

Abstract
Background
Allergic rhinitis often gives rise to impaired quality of life and is believed to also affect cognitive function. We aimed to examine whether cognitive functions were impaired during grass pollen season in symptomatic allergic children and to relate the degree of impairment to quality of life and biomarkers related to stress and inflammation.
Methods
Forty‐three grass pollen‐allergic children (age 8‐17 years) with non‐satisfactory effect of medication (antihistamines and nasal steroids daily) during previous seasons were included. In addition, 26 matched non‐allergic children were included as controls. Both groups performed cognitive tests (CANTAB) and completed Quality of Life questionnaires outside and during the pollen season. Blood samples were collected and analyzed for stress and inflammatory biomarkers. Pollen level was measured daily.
Results
Impaired cognitive function was found in spatial working memory, where the allergic group made more errors compared to the non‐allergic group during pollen season, but not off‐season. No significant differences could be seen between the allergic group and the controls in the other tests investigating visual memory or attention. Quality of health questionnaires revealed more symptoms and impaired quality of life in allergic compared to non‐allergic children, and increased symptoms in allergic children were associated with longer reaction time for simple movement during pollen season. No differences in stress or inflammatory biomarkers could be found between the groups.
Conclusion
Cognitive function was affected during pollen season in pollen‐allergic children, and the more symptoms the allergic children had, the longer the reaction time in the cognitive tests.
Keywords: allergic rhinitis, biomarker, Cognitive function, pollen season, quality of life
Key Message.
Cognitive function was affected during pollen season in pollen‐allergic children, and the more symptoms the allergic children had, the longer the reaction time for simple movement. It is therefore important to tackle the disadvantage that many young people with allergic rhinitis often experience, and aim for accurate diagnosis of the disease, improve education toward effective self‐management, and optimize treatment.
1. INTRODUCTION
The prevalence of allergic rhinitis has increased worldwide, and the International Study of Asthma and Allergies in Childhood (ISAAC) showed an overall prevalence of 1.4‐39.7%, and the prevalence in Sweden was 11%‐12%. 1 Approximately one in five children of school age is sensitized to grass pollen, and 19.8% of patients with allergic rhinitis also indicate that they have asthma. 2 Between 60 and 85% of those with asthma indicates simultaneous rhinitis symptoms. 3 , 4
Individuals suffering from moderate/severe allergic rhinitis often experience troublesome symptoms 5 (i.e., persisting symptoms despite combination treatment, causing impairment in daily activities, sport, leisure, school, and/or sleep disturbance) alongside with physical complications. 6 It is assumed that it would be possible to achieve good symptom control with optimal medication regimens in the vast majority of young people. Accurate diagnosis of rhinitis, education of patients and caregivers toward effective self‐management, and appropriate treatments are important to tackle the disadvantage that many young people with rhinitis often experience. Though in those that still experience uncontrolled symptoms, there is also the need to consider rhinitis as an impairing factor of daily performance. 7
A less studied aspect of this chronic disease is the belief that it affects cognitive functions. Allergic rhinitis has also been shown to impair sleep, causing daytime sleepiness 8 because of an increase in nasal airway resistance and the pathological changes in airflow velocity, 9 and is associated with poorer school records in adolescents. 10 It has been shown that teenagers with rhinitis had difficulties concentrating at school, but the authors pointed out that a large proportion of the students with impaired results used sedative antihistamines. 11 In direct relation to pollen levels, it has been shown that an increase in the ambient pollen levels by one standard deviation at the mean leads to a 2.5% standard deviation decrease in test scores at high school examinations, with potentially larger effects for allergic students. 12 These studies focus mainly on physical factors in allergic rhinitis and patient reported health‐related quality of life. A study of specific cognitive functions in allergic rhinitis would broaden the knowledge of how the disease affects the individual via another target organ, the central nervous system. There are today tools to estimate cognitive function more specifically. The Cambridge Neuropsychological Test Automated Battery (CANTAB) is such an example and includes objective measures of cognitive function. 13 It includes several tests that can be used to assess working memory, learning, executive function of visual, verbal and episodic memory, and attention (information processing and reaction time).
In the present study, we aimed to examine whether cognitive functions were impaired during grass pollen season in allergic children with troublesome symptoms compared to control children and whether the potential degree of cognitive impairment was related to (a) quality of life, (b) the extent of rhinitis symptoms, and (c) biomarkers related to stress and inflammation.
2. METHODS
2.1. Study population
A total of 69 children, 8‐17 years old (mean age 12 years), were included. Children with grass pollen allergy (n = 43) were recruited consecutively in a pediatric clinic, and a primary care unit and age‐ and sex‐matched non‐allergic controls (n = 26) were recruited. For patient characteristics, see Table 1.
TABLE 1.
Subject characteristics
| Controls (n = 26) | Allergics (n = 43) | p‐value | |
|---|---|---|---|
| Male/female, n (%) | 14/12 (54%/46%) | 28/15 (65%/35%) | .35 |
| Age, years | 12 (10‐15) a | 12 (11‐15) a | .98 |
| Number of IgE sensitizations, n | 0 (0‐1) b | 4 (2‐6) | <.001 |
| House dust mite sensitized, n | 4 b | 13 b | .20 |
| Off‐season visit first, n (%) | 12 (46%) | 17 (39%) | .59 |
| Reporting any of the VAS symptoms c | |||
| Nose, n (%) | 7 (27%) | 43 (100%) | |
| Eyes, n (%) | 4 (15%) | 43 (100%) | |
| Lungs, n (%) | 5 (19%) | 31 (72%) | |
| Overall, n (%) | 1 (4%) | 43 (100%) | |
| Cross‐reactivity, n (%) | 0 (0%) | 26 (60%) | |
p = p‐values denote comparison of controls versus allergics.
Data is presented as median (IQR).
Four of the controls and 13 of the allergics had house dust mite sensitization but no allergic symptoms related to house dust mite.
