
FIGURE 7.
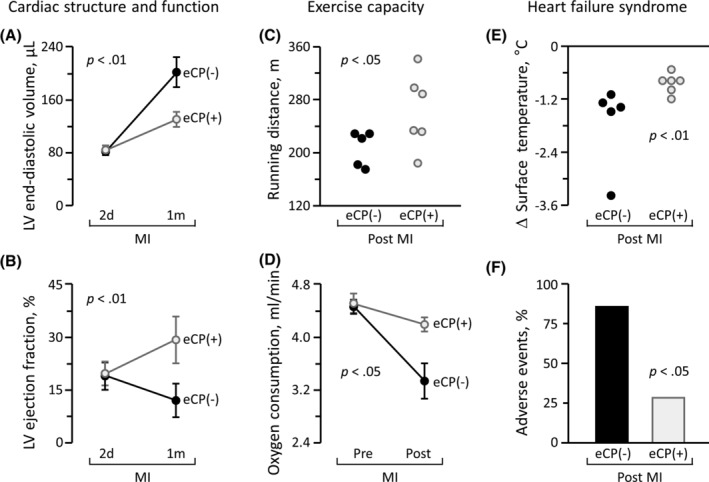
Therapeutic benefit in ischemic heart failure syndrome. Age and sex‐matched mice underwent myocardial infarction (MI) followed by randomization to vehicle control (eCP[−], n = 7) or eCP (eCP[+], 600 000 cells per heart, n = 7) treatment. Multiparametric validation of efficacy included monitoring of cardiac structure and function on echocardiography (A, B), exercise capacity on treadmill (C), whole body metabolism (D), vital sign (E), and cardiac events (F). Despite similar deterioration 2 days (2d) post‐MI induction, eCP(−) and eCP(+) cohorts diverged over time. Within 1 month (1m) of follow‐up, infarcted animals assigned to the eCP(−) group developed progressive cardiac dilatation and pump failure (A, B), reduced exercise performance (C, D), and poor circulation (E), resulting in a high incidence of adverse events (F). In contrast, eCP treatment prevented left ventricular (LV) enlargement (A), improved LV contractility (B), extended running distance (C), augmented maximum oxygen consumption (D), and maintained systemic circulation (E), protecting from severe decompensated heart failure (F). Animal numbers (n) with statistical analysis were; in (A, B, D), n = 5 in eCP(−) and n = 6 in eCP(+) with two‐way repeated measures ANOVA; in (C, E), n = 5 in eCP(−) and n = 6 in eCP(+) with Mann‐Whitney test; in (F), n = 7 in eCP(−) and n = 7 in eCP(+) with Fisher's exact test, respectively. The number declines in (A‐E), from the original cohorts (seven per group), is reflective of mortality during follow‐up. ANOVA, analysis of variance