

Abstract
Background
Unlike infant and child mortality, neonatal mortality has declined steadily in Ethiopia. Despite the large-scale investment made by Ethiopia to improve the health of newborns and infants, it is among the regions with the highest burden of neonatal mortality. Although there are studies done on neonatal mortality in different areas of Ethiopia, as to our search of pieces of literature there is no study in Emerging regions of the country. Therefore, this study aimed to investigate the individual and community-level determinants of neonatal mortality in the Emerging regions of Ethiopia.
Methods
Using the 2016 Ethiopian Demographic and Health Survey (EDHS) data, secondary data analysis was done. A total weighted sample of 4238 live births in Emerging regions were included for the final analysis. A multilevel binary logistic regression was fitted to identify the significant determinants of neonatal mortality. The Intra-class Correlation Coefficient (ICC), Median Odds Ratio (MOR), Proportional Change in Variance (PCV) were used for assessing the clustering effect, and deviance for model comparison. Variables with a p-value < 0.2 in the bi-variable analysis were considered in the multivariable analysis. In the multivariable multilevel binary logistic regression analysis, Adjusted Odds Ratio (AOR) with 95% Confidence Interval (CI) were reported to declare statistically significant determinants of neonatal mortality.
Results
The neonatal mortality rate in Emerging regions of Ethiopia was 34.9 per 1000 live births (95% CI: 29.8, 40.9). Being born to a mother who had no formal education (AOR = 1.79, 95% CI: 1.12, 2.88), being born to a mother who did not participate in making health care decisions (AOR = 1.25, 95% CI: 1.14, 1.79), and being twin birth (AOR = 6.85, 95% CI: 3.69, 12.70) were significantly associated with higher odds of neonatal mortality. On the other hand, being female (AOR = 0.67, 95% CI: 0.47, 0.95), having 1–3 Antenatal Care (ANC) visits (AOR = 0.34, 95% CI: 0.15, 0.74), high community media exposure (AOR = 0.64, 95% CI: 0.41, 0.98), and preceding birth interval of two to 4 years (AOR = 0.38, 95% CI: 0.24, 0.58) were significantly associated with lower odds of neonatal mortality.
Conclusion
Neonatal mortality in Emerging regions of Ethiopia was unacceptably high. Maternal education, women’s autonomy in making decisions for health care, sex of a child, type of birth, preceding birth interval, ANC visit, and community media exposure were found significant determinants of neonatal mortality. Therefore, empowering women in making health care decisions and increasing access to mass media play a major role in reducing the incidence of neonatal mortality in Emerging regions of Ethiopia.
Keywords: Ethiopia, Neonatal mortality, Emerging regions, Multilevel analysis
Background
Globally, under-five mortality significantly decreased from 12.7 million in 1990 to 6.3 million in 2015 with 2.6 million died during the neonatal period [1]. It accounting for 40% of under-five mortality [2]. Approximately 98% of neonatal deaths occurred in low and middle-income countries [3, 4] and 39% in sub-Saharan African (SSA) countries [5]. The neonatal mortality rate has varied across countries ranged from 20 per 1000 live births in high-income countries to 31 per 1000 live births in SSA [6]. It is far below to achieve the Sustainable Development Goal (SDG) target of reducing the neonatal mortality rate of 12 or less per 1000 live births by 2030 [7, 8].
Despite the substantial decrease in child and infant mortality, the decline in neonatal mortality is steady [9]. As in most African countries, Ethiopia is one of the countries with the highest burden of neonatal mortality [10]. In Ethiopia, though child and under-5 mortality has dramatically decreased in the last two decades, neonatal mortality has steadily decreased [11]. According to the Ethiopian Demographic and Health Surveys (EDHSs) report, under-five mortality decreased from 166 per 1000 live births to 67 per 1000 live births, and infant mortality decreased from 97 per 1000 births to 48 per 1000 births, while neonatal mortality decreased from 49 per 1000 live births to 29 per 1000 live births, which is lower than under-five and infant mortality [12–14].
Infectious diseases, malnutrition, and birth complications are identified as the leading causes of neonatal mortality [2, 4, 15]. Previous studies conducted on neonatal mortality showed that residence [16], parity [17], educational status [17], mode of delivery [18], ANC utilization [19], birth interval [20], place of delivery [21], maternal nutritional status [22], and maternal obstetric factors [23] were statistically significant determinants of neonatal mortality. Neonatal mortality has significantly reduced in Ethiopia in the last two decades. However, it is marginally higher in Somalia, Afar, Gambella, and Benishangul-Gumuz regions [13, 24]. This highlights Ethiopia should work further to reach the Every Newborn Action Plan (ENAP) set a national target of less than 10 per 1000 live births by 2035 [25].
Though there are studies conducted on neonatal mortality in different areas of Ethiopia [26–29], there is limited evidence on the individual-and community-level determinants of neonatal mortality in Emerging regions. Therefore, this study aimed to investigate the individual and community level determinants of neonatal mortality in Emerging regions of Ethiopia using multilevel logistic regression analysis. Identifying significant individual and community-level determinants of neonatal mortality is crucial to reduce the incidence of neonatal mortality in Emerging regions of Ethiopia.
Methods
Study setting and design
The study used the 2016 Ethiopian Demographic and Health Survey (EDHS) data, which was obtained using a community-based cross-sectional study design. The 2016 EDHS is the fourth survey conducted in every five-year interval in Ethiopia. There are nine regional states (Afar, Amhara, Benishangul-Gumuz, Gambella, Harari, Oromia, Somali, Southern Nations Nationalities and People’s Region (SNNPR), and Tigray) and two city administrations (Addis Ababa and Dire Dawa) in Ethiopia. These regions are classified into three regions; emerging regions (Afar, Somali, Benishangul-Gumuz, and Gambella), developed regions (Amhara, Oromia, Harari, Southern Nations Nationalities and People’s Region (SNNPR) and Tigray) and two city administrations (Addis Ababa and Dire Dawa) [30]. A total of 13.1 million people of Ethiopia are living in Somali, Afar, Benishangul-Gumuz, and Gambella regions [31]. These regions are characterized by scattered pastoralists and semi-pastoral populations with extreme poverty and limited access to health care.
