

Abstract
The Danger Assessment (DA) is an instrument designed to assess the likelihood of lethality or near lethality occurring in a case of intimate partner violence. This article describes the development, psychometric validation, and suggestions for use of the DA. An 11-city study of intimate partner femicide used multivariate analysis to test the predictive validity of the risk factors on the DA from intimate partner femicide cases (N = 310) compared with 324 abused women in the same cities (controls). The results were used to revise the DA (four items added; one “double-barreled” item divided into two), and the calculated weights (adjusted odds ratios) used to develop a scoring algorithm with levels of risk. These levels of risk were then tested with an independent sample of attempted femicides (N = 194) with a final outcome of .90 of the cases included in the area under the receiver operating characteristic (ROC) curve.
Keywords: lethality, risk assessment, intimate partner femicide
Over the past two decades, there has been a dramatic transformation in the response to intimate partner violence (IPV) by the general public and across the criminal justice, social service, and health care systems (Campbell, 2005; Kline, Campbell, Soler, & Ghez, 1997). The increased use of these systems and increased public scrutiny has led to a demand for valid strategies to determine which IPV cases need the most immediate attention and extensive interventions because the demand for domestic violence services far exceeds supply (Crowell & Burgess, 1996). Further, strategies need to be tailored to the level of dangerousness in the violent relationship in order to reduce further disrupting the lives of IPV survivors and their children or unnecessarily restricting the freedom of IPV offenders.
The most serious outcome of IPV is intimate partner homicide (IPH). Practitioners working in the field of IPV are concerned that a case they have worked with will end in a homicide or homicide–suicide without their taking every possible action to avert such an outcome.
The purpose of this article is to report on the further development and validation of the Danger Assessment (DA), an instrument designed to assess risk factors for IPH (see Figure 1 and http://www.dangerassessment.com) in violent intimate relationships. Specifically, data from an independent sample of women whose partners or ex-partners tried to kill them (i.e., attempted femicides) was used to support the predictive validity of the revised 20-item version of the DA with its weighted scoring.
Figure 1.
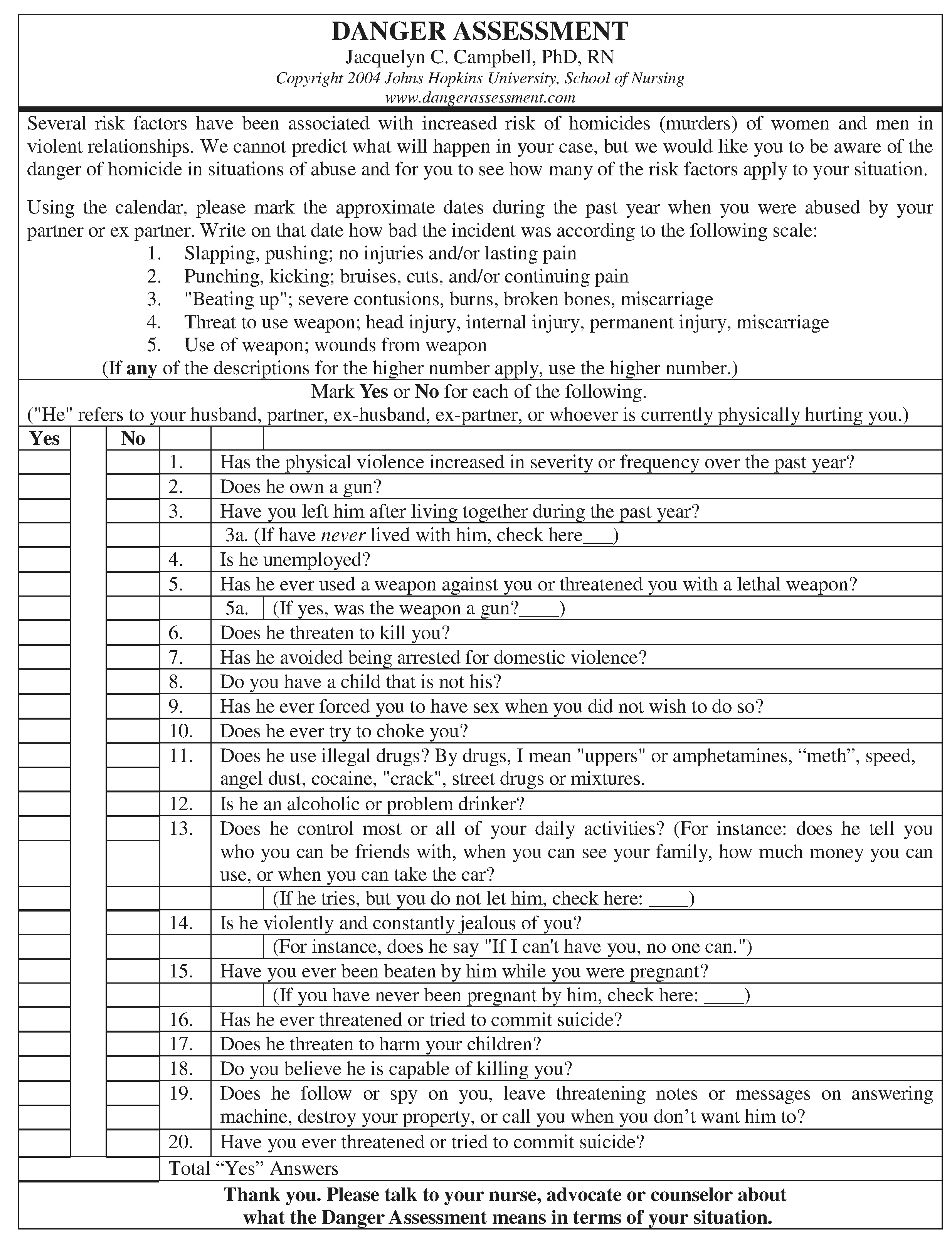
Revised 20-Item Danger Assessment
Prior to presenting the data that supports the predictive validity of the DA, we will review the research on intimate partner (i.e., current or former spouse, boyfriend–girlfriend, or same-sex partner) homicide and describe the state of the science in risk assessment in the field of IPV. We will also explain the development and support for validity of the original 15-item DA and then briefly describe the 11-city study of risk factors for intimate partner femicide that resulted in revisions of the DA to a 20-item instrument with weighted scoring.
