
Figure 2.
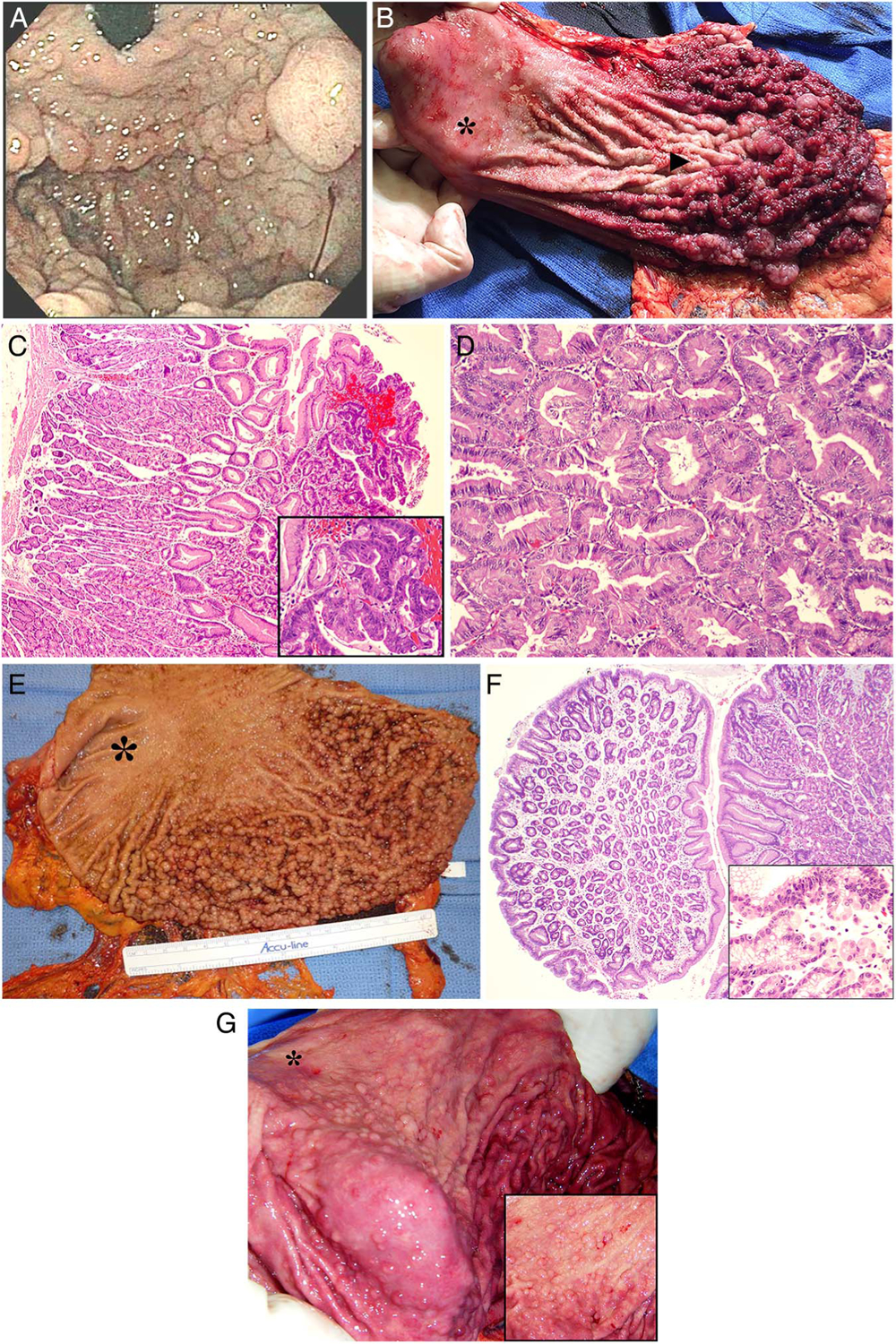
Endoscopy, gastrectomy and histopathology of family members affected by gastric adenocarcinoma and proximal polyposis of the stomach. (A) Retroflexed gastric endoscopy in patient I-1 showing fundic polyposis. (B) Total gastrectomy specimen opened at lesser curvature shows polyposis in the fundus, cardia and body of the stomach (arrowhead) with typical non-involvement of the antrum (asterisk). (C) Fundic gland polyp with high-grade dysplasia (inset 20×) in gastrectomy specimen of patient I-1. (D) T1a well-differentiated intestinal-type gastric adenocarcinoma at lesser curvature in patient (I-1). (E) Gastric polyposis with antral sparing (asterisk) in patient II-11. (F) Fundic gland polyp with focal area of low-grade dysplasia in patient II-11. (G) Gastrectomy specimen from patient II-12 showing diffuse gastric polyposis with antral sparing (asterisk). Inset shows direct view of polyps in the fundus (zoomed in).