
Fig. 6. The optimal carrier dose (or antibody loading) depends on both the local and systemic ADC distribution.
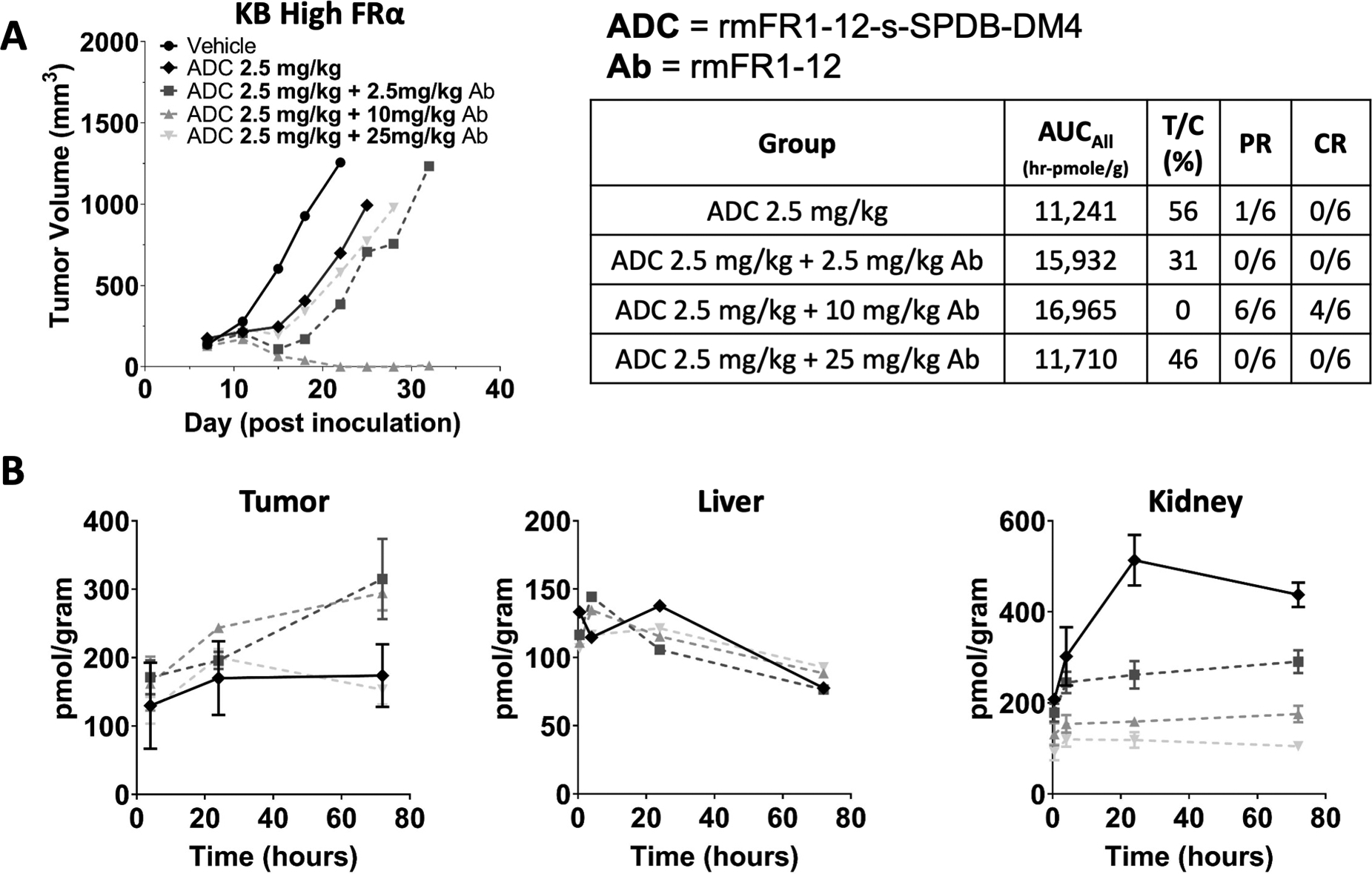
Increasing doses of unconjugated antibody co-administered with the DM4-ADC also improved efficacy (A) as they did with the DGN549 ADC (Fig. 5). However, with a carrier dose of 25 mg/kg of antibody, the efficacy dropped back down to a level seen with the ADC alone. While carrier doses of 2.5 and 10 mg/kg reduced plasma clearance and increased tumor uptake, at 25 mg/kg, the tumor is super-saturated, and tumor uptake is reduced (B). The 2.5 and 10 mg/kg carrier doses resulted in the same total tumor uptake (B), but the higher carrier dose was more effective, likely due to improved tissue penetration. Therefore, both the local (tumor distribution) and systemic (tumor exposure/uptake) effects determine the maximum ADC efficacy. For toxicity, the carrier dose had minimal impact on non-target mediated uptake in the liver (C). However, the carrier dose significantly reduced target-mediated uptake in the kidney (D). PR = partial response, CR = complete response