Review of Research on Intimate Partner Homicide
The United States has the highest rate of IPH of any industrialized country (Krug, Dahlberg, Mercy, Zwi, & Lozano, 2002). In the United States, approximately 1,200 women have been killed by their current or former intimate partner during each year of the 21st century, with approximately 300 males killed by their intimate partners during those same years (Fox & Zawitz, 2004). These data are from the Federal Bureau of Investigation’s (FBI) Supplemental Homicide Report (SHR) and do not include an offender category for ex-boyfriend or ex-girlfriend. This is an important omission in the SHR, given that Langford, Isaac, and Kabat (1998) and Chilton and Weber (1999) both found the SHR miscategorized as many as 13% of the partner homicides in state data (Massachusetts and Florida, respectively) primarily because of the omission of ex-boyfriend/ex-girlfriend perpetrators. In another more recent study, 19% of the intimate partner femicides (i.e., murder of women) were committed by former boyfriends (Campbell et al., 2003a,b). Thus, if we included ex-boyfriends as perpetrators in the annual number of femicides perpetrated by a current or former intimate partner, there were approximately 1,400 to 1,750 intimate partner femicides annually during the period from 2000 to 2004. Intimate partner homicide has decreased over the past 30 years in the United States; however, the rate of decline of homicides in which the husbands and ex-husbands are victims is nearly twice that for wives and ex-wives (Fox & Zawitz, 2004; Puzone, Saltzman, Kresnow, Thompson, & Mercy, 2000).
Risk Factors for IPH
Across studies of risk factors for IPH, prior IPV is clearly the most common risk factor (67%-80% of IPH cases), whether the woman or the male partner is killed (Browne, Williams, & Dutton, 1998; Moracco, Runyan, & Butts, 1998; Saunders & Browne, 2000; Bailey et al., 1997). Other demographic and relationship risk factors identified include age difference between partners, with the abuser being older (Breitman, Shackelford, & Block, 2004), younger age (15–44 years) of women (Shackelford & Mouzos, 2005), cohabitation versus formal marriage (Moracco et al.), estrangement (Moracco et al.; Wilson & Daly, 1993), and a child in the home who is not the biological child of the abuser (Daly, Wiseman, & Wilson, 1997). In a study of risk factors for women being murdered in their homes, the vast majority of the time by a current or former intimate partner, Bailey et al. found that mental illness, illicit drug use, prior criminal involvement, and the presence of firearms in the home were each independently associated with increased risk of homicide to female household members. These risk factors are salient whether or not there is clear intent of murder, which is often difficult to ascertain (Block & Christakos, 1995; Campbell, 1992).
State of the Science in IPV Risk Assessment
In spite of increasing demand for risk assessment in the field of IPV, the science is relatively young. For example, a recent meta-analysis of prediction of sexual assault re-offending was based on 95 sufficiently rigorous prospective studies (Hanson & Morton-Bourgon, 2004). In comparison, the field of IPV research has only nine comparable investigations, and not all have been published.
Most of the validated IPV risk assessment instruments (e.g., Domestic Violence Screening Inventory [DVSI; Williams & Houghton, 2004], the Kingston Screening Instrument for Domestic Violence [K-SID; Gelles, 1998; Lyon, 1998], Ontario Domestic Abuse Risk Assessment [O.D.A.R.A.; Hilton et al., 2005], and the Partner Abuse Scale [PAS; Dutton, Landolt, Starzomski, & Bodnarchuk, 2001]) are primarily aimed at predicting reassault of IPV rather than IPH. Intimate partner violence reassault is easier to predict accurately because IPV reassault has a higher occurrence (approximately 25% to 30% of IPV cases) than does IPH (approximately 0.04% of IPV cases). Further, the IPV reassault paradigm is analogous to well-established risk-assessment enterprises, such as predicting reassault in sexual assault and violence among the mentally ill. One risk assessment instrument, the Spousal Assault Risk Assessment (SARA; Kropp, Hart, Webster, & Eaves, 2000), is aimed at predicting both lethal violence and reassault outcomes; however, it has only been evaluated on the basis of IPV reassault outcomes (Kropp et al., 2000). Although the factors on risk assessments for IPV reassault and IPH overlap, they are not exactly the same (Campbell, 2004). Only a few instruments have been developed that focus on the assessment of dangerousness related to lethal, near lethal, or potentially lethal outcomes, primarily the threat assessment system, Method of Assessment of Domestic Violence Situations or Domestic Violence Method (DV-MOSAIC, see http://www.mosaicsystem.com/dv.htm; DeBecker, 1997) and the Danger Assessment (DA; Campbell, 2004). Existing risk models and risk assessment instruments have been developed and tested with heterosexual samples and then applied to women in same-sex relationships. Recently, Glass and colleagues (in press) have revised the existing validated DA, to a 18-item Danger Assessment- Revised (DA-R) to assess for reassault in abusive female same-sex intimate relationships. Result from the testing of the DA-R can be found in Glass and colleagues.
In addition to formalized instruments or systems, it has been established that abused women are fairly good assessors of their own risk of reassault (Campbell, O’Sullivan, Roehl, & Webster, 2005; Goodman, Dutton, & Bennett, 2000; Heckert & Gondolf, 2004; Weisz, Tolman, & Saunders, 2000). The recently completed National Institute of Justice (NIJ)–funded Risk Assessment Validation Experiment (the RAVE study) study of 782 abused women found that women’s perceived risk of severe reassault achieved a .62 predictive accuracy with receiver operating characteristic (ROC) curve analysis, approximately the same as the K-SID (.62) and the DVSI (.62), but less than the DA (.69; Campbell et al., 2005) and DV-MOSAIC (.65; DeBecker, 1997). The next section will present the development of and validation of the DA.
Development of the Original 15-Item Danger Assessment Instrument
In contrast to the instruments designed to address risk of IPV reassault, the DA (Figure 1) is a clinical and research instrument that was designed to assist battered women in assessing their danger of being murdered (or seriously injured) by their intimate partner or ex–intimate partner. The DA was originally developed with consultation and content validity support from battered women, shelter workers, law enforcement officials, and other clinical experts on battering (Campbell, 1986, 2005). The initial 15-items on the DA were developed from the authors’ and others’ retrospective research studies of IPH or serious injury from IPV (Browne, 1987; Berk, Berk, Loseke, & Rauma, 1983; Campbell, 1981; Fagan, Stewart, & Hansen, 1983) and from input from abused women in shelters (Stuart & Campbell, 1989). It was originally designed to assess risk of women killing their abusive male partner as well as being murdered by their male intimate partner.
The first portion of the DA assesses severity and frequency of battering by presenting the woman with a calendar of the past year. The woman is asked to mark the approximate days during the past year when physically abusive incidents occurred and to rank the severity of the incident on a 1-to-5 scale (1 = slap, pushing, no injuries, and/or lasting pain through 5 = use of weapon, wounds from weapon). The calendar portion was conceptualized as a way to raise the consciousness of the woman and reduce the normal minimization of IPV, especially given that using a calendar increases accurate recall in other situations (Campbell, 1995; Ferraro & Johnson, 1983). In the original DA development, 38% of women who initially reported no increase in severity and frequency of physical violence in the past year changed their response to yes, an increase in severity and frequency of physical violence in the past year, after filling out the calendar portion of the DA (Campbell, 1986, 1995).
