

Abstract
Alterations in brain functioning, especially in regions associated with cognition, can result from infection with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and are predicted to result in various psychiatric diseases. Recent studies have shown that SARS-CoV-2 infection and coronavirus disease 2019 (COVID-19) can directly or indirectly affect the central nervous system (CNS). Therefore, diseases associated with sequelae of COVID-19, or ‘long COVID’, also include serious long-term mental and cognitive changes, including the condition recently termed ‘brain fog’. Hypoxia in the microenvironment of select brain areas may benefit the reproductive capacity of the virus. It is possible that in areas of cerebral hypoxia, neuronal cell energy metabolism may become compromised after integration of the viral genome, resulting in mitochondrial dysfunction. Because of their need for constant high metabolism, cerebral tissues require an immediate and constant supply of oxygen. In hypoxic conditions, neurons with the highest oxygen demand become dysfunctional. The resulting cognitive impairment benefits viral spread, as infected individuals exhibit behaviors that reduce protection against infection. The effects of compromised mitochondrial function may also be an evolutionary advantage for SARS-CoV-2 in terms of host interaction. A high viral load in patients with COVID-19 that involves the CNS results in the compromise of neurons with high-level energy metabolism. Therefore, we propose that selective neuronal mitochondrial targeting in SARS-CoV-2 infection affects cognitive processes to induce ‘brain fog’ and results in behavioral changes that favor viral propagation. Cognitive changes associated with COVID-19 will have increasing significance for patient diagnosis, prognosis, and long-term care.
MeSH Keywords: Coronavirus; COVID-19; Hypoxia, Brain; Mitochondria
Cerebral infection with SARS-CoV-2 results in acute and chronic pathologic changes [1–3]. Because this new pandemic infection has been studied clinically for less than a year, the long-term effects on the CNS, including whether SARS-CoV-2 causes or accelerates the clinical course of neurodegenerative diseases, such as Parkinson disease and Alzheimer disease, remain unknown [1]. Interestingly, there have now been several studies that have shown that infection with SARS-CoV-2 affects cognitive function and is associated with mental illness, including depression, and developmental or functional CNS changes, including autism [4–13]. Recently, patients with COVID-19 and CNS involvement have shown psychological symptoms, behavioral changes, cognitive impairment, confusion, and poor concentration; collectively termed ‘brain fog’ [14].
It is now known that the initial pulmonary infection with SARS-CoV-2 damages the alveoli and impairs alveolar oxygenation. COVID-19 pneumonia can result in acute respiratory distress syndrome, hypoxemia, and acidosis [15–17]. The degree of initial lung damage can determine the long-term effects of infection and may be associated with acute and chronic changes in the heart and CNS [15–17]. Recent modeling data have shown that the genomic and subgenomic RNA (sgRNA) transcripts of SARS-CoV-2 can take over the host cell by involving the mitochondrial matrix and nucleolus [18]. It is possible that SARS-CoV-2 can directly impair mitochondrial energy metabolism via targeted action on oxygen availability and utilization [18–20]. Importantly, these effects may result from the integration of the viral genome into the host cell mitochondrial matrix, resulting in a viral-mitochondrial interaction or viral ‘hijacking’ of the mitochondrial genome [18–20]. This viral-mitochondrial interaction depends on enhanced energy and reduced host immune responsiveness, promoting viral replication and survival [19–21]. Therefore, these pathological effects of SARS-CoV-2 infection may explain the long-term psychiatric, cognitive, and neurodegenerative sequelae of CNS infection (Figure 1) [13]. Also, the generation of an effective host immune response will be impaired when the available mitochondrial energy is reduced [13].
Figure 1.