Data source and sampling procedure
The data used for this study were retrieved from the most recent Ethiopian DHS survey (EDHS 2016). The EDHS is conducted every five-year using structured methodology and pretested validated standard tools to generate updated health and health-related indicators. The EDHS employs a multi-stage stratified cluster sampling technique to select the study subjects. In the first stage, a total of 645 Enumeration Areas (EAs) that represent the country were selected. In the second stage, systematic random sampling was employed and on average 28 households per EAs were selected. For this study, neonates born in Emerging regions of Ethiopia within 5 years preceding the survey were included. A total of 4238 neonates were used for analysis. The overall data collection and the sampling procedure was presented in the full EDHS 2016 report [13].
Study variables
Outcome variable
The outcome variable for this study was neonatal death as reported by the mother, and it was defined as the death of a neonate within the first months of birth. This takes a binary outcome; such that neonatal death will be regarded as death (1 = if death occurs in the first month of life) or alive (0 = if the newborn alive in the first month of life).
Independent variables
The independent variable considered for this study were from two levels (at individual and community levels). At the individual, maternal age, marital status, religion, maternal education, paternal education, wealth index, maternal occupation, media exposure, maternal Body Mass Index (BMI)), number of ANC visit, the timing of first ANC visit, mode of delivery, preceding birth interval, place of delivery, women health care decision autonomy, size at birth, type of birth and birth order were included. At the community level, region, residence, community women education, community poverty, community media exposure, and distance to a health facility were considered. Community-level variables used in the analysis were from two sources; direct community-level variables that were used without any manipulation and aggregated community-level variables that were generated by aggregating individual-level variables at the cluster level.
Media exposure was measured from three variables such as reading the newspaper, listening to the radio, and watching television. These variables were merged and categorized as no “when there was no exposure to either of the three” and yes “when there was exposure to either of reading newspaper, listening radio and watching television”. Women’s health care decision making autonomy was assessed in EDHS, as a person decides on the respondent’s own health care. Which was categorized as women participating in making their own health care decisions and didn’t participate in making health care decisions (decides by their husband/partner). Birth weight was categorized as small, average, and large size at birth. Small size at birth is defined as birth weight less than 2500 g while birth weight greater than 4000 g is considered as large size at birth.
Data collection procedure
The research was performed based on the 2016 EDHS data by accessing the data from the official database of the MEASURE DHS program www.measuredhs.com. For the study, we used the Birth Record (BR) data set.
Data management and analysis
The variables were extracted from the BR dataset using STATA version 14 statistical software. The weighted data were used for analysis to adjust for unequal probability of selection and non-response. In EDHS, multistage stratified cluster sampling techniques were employed and the data were not flat. So, to draw valid inference and conclusion advanced statistical models such as hierarchical modelling, which consider independent variables measured at individual and community levels should be employed to consider the clustering effect/dependency. A two-level binary logistic regression model was employed to estimate the effect size of independent variables on neonatal mortality. Four models were fitted. The first model was the null model (a model without the explanatory variable), which was a model fitted to calculate the extent of cluster variability on neonatal mortality. It was assessed using the Likelihood Ratio test (LR), Intra-class Correlation Coefficient (ICC), Median Odds Ratio (MOR), and Proportional Change in Variance (PCV). The ICC is the proportion of total variance explained by the cluster variation [32].
ICC = σ2/(σ2 + π2/3)
Where ∂ 2 indicates that cluster variance.
MOR is the median values of the odds ratio of the cluster at high risk and cluster at lower risk of neonatal mortality when randomly picking two neonates from two clusters (EAs) [33].
PCV is defined as the total variation of neonatal mortality explained by the final model (a model with individual-level factors and community-level variables) relative to the null model (a model without independent variables).
Var (null model)
Model II (a multilevel model with individual-level variables); Model III (a multilevel model with community-level variables) and Model IV (a multilevel model adjusted with individual-and community-level variables) were fitted and a model comparison was made based on deviance.
Both bivariable and multivariable analyses were done. In the bivariable two-level binary logistic regression analysis, variables with a p-value ≤0.2 were considered in the multivariable analysis. The Adjusted Odds Ratio (AOR) with a 95% Confidence Interval (CI) in the multivariable multilevel analysis were reported to declare the statistical significance and strength of association between neonatal mortality and independent variables. By doing the pseudo linear regression analysis, the multi-collinearity was checked and the mean VIF was less than 5.
Results
Socio-demographic and economic characteristics of the mothers
A total weighted sample of 4238 neonates were used for this study. The majority (74.8%) of neonates were born to mothers with no formal education and 3997 (94.3%) of neonate’s mother were married. Of the total neonates, 3397 (80.2%) of their mothers did not have media exposure and 3082 (72.7%) of neonates were born to mothers aged 20–34 years. The majority (72.4%) of neonate’s mother was Muslim religion followers (Table 1).
Table 1.
Socio-demographic and economic characteristics of mothers, 2016
| Variables | Frequency (N = 4238) | Percentage (%) |
|---|---|---|
| Maternal age (years) | ||
| < 20 | 146 | 3.5 |
| 20–34 | 3082 | 72.7 |
| 35+ | 1010 | 23.8 |
| Maternal education status | ||
| No education | 3170 | 74.8 |
| Primary | 764 | 18.0 |
| Secondary and above | 304 | 7.2 |
| Religion | ||
| Orthodox | 352 | 8.3 |
| Muslim | 3068 | 72.4 |
| Protestant | 697 | 16.5 |
| Others | 121 | 2.9 |
| Wealth status | ||
| Rich | 776 | 18.3 |
| Medium | 303 | 7.2 |
| Poor | 3159 | 74.5 |
| Marital status | ||
| Never married | 9 | 0.2 |
| Married | 3997 | 94.3 |
| Divorced/separated/widowed | 232 | 5.5 |
| Women’s occupation status | ||
| Not working | 2787 | 65.8 |
| Working | 1451 | 34.2 |
| Paternal education | ||
| No education | 2476 | 58.4 |
| Primary | 800 | 18.9 |
| Secondary and above | 962 | 22.7 |
| Media exposure | ||
| No | 3397 | 80.2 |
| Yes | 841 | 19.8 |
| Maternal BMI | ||
| < 18.5 kg/m2 | 1256 | 29.6 |
| 18.5–24.9 kg/m2 | 2450 | 57.8 |
| ≥ 25 kg/m2 | 532 | 12.6 |
BMI Body Mass Index, kg Kilograms, m2 Meter Square
Child and maternal obstetric related characteristics
From a total of 4238 neonates, 52.5% were males and 68.2% were born at home. About 13.1% of the mothers had 1–3 ANC visits during their pregnancy and 2.8% were delivered through caesarean section. About 2.4% were twin births and 40.6% were large size at birth. Nearly three-fourths (70.2%) of the mothers were participated in making their own health care decisions (Table 2).