The second part of the original DA is a 15-item yes/no dichotomous response format of risk factors associated with IPH (Campbell, 1995). Both portions (calendar and 15 items) of the DA take approximately 20 min to complete. The woman can complete the DA by herself or with professionals from the health care, criminal justice, or victim advocate systems assisting in the interpretation of the DA within the context of her situation. The original DA can be scored by counting the yes responses with no classification or cutoff score, with a higher number of yes indicating that more of the risk factors for IPH are present in the relationship. The original 15-item DA has published data on construct validity (Campbell, 1995); however, all studies using the DA thus far (except for the original study, Campbell, 1981, 1992), address issues of risk with women as victims and men as perpetrators.
The initial studies using the original 15-item DA are described in detail elsewhere (Campbell, 1986, 1995, 2007). These studies have examined reliability and validity of the DA, with internal consistency acceptable (.70-.80; Campbell, 1995) and in the two studies in which test–retest reliability was assessed, it ranged from .89 to .94 (Campbell, 1995; Stuart & Campbell, 1989). Discriminant group validity was supported by significant differences in DA mean scores among contrasting groups of women. The lowest mean score was found in the nonabused sample with the highest score among the sample of women in the emergency department (Campbell, 1995). Convergent construct validity has been supported in the majority of the studies with moderate to strong correlations between the DA and validated instruments measuring severity and frequency of IPV, including the Index of Spouse Abuse, the Conflict Tactics Scale, and injury from abuse (Campbell, 1995).
As well as the cross-sectional study support for the original 15-item DA and its ability to assess risk of lethal violence described above, there have been three independent predictive validity studies published that at least partially support the DA’s ability to predict IPV reassault (Goodman et al., 2000; Heckert & Gondolf, 2004; Weisz et al., 2000).
The next major step in the development of and validation of the DA is reported in next section and is based on data from the 11-city intimate partner femicide study (Campbell et al., 2003b). The details of the methodology of the study are reported elsewhere (Campbell et al., 2003b), but these are reviewed briefly in the following section.
Risk Factors for Intimate Partner Femicide Study
Study Overview
The primary purpose of the 11-city case-control study was to identify risk factors for intimate partner femicide and inform the assessment and possible revision of the DA (Campbell et al., 2003b). Risk-factor data were collected using a structured survey administered by researchers and interviewers trained in interviewing victims of violence. Each collaborating site obtained institutional review board approval.
Selection of Participants
Femicide cases.
All consecutive police or medical examiner intimate partner female homicide records from 1994 to 2000 in each study city were examined for victim–perpetrator relationship. Cases were eligible if the victim was a woman aged 18 or older, the perpetrator was a current or ex-intimate partner, and the case was designated as closed by the police. Records were abstracted for data specific to the homicide and to identify potential proxy informants (i.e., mother, sister, brother, or friend) who might be knowledgeable about details concerning the victim’s relationship with the perpetrator. Proxies were then sent a letter explaining the study and inviting their participation (Block, McFarlane, Walker, & Devitt, 1999). Researcher phone and address contact information was provided in the letter for proxies to find out more about the study or to request no further communication (Block et al., 1999). Two weeks following the letter, study personnel made contact, either by telephone or in person (in the few cases where no phone contact was possible), with the proxies unless they had requested noncontact. If the first proxy reported that they were not knowledgeable about details of the relationship, she or he was asked to identify another more informed potential proxy informant who was then contacted. In-person or telephone interviews were conducted, following informed consent, with the proxy who was most knowledgeable about details of the victim–perpetrator relationship. In 373 of the 545 (68%) total intimate partner femicide cases abstracted, a knowledgeable proxy was identified and located. Proxies agreed to participate in 83% (310/373) of cases; therefore, 310 femicides are included in this analysis.
Attempted femicide cases.
A secondary objective of the 11-city study was to determine whether the risk factors for attempted femicide—situations in which we had an opportunity to collect risk factor information directly from victims—were similar to those identified for femicides through proxy interviews. Attempted femicides were identified through the offices of the district attorney, law enforcement, community domestic violence advocacy, or trauma centers in each participating city. Attempted femicide was defined as a nonfatal gunshot or stab wound to the head, neck, or torso, strangulation or near drowning with loss of consciousness, severe injuries inflicted that easily could have led to death, or gunshot or stab wound to other body part with evidence of unambiguous (additional to victim report) intent to kill on the part of a perpetrator who was a current or former intimate partner. When a woman was identified, she was sent an introductory letter inviting her to participate in a “Woman’s Health and Relationships Study” and a statement that she would receive a follow-up phone call in 2 weeks unless she contacted the investigators requesting not to be called. The follow-up phone call established safety and privacy, further explained the study, established informed consent, and either proceeded with the telephone interview or scheduled a safe and convenient time to conduct the telephone or in-person interview. The attempted femicide cases gave the advantage of direct interviews with victims rather than their proxies, but the disadvantage of a lower location rate (56%), because a large proportion of the women had moved from the place where they were almost killed as would be expected. However, once located, almost all (90%) the attempted femicide victims (n = 215) contacted agreed to participate for a sample of 194.
Abused controls.
Stratified random-digit dialing (up to six attempts per number) conducted by an experienced survey research firm was used to select English and Spanish speaking women aged 18 to 50 years who had been involved romantically or sexually in a relationship at some time in the past 2 years in the same cities in which the homicides occurred. A woman was considered abused if she had been physically assaulted or threatened with a weapon by a current or former intimate partner during the past 2 years; we identified episodes of abuse using a modified version of the Conflict Tactics Scale with stalking items added (Campbell, 1992; Straus & Gelles, 1990). A total of 4,746 women met the age and relationship criteria and were read the consent statement. Among these women, 3,637 (76.6%) agreed to participate. A total of 427 (8.5%) of these women had been physically abused or threatened with a weapon by a current or recent intimate partner and are included in this analysis. Thirteen abused controls were excluded because they reported that the injuries from their most severe incident of abuse were so severe that they thought they could have died. Safety protocols originally developed by Johnson and Sacco (1995) for the Canadian national domestic violence study were adapted and followed for the study.
Methods of Measurement
The interview included the DA (Campbell, 1986, 1995; Campbell, Sharps, & Glass, 2001), along with demographic and relationship characteristics, including type, frequency, and severity of any violence, psychological abuse and harassment, alcohol and drug use, and weapon availability. The proxies for the femicide cases and victims of attempted femicide were asked to report on risk factors for IPH in the year prior to the femicide or attempted femicide incident. The abused controls were asked to report on physical or sexual violence or threat of physical or sexual violence in the past 2 years and the worst incident of abuse. The interview was administered in either English or Spanish (following translation and back-translation procedures). The study measure has been described in detail in previous publications (Campbell et al., 2003b; Thompson, Basile, Hertz, & Sitterle, 2006).