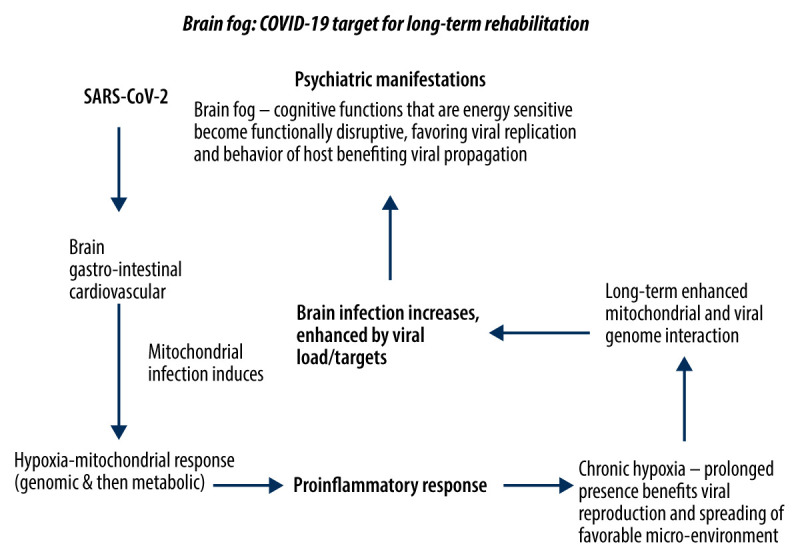
‘Brain fog’ and COVID-19 targeting for long-term rehabilitation. SARS-CoV-2, which causes COVID-19, can infect the lungs, CNS, gastrointestinal system, and cardiovascular system. With time, widespread infection increases the total viral load in the infected individual. SARS-CoV-2 can integrate its genome into mitochondria to reduce energy metabolism. The brain is especially vulnerable to hypoxia because cognitive neural processes adjust poorly to hypoxic conditions. Hypoxia is also pro-inflammatory. Therefore, as the viral load increases, cognitive impairment and confusion increase, a condition known as ‘brain fog’. This ongoing cascade of neuronal dysfunction is an important factor in understanding the long-term pathogenesis of CNS infection with SARS-CoV-2. Importantly, the behaviors resulting from ‘brain fog’ may increase the spread of SARS-CoV-2. COVID-19 – coronavirus disease 2019; SARS-CoV-2 – severe acute respiratory syndrome coronavirus 2; CNS – central nervous system.
The role of impaired mitochondrial function and energy metabolism in SARS-CoV-2 infection may also explain the development of impaired cognitive function in CNS infection. Mitochondria evolved from bacteria, and retain the ability to move between cells and toward hypoxic microenvironments, as well as to exist in extracellular environments such as cerebrospinal fluid [21–24]. We previously speculated that mitochondria represent the initial step in the cellular stress response [25]. Their unique oxygen-sensitive functions highlight the significance of mitochondria in initiating pro-inflammatory reactions [25].
It has previously been reported that several neurological disorders can be initiated by chronic inflammation [26,27]. Physiological stress caused by inflammation can increase susceptibility to viral infection [26,27]. Given the dependence of neural tissue on high oxygen levels, the effects of mitochondrial dysfunction associated with SARS-CoV-2 infection may underlie the observed COVID-19-associated neurological effects [26,27]. Targeted involvement of the mitochondria in SARS-CoV-2 may also involve mitochondrial synchronization in multiple cells [27–29]. Combined with its induced pro-inflammatory response, SARS-CoV-2 infection leads to neuronal dysfunction, resulting in ‘brain fog’, as cognition requires a high and uninterrupted supply of oxygen (Figure 1) [3]. If energy metabolism is compromised, the resulting impairment of the immune response serves to increase the spread of the virus within an individual and between individuals. Therefore, the development of ‘brain fog’ as a long-term outcome of SARS-CoV-2 infection may be considered to be an evolutionarily conserved and strategic mechanism on the part of the virus that aids its spread and survival.
