
FIGURE 2.
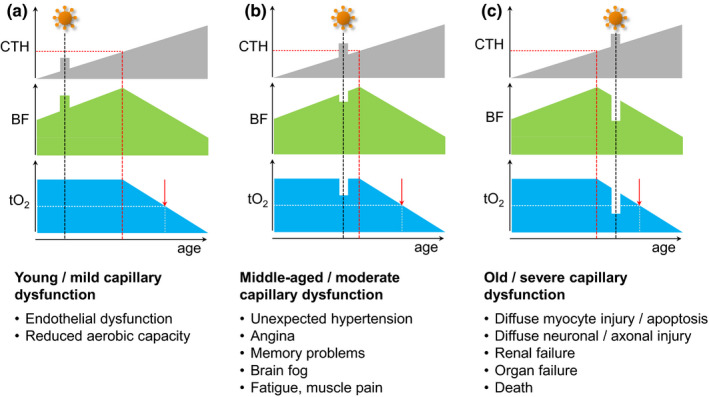
Temporary capillary flow disturbances and tissue oxygenation. This figure illustrates how temporary COVID‐19‐related flow disturbances are expected to affect flood flow (BF) and tissue oxygen tension (tO2). Panels show expected responses in tissue with mild (panel a), moderate (panel b), and severe (panel c) pre‐existing capillary dysfunction. (a) If tissue CTH remains below CTHc during COVID‐19‐related capillary flow disturbances, tO2, and thereby organ functions during rest, are likely to remain unaltered. For organs that rely on capillary transit time homogenization to meet their metabolic demands during work, such as the heart and skeletal muscle (Angleys & Østergaard, 2020), the additional capillary dysfunction is expected to reduce maximum aerobic capacity, affecting the performance of, for example, young athletes. These signs are expected to reverse upon successful therapeutic or intrinsic capillary recanalization/repair. Irreversible changes to the capillary bed's oxygen extraction capacity, however, may accelerate the emergence of symptoms and disease changes in the affected tissues, cf. Figure 1d. (b) For patients with asymptomatic, moderate preexisting capillary flow disturbances, a COVID‐19‐related CTH increase may cause them to exceed CTHc and lead to a reduction in blood flow and tissue oxygen tension. While, for example, MCI‐like symptoms are expected to disappear with disease‐related capillary flow disturbances, they may herald developing capillary dysfunction and the benefits of managing cardiovascular risk factors to prevent or delay their recurrence in later life (Hachinski et al., 2019). In COVID‐19 patients with pre‐existing myocardial capillary dysfunction, a sudden CTH increases may reduce tO2 to levels so that they experience angina during exercise in the absence of flow‐limiting coronary disease (Østergaard et al., 2014). (c) In patients with symptomatic, pre‐existing severe capillary dysfunction, further increases in CTH are expected to cause immediate drops in oxygen availability and worsen preexisting symptoms (e.g., confusion or delirium in patients who already have dementia, myocardial damage, or kidney failure). If oxygen levels fall below the metabolic requirement of critical cell functions, tissue and organ damage is expected to cause lasting symptoms or even organ failure and premature death