Number of participants that reported any symptoms in the different categories of VAS (visual analogue scales): Nose = secretion, congestion, itching and sneezing; Eyes = redness, itching, watery; Lungs = cough, breathlessness, wheezing and asthmatics symptoms during exercise; Overall = general condition, fatigue and impact in everyday life; Cross‐reactivity = itching and irritation in the mouth and throat, stomach pain.
The allergic group consisted of grass pollen‐allergic patients, who experienced troublesome symptoms during previous grass pollen seasons despite a combination treatment of non‐sedative antihistamines and nasal steroids daily. All allergic children were still on this treatment, and their allergy medication (antihistamines and nasal steroids) was taken daily as usual in conjunction with the visits, as well as asthma medication, as prescribed.
Children sensitized to cat, dog, and horse allergen were included provided that they were not regularly exposed to these allergens. Children sensitized to house dust mite were excluded if they had a clinical history of symptoms due to house dust mite. No other medical conditions that could interfere with the study were accepted, besides a well‐controlled asthma. Participants were tested for the most common aeroallergens in Sweden (grass, birch, mug worth, cat, dog, horse, house dust mite, and Cladosporium herbarum) with either skin prick test or Phadiatop®. Subjects in the control group had a negative skin prick test or Phadiatop® and no clinical history of allergy or other conditions that could interfere with the study.
The study was approved by the Regional Ethical Review Board in Lund. All child custodians gave written informed consent, and all children gave oral informed consent.
2.2. Study design
The off‐season visit was performed outside the pollen season, either before (March‐April, 2015) or after (November‐December, 2015), and the season visit was performed during pollen season (Skåne Region, Sweden, May 19,‐August 31, 2015). Airborne pollen was monitored using a Burkard 7‐day volumetric spore trap, situated at a roof top about 30 m above ground level, at Skåne University Hospital (SUS) in Malmö, 55°60′N, 13°00′E.
2.3. Cognitive test
CANTAB is a series of touchscreen tests, 13 which can be repeated without the risk of learning effects, making it possible to assess subjects more than once. From a total of 25 tests that the CANTAB system contains, four tests were chosen in order to assess specific cognitive functions that appeared to be affected according to previous studies 14 , 15 , 16 , 17 : paired associated learning (PAL), spatial working memory (SWM), reaction time (RTI), and rapid visual information Processing (RVIP). Additionally, a fifth test, Motor screening test, was used to screen for visual, movement, and comprehensive difficulties/familiarization. The PAL test measures visual memory, both episodic memory and learning, and a lower value reflects better performance. The SWM test measures the working memory and strategy use, and a lower value reflects a better spatial working memory. The RTI test is an attention test which measures the speed of response and movement, and a lower value reflects a shorter reaction time. Finally, the RVIP test is an attention test that measure visual sustained attention in four parameters: 1. probability of hits (=h, the participant responding correctly), that is, total hits divided by the sum of total hits and total misses; a higher value reflects a better performance, 2. probability of false alarms (=f, the participant responding inappropriately), that is total false alarms divided by the sum of total false alarms and total correct rejections; a lower value reflects better performance, 3. A′ (calculated as 0.5+[(h − f)+(h − f)2]/[4 × h×(1 − f)]), a signal detection measure of sensitivity to the target, regardless of response tendency; a higher value reflects better performance, and 4. median latency is the median time taken to respond in correct responses; a lower value reflects better performance.
2.4. Questionnaires
The DISABKIDS questionnaire, 18 a generic health‐related quality of life instrument that can be used in every chronic disease, was applied to estimate the quality of life and the level of distress the last four weeks caused by allergy as a chronic disease. The DISABKIDS questionnaire (scoring 1‐5) can be divided into mental, social, and physical sections, and a higher score reflects a better quality of life.
The global visual analogue scale (VAS) was applied for estimating the perceived degree of symptoms of various organs (eyes, nose, and lungs), the subjects’ general condition and cross‐reactivity to oral and stomach symptoms to assess severity of rhinitis during pollen season. 19 Scoring was between 0 and 10, and a lower score reflects less symptoms.
The LILA questionnaire, 20 the Swedish version of PADQLQ (Pediatric Allergic Disease Quality of Life Questionnaire), 21 is a disease‐specific questionnaire for allergic children and adolescents to assess impact on quality of life during pollen season. It has a generally higher sensitivity and suitability in comparison with the effect of different treatments/types of intervention. The LILA questionnaire (scoring 0‐6) can be divided into practical, physical, and emotional sections, and a lower score reflects a better quality of life.
2.5. Inflammatory biomarkers
Serum samples were collected at the same days as the children performed the cognitive tests. Inflammation biomarkers (interleukin‐13 (IL‐13), tumor necrosis factor‐α (TNF‐α), and transforming growth factor‐β (TGF‐β)) were analyzed using commercially available ELISAs (R&D Systems), and stress biomarkers (cortisol and catecholamines (adrenalin and noradrenalin)) were analyzed according to clinical routine (cortisol, adrenalin, and noradrenalin: at Clinical chemistry unit, Skåne’s University Hospital).
2.6. Data analyses
All statistical calculations were performed using SPSS 25.0 for Windows (SPSS, Inc.), and data are presented as median (interquartile range) unless otherwise stated. Due to non‐normally distributed data, all statistical analyses were done using non‐parametric tests; Mann‐Whitney U test for unpaired data was used to compare two independent groups (allergic group versus control group), Wilcoxon signed‐rank test was used for paired data (pollen season versus off‐season), and correlations were calculated by Spearman's correlation test. Chi‐square test was used for number comparisons, with Fisher's correction when low numbers. A p < .05 was considered statistically significant.
3. RESULTS
3.1. Description of study participants
The allergic subjects were often multi‐sensitized to other airborne allergens with a median of 4 (IQR 2‐6) sensitizations per participant (Table 1).
VAS scale results showed that all allergic children reported nose and eye symptoms as well as impaired general condition. In addition, 72% reported symptoms from the lungs, which might include comorbidity of asthma. Some symptoms from nose and eyes were also reported by subjects in the control group, but were of mild grade and not attributed to underlying allergy.