Table 2.
Obstetric and health service related characteristics of respondents
| Variable | frequency | Percentage (%) |
|---|---|---|
| Place of delivery | ||
| Home | 2894 | 68.2 |
| Health facility | 1347 | 31.8 |
| Mode of delivery | ||
| Vaginal | 4118 | 97.2 |
| Caesarean section | 120 | 2.8 |
| Type of birth | ||
| Single | 4134 | 97.6 |
| Twin | 104 | 2.4 |
| Birth order | ||
| First birth | 769 | 18.2 |
| 2–4 | 1848 | 43.6 |
| ≥ 5 | 1621 | 38.2 |
| Preceding birth interval (in years) | ||
| < 2 | 1239 | 29.2 |
| 2–4 | 1748 | 41.3 |
| > 4 | 1251 | 29.5 |
| Timing of first ANC visit | ||
| No ANC visit | 3177 | 74.9 |
| First trimester | 354 | 8.3 |
| Second trimester | 672 | 15.9 |
| Third trimester | 35 | 0.9 |
| Number of ANC visit | ||
| No | 3177 | 75.0 |
| 1–3 | 554 | 13.1 |
| ≥ 4 | 507 | 11.9 |
| Size of neonate at birth | ||
| Small | 1031 | 24.3 |
| Average | 1488 | 35.1 |
| Large | 1719 | 40.6 |
| Women participating in making health care decisions | ||
| No | 1264 | 29.8 |
| Yes | 2974 | 70.2 |
| Sex of child | ||
| Male | 2223 | 52.5 |
| Female | 2015 | 47.5 |
ANC Antenatal Care
Community-level characteristics of the mothers
About 85.1% of neonate’s mothers were from rural residents and 36.0% were in the Somali region. The majority (55.7%) of their mother was from a community with high poverty and 58.3% of the mothers reported perceived distance to visit health facilities as a big problem (Table 3).
Table 3.
Community level characteristics of respondents, 2016
| Variable | Frequency | Percentage (%) |
|---|---|---|
| Region | ||
| Afar | 1097 | 25.9 |
| Benishangul-Gumuz | 890 | 21.0 |
| Gambella | 724 | 17.1 |
| Somali | 1527 | 36.0 |
| Residence | ||
| Rural | 3605 | 85.1 |
| Urban | 633 | 14.9 |
| Distance to health facility | ||
| Big problem | 2472 | 58.3 |
| Not a big problem | 1766 | 41.7 |
| Community poverty | ||
| Low | 1879 | 44.3 |
| High | 2359 | 55.7 |
| Community women education | ||
| Low | 2429 | 57.3 |
| High | 1812 | 42.7 |
| Community media exposure | ||
| Low | 2273 | 53.6 |
| High | 1965 | 46.4 |
Neonatal mortality rate by respondent characteristics
The neonatal mortality rate in Emerging regions of Ethiopia was 34.9 (95% CI: 29.8, 40.9) per 1000 live births, which was highest in the Somali region (41 per 1000 live births) and lowest in the Benishangul region (35 per 1000 live births) (Fig. 1). The neonatal mortality rate among rural residents was 38.6 per 1000 live births (Table 4).
Fig. 1.
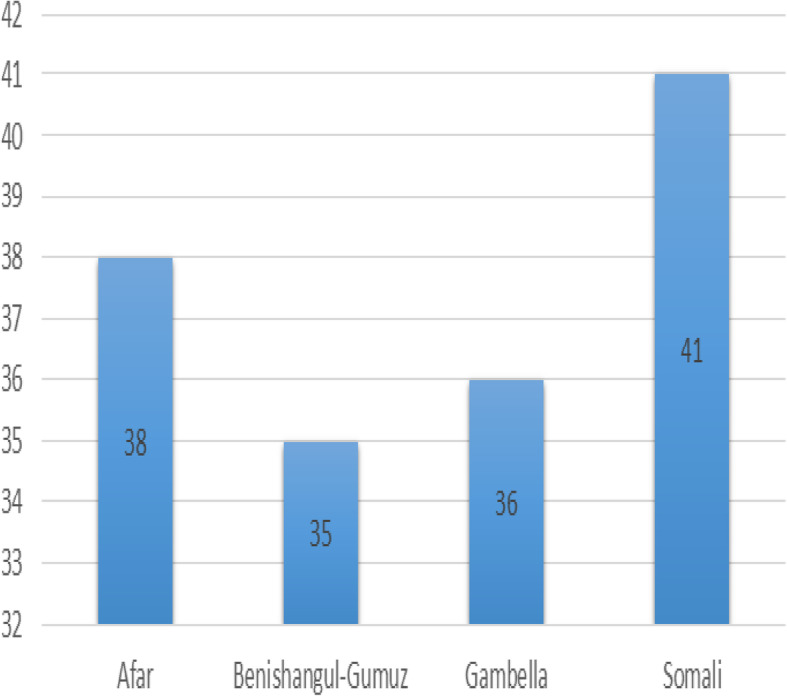
The neonatal mortality rates in Emerging regions of Ethiopia, 2016
Table 4.
