

Abstract
Goals:
A comprehensive review of treatments for nausea and vomiting.
Background:
Nausea and vomiting (N/V) are common symptoms encountered in medicine. While most cases of acute N/V related to a specific cause can be straightforward to manage, other cases of acute N/V such as chemotherapy-induced nausea and vomiting (CINV) and especially chronic unexplained nausea and vomiting (CUNV)] can be difficult to control, leading to significant decline in the patient’s quality of life and increased cost of medical care from repeated hospitalizations.
Study:
Traditional management has relied on pharmacotherapy which may be inadequate in a certain proportion of these patients. Many of the medications used in the management of N/V have significant side effect profiles making the need for new and improved interventions of great importance.
Results:
This review covers a broad review of the pathophysiology of N/V, pharmacotherapy, including safety concerns and controversies with established pharmaceuticals, newer immunotherapies, bio-electric neuromodulation (including gastric electrical stimulation), behavioral and surgical therapies, and complimentary medicine.
Conclusions:
Based on emerging understandings of the pathophysiology of nausea and vomiting, improved therapies are becoming available.
Keywords: ausea, Vomiting, Pharmacotherapy, Gastric Electric Stimulation, Autonomic Dysfunction
Introduction
Nausea and vomiting (N/V) are common symptoms which may occur as a chronic or recurrent condition, but in many cases are difficult to manage. Nausea and/or vomiting occur in a variety of clinical settings, such as the post-operative period, and are often associated with the use of chemotherapeutic agents or as a result of disease or dysfunction of the gastrointestinal system including motility disorders. In some patients with nausea and vomiting no apparent cause is found.1 While acute episodes of N/V associated with a specific cause (e.g. motion sickness) may be straightforward to manage, chronic N/V either related to a disease like gastroparesis or as a functional disorder, can be disabling for the patent and difficult to manage. Traditionally, pharmacotherapy has been the cornerstone of management, but this approach may prove inadequate in a number of patients. Newer and emerging management modalities include bio-electrical stimulation of the gastrointestinal tract, behavioral training and newer surgical therapies. Additionally, alternative therapies like acupuncture and ginger may help some patients. In this article, we review the basic pathogenic mechanisms involved in N/V, outline the management approach including pharmacologic therapy, bio-electric stimulation and alternative therapies like behavioral therapy and provide some insight into future directions.
Brief review of the pathophysiology of Nausea and Vomiting (N/V)
Nausea and vomiting may occur together or independent of each other and this may be due to differing pathophysiologic mechanisms. Newer antiemetic agents like the 5-Hydroxytryptamine 3 (5-HT3) and Neurokinin 1 (NK1) receptor antagonists, while being very effective for vomiting, are less satisfactory for the management of nausea.2–5 A brief review of the pathways and the chemicals involved in the genesis of N/V is outlined specifically as it applies to the use of pharmacologic agents and electrical stimulation of the GI tract for the treatment of N/V.