3.2. Pollen levels
The pollen report from the local station (Figure 1) shows the grass pollen levels during the pollen season period of the study (May‐August 2015). Very high levels of grass pollen (>80 pollen grains per m3) were observed for only five days in total with a maximum of two consecutive days. Only six allergic children and four healthy controls undertook the tests during very high levels of grass pollen, and additionally, 14 allergic children and nine healthy controls undertook their tests during high levels of grass pollen.
FIGURE 1.
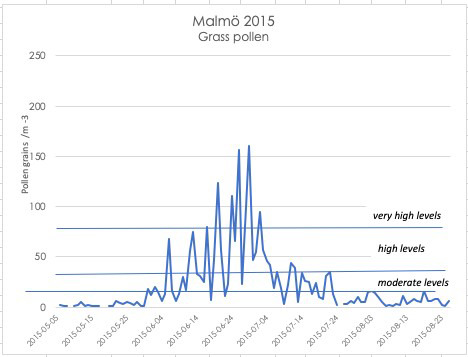
Grass pollen levels in Malmö, Sweden, measured daily during the study season period (May 19, 2015 to August 31, 2015)
3.3. Cognitive dysfunction during season
Impaired cognitive function was exhibited in the spatial working memory test (Figure 2), where the allergic group made significantly more errors compared to the non‐allergic group during pollen season, but not off‐season. In addition, the allergic group showed a tendency of worse strategy use in the spatial working memory test both during the pollen season and of‐season. In the attention tests of speed of response and movement, the allergic group had a tendency of delivering worse results with a higher mean value in many of the tested categories, specifically in speed of response (i.e. reaction times), both in comparison with the non‐allergic group during pollen season and the allergic group off‐season (Table 2). In the attention test of visual sustained attention, there were no differences between the allergic group and the controls in any of the measured parameters, neither during season nor off‐season.
FIGURE 2.
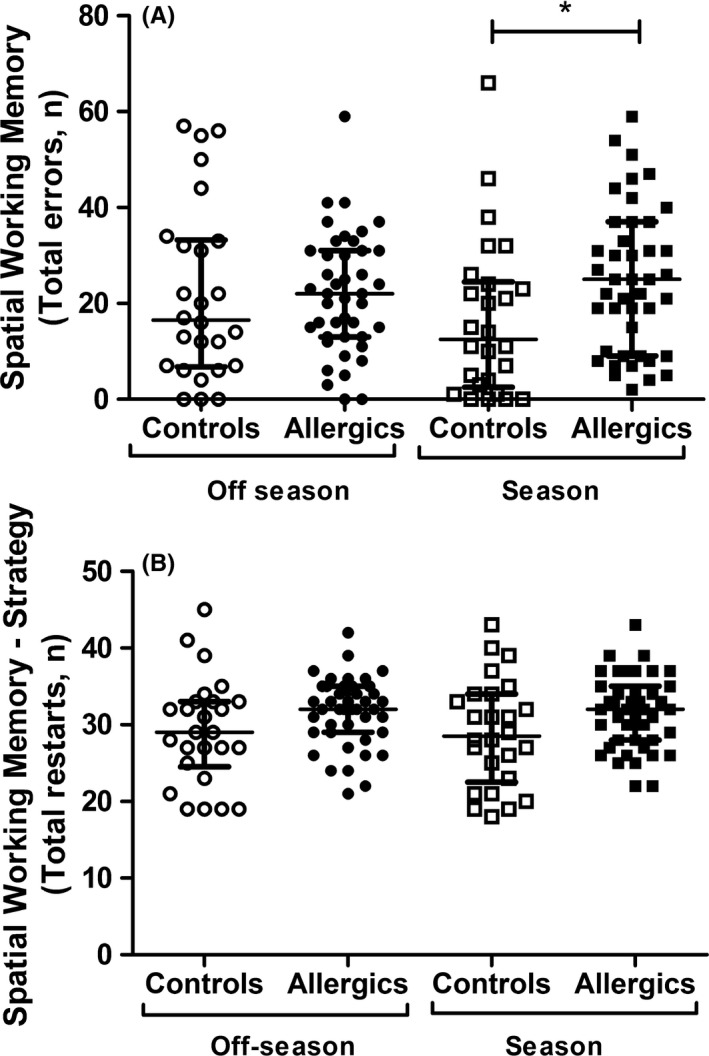
Spatial Working memory test results showing total errors (A) and total number of restarts (B) in allergic subjects and controls during off‐season and season. *p < .05 comparing allergic group and controls during pollen season
TABLE 2.