Neonatal mortality rate by respondent characteristics, 2016
| Variable | Neonatal mortality rate |
|---|---|
| Residence | |
| Urban | 14.2 |
| Rural | 38.6 |
| Wealth status | |
| Poor | 39.6 |
| Medium | 26.4 |
| Rich | 19.3 |
| Media exposure | |
| No | 37.7 |
| Yes | 23.8 |
| Maternal age | |
| < 20 | 47.9 |
| 20–34 | 30.8 |
| 35+ | 45.5 |
| Place of delivery | |
| Home | 38.4 |
| Health facility | 27.5 |
| Type of birth | |
| Single | 31.7 |
| Twin | 163.5 |
| Size at birth | |
| Small | 36.6 |
| Average | 31.6 |
| Large | 36.9 |
| Maternal education | |
| No education | 34.4 |
| Primary | 40.6 |
| Secondary and above | 26.3 |
Determinants of neonatal mortality
Model comparison
The final model was the best-fitted model since it had the lowest deviance value. The ICC was 13.5% in the null model indicated that 13.5% of the total variability of neonatal mortality was due to differences between clusters/EA, with the remaining unexplained 86.5% was attributable to individual differences. Moreover, the MOR was 1.98 in the null model which indicates that there was variation between clusters, if we randomly select neonate from two different clusters, neonate at the cluster with a higher risk of neonatal mortality had 1.98 times higher odds of neonatal mortality as compared with neonate at cluster with a lower risk of neonatal mortality. PCV for the final model was 37.3%, indicated that 37.3% of the variability in neonatal mortality was explained by the full model (Table 5).
Table 5.
Multivariable multilevel logistic regression analysis of neonatal mortality in emerging regions of Ethiopia, 2016
| Variable | Null model | Model 1 (individual level factors) | Model 2 (Community level factors) | Model 4 (model with individual and community level factors) |
|---|---|---|---|---|
| Sex of neonate | ||||
| Male | 1 | 1 | ||
| Female | 0.67 [0.47, 0.94] | 0.67 [0.47, 0.94]a | ||
| Wealth index | ||||
| Rich | 1 | 1 | ||
| Middle | 1.11 [0.44, 2.80] | 0.87 [0.33, 2.27] | ||
| Poor | 1.73 [0.91, 3.27] | 1.22 [0.58, 2.55] | ||
| Birth order | ||||
| First birth | 1 | 1 | ||
| 2–4 | 0.55 [0.28, 1.07] | 0.62 [0.32, 1.21] | ||
| ≥ 5 | 0.73 [0.36, 1.48] | 0.82 [0.40, 1.66] | ||
| Type of birth | ||||
| Single | 1 | 1 | ||
| Twin | 7.14 [3.84, 13.29] | 6.85 [3.69, 12.70]a | ||
| Preceding birth interval | ||||
| < 2 year | 1 | 1 | ||
| 2–4 year | 0.36 [0.23, 0.56] | 0.38 [0.24, 0.58]a | ||
| > 4 year | 0.58 [0.32, 1.04] | 0.64 [0.35, 1.17] | ||
| Women participating in making their own heath care decisions | ||||
| Yes | 1 | 1 | ||
| No | 1.24 [1.12, 1.79] | 1.25 [1.14, 1.79]a | ||
| Media exposure | ||||
| No | 1 | 1 | ||
| Yes | 0.73 [0.42, 1.25] | 0.97 [0.55, 1.73] | ||
| Number of ANC visits | ||||
| No visit | 1 | 1 | ||
| 1–3 | 0.30 (0.14, 0.65) | 0.34 (0.15, 0.74)a | ||
| ≥ 4 | 0.44 (0.22, 0.88) | 0.55 (0.26, 1.15) | ||
| Place of delivery | ||||
| Home | 1 | 1 | ||
| Health facility | 0.77 [0.51, 1.16] | 0.81 [0.54, 1.23] | ||
| Maternal education | ||||
| No education | 1.66 [1.04, 2.65] | 1.79 [1.12, 2.88]a | ||
| Primary | 1.21 [0.53, 2.78] | 1.50 [0.65, 3.46] | ||
| Secondary and higher | 1 | 1 | ||
| Residence | ||||
| Urban | 1 | 1 | ||
| Rural | 2.04 [0.91, 4.54] | 1.82 [0.75, 4.38] | ||
| Distance to health facility | ||||
| Not a big problem | 1 | 1 | ||
| Big problem | 1.21 [0.83, 1.78] | 1.16 [0.78, 1.72] | ||
| Community poverty | ||||
| Low | 1 | 1 | ||
| High | 1.04 [0.67, 1.62] | 0.85 [0.52, 1.39] | ||
| Community media exposure | ||||
| No | 1 | 1 | ||
| Yes | 0.63 [0.41, 0.97] | 0.64 [0.41, 0.98]a | ||
| Random effect | ||||
| Community level variance | 0.51 | 0.41 | 0.37 | 0.32 |
| Log likelihood | − 635.27 | − 597.78 | − 627.50 | − 593.68 |
| Deviance | 1270.54 | 1195.56 | 1255.0 | 1187.36 |
| ICC | 13.5% | 11.0% | 10.0% | 8.9% |
| MOR | 1.98 | 1.84 | 1.78 | 1.72 |
| PCV | ref | 19.6% | 27.5% | 37.3% |
aICC Intra-class Correlation Coefficient, MOR Median Odds Ratio, PCV Proportional Change in Variance
In the multivariable multilevel analysis; maternal education, women who didn’t participate in making their own health care decisions, twin births, preceding birth interval, number of ANC visits, community media exposure, and sex of child were significantly associated with neonatal mortality. The odds of neonatal mortality among live births born to mothers who didn’t attend formal education had 1.79 (AOR = 1.79, 95% CI: 1.12, 2.88) times higher than live births born to mothers who attained secondary education and above. The odds of neonatal mortality among female births were decreased by 33% (AOR = 0.67, 95% CI: 0.47, 0.95) compared to male births. Being born to mothers who didn’t participate in making their own health care decisions were 1.25 (AOR = 1.25, 95% CI: 1.14, 1.79) times higher odds of neonatal mortality than births whose mother who participated in making health care decisions. The odds of neonatal mortality among twin births were 6.85 (AOR = 6.85, 95% CI: 3.69, 12.70) times higher compared to singletons. Furthermore, the odds of neonatal mortality among neonates in the community that had high media exposure were decreased by 36% (AOR = 0.64, 95% CI: 0.41, 0.98) compared to neonates in the community with low media exposure. The odds of neonatal death for neonates with preceding birth interval 2 to 4 years were decreased by 62% (AOR = 0.38, 95% CI: 0.24, 0.58) compared to neonates with preceding birth interval less than 2 years. The odds of neonatal mortality among children born to mothers who had 1–3 ANC visits during pregnancy were decreased by 66% (AOR = 0.34, 95% CI: 0.15, 0.74) than a child born to a mother who didn’t have ANC visit during pregnancy (Table 5).