The central conductor orchestrating the vomiting mechanism has been called the vomiting center (emetic center). Rather than being a distinct anatomical area this is considered more of a functional zone or a signal generating area in the medulla and comprises the reticular formation and the nucleus tractus solitarius. This center receives input from various areas of the body which include vagal afferents from the gastrointestinal tract, psychogenic stimuli from the cerebral cortex and stimuli from the vestibular and visual areas as well as the chemoreceptor trigger zone (CTZ). The CTZ is an area of the medulla located in the area postrema that is functionally outside of the blood brain barrier (BBB) and is activated by various endogenous and exogenous chemicals including medications as demonstrated in Figure 1. Efferent fibers from the emetic center that coordinate the various responses involved in the process of N/V travel mainly via the vagus nerve but also via cranial nerves V, VII, IX and X.6 However, the roles of the peripheral and autonomic nervous systems in nausea and vomiting have not yet been thoroughly investigated.7
Figure 1:
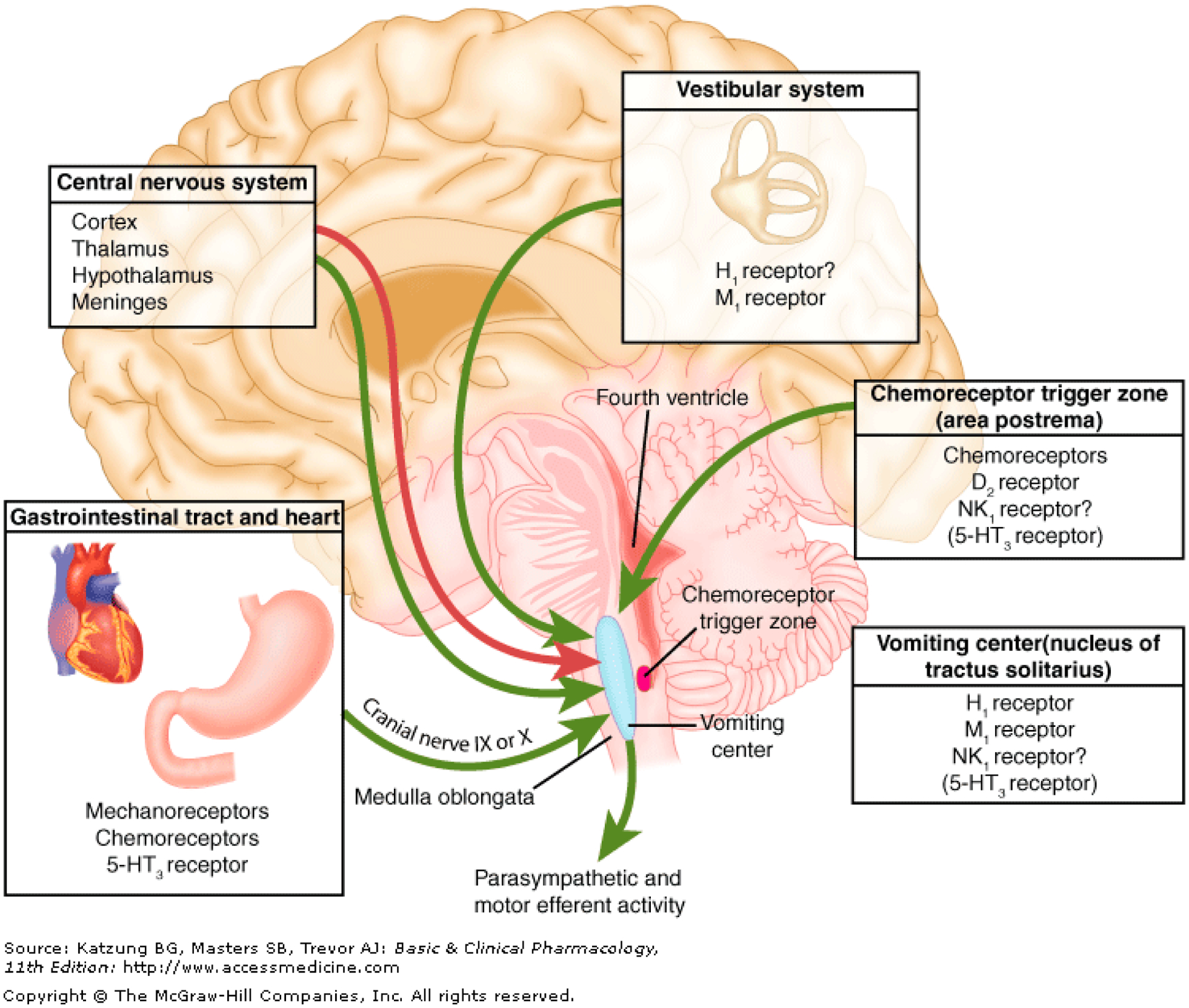
The Pathophysiology of Nausea and Vomiting. From: Krakauer EL, Zhu AX, Bounds BC, Sahani D, McDonald KR, Brachtel EF. Case records of the Massachusetts General Hospital. Weekly clinicopathological exercises. Case 6–2005. A 58-year-old man with esophageal cancer and nausea, vomiting, and intractable hiccups. N Engl J Med. 2005 Feb 24;352(8):817–25. doi: 10.1056/NEJMcpc049037. PMID: 15728815. Used with permission.