Cognitive test results from the CANTAB test in controls and allergic children off‐season and during season
| Off‐season | Season | p c | p d | |||||
|---|---|---|---|---|---|---|---|---|
| Controls | Allergics | p a | Controls | Allergics | p b | |||
| Paired associated learning (PAL)= Visual memory: episodic memory and learning | ||||||||
| Total errors | 3 (1‐6) | 3 (1‐6) | .93 | 3.5 (2‐6) | 4 (2‐8) | .61 | .60 | .37 |
| Total errors 6 shapes | 0 (0‐2) | 0 (0‐2) | .51 | 2 (0‐2) | 0 (0‐2) | .021 | .076 | .82 |
| Spatial Working Memory (SWM): working memory and strategy use | ||||||||
| Between errors | 17 (7‐33) | 22 (13‐31) | .53 | 13 (3‐25) | 25 (9‐37) | .020 | .018 | .13 |
| Strategy | 29 (25‐33) | 32 (29‐35) | .060 | 29 (23‐34) | 32 (28‐35) | .090 | 0.73 | 1.00 |
| Reaction time (RTI) = Attention test: speed of response and movement | ||||||||
| Simple reaction time | 276 (258‐321) | 305 (288‐343) | .030 | 290 (270‐330) | 312 (287‐363) | .069 | .22 | .13 |
| Simple movement time | 284 (249‐338) | 302 (247‐392) | .48 | 326 (286‐416) | 331 (275‐437) | .65 | .041 | .015 |
| Five‐choice reaction time | 317 (278‐341) | 328 (306‐376) | .10 | 324 (303‐367) | 341 (319‐396) | .16 | .002 | .050 |
| Five‐choice movement time | 309 (271‐364) | 321 (277‐417) | .63 | 340 (288‐388) | 343 (293‐440) | .58 | .43 | .32 |
| Rapid Visual Information Processing (RVIP) = Attention test: visual sustained attention | ||||||||
| A' | 0.86 (0.81‐0.90) | 0.86 (0.83‐0.89) | .59 | 0.86 (0.83‐0.88) | 0.85 (0.82‐0.89) | .77 | .43 | .17 |
| Probability of hit | 0.44 (0.32‐0.60) | 0.48 (0.37‐0.59) | .61 | 0.44 (0.33‐0.56) | 0.41 (0.33‐0.59) | .90 | .45 | .25 |
| Total false alarms | 1.0 (0.8‐4.0) | 2 (1‐3) | .73 | 2 (1‐4) | 2 (1‐4) | .43 | .39 | .14 |
| Latency | 384 (322‐464) | 364 (329‐457) | .82 | 384 (344‐477) | 382 (318‐476) | .50 | .40 | .21 |
Data are presented as median (IQR). p‐values for comparison of:
controls versus allergics during off‐season,
controls versus allergics during season
off‐season versus season in controls
off‐season versus season in allergics.
Bold values are significant values p < .05.
When analyzing results from only the allergic children that undertook the tests during days with high or very high pollen levels (n = 14+6 = 20), this allergic group similarly performed significantly worse compared to the total control group in the spatial working memory test, both in working memory (p = .031), but also in strategy use (p = .033). There were, however, no significant differences in the results from any of the other cognitive tests.
3.4. Quality of life and rhinitis symptoms
The DISABKIDS questionnaire revealed consistent differences between the two groups regarding the quality of life. A mental, social, and physical impairment was exhibited in the group of allergic children in comparison with the control group, both during the season and off‐season (Table 3). In addition, there was a physical impairment shown in the allergic children during pollen season compared to off‐season that could be read from the DISABKIDS questionnaire.
TABLE 3.
Health‐related quality of life Questionnaire scores in controls and allergic children off‐season and during season
| Off‐season | Season | p c | p d | |||||
|---|---|---|---|---|---|---|---|---|
| Controls | Allergics | p a | Controls | Allergics | p b | |||
| DISABKIDS | ||||||||
| Mental | 20 (20‐20) | 19 (17‐20) | <.001 | 20 (20‐20) | 18 (17‐19) | <.001 | .18 | .35 |
| Social | 20 (20‐20) | 19 (18‐20) | .001 | 20 (20‐20) | 19 (18‐20) | <.001 | .34 | .39 |
| Physical | 10 (10‐10) | 8 (7‐9) | <.001 | 10 (10‐10) | 8 (6‐9) | <.001 | .14 | .035 |
| Total | 50 (50‐50) | 46 (43‐49) | <.001 | 50 (50‐50) | 45 (40‐47) | <.001 | .18 | .12 |
| VAS | ||||||||
| Nose | 0 (0‐1) | 7 (5‐8) | <.001 | |||||
| Eyes | 0 (0‐0) | 6 (5‐8) | <.001 | |||||
| Lungs | 0 (0‐0) | 2 (0‐7) | <.001 | |||||
| Overall | 0 (0‐0) | 5 (4‐8) | <.001 | |||||
| Cross‐reactivity | 0 (0‐0) | 1 (0‐3) | <.001 | |||||
| Total | 0 (0‐2) | 22 (18‐30) | <.001 | |||||
| LILA | ||||||||
| Practical | 0 (0‐1) | 14 (9‐23) | <.001 | |||||
| Physical | 1 (0‐4) | 36 (25‐51) | <.001 | |||||
| Emotional | 0 (0‐0) | 2 (0‐5) | <.001 | |||||
| Total | 1 (0‐6) | 59 (41‐74) | <.001 | |||||
LILA: the Swedish version of Paediatric Allergic Disease Quality of Life. Data is presented as median (IQR). p‐values for comparison of:
controls versus allergics during off‐season,
controls versus allergics during season,
off‐season versus season in controls,
off‐season versus season in allergics. VAS definitions: Nose = secretion, congestion, itching and sneezing; Eyes = redness, itching, watery; Lungs = cough, breathlessness, wheezing, and asthmatics symptoms during exercise; Overall = general condition, fatigue, and impact in everyday life; Cross‐reactivity = itching and irritation in the mouth and throat, stomach pain.
Bold values are significant values p < .05.
A clear pattern was also exhibited in the VAS results during the pollen season, showing that allergic children scored higher points, and thereby had more symptoms, in comparison with the control group in all categories.
The disease‐specific questionnaire, LILA, also revealed an impaired quality of life in the group of allergic children in comparison with the control group during the pollen season.
3.5. Biomarkers of stress and inflammation
Cortisol was significantly higher during the season visit in comparison with off‐season in both allergic children and controls, but there were no significant differences between the groups at any time point (Table 4). No difference could be seen in levels of adrenalin or noradrenalin, neither between the groups nor between season and off‐season. Neither did the inflammatory biomarkers (IL‐13, TNFα, and TGF‐β) differ between the groups or between season and off‐season visits.
TABLE 4.