Revision of the Original DA
The DA was revised based on the findings from the 11-city study as previously reported (see Campbell et al., 2003a). These revisions to the original 15-item DA included the addition of four items: abuser unemployment, the victim having a child in the home who is not the offspring of the abusive partner, stalking behavior by the abuser, and the victim leaving her abuser after the couple lived together. The item formerly worded “Is he violent toward your children?” was reworded to read “Does he threaten to harm your children?” to reflect the new item’s greater strength as a risk factor and to avoid an automatic report to Child Protective Services when there is an affirmative reply. One “double-barreled” item (i.e., “threaten to kill you and perceive him as capable of killing you”) was divided into two separate items, and the item on abuser violence outside of the home was removed because its lack of predictive salience. An item on prior arrest of the abusive partner for IPV was substituted for the abuser “being violent outside of the home” because it was significantly predictive in the multivariate analysis (Campbell et al., 2003b). With these revisions, there is now a total of 20 items on the DA.
Development of Weighted Scoring for the Revised 20-Item DA
The adjusted odds ratios from the multivariate analyses of the femicide cases in comparison to the controls (abused women) from the 11-city study (Campbell et al., 2003b) were used to develop a weighted scoring algorithm that identifies four levels of danger. The levels of danger are defined based on the DA score as: (a) variable danger (score of 0–7); (b) increased danger (score of 9–13); (c) severe danger (score of 14–17); and (d) extreme danger (18 and above). The language used to define the levels of danger were chosen to have meaning for abused women based on consultation with survivors and advocates and to convey that even at the lowest level (variable danger), the risk of lethal violence is never negligible and can change quickly.
Analysis
To determine the predictive validity of the revised 20-item version of the DA with its weighted scoring, the investigators used data reported from the attempted femicide cases and abused controls on the revised 20-item DA. The ability of the revised DA to correctly identify the attempted femicide cases, an independent sample, was evaluated through plots of ROC curves. Receiver operating characteristic curves represent the sensitivity and 1-specificity of a measure at each successive unit that could be a potential threshold for high-risk designation. We developed estimates of the area under the ROC curve (AUC), and tested whether the AUC was greater than the chance diagonal (.500), the average value under random prediction methods. In addition, we calculated sensitivity and specificity using each of the top three levels of danger (increased danger, severe danger, and extreme danger) as a threshold for being designated high risk for attempted femicide. In addition, we also compared the mean scores on the revised 20-item DA between the three study groups (e.g., femicide, attempted femicide, and abused controls) using analysis of variance (ANOVA) and Tamhane’s T2 statistic for testing whether pairwise comparisons of group means were equal when the variance differs between the groups.
Positive predictive value (PPV) is defined as the proportion of individuals that screened positive or were designated as high risk that had or developed the outcome of interest. Negative predictive power (NPP) is the proportion of individuals that were not identified as high risk that did not have or develop the outcome. We were unable to assess PPV or NPV because the case control study design did not allow us to identify the number of female IPV victims in the cities involved in the study that could have been screened.
Community samples of IPV victims include many who experience infrequent abuse of relatively low severity, and are therefore unlikely to be identified as IPV victims by criminal justice, social service, or health care agencies. Analyses that include many of these cases could overstate how well the revised DA would perform in practice in distinguishing those at greatest risk for lethal violence from all other cases of IPV. Therefore, we performed the same analyses described above for the IPV victims (abused controls and attempted femicides) who were most likely to have been identified as a victim of IPV and therefore been screened for high danger—those who reported having previously received medical treatment for injuries due to IPV, had obtained a civil protective order from a court, reported her partner to the police for assaulting her, or for whom the abusive partner had been arrested for domestic violence.
Results
Table 1 provides information on the social and demographic characteristics of the two groups of cases (femicides and attempted femicides) and the abused controls. Victims and perpetrators of femicides and attempted femicide were similar in their social and demographic characteristics with the exception of perpetrators of attempted femicides being somewhat more likely to be African American than perpetrators of femicide (64.1% vs. 48.9%) and victims of attempted femicide being more likely to have had a child with their abusive partner (44.2% vs. 33.2%). These femicide and attempted femicide cases differed from abused control cases with respect to race (abused controls and abusers more likely to be White), educational attainment (abused controls having more formal education), employment (abused controls and their abusers less likely to be unemployed), relationship status (abused controls abusers more likely to be ex-boyfriends), cohabitation (abused controls less likely to have lived with their abuser), and whether the victim had a child by someone other than the abuser (abused controls less likely).
Table 1.