Mechanism of Nausea and Vomiting of Gastrointestinal (GI) Tract Etiology
Chemoreceptors and mechanoreceptors in the GI tract can sense various chemical (acids, irritants, toxins) and mechanical (distension) stimuli. As seen in Figure 1, afferent fibers take this signal to the emesis center, primarily via vagal pathways. Detection of these various stimuli is the function of the enterochromaffin cells (ECC), which in turn release mediators that stimulate the above mentioned vagal pathways.8 A variety of chemical mediators are involved including 5HT acting on the 5HT3 receptor, substance P acting on the NK1 receptor and cholecystokinin (CCK). Various other mediators are involved in enhancing or attenuating the effects of these initial mediators. For example, in the case of 5HT release, acetylcholine (M3 receptors), norepinephrine (B receptors), histamine (H2 receptors) and 5HT itself increase 5HT release whereas GABA (GABA-B receptors), VIP and somatostatin inhibit 5HT release.9 Antagonism of these various chemical mediators form the basis of antiemetic medications. However, the roles of the autonomic nervous systems and the peripheral nervous systems, in addition to the enteric nervous system, remain much less well defined as etiologies of N/V, whether of GI tract origin or not.10
Historically nausea and vomiting have been thought to be a continuum of the same pathophysiologic mechanism caused by similar stimuli and involving the same neural circuits but of a varying intensity and or duration. However, the two symptoms can occur independently of each other. Thus, nausea and vomiting have traditionally been studied together and it has been expected that management of one would effectively manage the other. Since vomiting is more explicit and objective, studies have focused on vomiting as the primary endpoint. However, in the setting of CINV, CUNV, and post-operative nausea and vomiting (PONV), nausea still remains a poorly controlled symptom compared to vomiting.11 Both 5HT3 and NK1 blockers are less effective in controlling nausea than vomiting.4 In addition, a significant proportion of patients undergoing chemotherapy may experience nausea alone.12,13 Some patients continue to experience distressing nausea symptoms even after placement of enteral tubes for feeding.14 These factors have led some to declare that nausea remains a neglected symptom.5
Functional gastrointestinal disorders (FGIDs) represent a group of chronic unexplained gut syndromes and have traditionally been considered to have no pathology and no known cause although various alterations in the brain-gut axis have been implicated. Functional dyspepsia (FD) is often misdiagnosed as gastroparesis as it shares many of the same symptoms, including nausea and delayed gastric emptying. Emerging evidence suggests that immune activation and subtle intestinal pathologies are involved in the disease process. In genetically primed hosts, antigen presentation to the mucosa (e.g. microbial antigens) induces intestinal immune activation with low grade inflammatory changes. This inflammation subsequently causes neuronal functional and structural alterations with local intestinal hypersensitivity and motor dysfunction. Immune activation may account for the female predominance in these functional disorders. FGIDs are often associated with extraintestinal symptoms such as anxiety and fatigue which may be attributed to cytokine release with intestinal immune activation.15
The pathophysiology of nausea and vomiting related to gastroparesis is not fully understood. Much controversy exists about the distinction between gastroparesis and FD as many with gastroparetic symptoms, including nausea and vomiting, do not have delayed gastric emptying. It is hypothesized that multiple systems, including anatomic, autonomic, inflammatory, electrophysiologic and hormonal, are involved in patients with gastroparesis symptoms. A recent study of patients with gastroparesis symptoms evaluated them in each of these 5 categories. They found that all patients with these symptoms had abnormalities in each of the 5 categories studied.10 A vast majority were found to have elevated inflammatory markers including TNFα and IL-6, elevated cutaneous electrogastrogram frequency, interstitial cells of Cajal count abnormalities as well as dysfunction in anatomic and hormonal functions. N/V related to gastroparesis appears to be a multifactorial process with inflammation playing a key role in symptom development.10
Nausea and Vomiting related to Autonomic Dysfunction.