Biomarker concentration in controls and allergic children off‐season and during season
| Off‐season | Season | p c | p d | |||||
|---|---|---|---|---|---|---|---|---|
| Controls | Allergics | p a | Controls | Allergics | p b | |||
| Stress biomarkers | ||||||||
| Cortisol, nmol/L | 161 (122‐216) | 180 (122‐302) | .26 | 334 (192‐456) | 299 (180‐419) | .73 | <.001 | <.001 |
| Adrenalin, nmol/L | 0.26 (0.15‐0.39) | 0.18 (0.13‐0.27) | .061 | 0.21 (0.13‐0.29) | 0.20 (0.14‐0.28) | 8 | .27 | .82 |
| Noradrenalin, nmol/L | 2.9 (2.2‐3.5) | 2.5 (1.9‐3.1) | .15 | 2.5 (2.1‐3.5) | 2.5 (2.0‐3.5) | .57 | .88 | .53 |
| Inflammatory biomarkers | ||||||||
| IL‐13, pg/mL | 1326 (410‐5606) | 955 (125‐4458) | .45 | 1488 (281‐4919) | 809 (225‐3717) | .48 | .35 | .36 |
| TNF‐α, pg/mL | 7.1 (1.2‐47.4) | 9.7 (0.0‐66.7) | .99 | 7.3 (2.2‐66.4) | 7.5 (0.0‐60.8) | .63 | .82 | .35 |
| TGF‐β, ng/mL | 41 (30‐44) | 40 (31‐46) | .99 | 46 (30‐56) | 38 (32‐47) | .26 | .14 | .92 |
Data is presented as median (IQR). Results below detection limit were set as 0. IL‐13 = interleukin‐13, TNF‐α = tumor necrosis factor alpha, TGF‐β = transforming growth factor‐beta.
p‐values for comparison of:
controls versus allergics during off‐season,
controls versus allergics during season,
off‐season versus season in controls,
off‐season versus season in allergics.
Bold values are significant values p < .05.
3.6. Associations between cognitive function and symptom score
There was an overall conformity showed by a correlation between scores in all the questionnaires (VAS, DISABKIDS, and LILA) within the allergic children during season (p < .0001). In addition, reaction time for simple movement correlates negatively to total DISABKIDS score (p = .007, r=−0.42) and positively to total LILA score (p = .030, r = 0.35) during pollen season, showing that the poorer quality of life the allergic children had, the longer the reaction time for simple movement. When separating the total scores of the DISABKIDS and LILA questionnaires into their respective sections, there was a significant correlation between the reaction time for simple movement and all of the separate sections. Similar correlations to symptoms were shown for the other reaction time parameters, but not significant. In addition, a significant correlation (r = 0.36, p = .022) between grass pollen level and change in five‐choice reaction time from off‐season to season was found in the allergic group.
No correlations were found between cognitive function and stress factors (cortisol, adrenalin, or noradrenalin) or inflammatory biomarkers (IL‐13, TNFα, and TGF‐β) in neither allergic children nor controls, and neither during season nor off‐season.
4. DISCUSSION
The present study shows that the allergic group delivered an increased amount of total errors in specific measurements of spatial working memory during the pollen season compared to the control group. No other cognitive deficits were shown to be significant in the allergic group although this was a group of children with an impaired quality of life and troublesome symptoms. However, the poorer quality of life and the more symptoms the allergic children had, the longer the reaction time for simple movement.
The effect on cognitive function in allergic patients shown in previous studies is not uniform, and it is difficult to compare due to different cognitive tests and study populations. Though, many studies reveal an impact of allergic rhinitis on some but not all cognitive functions, it has been shown that untreated allergic patients experience a subtle slowed speed of cognitive processing and to some extent difficulties in working memory, but not deficits in attention and recent memory. 22 In the present study, an overall higher median reaction time was longer during the season for the allergic group in comparison with the same group outside the season but did not reach statistical significance. This is in contrast to a previous study, 23 where the allergic subjects were submitted to tests after having experienced symptoms for 2 weeks, with a discontinuation of all treatment 7 days before taking the tests. Though, in our study, tests were conducted randomly throughout the season (which during 2015 was a season with relatively low pollen levels overall) and participants were treated daily with antihistamines and nasal steroids during the season, which might explain the discrepancies. The sedative effect of many antihistamines is well known, but many second‐generation antihistamines, such as desloratadine (which is the first choice antihistamine according to Regional guidelines), have been found to be non‐sedating and appeared to have no cognitive effects in a previous study. 24
Despite daily treatment with antihistamines and nasal steroids, both the generic (DISABKIDS) and the disease‐specific (LILA and VAS) health‐related Quality of Life questionnaires revealed poorer quality of life and more symptoms in the allergic children compared to the control group. This impaired quality of life was obvious also during the off‐season visit in the allergic group and the only difference being an increase in physical symptoms during the season, as revealed by the DISABKIDS questionnaire. As expected, the control group did not report any significant symptoms that could be clinically related to allergy and thereby affect the study results.
Previous studies have shown that respiratory allergies can affect the performance of young people in school through lack of concentration and insomnia, which in turn leads to daytime sleepiness. The disease itself is considered to give a significant fatigue. Although it seems likely that cognitive dysfunction is present during the pollen season, it was previously not directly connected to the degree of usual symptoms. 23 In the present study, we showed that the more symptoms the allergic children had, the longer the reaction time for simple movement. In contrast to many previous studies, we investigated a population with physician verified diagnosis of severe allergic rhinitis and not just self‐reported, which might explain this discrepancy.
Visual sustained attention (RVIP) did not appear to be affected in the allergic group in the present study, which might be due to a short average test duration (7 minutes). When measured by a 45‐minute test 25 , sustained attention was impaired shortly after nasal provocation, but no effect on short‐term cognitive performance. Similarly, another study showed that ragweed‐induced allergic rhinitis decreased attentiveness and decremented both speed and efficiency across several cognitive domains 24 .