Demographic Characteristics of Victims and Perpetrators of Femicides, Attempted Femicides, and Abused Controls at Time of Worst Incident of Abuse
| Femicides n (%) | Attempted Femicides n (%) | Abused Controls n (%) | p value | |
|---|---|---|---|---|
| Victim characteristics | ||||
| Race/ethnicity | < .001 | |||
| White | 53 (24.1) | 33 (21.6) | 157 (46.3) | |
| Black/African American | 104 (47.3) | 87 (56.9) | 70 (20.6) | |
| Latina/Hispanic | 53 (24.1) | 26 (17.0) | 82 (24.2) | |
| Other race/ethnicity | 10 (4.5) | 7 (4.6) | 30 (8.8) | |
| Refused | 0 | 3 | 4 | |
| Educational attainment | < .001 | |||
| Did not graduate high school | 71 (33.2) | 50 (32.3) | 61 (17.9) | |
| High school graduate | 59 (27.6) | 38 (24.5) | 73 (21.5) | |
| Some college | 68 (31.8) | 52 (33.5) | 109 (32.1) | |
| College graduate | 16 (7.5) | 15 (9.7) | 97 (28.5) | |
| Unknown/refused | 6 | 1 | 3 | |
| Employment status | < .001 | |||
| Employed full-time | 114 (51.8) | 66 (42.9) | 179 (52.2) | |
| Employed part-time | 31 (14.1) | 14 (9.1) | 70 (20.4) | |
| Unemployed, looking | 12 (5.5) | 21 (13.6) | 40 (11.7) | |
| Unemployed, not looking | 63 (28.6) | 53 (34.4) | 54 (15.7) | |
| Unknown/refused | 0 | 2 | 0 | |
| Offender relationship to victim | 1 | |||
| Spouse/common-law | 85 (39.9) | 51 (32.7) | 101 (29.7) | |
| Boyfriend | 65 (29.8) | 61 (39.1) | 86 (25.3) | |
| Ex-spouse | 20 (9.2) | 12 (7.7) | 36 (10.6) | |
| Ex-boyfriend | 48 (22.0) | 32 (20.5) | 117 (34.4) | |
| Unknown/refused | 2 | 0 | 3 | |
| Cohabitation with abuser | < .001 | |||
| Lived together | 81 (45.0) | 74 (48.1) | 174 (50.9) | |
| Separated after living together | 79 (43.9) | 70 (45.5) | 50 (14.6) | |
| Victim never lived with abuser | 20 (11.1) | 10 (6.5) | 118 (34.5) | |
| Don’t know/refused | 40 | 2 | 1 | |
| Victim and abuser had a child together | 0.003 | |||
| Yes | 73 (33.2) | 69 (44.2) | 98 (28.6) | |
| No | 142 (66.8) | 87 (55.8) | 245 (71.4) | |
| Abuser characteristics | ||||
| Race/ethnicity | < .001 | |||
| White | 49 (22.4) | 21 (13.5) | 153 (44.7) | |
| Black/African American | 107 (48.9) | 100 (64.1) | 83 (24.3) | |
| Latina/Hispanic | 58 (26.5) | 25 (16.0) | 80 (23.4) | |
| Other race/ethnicity | 5 (2.3) | 10 (6.4) | 26 (7.6) | |
| Refused | 1 | 0 | 1 | |
| Educational attainment | < .001 | |||
| Did not graduate high school | 70 (49.0) | 69 (48.6) | 92 (28.0) | |
| High school graduate | 47 (32.9) | 49 (34.5) | 91 (27.7) | |
| Some college | 17 (11.9) | 17 (12.0) | 58 (17.7) | |
| College graduate | 9 (6.3) | 7 (4.9) | 87 (26.5) | |
| Unknown/refused | 77 | 14 | 0 | |
| Employment status | < .001 | |||
| Employed full-time | 84 (39.6) | 68 (45.9) | 229 (68.2) | |
| Employed part-time | 20 (9.4) | 16 (10.8) | 39 (11.6) | |
| Unemployed, looking | 13 (6.1) | 17 (11.5) | 25 (7.4) | |
| Unemployed, not looking | 95 (44.8) | 47 (31.8) | 43 (12.8) | |
| Unknown/refused | 8 | 8 | 7 | |
These differences were reflected by items on the DA with the other demographic factors subsumed under the unemployment item as demonstrated in the multivariate analysis of the original femicide study (Campbell et al., 2003b).
Femicides and attempted femicides had similar mean and median scores on the revised DA, which were more than twice as high as that of the abused control group (Table 2; Tamhane’s T2 significant at p < .001 for each comparison of the femicides and attempted femicides with the abused controls).
Table 2.
Comparison of Attempted Femicides and Nonlethal Intimate Partner Violence Comparisons on Danger Assessment Scores
| M (SD) | Median | Area Under ROC Curve (AUC) | 95% Confidence Interval for AUC | |
|---|---|---|---|---|
| Attempted femicides | 18.7*** (6.1) | 18.0 | 0.916 | .892–.941 |
| Abused controls | 7.7 (5.0) | 7.0 | ||
Note: ROC = receiver operating characteristic.
t = 21.1, df = 2, p < .001.
p < .001 for test of null hypothesis that the Danger Assessment score does not distinguish between attempted femicides and the nonlethal partner violence comparisons.
The AUC for the ROC curve comparing attempted femicides to the abused controls was .916 (p < .001; 95% Confidence Interval [CI] .892 to .941). Attempted femicides were much more likely to fall into the higher danger categories on the revised DA than were the abused controls (Table 3). For example, 1.3% of attempted femicides were in the increased danger level based on their situation prior to the worst incident of abuse, whereas 53.1% of the abused controls were in this level of danger. Conversely, 54.5% of attempted femicides were in the extreme danger category versus 3.5% of the abused controls.
Table 3.
Danger Assessment (DA) Category by Intimate Partner Violence Lethality Category and Sensitivity and Specificity if High-Risk Status Is Conferred at the DA Category
| Danger Category (DA Scores) | Abused Controls n (%) Specificity | Attempted Femicides n (%) Sensitivity |
|---|---|---|
| Variable (< 8) | 182 (53.1) | 2 (1.3) |
| Increased (8–13) | 114 (33.2) .531 | 31 (19.9) .987 |
| Severe (14–17) | 35 (10.2) .863 | 38 (24.4) .788 |
| Extreme (18+) | 12 (3.5) .965 | 85 (54.5) .545 |
| Total | 343 | 156 |
Sensitivity of the revised DA for identifying attempted femicides ranged from .545 for the extreme danger level to .987 if increased danger is used to designate high-risk status. The sum of sensitivity and specificity is maximized if the severe danger level is the threshold for high-risk designation (sensitivity = .750 and specificity = .863). As a point of comparison, victims’ responses to the question “Do you think he (abuser) was capable of killing you?” (question asked after the most severe incident of abuse) produced a sensitivity of .622 and a specificity of .770.
When the analyses were restricted to victims who had contact with a health care provider, law enforcement agency, or domestic violence service agency as a result of prior partner violence (92 abused controls and 104 attempted femicides), differences in the mean DA score between the abused controls (M = 9.9, standard deviation [SD] = 5.3) and attempted femicides (M = 18.6, SD = 7.5) remained statistically significant (p < .001). The AUC for the ROC curves indicated that the DA scores discriminated between the abused controls and attempted femicides (AUC = .862, 95% CI .812 to .913; p < .001).
As Table 4 reveals, the somewhat reduced discriminatory power of the revised DA among the subset of cases and controls that have the greatest likelihood of being screened for danger is primarily due to lower specificity than was obtained with the whole sample. Specificity within the subset most likely to be screened ranged from .370 if the increased danger level is used to designate high-risk status to .913 if the extreme danger level is the benchmark for high-risk. Sensitivity of the revised DA danger levels among the subset most likely to be screened was similar to that obtained on the whole sample, topping out at .981 for attempted femicides at the increased danger level (Table 4).
Table 4.
