
Fig. 2.
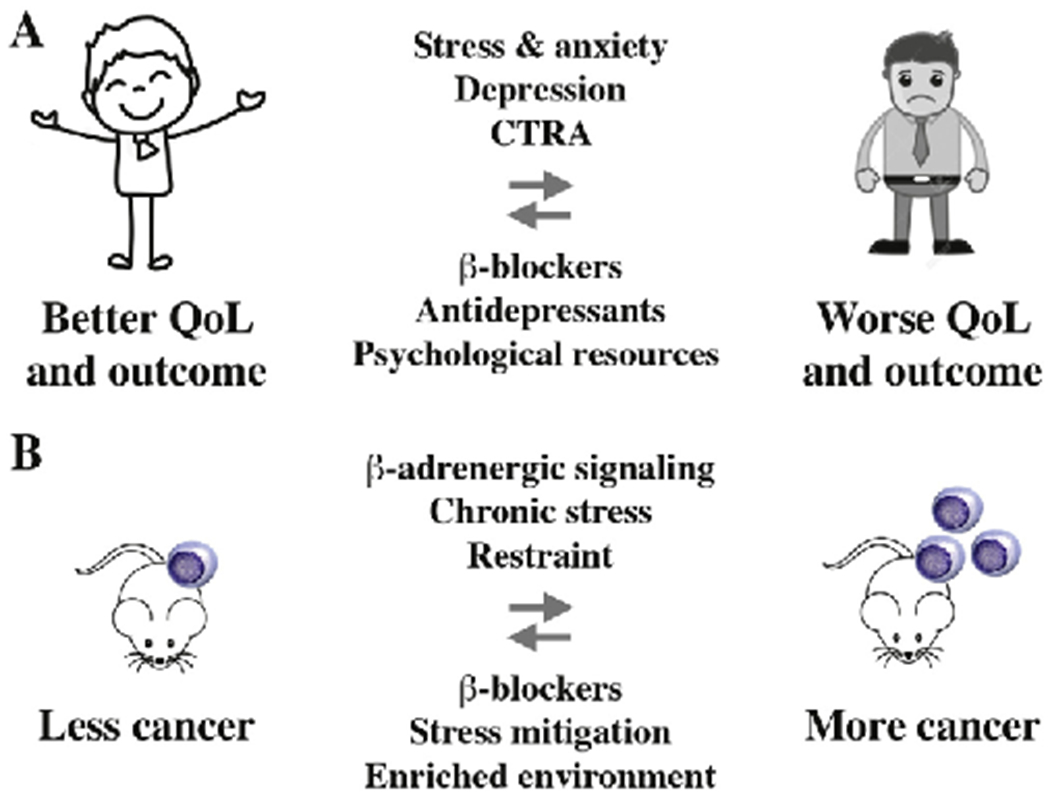
Dampening adrenergic signaling benefits patients with myeloma. Panel A shows that β-blocker intake, which dampens adrenergic signaling, reduces disease-specific mortality in patients with myeloma (arrow pointing left). Conversely, psychological distress (anxiety, depression), which leads to increased adrenergic signaling, is associated with inferior survival and reduced quality of life (QoL; arrow pointing right). Stress and anxiety relief using antidepressants and/or psychotherapy may improve outcome of myeloma by virtue of a mechanism that involves adrenergic regulation of immune cells in the BMM [85]. Dysregulation of adrenergic and other stress-related signaling pathways is evident at the transcriptomic level, as recently shown in a study on lethal prostate cancer [86] and, more broadly, in the context of a newly developed psycho-oncological framework [87] termed conserved transcriptional response to adversity (CTRA) [88]. In accordance with that, the broad-spectrum β-blocker propranolol [6] inhibited the CTRA in a recent clinical trial in myeloma [7]. Panel B depicts the principal outcome of preclinical studies using laboratory mice that linked chronic stress (elevated adrenergic signaling) and cancer (right-pointing arrow) [29,60,89–92]. In contrast, mice housed in a stress-mitigated, enriched environment or treated with anti-adrenergic β-blocker exhibited reduced rates of malignant growth, such as melanoma and colon cancer (left-pointing arrow). Tumor inhibition relied on a pathway that involved downregulation of leptin production in adipocytes in response to β-adrenergic input [93].