It is unclear whether troublesome allergy symptoms phenomenon is a result of biologic stress, 26 but there is some evidence that the circadian rhythm of cortisol in patients with allergic rhinitis is flattened when compared to healthy non‐allergic individuals. 27 , 28 There is also some evidence that the response to stress is differentiated in the allergic patients. 29 .The results from the present study show an increase in cortisol during pollen season, both in the allergic group and the controls. This might be due an effect of circadian change of cortisol concentration in relation to annual variation in daily light exposure. 30 The hypothesis of stress induced higher cortisol levels in allergics could not be confirmed, but a potential increase in cortisol in the allergic group might have been eliminated by the use of nasal corticosteroids. 31
In this study, IL‐13 was used as a biomarker of the type‐2 response, but was not affected in relation to pollen season which might be due to the use of nasal corticosteroids. 32 Neither was there any difference in TNF‐alpha nor TGF‐beta during season compared to off‐season. The initial hypothesis was that TNF‐alpha and TGF‐beta would reflect systemic inflammation that could be induced during the allergen‐induced stress status. Maybe other biomarkers that might be more related to neurologic stress would be more useful.
When it comes to reaction time for simple movement and five‐choice reaction time (Table 2), the allergic children and the controls show the same significant pattern of significantly higher reaction times during season compared to off‐season, which is in conjunction with a previous large study. 33 Though, the numerical values indicate worse problems in allergics, which show higher median reaction times compared to controls in all reaction time variables. The longer reaction time during season is probably due to other factors than allergic rhinitis, and may be due to for example a higher ambient temperature during season. Unfortunately, we have not measured ambient temperature at the visits, but the pollen levels may give us a hint since nice weather often goes with higher pollen levels. This hypothesis may then be confirmed in the correlation between grass pollen level and change in five‐choice reaction time from off‐season to season was found in the allergic group. More research is needed to answer this question.
The control group's results at spatial working memory also deserve a comment. The differences between the allergic group and controls seem logic (Table 2); that is, the allergic group has a tendency of worse spatial working memory during season compared to off‐season (although not significant) and worse values during season as well as off‐season compared to the controls. However, in “between errors” of spatial working memory, control children do less faults in spatial working memory during season compared to off‐season. This is difficult to interpret since there is no effect of learning in this study (i.e., no difference is shown between those who do their first visit during off‐season versus those that do their first visit during season) and the increase in reaction time during season point in the opposite direction.
One of the main problems in conducting studies on allergic subjects is difficulties for forecasting pollen levels at the time of the tests. Unfortunately, during the summer of 2015 when the study was conducted, there were only a few days with high or very high levels of pollen, which might have affected the results. 34 However, when investigating results from visits during these days only, in addition to spatial working memory dysfunction, a significantly worse strategy use was then seen in the allergic children. This strengthens the hypothesis of impaired cognitive function due to pollen exposure in these children. A short exposure may be sufficient for noticing immediate results of inflammation such as rhinitis symptoms and fatigue, while the cognitive impairment might be even more evident after higher and longer exposure. Grass pollen‐allergic individuals though tend to avoid exposure by staying indoors, which is an independent factor that probably diminishes the inflammation mechanism.
A limitation of this study might be the age span among the children. A narrower age span of might have narrowed the results, but the CANTAB tests are recommended for this age group and the wider age span was therefore chosen. The study was relatively small, which might have underpowered the results. Significant impairment of cognitive dysfunction in allergic children can though be found and maybe more differences, which have been shown in other studies 23 and could have be revealed in a large setting. Another factor is the psychologic comorbidities that might affected cognitive skills. Pediatric patients with allergic rhinitis has been shown to have a substantially increased rate of attention deficit/hyperactivity disorder (ADHD). 35 The scores of hyperactivity/impulsivity subscales of ADHD symptoms were significantly higher in the allergic rhinitis children and revealed higher commission errors, shorter reaction times, and more perseveration, 36 and their ADHD scores decreased significantly after allergy treatment. 37 Unfortunately, this study did not screen for ADHD scores or ADHD diagnosis, but the prevalence of ADHD among children in Sweden is about 5‐7% in this age group, and the large majority of them are under medication. Statistically, there would be only a very few of the participants in this study that would have an ADHD diagnosis, and this would most probably not affect the results of the study significantly. It would though be interesting to investigate ADHD scores in these children as well as in relation to pollen season and specifically compare state markers and endophenotype markers of ADHD in allergic rhinitis children. 38
A strength of this study is the real‐life design. The achievements were recorded during regular school days, and the teenagers used their allergic medicines (non‐sedative antihistamines, nasal steroids, and eye drops) as usual. The use of the CANTAB instrument was also a strength since this tool is well documented and recommended in clinical evaluation.
Further research is needed to clarify the relationship between allergic rhinitis and specific cognitive dysfunction to clinically help children with allergic rhinitis in their daily life. Future research projects in this area should consider the use of other CANTAB variables in other test panels to reveal defined cognitive impairment. Investigating a larger population in a more limited age range could maybe also expose age‐dependent effects of cognitive impairment in various daily life situations. It would also be interesting to valuate other biomarkers that might be of interest in relation to neurologic stress.
In summary, we show that cognitive function of pollen‐allergic children was affected during pollen season, and the more symptoms the allergic children had, the longer the reaction time for simple movement. Cognitive dysfunction was, however, not associated with levels of serum biomarkers related to stress or inflammation. This study demonstrates the importance of an understanding in the society that children with pollen allergy and troublesome symptoms have impaired cognitive function during season, which can have a further effect in their daily lives.
CONFLICT OF INTEREST
None declared.
AUTHOR CONTRIBUTION
Georgia Papapostolou: Conceptualization (equal); Data curation (equal); Formal analysis (equal); Investigation (equal); Writing‐original draft (equal). Hampus Kiotseridis: Conceptualization (equal); Data curation (equal); Investigation (equal); Resources (equal); Validation (equal); Writing‐review & editing (equal). Kerstin Romberg: Conceptualization (equal); Investigation (equal); Resources (equal); Writing‐review & editing (equal). Åslög Dahl: Investigation (equal); Methodology (equal); Writing‐review & editing (equal). Leif Bjermer: Conceptualization (equal); Investigation (equal); Project administration (equal); Supervision (equal); Validation (equal); Writing‐review & editing (equal). Magnus Lindgren: Conceptualization (equal); Formal analysis (equal); Investigation (equal); Methodology (equal); Software (lead); Supervision (equal); Writing‐review & editing (equal). David Aronsson: Formal analysis (equal); Investigation (equal); Validation (equal); Writing‐review & editing (equal). Alf Tunsäter: Conceptualization (equal); Formal analysis (equal); Funding acquisition (equal); Investigation (equal); Methodology (equal); Project administration (lead); Supervision (equal); Writing‐review & editing (equal). Ellen Tufvesson: Conceptualization (equal); Data curation (equal); Formal analysis (lead); Investigation (equal); Project administration (equal); Resources (equal); Supervision (equal); Validation (equal); Visualization (equal); Writing‐original draft (equal).