Danger Assessment (DA) Category by Intimate Partner Violence Lethality Category and Sensitivity and Specificity if High-risk Status Is Conferred at the DA Category for a Subset Who Had Previously Interfaced With a Criminal Justice, Health Care, or Victims’ Service Agency as a Result of Intimate Partner Violence
| Danger Category (DA Scores) | Abused Controls n (%) Specificity | Attempted Femicides n (%) Sensitivity |
|---|---|---|
| Variable (< 8) | 34 (37.0) | 2 (1.9) |
| Increased (8–13) | 36 (39.1) .370 | 17 (16.3) .981 |
| Severe (14–17) | 14 (15.2) .761 | 31 (29.8) .817 |
| Extreme (18+) | 8 (8.7) .913 | 54 (51.9) .519 |
| Total | 92 | 104 |
Discussion
The data from the completed 11-city risk factors for intimate partner femicide study allowed us to revise the original DA by adding four items that were predictive of IPH and rewording items for clarity as well as develop a weighted scoring for the DA, all appropriate steps in the further development of the instrument. The revised DA was then tested to determine how well it predicted attempted femicides committed by current or former intimate partners. The attempted femicides were an independent sample, giving important validation for the revised DA. Sensitivity and specificity were acceptable with higher values for the revised DA than victim perception of risk of lethal or near lethal violence. The AUC for the ROC curve analysis was strongly supportive of the predictive accuracy of the revised DA, far better than the .70 considered acceptable in risk assessment instruments (Hilton et al., 2005).
The results support using the ranges of danger levels developed. For example, domestic violence prevention and intervention advocates might choose the increased danger levels as a cut-off for shelter admission (assuming insufficient beds for all seeking shelter) to maximize sensitivity. The findings suggest that they are likely to capture more than 90% of potentially lethal IPV cases by using the increased level of danger. For criminal justice practitioners (such as judges, probation officers), using the extreme danger level should result in fewer than 5% false negatives.
This study had some important limitations. The retrospective design of the study introduces bias in the items that go into the DA. For example, victims of attempted femicide may be more inclined to report a risk factor (e.g., sexual abuse, prior threat to kill) after the experience of the attempted femicide event. However imperfect a retrospective design, events such as femicide or attempted femicide by a current or former partner are too rare to make prospective study designs practical. The revised DA was recently evaluated in a prospective study of 782 abused women and found to be predictive of the likelihood of severe re-assaults (Campbell et al., 2005).
The data used to validate the revised DA were only partially independent of the data used to generate the scoring weights for the measure. We did use an independent sample of attempted femicides; however, the scoring weights were determined, in part, by the conditions of the abused controls used in the 11-city study. In addition, our findings are based on an urban sample and we do not know how well the findings would hold in a sample of rural femicides, attempted femicides, and abused women.
Although we demonstrated that the revised DA, particularly when using the severe danger category threshold for determining high-risk status, had relatively high sensitivity and specificity, the study design did not allow us to examine other important indicators of the predictive utility of screening devices. For example, PPV can be considered an indicator of the efficiency of a screening method and measures the proportion of those who screen as high risk who later experience the condition for which you are screening. To calculate a PPV for a screening method, one must first know which individuals would be screened (e.g., IPV victims who come into contact with health care professionals or social service agencies) during some baseline period and follow that group for some standard period of time. Our case-control study design, made necessary because homicides and attempted homicides perpetrated by current or former intimate partners are relatively rare events, did not provide the conditions necessary to calculate a meaningful PPV. Although the highest categories of danger on the DA produce acceptable levels of specificity, when screening for risk of relatively rare outcomes, incredibly high accuracy is required to avoid identifying many false positives for every true positive and thus a low PPV. Nevertheless, a study of recidivism for nonlethal reassault by current or former partners has shown that baseline DA scores and danger categories are highly associated with reassaults (Campbell et al., 2005). Practitioners will have to decide how to weigh the advantages of being able to identify most of the individuals at risk of being killed, nearly killed, or nonfatally reassaulted against the consequences of falsely identifying some victims and perpetrators as being at high risk for lethal and near lethal IPV.
Finally, although women’s assessment is valuable in predicting reassault and is queried in the DA in the item “Do you believe he is capable of killing you?” only about one half of the actual (45%) and near lethal violence (54%) victims accurately determined their risk of lethal violence in an abusive intimate relationship in the femicide data. Although significantly more of the killed or almost killed women affirmed this item, compared with abused controls, the multivariate analysis did not show this item to be as important as several others. Therefore, although important to take into account, women’s assessment of risk should not be the only risk factor assessed for risk of intimate partner femicide.
Conclusion
The revised 20-item DA can accurately identify the vast majority of abused women who are at increased risk of femicide or attempted femicide as well as distinguish most of the IPV cases that are at lowest risk of femicide or attempted femicide, at least in this urban sample of women. However, further development and testing of the DA is needed, as with all of the IPV risk assessment strategies. Independent evaluations are needed as well as meta-analyses when there are sufficient prospective studies to conduct such investigations. The DA and other risk assessment systems need to also be psychometrically evaluated with various ethnic groups, as well as rural and immigrant populations to be sure they are culturally and linguistically appropriate. The science in the field is as yet young, but this study lends substantive support for use of the DA with IPV victims as they make important decisions about their safety.
The DA is meant to be a collaborative exercise between a domestic violence advocate, health care professional, and/or criminal justice practitioner and the abused woman herself (Campbell, 2005). Only about half (45%) of proxy informants for actual victims and slightly more than half (54%) of victims of near lethal violence accurately determined their risk of lethal violence in an abusive intimate relationship. Women’s perception of risk is important in developing safety plans and interventions; however, even though their perception of risk of re-assault can be accurate (Goodman et al., 2000; Heckert & Gondolf, 2004; Weisz et al., 2000), abused women often underestimate the potential for homicide. Only about one half of the femicide victims in our study accurately assessed that they were likely to be killed (Campbell et al., 2003b). The revised DA outperformed victim’s perception of risk of reassault in the RAVE study (Campbell et al., 2005) and the Gondolf investigation (Heckert & Gondolf, 2004). Further, the DA can provide powerful information for abused woman and the practitioner as they navigate the criminal justice, advocacy, social welfare, substance abuse, batterer intervention, and/or health care systems seeking safety. As pointed out by Dutton and Kropp (2000), the use of the DA or any risk assessment method should be only the first step in a process of safety planning or “risk management.” Use of the DA can be helpful in substantiating the victim’s and/or the clinician’s perception of risk for use in systems such as criminal justice and advocacy services. The DA can also be used as an adjunct to batterer intervention programs, as part of an approach that reaches out to the partners of abusive men enrolled in batterers’ programs as tested by Gondolf (2000), given that few abused women seek assistance through community-based domestic violence services (Sharps et al., 2001).
Protocols addressing issues such as of confidentiality and communication of results and training for assessors for the use of the DA as with any IPV risk assessment process need to be developed in each system where it is used (Campbell, 2005). Abused women’s perception of risk of IPH or IPV reassaults by her partner or ex-partner should always be ascertained and taken into account in any safety-planning endeavor. The DA can help her come to a more realistic appraisal of her risk as well as improve the predictive accuracy of those who are trying to help her.