Discussion
Thousands of newborns die each year from preventable causes such as infectious diseases, malnutrition, and accidents, despite impressive success in reducing neonatal, infant, and child mortality in Ethiopia [34]. Neonatal mortality is the most sensitive indicator of limited health care access such as institutional delivery, vaccination, medical treatment of diseases, nutrition, and hygiene [35, 36].
This study found that the neonatal mortality rate in emerging regions of Ethiopia was 34.9 [95% CI: 29.8, 40.9] per 1000 live births. It was consistent with studies reported in the Jimma zone [26], and Nigeria [37]. However, it was higher than the 2016 EDHS report [13], and Afghanistan [38]. The possible explanation could be due to the present study was undertaken in Emerging regions (Somali, Afar, Gambella, and Benishangul-Gumuz) of Ethiopia where maternal and child health care services are relatively low and economically disadvantaged in contrast to other regions [39]. Furthermore, lower vaccine coverage reduced access to healthcare, poorly urbanized, and a comparatively high incidence of childhood infectious diseases such as malaria, and acute respiratory tract infections are found in Emerging regions compared to the other regions of the country [40, 41].
In the multilevel analysis; maternal education, preceding birth interval, type of birth, sex of neonate, community media exposure, number of ANC visits, and women participation in making health care decisions were significantly associated with neonatal mortality. A neonate born to mothers who do not have formal education had higher odds of neonatal mortality than a neonate born to mothers who attained secondary education and above. It is in line with studies reported in Sudan [42], Bangladesh [22], and Nigeria [16]. This may be because uneducated mothers may not have access to health information and less likely to visit maternal health care such as institutional delivery, ANC, and PNC [43, 44]. Another reason is uneducated mothers are reluctant to pursue childhood vaccination [45, 46] and more likely to practice prelacteal feeding [47], this could increase the risk of neonatal mortality. Besides, maternal education could result in good childhood feeding practices and have an improved awareness of common childhood disease preventive approaches that play a significant role in increasing newborn survival [48, 49].
In this study, being twin birth was a significant predictor of neonatal mortality. Twin births had higher odds of death in the first month of birth than singletons. It is consistent with the study finding in Ghana [17]. This could be since twin births are at higher risk of preterm delivery and fetal growth restriction and this could increase their risk of hypothermia, sepsis, and hypoglycemia that might increase the risk of neonatal mortality [50]. Neonates born within the preceding birth interval of 2 to 4 years had lower odds of dying within the neonatal period than those having a preceding birth interval less than 2 years. It was consistent with prior studies conducted in India [51], Afghanistan [38], and Indonesia [52]. The possible justification might be due to the reason that optimal birth spacing is vital for the health of the mother and newborn. The interbirth interval of 2 to 4 years could result in good pregnancy outcomes as women restore their nutritional and physiological loss from a previous birth, this could decrease their incidence of neonatal mortality.
Births to women who did not participate in making health care decisions had higher odds of neonatal death. This was in line with a study conducted in Bangladesh [53], it might be due to the reason that women who have participated in making health care decisions are more likely to use antenatal care service, gave birth at the health facility, and have a postnatal checkup in the early neonatal period, this could help to early identify danger signs of pregnancy and neonates and to seek medical treatment [54, 55].
The odds of neonatal mortality among female neonates were lower than male neonates. This was consistent with studies reported in Indonesia [52], and Nigeria [37]. This could be due to the sex differences in genetic and biological makeup, with males being biologically weaker and more susceptible to diseases and mortality [56]. Besides, the difference in mortality might be attributed to the different protein and gene expression variation in the placenta [57].
This study found that community media exposure was a significant predictor of neonatal mortality. Newborns from the community with high media exposure had decreased odds of death in the neonatal period than neonates from the community with low media exposure. This is in line with the study done in Bangladesh [58], the possible explanation might be the reason that mothers who have media exposure had better awareness of ANC utilization, institutional delivery, and childhood illness [59].
Newborns born to mothers who had 1–3 ANC visits during pregnancy had lower odds of neonatal mortality than newborns born to mothers who did not have ANC visits during pregnancy. It was consistent with studies in Kenya [60] and India [61]. This might be because a pregnant mother who had antenatal care visits receives health care such as iron, deworming, folic acid, and tetanus immunizations, this could decrease the risk of neonatal mortality. Besides, ANC creates an opportunity for mothers and newborns to receive different interventions such as anti-D, childhood vaccinations, and nutritional supplementation.
The strength of this study was the use of multilevel modelling taking into account the clustering effect in EDHS to draw valid inferences and conclusions. This study had limitations. As this stud was a cross-sectional study, it shares the limitations of cross-sectional study design. Besides, variables such as infectious diseases, sepsis, congenital anomalies, transplacental infections, HIV status, and medication use which are considered as the most common cause of neonatal mortality were not included in this study since it was not collected in EDHS 2016.
Conclusion
Neonatal mortality in emerging regions of Ethiopia remains a major public health concern. Maternal education, women’s participation in health care decision making, sex of the child, type of birth, preceding birth interval, number of ANC visits, and community media exposure were significantly associated with neonatal mortality. Therefore, empowering women in education and their autonomy in making health care decisions as well as improving access to media plays a significant role in reducing neonatal mortality in emerging regions of Ethiopia. The government should scale up maternal and child health services in these regions to reduce neonatal mortality at the national level.