Peer Review
The peer review history for this article is available at https://publons.com/publon/10.1111/pai.13328.
ACKNOWLEDGMENTS
We thank Gunill‐Louise Femtvik and Agnetha Roswall for helping out in patient testing and Ida Åberg for performing biomarker analyses.
Papapostolou G, Kiotseridis H, Romberg K, et al. Cognitive dysfunction and quality of life during pollen season in children with seasonal allergic rhinitis. Pediatr Allergy Immunol. 2021;32:67–76. 10.1111/pai.13328
Alf Tunsäter and Ellen Tufvesson shared last authorship.
Funding information
This work was supported by independent research grants from the Swedish Heart and Lung Foundation, the Swedish Asthma and Allergy Foundation, the Crafoord Foundation, and the Medical Faculty of Lund University.
REFERENCES
- 1. Beasley R. Worldwide variation in prevalence of symptoms of asthma, allergic rhinoconjunctivitis, and atopic eczema: ISAAC. Lancet. 1998;351(9111):1225–1232. [PubMed] [Google Scholar]
- 2. Eriksson J, Bjerg A, Lotvall J, et al. Rhinitis phenotypes correlate with different symptom presentation and risk factor patterns of asthma. Respir Med. 2011;105(11):1611–1621. [DOI] [PubMed] [Google Scholar]
- 3. Bousquet J, van Cauwenberge P, Khaltaev N. Allergic rhinitis and its impact on asthma. J Allergy Clin Immunol. 2001;108(5):S147–S334. [DOI] [PubMed] [Google Scholar]
- 4. Kiotseridis H, Cilio CM, Bjermer L, et al. Quality of life in children and adolescents with respiratory allergy, assessed with a generic and disease‐specific instrument. Clin Respir J. 2013;7(2):168–175. [DOI] [PubMed] [Google Scholar]
- 5. Bousquet J, Khaltaev N, Cruz AA, et al. Allergic rhinitis and its impact on asthma (ARIA) 2008 update (in collaboration with the World Health Organization, GA(2)LEN and AllerGen). Allergy. 2008;63(Suppl 86):8–160. [DOI] [PubMed] [Google Scholar]
- 6. Stuck BA, Czajkowski J, Hagner AE, et al. Changes in daytime sleepiness, quality of life, and objective sleep patterns in seasonal allergic rhinitis: a controlled clinical trial. J Allergy Clin Immunol. 2004;113(4):663–668. [DOI] [PubMed] [Google Scholar]
- 7. Hammersley V, Walker S, Sheikh A. Is it unfair to hayfever sufferers to have to sit examinations during periods of high pollen counts? Expert Rev Respir Med. 2010;4(4):421–425. [DOI] [PubMed] [Google Scholar]
- 8. Meltzer EO. Introduction: stuffy is also related to Sleepy and Grumpy–the link between rhinitis and sleep‐disordered breathing. J Allergy Clin Immunol. 2004;114(5 Suppl):S133–4. [DOI] [PubMed] [Google Scholar]
- 9. Hill CM, Hogan AM, Onugha N, Harrison D, Cooper S, McGrigor VJ, et al. Increased cerebral blood flow velocity in children with mild sleep‐disordered breathing: a possible association with abnormal neuropsychological function. Pediatrics. 2006;118(4):e1100–e1108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Walker S, Khan‐Wasti S, Fletcher M, Cullinan P, Harris J, Sheikh A. Seasonal allergic rhinitis is associated with a detrimental effect on examination performance in United Kingdom teenagers: case‐control study. J Allergy Clin Immunol. 2007;120(2):381–387. [DOI] [PubMed] [Google Scholar]
- 11. Juniper EF, Guyatt GH, Dolovich J. Assessment of quality of life in adolescents with allergic rhinoconjunctivitis: development and testing of a questionnaire for clinical trials. J Allergy Clin Immunol. 1994;93(2):413–423. [DOI] [PubMed] [Google Scholar]
- 12. Bensnes SS. You sneeze, you lose: the impact of pollen exposure on cognitive performance during high‐stakes high school exams. J Health Econ. 2016;49:1–13. [DOI] [PubMed] [Google Scholar]
- 13. Luciana M. Practitioner review: computerized assessment of neuropsychological function in children: clinical and research applications of the Cambridge Neuropsychological Testing Automated Battery (CANTAB). J Child Psychol Psychiatry Allied Discipl. 2003;44(5):649–663. [DOI] [PubMed] [Google Scholar]
- 14. Yamasaki A, Burks CA, Bhattacharyya N. Cognitive and quality of life‐related burdens of illness in pediatric allergic airway disease. Otolaryngol Head Neck Surg. 2020;162(4):566–571. [DOI] [PubMed] [Google Scholar]
- 15. Marcotte DE. Allergy test: Seasonal allergens and performance in school. Journal of health economics. 2015;40:132–40. [DOI] [PubMed] [Google Scholar]
- 16. Borres MP. Allergic rhinitis: more than just a stuffy nose. Acta Paediatr. 2009;98(7):1088–1092. [DOI] [PubMed] [Google Scholar]
- 17. Julvez J, Torrent M, Guxens M, Antó JM, Guerra S, Sunyer J. Neuropsychologic status at the age 4 years and atopy in a population‐based birth cohort. Allergy. 2009;64(9):1279–1285. [DOI] [PubMed] [Google Scholar]
- 18. Bullinger M, Schmidt S, Petersen C. Assessing quality of life of children with chronic health conditions and disabilities: a European approach. Int J Rehabil Res. 2002;25(3):197–206. [DOI] [PubMed] [Google Scholar]