Acknowledgments
Authors’ Note: Funding from NIH (NIDA, NIMH, NIA) /CDC/NIJ (R01 DA/AA11156, J. Campbell, PI); Risk factors for Homicide in Violent Intimate Relationships and NIJ (2000WTVX0011, J. Campbell, PI); Evaluation of domestic violence risk assessment instruments.
Biography
Jacquelyn C. Campbell is the Anna D. Wolf Chair and a Professor in the Johns Hopkins University School of Nursing with a joint appointment in the Bloomberg School of Public Health. She has been conducting advocacy policy work and research in the area of family violence and addressing health disparities related to trauma since 1980. Dr. Campbell has been continuously funded as Principal Investigator (PI) since 1984 on National Institutes of Health (NIH) or other governmental research awards, including 10 major NIH, National Institute of Justice (NIJ), or Centers for Disease Control (CDC) research grants and has published more than 150 articles and 7 books on violence against women. She is an elected member of the Institute of Medicine and the American Academy of Nursing, and served on the congressionally appointed U.S. Department of Defense Domestic Violence Task Force as well as the Board of Directors of the Baltimore House of Ruth Battered Women’s Shelter. Currently, Dr. Campbell is the National Program Director for the new Robert Wood Johnson Foundation Nurse Faculty Scholars program, and is PI of a National Institute for Occupational Safety and Health (NIOSH)–funded project on workplace violence.
Daniel W. Webster is Associate Professor of Health Policy and Management at the Johns Hopkins Bloomberg School of Public Health where he serves as Co-Director of the Center for Gun Policy and Research and as Associate Director of Research for the Center for the Prevention of Youth Violence. His research focuses on firearm policy, illegal gun markets, intimate partner violence, and the prevention of youth violence. He has taught violence prevention at Johns Hopkins for the past 16 years and serves as a core faculty member of Hopkins’ pre- and postdoctoral Interdisciplinary Training Program in Violence Research.
Nancy Glass, PhD, MPH, RN, is Associate Professor at Johns Hopkins University School of Nursing and Associate Director Johns Hopkins Center for Global Health. Dr. Glass provides clinical services and conducts intervention research using community-based participatory approaches in the areas of violence prevention and health disparities. She is the Principal Investigator (PI) on a National Institute of Health (NIH)/National Institute of Nursing Research (NINR) funded study to evaluate a workplace intervention to prevent and reduce the impact of Intimate Partner Violence (IPV) on the health, safety, and employment of low-income immigrant and U.S.-born women. In addition, Dr. Glass is the PI of Centers for Disease Control and Prevention (CDC)–funded study to assess for risk and protective factors of repeat victimization for women in same-sex relationships and the Co-PI of a CDC-funded study to evaluate the effectiveness of a permanent housing program for battered women. Dr. Glass is the Past-President of the Nursing Network on Violence Against Women, International and serves as an Ambassador for ResearchAmerica’s Paul G. Rogers Society for Global Health Research.
References
- Bailey JE, Kellerman AL, Somes GW, Banton JG, Rivara FP, & Rushford NP (1997). Risk factors for violent death of women in the home. Archives of Internal Medicine, 157, 777–782. [PubMed] [Google Scholar]
- Berk RA, Berk S, Loseke DR, & Rauma D (1983). Mutual combat and other family violence myths In Finkelhor D, Gelles RJ, Hotaling GT, & Straus MA (Eds.), The dark side of families (pp. 197–212). Beverly Hills, CA: Sage. [Google Scholar]
- Block CR, & Christakos A (1995). Intimate partner homicide in Chicago over 29 years. Crime & Delinquency, 41(4), 406–526. [Google Scholar]
- Block CR, McFarlane JM, Walker GR, & Devitt CO (1999). Beyond public records databases: Field strategies for locating and interviewing proxy respondents in homicide research. Homicide Studies, 3, 349–366. [Google Scholar]
- Breitman N, Shackelford TK, & Block CR (2004). Couple age discrepancy and risk of intimate partner homicide. Violence and Victims, 19, 321–342. [DOI] [PubMed] [Google Scholar]
- Browne A (1987). Battered women who kill. New York: Free Press. [Google Scholar]
- Browne A, Williams KR, & Dutton DC (1998). Homicide between intimate partners In Smith MD & Zahn M (Eds.), Homicide: A sourcebook of social research (pp. 149–164). Thousand Oaks, CA: Sage. [Google Scholar]
- Campbell JC (1981). Misogyny and homicide of women. Advances in Nursing Science, 3(2), 67–85. [DOI] [PubMed] [Google Scholar]
- Campbell JC (1986). Nursing assessment of risk of homicide for battered women. Advances in Nursing Science, 8(4), 36–51. [DOI] [PubMed] [Google Scholar]
- Campbell JC (1992). “If I can’t have you, no one can”: Power and control in homicide of female partners In Radford J & Russell DEH (Eds.), Femicide: The politics of woman killing (pp. 99–113). New York: Twayne. [Google Scholar]
- Campbell JC (1995). Assessing dangerousness. Newbury Park, CA: Sage. [Google Scholar]
- Campbell JC (2002). Safety planning based on lethality assessment for partners of batterers in treatment. Journal of Aggression, Maltreatment, and Trauma, 5(2), 129–143. [Google Scholar]
- Campbell J. C. (2004). Helping women understand their risk in situations of intimate partner violence. Journal of Interpersonal Violence, 19(12),1464–1477. [DOI] [PubMed] [Google Scholar]
- Campbell JC (2005). Assessing dangerousness in domestic violence cases: History, challenges, and opportunities. Criminology and Public Policy, 4(4), 653–672. [Google Scholar]
- Campbell JC (2007). Assessing dangerousness: Violence by batterers and child abusers. New York: Springer. [Google Scholar]
- Campbell JC, O’Sullivan C, Roehl J, & Webster DW (2005). Intimate Partner Violence Risk Assessment Validation Study: The RAVE Study. Final Report to the National Institute of Justice (NCJ 209731–209732). Retrieved February 1, 2007, from http://www.ncjrs.org/pdffiles1/nij/grants/209731.pdf.