Acknowledgments
We would like to thank the measure DHS program for providing the data set.
Abbreviations
- ANC
Antenatal Care
- AOR
Adjusted Odds Ratio, ARR
- BMI
Body Mass Index
- CI
Confidence Interval
- COR
Crude Odds Ratio
- CSA
Central Statistical Agency
- DHS
Demographic Health Survey
- EA
Enumeration Area
- EDHS
Ethiopian Demographic Health Survey
- ICC
Intra-cluster Correlation Coefficient
- LLR
Log-likelihood Ratio
- LR
Likelihood Ratio
- MOR
Median Odds Ratio
- PCV
Proportional Change in Variance
- PHC
Population and Housing census
- SNNPRs
Southern Nations and Nationality People Regional state
- WHO
World Health Organization
Authors’ contributions
Conceptualization: GAT and MGW, Data curation: GAT and MGW, Investigation: GAT and MGW, Methodology: GAT and MGW, Resources: GAT and MGW, Software: GAT and MGW, Supervision: GAT, Validation: GAT, Visualization: GAT and MGW, Writing: GAT and MGW, Writing – review and editing: GAT and MGW. All the authors read and approve the manuscript.
Funding
No funding was obtained for this study.
Availability of data and materials
Data is available online and you can access it from www.measuredhs.com.
Ethics approval and consent to participate
The EDHS data is available to the general public by request in different formats from the Measure DHS website http://www.measuredhs.com. We submitted a request to the Measure DHS by briefly stating the objectives of this analysis and thereafter received permission to download the maternal and children’s dataset in STATA format.
Consent for publication
Not applicable.
Competing interests
Authors declare that they have no conflict of interest.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Vakili R, Emami Moghadam Z, Khademi G, Vakili S, Saeidi M. Child mortality at different world regions: a comparison review. Int J Pediatr. 2015;3(4.2):809–816. [Google Scholar]
- 2.Liu L, Oza S, Hogan D, Perin J, Rudan I, Lawn JE, et al. Global, regional, and national causes of child mortality in 2000–13, with projections to inform post-2015 priorities: an updated systematic analysis. Lancet. 2015;385(9966):430–440. doi: 10.1016/S0140-6736(14)61698-6. [DOI] [PubMed] [Google Scholar]
- 3.Saleem S, McClure EM, Goudar SS, Patel A, Esamai F, Garces A, et al. A prospective study of maternal, fetal and neonatal deaths in low-and middle-income countries. Bull World Health Organ. 2014;92:605–612. doi: 10.2471/BLT.13.127464. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Smith ER, Shankar AH, Wu LS, Aboud S, Adu-Afarwuah S, Ali H, et al. Modifiers of the effect of maternal multiple micronutrient supplementation on stillbirth, birth outcomes, and infant mortality: a meta-analysis of individual patient data from 17 randomised trials in low-income and middle-income countries. Lancet Glob Health. 2017;5(11):e1090–ee100. doi: 10.1016/S2214-109X(17)30371-6. [DOI] [PubMed] [Google Scholar]
- 5.Moyer CA, Dako-Gyeke P, Adanu RM. Facility-based delivery and maternal and early neonatal mortality in sub-Saharan Africa: a regional review of the literature. Afr J Reprod Health. 2013;17(3):30–43. [PubMed] [Google Scholar]
- 6.Lawn JE, Blencowe H, Oza S, You D, Lee AC, Waiswa P, et al. Every newborn: progress, priorities, and potential beyond survival. Lancet. 2014;384(9938):189–205. doi: 10.1016/S0140-6736(14)60496-7. [DOI] [PubMed] [Google Scholar]
- 7.Kc A, Jha AK, Shrestha MP, Zhou H, Gurung A, Thapa J, et al. Trends for neonatal deaths in Nepal (2001–2016) to project progress towards the SDG target in 2030, and risk factor analyses to focus action. Matern Child Health J. 2020;24(1):5–14. doi: 10.1007/s10995-019-02826-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Puthenkalam JJ. Sustainable Development Goals as New Framework for Development From MDGs to SDGs. 上智経済論集. 2016;61(1):1–18. [Google Scholar]
- 9.Wang H, Liddell CA, Coates MM, Mooney MD, Levitz CE, Schumacher AE, et al. Global, regional, and national levels of neonatal, infant, and under-5 mortality during 1990–2013: a systematic analysis for the global burden of disease study 2013. Lancet. 2014;384(9947):957–979. doi: 10.1016/S0140-6736(14)60497-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Golding N, Burstein R, Longbottom J, Browne AJ, Fullman N, Osgood-Zimmerman A, et al. Mapping under-5 and neonatal mortality in Africa, 2000–15: a baseline analysis for the sustainable development goals. Lancet. 2017;390(10108):2171–2182. doi: 10.1016/S0140-6736(17)31758-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Mekonnen Y, Tensou B, Telake DS, Degefie T, Bekele A. Neonatal mortality in Ethiopia: trends and determinants. BMC Public Health. 2013;13(1):483. doi: 10.1186/1471-2458-13-483. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Icf C. Ethiopian demographic health survey 2011. Addis Ababa and Calverton: Central Statistical Agency (Ethiopia) and ICF International; 2012. pp. 17–27. [Google Scholar]
- 13.ICF CSACEa . Ethiopia Demographic and Health Survey 2016. Addis Ababa, and Rockville: CSA and ICF; 2016. [Google Scholar]
- 14.macro CsAEaO . Ethiopian Demographic and Health survey 2005. Addis Ababa Calverton: CSA and ORC macro; 2005. [Google Scholar]
- 15.Black RE, Cousens S, Johnson HL, Lawn JE, Rudan I, Bassani DG, et al. Global, regional, and national causes of child mortality in 2008: a systematic analysis. Lancet. 2010;375(9730):1969–1987. doi: 10.1016/S0140-6736(10)60549-1. [DOI] [PubMed] [Google Scholar]