- 19. Bousquet PJ, Combescure C, Neukirch F, Klossek JM, Mechin H, Daures JP, et al. Visual analog scales can assess the severity of rhinitis graded according to ARIA guidelines. Allergy. 2007;62(4):367–72. [DOI] [PubMed] [Google Scholar]
- 20. Kiotseridis H, Cilio CM, Bjermer L, Aurivillius M, Jacobsson H, Tunsater A. Swedish translation and validation of the Pediatric Allergic Disease Quality of Life Questionnaire (PADQLQ). Acta Paediatr. 2011;100(2):242–247. [DOI] [PubMed] [Google Scholar]
- 21. Roberts G, Hurley C, Lack G. Development of a quality‐of‐life assessment for the allergic child or teenager with multisystem allergic disease. J Allergy Clin Immunol. 2003;111(3):491–497. [DOI] [PubMed] [Google Scholar]
- 22. Marshall PS, O'Hara C, Steinberg P. Effects of seasonal allergic rhinitis on selected cognitive abilities. Ann Allergy, Asthma Immunol. 2000;84(4):403–410. [DOI] [PubMed] [Google Scholar]
- 23. Trikojat K, Buske‐Kirschbaum A, Schmitt J, Plessow F. Altered performance in attention tasks in patients with seasonal allergic rhinitis: seasonal dependency and association with disease characteristics. Psychol Med. 2015;45(6):1289–1299. [DOI] [PubMed] [Google Scholar]
- 24. Wilken JA, Berkowitz R, Kane R. Decrements in vigilance and cognitive functioning associated with ragweed‐induced allergic rhinitis. Ann Allergy Asthma Immunol. 2002;89(4):372–380. [DOI] [PubMed] [Google Scholar]
- 25. Hartgerink‐Lutgens I, Vermeeren A, Vuurman E, Kremer B. Disturbed cognitive functions after nasal provocation in patients with seasonal allergic rhinitis. Clin Exp Allergy. 2009;39(4):500–508. [DOI] [PubMed] [Google Scholar]
- 26. Soler ZM, Eckert MA, Storck K, Schlosser RJ. Cognitive function in chronic rhinosinusitis: a controlled clinical study. Int Forum Allergy Rhinol. 2015;5(11):1010–1017. [DOI] [PubMed] [Google Scholar]
- 27. den Hartog HM, Nicolson NA, Derix MM, van Bemmel AL, Kremer B, Jolles J. Salivary cortisol patterns and cognitive speed in major depression: a comparison with allergic rhinitis and healthy control subjects. Biol Psychol. 2003;63(1):1–14. [DOI] [PubMed] [Google Scholar]
- 28. Fidan V, Alp HH, Gozeler M, Karaaslan O, Binay O, Cingi C. Variance of melatonin and cortisol rhythm in patients with allergic rhinitis. Am J Otolaryngol. 2013;34(5):416–419. [DOI] [PubMed] [Google Scholar]
- 29. Wamboldt MZ, Laudenslager M, Wamboldt FS, Kelsay K, Hewitt J. Adolescents with atopic disorders have an attenuated cortisol response to laboratory stress. J Allergy Clin Immunol. 2003;111(3):509–514. [DOI] [PubMed] [Google Scholar]
- 30. Adamsson M, Laike T, Morita T. Annual variation in daily light exposure and circadian change of melatonin and cortisol concentrations at a northern latitude with large seasonal differences in photoperiod length. J Physiol Anthropol. 2016;36(1):6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Masharani U, Shiboski S, Eisner MD, Katz PP, Janson SL, Granger DA, et al. Impact of exogenous glucocorticoid use on salivary cortisol measurements among adults with asthma and rhinitis. Psychoneuroendocrinology. 2005;30(8):744–752. [DOI] [PubMed] [Google Scholar]
- 32. al Ghamdi K, Ghaffar O, Small P, Frenkiel S, Hamid Q. IL‐4 and IL‐13 expression in chronic sinusitis: relationship with cellular infiltrate and effect of topical corticosteroid treatment. J Otolaryngol. 1997;26(3):160–166. [PubMed] [Google Scholar]
- 33. Didikoglu A, Canal MM, Pendleton N, Payton A. Seasonality and season of birth effect in the UK Biobank cohort. Am J Human Biol. e23417. [DOI] [PubMed] [Google Scholar]
- 34. Roberts G, Mylonopoulou M, Hurley C, Lack G. Impairment in quality of life is directly related to the level of allergen exposure and allergic airway inflammation. Clin Exp Allergy. 2005;35(10):1295–1300. [DOI] [PubMed] [Google Scholar]
- 35. Tsai MC, Lin HK, Lin CH, Fu LS. Prevalence of attention deficit/hyperactivity disorder in pediatric allergic rhinitis: a nationwide population‐based study. Allergy Asthma Proc. 2011;32(6):41–46. [DOI] [PubMed] [Google Scholar]
- 36. Yang MT, Lee WT, Liang JS, Lin YJ, Fu WM, Chen CC. Hyperactivity and impulsivity in children with untreated allergic rhinitis: corroborated by rating scale and continuous performance test. Pediatr Neonatol. 2014;55(3):168–174. [DOI] [PubMed] [Google Scholar]
- 37. Yang MT, Chen CC, Lee WT, Liang JS, Fu WM, Yang YH. Attention‐deficit/hyperactivity disorder‐related symptoms improved with allergic rhinitis treatment in children. Am J Rhinol Allergy. 2016;30(3):209–214. [DOI] [PubMed] [Google Scholar]
- 38. Gau SS, Huang WL. Rapid visual information processing as a cognitive endophenotype of attention deficit hyperactivity disorder. Psychol Med. 2014;44(2):435–446. [DOI] [PubMed] [Google Scholar]