- Campbell JC, Sharps P, & Glass N (2001). Risk assessment for intimate partner violence In Pinard GF & Pagani L (Eds.), Clinical assessment of dangerousness: Empirical contributions (pp. 136–157). New York: Cambridge University Press. [Google Scholar]
- Campbell JC, Webster D, Koziol-McLain J, Block CR, Campbell DW, Curry MA Gary FA, et al. (2003a). Assessing risk factors for intimate partner homicide. National Institute of Justice Journal, 250, 14–19. [Google Scholar]
- Campbell JC, Webster D, Koziol-McLain J, Block CR, Campbell DW, Curry MA Gary FA, et al. (2003b). Risk factors for femicide in abusive relationships: Results from a multisite case control study. American Journal of Public Health, 93(7), 1089–1097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chilton R, & Weber D (1999). Uniform crime reporting program [United States]: Arrests by age, sex, and race for police agencies in metropolitan statistical areas, 1960–1995, ICPSR version [Computer File] Amherst, MA: University of Massachusetts; [producer], 1998. Ann Arbor, MI: Inter-University Consortium for Political and Social Research [distributor]. [Google Scholar]
- Crowell NA, & Burgess AW (1996). Understanding violence against women. Washington, DC: National Research Council. [Google Scholar]
- Daly M, Wiseman KA, & Wilson M (1997). Women with children sired by previous partners incur excess risk of uxoricide. Homicide Studies, 1(1), 61–71. [Google Scholar]
- De Becker G (1997). The gift of fear. Boston: Little, Brown & Co. [Google Scholar]
- Dutton DG, & Kropp PR (2000). A review of domestic violence risk instruments. Trauma, Violence, & Abuse, 1, 171–181. [Google Scholar]
- Dutton DG, Landolt MA, Starzomski A, & Bodnarchuk M (2001). Validation of the propensity for abusiveness scale in diverse male populations. Journal of Family Violence, 16(1), 59–73. [Google Scholar]
- Fagan J, Stewart DE, & Hansen K (1983). Violent men or violent husbands? Background factors and situational correlates In Gelles RJ, Hotaling G, Straus MA, & Finkelhor D (Eds.), The dark side of families (pp. 49–68). Beverly Hills, CA: Sage. [Google Scholar]
- Ferraro KJ, & Johnson JM (1983). How women experience battering: The process of victimization. Social Problems, 30, 325–339. [Google Scholar]
- Fox JA, & Zawitz M (2004). Homicide trends in the United States. Washington, DC: Bureau of Justice Statistics. [Google Scholar]
- Gelles R (1998, October). Lethality and risk assessment for family violence cases. Paper presented at the 4th International Conference on Children Exposed to Family Violence, San Diego, CA. [Google Scholar]
- Glass N, Perrin N, Hanson G, Bloom T, Gardner E, Campbell JC (in press). Risk of re-assault in abusive same-sex relationships. American Journal of Public Health, 98(6), 1021–1027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gondolf EW (2000). How batterer program participants avoid reassault. Violence Against Women, 6(11), 1204–1222. [Google Scholar]
- Goodman L, Dutton MA, & Bennett L (2000). Predicting repeat abuse among arrested batterers: Use of the danger assessment scale in the criminal justice system. Journal of Interpersonal Violence, 10, 63–74. [Google Scholar]
- Hanson RK, & Morton-Bourgon K (2004). Predictors of sexual recidivism: An updated meta-analysis (User Report 2004–02). Ottawa, Canada: Public Safety and Emergency Preparedness Canada. [Google Scholar]
- Heckert DA, & Gondolf EW (2004). Battered women’s perceptions of risk versus risk factors and instruments in predicting repeat reassault. Journal of Interpersonal Violence 19(7), 778–800. [DOI] [PubMed] [Google Scholar]
- Hilton NZ, Harris GT, Rice ME, Lang C, Cormier C, & Lines KJ (2005). A brief actuarial assessment for the prediction of wife assault recidivism: The Ontario Domestic Assault Risk Assessment. Psychological Assessment, 16, 267–275. [DOI] [PubMed] [Google Scholar]
- Johnson H, & Sacco VF (1995). Researching violence against women: Statistics Canada’s national survey. Canadian Journal of Criminology, 37, 281–304. [Google Scholar]
- Klein E, Campbell J, Soler E, & Ghez M (1997). Ending domestic violence: Changing public perceptions. Newbury Park, CA: Sage. [Google Scholar]
- Kropp PR, Hart SD, Webster CD, & Eaves D (2000). The spousal assault risk assessment guide (SARA): Reliability and validity in adult male offender. Law and Human Behavior, 24, 101–118. [DOI] [PubMed] [Google Scholar]
- Krug EG, Dahlberg LL, Mercy JA, Zwi AB, & Lozano R (2002). World report on violence and health. Geneva, Switzerland: World Health Organization. [Google Scholar]
- Langford L, Isaac NE, & Kabat S (1998). Homicides related to intimate partner violence in Massachusetts. Homicide Studies, 2(4), 353–377. [Google Scholar]
- Lyon E (1998, May). The revised K-SID: Analysis of reliability and relationships to new arrests after one year (An interim report). Hartford: The Office of Policy and Management State of Connecticut. [Google Scholar]
- Moracco KE, Runyan CW, & Butts J (1998). Femicide in North Carolina. Homicide Studies, 2, 422–446. [Google Scholar]
- Puzone CA, Saltzman LE, Kresnow M-J, Thompson MP, & Mercy JA (2000). National trends in intimate partner homicide: United States, 1976–1995. Violence Against Women, 6(4), 409–426. [Google Scholar]
- Saunders DG, & Browne A (2000). Intimate partner homicide In Ammerman RT & Hersen M (Eds.), Case studies in family violence (pp. 415–449). New York: Kluwer Academic/Plenum Publishers. [Google Scholar]
- Shackelford TK, & Mouzos J (2005). Partner killing by men in cohabiting and marital relationships. Journal of Interpersonal Violence, 20(10), 1310–1324. [DOI] [PubMed] [Google Scholar]
- Sharps PW, Koziol-McLain J, Campbell JC, McFarlance J, Sachs C, & Xu X (2001). Health care providers’ missed opportunities for preventing femicide. Preventive Medicine, 33(5), 373–380. [DOI] [PubMed] [Google Scholar]
- Strauss MA, & Gelles RJ (1990). Physical violence in American families. New Brunswick, NJ: Transaction. [Google Scholar]
- Stuart EP, & Campbell JC (1989). Assessment of patterns of dangerousness with battered women. Issues in Mental Health Nursing, 10(3–4), 245–260. [DOI] [PubMed] [Google Scholar]
- Thompson MP, Basile KC, Hertz MF, & Sitterle D (2006). Measuring intimate partner violence victimization and perpetration: A compendium of assessment tools. Atlanta, GA: Centers for Disease Control and Prevention, National Center for Injury Prevention and Control. [Google Scholar]
- Weisz A, Tolman R, & Saunders DG (2000). Assessing the risk of severe domestic violence. Journal of Interpersonal Violence, 15(1), 75–90. [Google Scholar]
- Williams KR, & Houghton AB (2004). Assessing the risk of domestic violence re-offending: A validation study. Law and Human Behavior, 28(4), 437–455. [DOI] [PubMed] [Google Scholar]
- Wilson M, & Daly M (1993). Spousal homicide risk and estrangement. Violence and Victims, 8(1), 3–15. [PubMed] [Google Scholar]