- 16.Ezeh OK, Agho KE, Dibley MJ, Hall J, Page AN. Determinants of neonatal mortality in Nigeria: evidence from the 2008 demographic and health survey. BMC Public Health. 2014;14(1):521. doi: 10.1186/1471-2458-14-521. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Kayode GA, Ansah E, Agyepong IA, Amoakoh-Coleman M, Grobbee DE, Klipstein-Grobusch K. Individual and community determinants of neonatal mortality in Ghana: a multilevel analysis. BMC Pregnancy Childbirth. 2014;14(1):165. doi: 10.1186/1471-2393-14-165. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Walsh CA, Robson M, McAuliffe FM. Mode of delivery at term and adverse neonatal outcomes. Obstet Gynecol. 2013;121(1):122–128. doi: 10.1097/AOG.0b013e3182749ac9. [DOI] [PubMed] [Google Scholar]
- 19.Corman H, Grossman M. Determinants of neonatal mortality rates in the US: a reduced form model. J Health Econ. 1985;4(3):213–236. doi: 10.1016/0167-6296(85)90030-X. [DOI] [PubMed] [Google Scholar]
- 20.Kolola T, Ekubay M, Tesfa E, Morka W. Determinants of neonatal mortality in north Shoa zone, Amhara regional state, Ethiopia. PloS One. 2016;11(10):e0164472. doi: 10.1371/journal.pone.0164472. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Ajaari J, Masanja H, Weiner R, Abokyi SA, Owusu-Agyei S. Impact of place of delivery on neonatal mortality in rural Tanzania. Int J MCH AIDS. 2012;1(1):49. doi: 10.21106/ijma.10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Kamal SM. Maternal education as a determinant of neonatal mortality in Bangladesh. J Health Manag. 2012;14(3):269–281. doi: 10.1177/0972063412457509. [DOI] [Google Scholar]
- 23.Abdullah A, Hort K, Butu Y, Simpson L. Risk factors associated with neonatal deaths: a matched case–control study in Indonesia. Glob Health Action. 2016;9(1):30445. doi: 10.3402/gha.v9.30445. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Negera A, Abelti G, Bogale T, Gebreselassie T, Pearson R. An analysis of the trends, differentials and key proximate determinants of infant and under-five mortality in Ethiopia. Calverton: ICF International; 2013. [Google Scholar]
- 25.Walker N, Yenokyan G, Friberg IK, Bryce J. Patterns in coverage of maternal, newborn, and child health interventions: projections of neonatal and under-5 mortality to 2035. Lancet. 2013;382(9897):1029–1038. doi: 10.1016/S0140-6736(13)61748-1. [DOI] [PubMed] [Google Scholar]
- 26.Debelew GT, Afework MF, Yalew AW. Determinants and causes of neonatal mortality in Jimma zone, southwest Ethiopia: a multilevel analysis of prospective follow up study. PLoS One. 2014;9(9):e107184. doi: 10.1371/journal.pone.0107184. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Kolola T, Ekubay M, Tesfa E, Morka W. Determinants of neonatal mortality in North Shoa Zone, Amhara regional state, Ethiopia. PLoS One. 2016;11(10):e0164472. doi: 10.1371/journal.pone.0164472. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Yirgu R, Molla M, Sibley L. Determinants of neonatal mortality in rural Northern Ethiopia: A population based nested case control study. PLoS One. 2017;12(4):e0172875–e017287e. doi: 10.1371/journal.pone.0172875. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Wolde HF, Gonete KA, Akalu TY, Baraki AG, Lakew AM. Factors affecting neonatal mortality in the general population: evidence from the 2016 Ethiopian demographic and health survey (EDHS)—multilevel analysis. BMC Res Notes. 2019;12(1):610. doi: 10.1186/s13104-019-4668-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.UNCDF:. Emerging Regions Development Programme (ERDP): Programme Document. www.uncdf.org/download/file/erdp54573prodoc0.pdf Accessed 16 Dec 2019.
- 31.Ababa A. Demographics of Ethiopia. 2020. [Google Scholar]
- 32.Rodriguez G, Elo I. Intra-class correlation in random-effects models for binary data. Stata J. 2003;3(1):32–46. doi: 10.1177/1536867X0300300102. [DOI] [Google Scholar]
- 33.Merlo J, Chaix B, Ohlsson H, Beckman A, Johnell K, Hjerpe P, et al. A brief conceptual tutorial of multilevel analysis in social epidemiology: using measures of clustering in multilevel logistic regression to investigate contextual phenomena. J Epidemiol Community Health. 2006;60(4):290–297. doi: 10.1136/jech.2004.029454. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Lawn JE, Kerber K, Enweronu-Laryea C, Cousens S, editors. 3.6 million neonatal deaths—what is progressing and what is not? Seminars in perinatology: Elsevier; 2010. [DOI] [PubMed]
- 35.Memon ZA, Khan GN, Soofi SB, Baig IY, Bhutta ZA. Impact of a community-based perinatal and newborn preventive care package on perinatal and neonatal mortality in a remote mountainous district in northern Pakistan. BMC Pregnancy Childbirth. 2015;15(1):106. doi: 10.1186/s12884-015-0538-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Dickson KE, Simen-Kapeu A, Kinney MV, Huicho L, Vesel L, Lackritz E, et al. Every newborn: health-systems bottlenecks and strategies to accelerate scale-up in countries. Lancet. 2014;384(9941):438–454. doi: 10.1016/S0140-6736(14)60582-1. [DOI] [PubMed] [Google Scholar]
- 37.Adewuyi E, Zhao Y, Lamichhane R. Socioeconomic, bio-demographic and health/behavioral determinants of neonatal mortality in Nigeria: a multilevel analysis of 2013 demographic and health survey. Int J Contemp Pediatr. 2016;3(2):311–323. doi: 10.18203/2349-3291.ijcp20160499. [DOI] [Google Scholar]
- 38.Al Kibria GM, Burrowes V, Choudhury A, Sharmeen A, Ghosh S, Mahmud A, et al. Determinants of early neonatal mortality in Afghanistan: an analysis of the demographic and health survey 2015. Glob Health. 2018;14(1):47. doi: 10.1186/s12992-018-0363-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Seide WM. The Nuer pastoralists: between large scale agriculture and villagization: a case study of the Lare District in the Gambella Region of Ethiopia: Nordiska Afrikainstitutet. 2017. [Google Scholar]
- 40.Admassie A, Abebaw D. Rural poverty and marginalization in Ethiopia: a review of development interventions. Marginality. 2014:269.