Conclusions
Recent studies and clinical observations of SARS-CoV-2 infections have yielded insights into the cellular and physiological processes that enhance the ability of the virus to reproduce and spread, including its need for a highly oxygenated microenvironment [28]. Recently, there has been an increased understanding of the possible role of compromised mitochondria in the pathogenesis of SARS-CoV-2 infection. Mitochondrial energy metabolism responds immediately to a hypoxic microenvironment, and mitochondria can serve as mobile sentinel organelles that can act together as an energy delivery system [25]. Given the high energy and oxygenation requirements in neural tissue, mitochondria can serve as indicators of early acute neuronal dysfunction. The relationship between cognitive function, mental health, virus susceptibility, and viral infectivity may be a function of CNS viral load, which increases with time in the case of ‘long-term COVID’. The resulting cognitive impairment benefits viral spread, as infected individuals exhibit reduced anti-infection behaviors (Figure 1). The effects of compromised mitochondrial function may also be an evolutionary advantage for SARS-CoV-2 in terms of its interaction with the host. A high viral load in COVID-19 patients that involves the CNS results in the compromise of neurons with high levels of energy metabolism. Therefore, we propose that selective neuronal mitochondrial targeting in SARS-CoV-2 infection affects cognitive processes to induce ‘brain fog’ and results in behavioral changes that favor viral survival and propagation. Cognitive changes associated with COVID-19 will have increasing significance in patient diagnosis, prognosis, and long-term care. Therefore, there will be an increasing need for support for mental health issues related to COVID-19. Long-term therapeutic strategies for COVID-19 should combine pharmacological agents targeting a chronic ischemic neural pro-inflammatory environment with behavioral activities to restore cognitive function [29,30].
Footnotes
Conflict of interest
None.
Source of support: Progress psychologie 1. LF UK
References
- 1.Wang F, Kream RM, Stefano GB. Long-term respiratory and neurological sequelae of COVID-19. Med Sci Monit. 2020;26:e928996. doi: 10.12659/MSM.928996. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Chen X, Laurent S, Onur OA, et al. A systematic review of neurological symptoms and complications of COVID-19. J Neurol. 2020;20:1–11. doi: 10.1007/s00415-020-10067-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Pezzini A, Padovani A. Lifting the mask on neurological manifestations of COVID-19. Nat Rev Neurol. 2020;16(11):636–44. doi: 10.1038/s41582-020-0398-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Lau KK, Yu WC, Chu CM, et al. Possible central nervous system infection by SARS coronavirus. Emerg Infect Dis. 2004;10(2):342–44. doi: 10.3201/eid1002.030638. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Tsai LK, Hsieh ST, Chao CC, et al. Neuromuscular disorders in severe acute respiratory syndrome. Arch Neurol. 2004;61(11):1669–73. doi: 10.1001/archneur.61.11.1669. [DOI] [PubMed] [Google Scholar]
- 6.Correa-Palacio AF, Hernandez-Huerta D, Gomez-Arnau J, et al. Affective psychosis after COVID-19 infection in a previously healthy patient: A case report. Psychiatry Res. 2020;290:113115. doi: 10.1016/j.psychres.2020.113115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Chandra PS, Shiva L, Nagendrappa S, et al. COVID 19 related psychosis as an interface of fears, socio-cultural issues and vulnerability – case report of two women from India. Psychiatry Res. 2020;290:113136. doi: 10.1016/j.psychres.2020.113136. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Mawhinney JA, Wilcock C, Haboubi H, Roshanzamir S. Neurotropism of SARS-CoV-2: COVID-19 presenting with an acute manic episode. BMJ Case Rep. 2020;13(6):e236123. doi: 10.1136/bcr-2020-236123. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Beach SR, Praschan NC, Hogan C, et al. Delirium in COVID-19: A case series and exploration of potential mechanisms for central nervous system involvement. Gen Hosp Psychiatry. 2020;65:47–53. doi: 10.1016/j.genhosppsych.2020.05.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Epstein D, Andrawis W, Lipsky AM, et al. Anxiety and suicidality in a hospitalized patient with COVID-19 infection. Eur J Case Rep Intern Med. 2020;7(5):001651. doi: 10.12890/2020_001651. