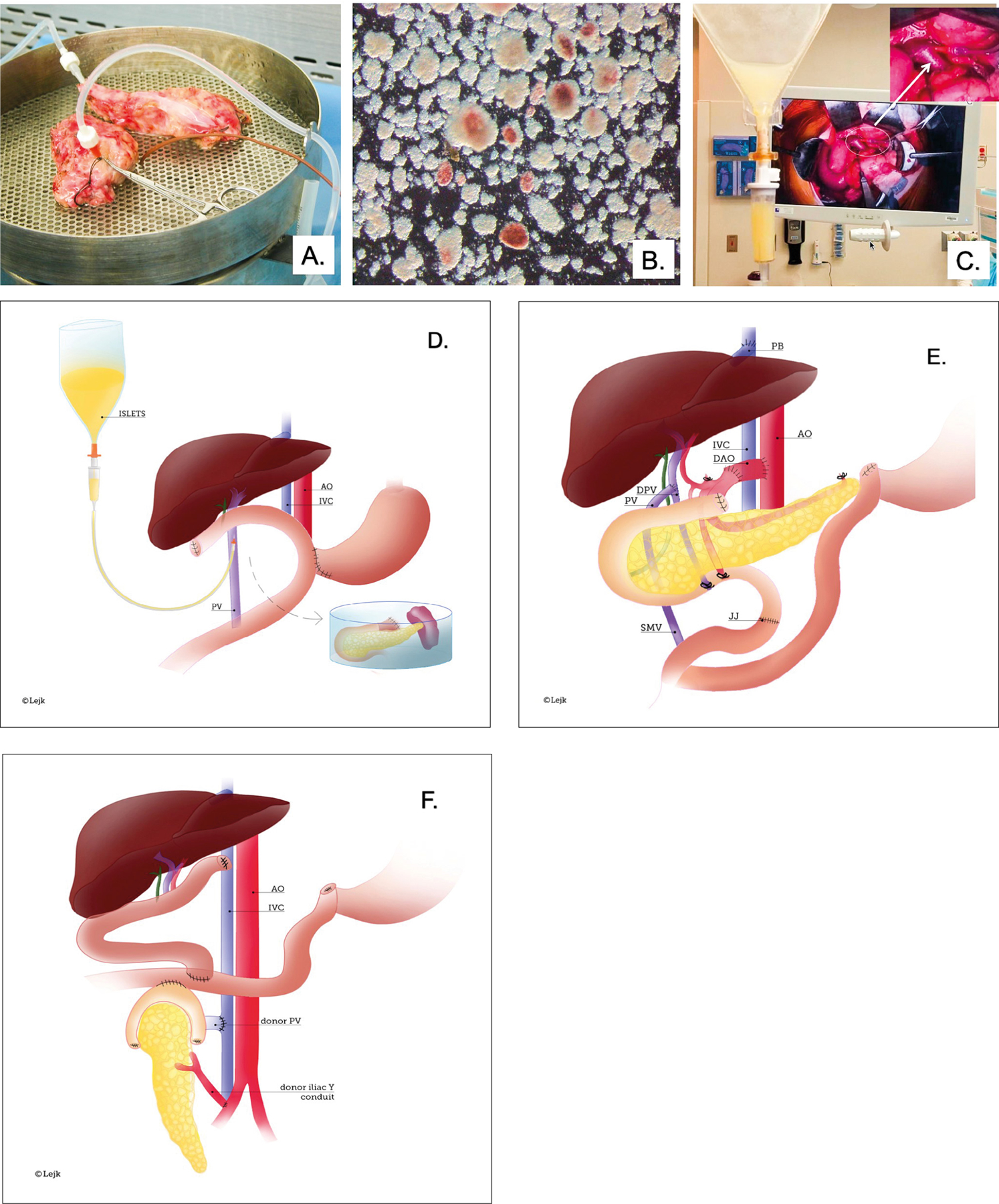
A, B, C. Major steps of islet isolation and islet transplantation
Panel A – Total Pancreatectomy. Excised pancreas after total pancreatectomy (TP) was transported to the Good Manufacture Practice (GMP) facility at University of Chicago for processing. The pancreas was divided, and the pancreatic duct cannulated and perfused with collagenase for enzymatic digestion and islet isolation.
Panel B – Islet Isolation. After digestion, a mixture of acinar tissue (light brown) and islets (stained with dithizone in red) was collected and the enzyme was washed off. The sample was tested for sterility and endotoxin and was suspended in transplant media in an infusion bag.
Panel C – Islet infusion. The portal vein (PV) was cannulated under direct vision and islets were infused intraportally. The white arrow points to the cannulated PV.
D, E, F. Illustration of TPIAT and en bloc combined liver pancreas transplantation and solitary pancreas transplantation procedures.
Panel D – TPIAT. Schematic demonstrates pancreas excised with duodenum, distal stomach, and spleen and placed on the back-table. Next, pancreatic duct was cannulated for further processing in GMP facility. Once islets were isolated, they were placed in a bag and infused under gravity via the cannulated portal vein.
Panel E – En bloc liver and pancreas transplantation. After hepatectomy, the donor hepatic veins were connected to the vena cava using the piggyback technique (PB). The recipient’s portal vein was connected to the side of the portal vein of the donor (PV/DPV). A donor aortic conduit (DAO) was used for the arterial supply to the liver/pancreas graft. Prior to the hepatectomy, the DOA was first anastomosed to the supraceliac recipient aorta (AO) and subsequently, the DOA was connected to a Carrel patch containing the donor celiac trunk and superior mesenteric artery (SMA) during liver/pancreas implantation. Roux-en-Y jejuno-jejunostomy (JJ) restored continuity of the gastrointestinal tract.
Panel F – Solitary pancreas transplantation. Schematic demonstrates the position of the transplanted deceased donor pancreas in the right lower abdomen. Arterial blood was provided to the graft via a Y-conduit made of donor iliac arteries. The portal vein of the graft is anastomosed to the distal cava and the duodenum to the side of the jejunum.