- 41.Woldesenbet PW. Provision of and participation in primary education in the pastoralist regions of Afar and Somali of Ethiopia. 2015. [Google Scholar]
- 42.Bashir AO, Ibrahim GH, Bashier IA, Adam I. Neonatal mortality in Sudan: analysis of the Sudan household survey, 2010. BMC Public Health. 2013;13(1):287. doi: 10.1186/1471-2458-13-287. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Tsegay Y, Gebrehiwot T, Goicolea I, Edin K, Lemma H, San SM. Determinants of antenatal and delivery care utilization in Tigray region, Ethiopia: a cross-sectional study. Int J Equity Health. 2013;12(1):30. doi: 10.1186/1475-9276-12-30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Shiferaw S, Spigt M, Godefrooij M, Melkamu Y, Tekie M. Why do women prefer home births in Ethiopia? BMC Pregnancy Childbirth. 2013;13(1):5. doi: 10.1186/1471-2393-13-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Siddiqi N, Siddiqi AA, Nisar N, Khan A. Mothers' knowledge about EPI and its relation with age-appropriate vaccination of infants in peri-urban Karachi. J Pak Med Assoc. 2010;60(11):940. [PubMed] [Google Scholar]
- 46.Bofarraj MA. Knowledge, attitude and practices of mothers regarding immunization of infants and preschool children at Al-Beida City, Libya 2008. Egypt J Pediatr Allergy Immunol (The). 2011;9(1).
- 47.Sefene A, Birhanu D, Awoke W, Taye T. Determinants of exclusive breastfeeding practice among mothers of children age less than 6 month in Bahir Dar city administration, Northwest Ethiopia; a community based cross-sectional survey. Sci J Clin Med. 2013;2(6):153–159. doi: 10.11648/j.sjcm.20130206.12. [DOI] [Google Scholar]
- 48.Campbell OM, Graham WJ. Group LMSSs. Strategies for reducing maternal mortality: getting on with what works. Lancet. 2006;368(9543):1284–1299. doi: 10.1016/S0140-6736(06)69381-1. [DOI] [PubMed] [Google Scholar]
- 49.Haines A, Sanders D, Lehmann U, Rowe AK, Lawn JE, Jan S, et al. Achieving child survival goals: potential contribution of community health workers. Lancet. 2007;369(9579):2121–2131. doi: 10.1016/S0140-6736(07)60325-0. [DOI] [PubMed] [Google Scholar]
- 50.Marchant T, Willey B, Katz J, Clarke S, Kariuki S, Ter Kuile F, et al. Neonatal mortality risk associated with preterm birth in East Africa, adjusted by weight for gestational age: individual participant level meta-analysis. PLoS Med. 2012;9(8):e1001292. doi: 10.1371/journal.pmed.1001292. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Bhalotra S, Van Soest A. Birth-spacing, fertility and neonatal mortality in India: dynamics, frailty, and fecundity. J Econ. 2008;143(2):274–290. doi: 10.1016/j.jeconom.2007.10.005. [DOI] [Google Scholar]
- 52.Titaley CR, Dibley MJ, Agho K, Roberts CL, Hall J. Determinants of neonatal mortality in Indonesia. BMC Public Health. 2008;8(1):232. doi: 10.1186/1471-2458-8-232. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Hossain MB, Phillips JF, Pence B. The effect of women's status on infant and child mortality in four rural areas of Bangladesh. J Biosoc Sci. 2007;39(3):355. doi: 10.1017/S002193200600143X. [DOI] [PubMed] [Google Scholar]
- 54.Mahapatro SR. Utilization of maternal and child health care services in India: does women s autonomy matter? 2012. [Google Scholar]
- 55.Dairo M, Owoyokun K. Factors affecting the utilization of antenatal care services in Ibadan, Nigeria. Benin J Postgrad Med. 2010;12(1).
- 56.Friedrich L, Stein RT, Pitrez PM, Corso AL, Jones MH. Reduced lung function in healthy preterm infants in the first months of life. Am J Respir Crit Care Med. 2006;173(4):442–447. doi: 10.1164/rccm.200503-444OC. [DOI] [PubMed] [Google Scholar]
- 57.Quiñones JN, Stamilio DM, Coassolo KM, Macones GA, Odibo AO. Is fetal gender associated with adverse perinatal outcome in intrauterine growth restriction (IUGR)? Am J Obstet Gynecol. 2005;193(3):1233–1237. doi: 10.1016/j.ajog.2005.05.053. [DOI] [PubMed] [Google Scholar]
- 58.Nilima S, Sultana R, Ireen S. Neonatal, infant and under-five mortality: an application of cox proportional Hazard model to BDHS data. J Asiatic Soc Bangladesh Sci. 2018;44(1):7–14. doi: 10.3329/jasbs.v44i1.46541. [DOI] [Google Scholar]
- 59.Agha S, Carton TW. Determinants of institutional delivery in rural Jhang, Pakistan. Int J Equity Health. 2011;10(1):1–12. doi: 10.1186/1475-9276-10-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Arunda M, Emmelin A, Asamoah BO. Effectiveness of antenatal care services in reducing neonatal mortality in Kenya: analysis of national survey data. Glob Health Action. 2017;10(1):1328796. doi: 10.1080/16549716.2017.1328796. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Singh A, Pallikadavath S, Ram F, Alagarajan M. Do antenatal care interventions improve neonatal survival in India? Health Policy Plan. 2014;29(7):842–848. doi: 10.1093/heapol/czt066. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Data is available online and you can access it from www.measuredhs.com.