
Figure 2.
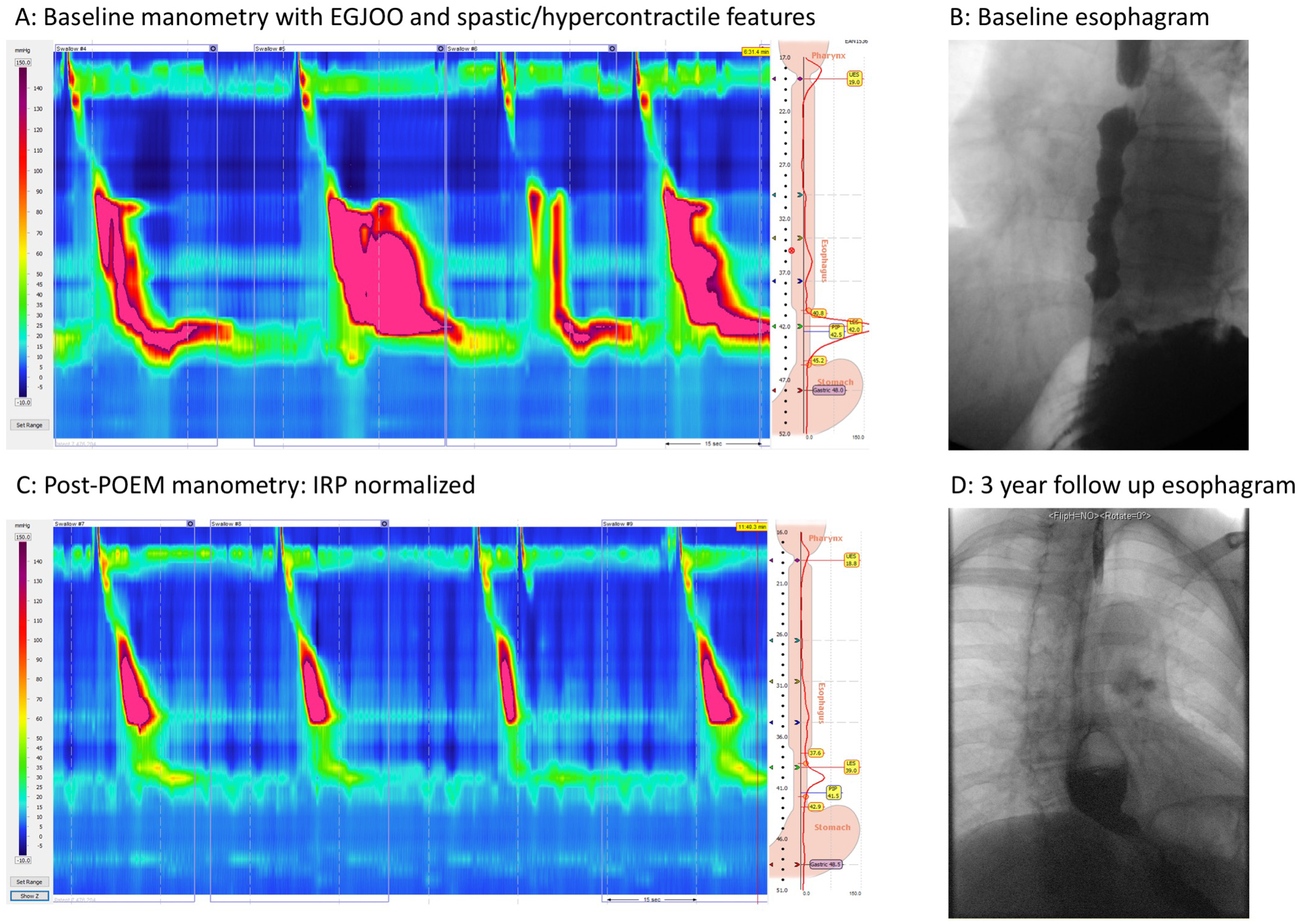
Patient presented with dysphagia and chest pain and was referred for manometry. Manometry was consistent with Type III achalasia (EGJOO and some component of jackhammer and short distal latency values) (Panel A). The esophagram was consistent with obstruction at the EGJ and there were spastic features and a normal caliber esophagus (Panel B). The patient underwent POEM with a standard 9cm myotomy and presented for follow-up evaluation with manometry which revealed normalized IRP and some residual contraction (Panel C). Approximately 3 years later she presented with new symptoms of hiccups and worsening dysphagia and chest pain and underwent an esophagram (Panel D). The esophagram revealed a large pouch along the myotomy length that failed to empty consistent with a blown out myotomy.