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Chen N, Zhou M, Dong X, et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet. 2020;395(10223):507–13. doi: 10.1016/S0140-6736(20)30211-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Zhang Y, Ma ZF. Impact of the COVID-19 pandemic on mental health and quality of life among local residents in Liaoning province, China: A cross-sectional study. Int J Environ Res Public Health. 2020;17(7):2381. doi: 10.3390/ijerph17072381. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Ptacek R, Ptackova H, Martin A, Stefano GB. Psychiatric manifestations of COVID-19 and their social significance. Med Sci Monit. 2020;26:e930340. doi: 10.12659/MSM.930340. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Croall ID, Hoggard N, Aziz I, et al. Brain fog and non-coeliac gluten sensitivity: Proof of concept brain MRI pilot study. PLoS One. 2020;15(8):e0238283. doi: 10.1371/journal.pone.0238283. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Calabrese F, Pezzuto F, Fortarezza F, et al. Pulmonary pathology and COVID-19: Lessons from autopsy. The experience of European Pulmonary Pathologists. Virchows Arch. 2020;477(3):359–72. doi: 10.1007/s00428-020-02886-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Tian S, Xiong Y, Liu H, et al. Pathological study of the 2019 novel coronavirus disease (COVID-19) through postmortem core biopsies. Mod Pathol. 2020;33(6):1007–14. doi: 10.1038/s41379-020-0536-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Xu Z, Shi L, Wang Y, et al. Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Respir Med. 2020;8(4):420–22. doi: 10.1016/S2213-2600(20)30076-X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Wu KE, Fazal FM, Parker KR, et al. RNA-GPS Predicts SARS-CoV-2 RNA residency to host mitochondria and nucleolus. Cell Syst. 2020;11(1):102–108.e3. doi: 10.1016/j.cels.2020.06.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Shenoy S. Coronavirus (Covid-19) sepsis: Revisiting mitochondrial dysfunction in pathogenesis, aging, inflammation, and mortality. Inflamm Res. 2020;69(11):1077–85. doi: 10.1007/s00011-020-01389-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Singh KK, Chaubey G, Chen JY, Suravajhala P. Decoding SARS-CoV-2 hijacking of host mitochondria in COVID-19 pathogenesis. Am J Physiol Cell Physiol. 2020;319(2):C258–67. doi: 10.1152/ajpcell.00224.2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Stefano GB, Esch T, Kream RM. Potential Immunoregulatory and antiviral/SARS-CoV-2 activities of nitric oxide. Med Sci Monit. 2020;26:e925679. doi: 10.12659/MSM.925679. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Stefano GB, Esch T, Kream RM. Behaviorally-mediated entrainment of whole-body metabolic processes: Conservation and evolutionary development of mitochondrial respiratory complexes. Med Sci Monit. 2019;25:9306–9. doi: 10.12659/MSM.920174. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Hayakawa K, Bruzzese M, Chou SH, et al. Extracellular mitochondria for therapy and diagnosis in acute central nervous system injury. JAMA Neurol. 2018;75(1):119–22. doi: 10.1001/jamaneurol.2017.3475. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Nakamura Y, Park JH, Hayakawa K. Therapeutic use of extracellular mitochondria in CNS injury and disease. Exp Neurol. 2020;324:113114. doi: 10.1016/j.expneurol.2019.113114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Esch T, Stefano GB, Ptacek R, Kream RM. Emerging roles of blood-borne intact and respiring mitochondria as bidirectional mediators of pro- and anti-inflammatory processes. Med Sci Monit. 2020;26:e924337. doi: 10.12659/MSM.924337. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Esch T, Stefano GB. Proinflammation: A common denominator or initiator of different pathophysiological disease processes. Med Sci Monit. 2002;8(5):HY1–9. [PubMed] [Google Scholar]
- 27.Esch T, Stefano GB, Fricchione GL, Benson H. The role of stress in neurodegenerative diseases and mental disorders. Neuro Endocrinol Lett. 2002;23(3):199–208. [PubMed] [Google Scholar]
- 28.Tobin MJ, Laghi F, Jubran A. Why COVID-19 silent hypoxemia is baffling to physicians. Am J Respir Crit Care Med. 2020;202(3):356–60. doi: 10.1164/rccm.202006-2157CP. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Huang L, Ma Q, Li Y, et al. Inhibition of microRNA-210 suppresses pro-inflammatory response and reduces acute brain injury of ischemic stroke in mice. Exp Neurol. 2018;300:41–50. doi: 10.1016/j.expneurol.2017.10.024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.von Arnim CAF, Bartsch T, Jacobs AH, et al. Diagnosis and treatment of cognitive impairment. Z Gerontol Geriatr. 2019;52(4):309–15. doi: 10.1007/s00391-019-01560-0. [DOI] [PubMed] [Google Scholar]