The functions of the majority of the gastrointestinal (GI) tract are independent of voluntary control rather being affected by the intrinsic enteric nervous system as well as the extrinsic neural supply via the autonomic nervous system (ANS). Thus, it is not surprising that disorders of the autonomic nervous system can manifest in a wide variety of GI symptoms including nausea and vomiting.
The autonomic nervous system is responsible for maintaining homeostasis through a variety of reflexes to external stimuli and change in organ function. The ANS regulates gastric emptying through a complex coordination of smooth muscle contraction and innervation by the enteric and central nervous systems.16 Parasympathetic activity is involved in increased secretions and motility while the sympathetic nervous system decreases secretions and motility.
There is a poor correlation between symptom severity of gastroparesis and degree of gastric emptying. CUNV, also known as gastroparesis-like syndrome, presents with similar symptoms as gastroparesis but patients have normal gastric emptying. Nguyen et al found that measures of autonomic dysfunction were commonly seen in patients with symptoms of gastroparesis and CUNV. Parasympathetic dysfunction was associated with more severe symptoms and delayed gastric emptying whereas sympathetic abnormalities were seen in patients with more mild symptoms. The authors believe the symptoms of both CUNV and gastroparesis are related to autonomic dysfunction and that sympathetic hypofunction is an early manifestation of these disease processes.
Orthostatic intolerance including postural orthostatic tachycardia syndrome (POTS) is one of the most common autonomic disorders. It has a wide variety of GI manifestations ranging from nausea and vomiting to abdominal pain and constipation.17–19 Treatment of the underlying orthostatic intolerance was found to resolve the GI symptoms.20 Chronic intestinal pseudo-obstruction is associated with nausea and vomiting and shows many associated features suggestive of autonomic neuropathy.21 Patients with gastroparesis also exhibit features of autonomic neuropathy. Human studies have shown increased sympathetic activity in nausea and vomiting caused by vestibular stimulation.22,23 Chemotherapy-induced nausea and vomiting (CINV) was associated with abnormalities on autonomic testing and patients with pre-existing motion sickness were more likely to have significant chemotherapy related N/V.24,25 In a study involving children with functional abdominal pain, abnormalities in autonomic function testing (orthostatic intolerance and abnormal sweat test) were noted in at least 75% of patients.26 Conversely, patients with dysautonomia of various etiologies have associated nausea and vomiting. Most of the antiemetic agents, especially the newer ones like 5HT3 antagonists and NK1 antagonists, exert their effect via autonomic pathways.
Clinical tests are available that assess the functional integrity of different aspects of the autonomic function system. Standard tests of autonomic functions include sudomotor (sympathetic cholinergic), cardiovagal (parasympathetic or cholinergic) and sympathetic adrenergic system function.
Multiple studies have utilized autonomic function testing for disorders manifesting nausea and vomiting. A study involving POTS patients found that POTS includes subgroups with and without autonomic neuropathy. In the subset with autonomic neuropathy a decreased sweat output on the Quantitative Sudomotor Axon Reflex Test (QSART) was the most frequent abnormal finding.27 Hejazi et al. showed that in adult patients with CVS, autonomic testing demonstrated autonomic dysfunction in 43% of patients.28
Studies have found a significant prevalence of autonomic disturbances in patients presenting with various symptoms of functional GI disorders as outlined above.26 In a study by Aslam et al, abnormalities in serum catecholamine levels and autonomic function were seen in patients with diabetic gastroparesis and liver cirrhosis, with a system that utilized photoplethysmography to determine adrenergic function.29
Another investigation looked at changes in systemic autonomic tests and heart rate variability before and after gastric neuromodulation in patients with nausea and vomiting. Systemic autonomic testing alone was performed in a subset of patients and systemic autonomic systemic testing and heart rate variability changes were recorded in a second group of patients. After gastric neuromodulation changes in autonomic profile (increase in cholinergic function and decrease in sympathetic function) was noted. It was proposed that gastric bio-electric neuromodulation may work via modulation of the ANS.30
The utility of autonomic function testing (AFT) has been evaluated to guide therapy for patients presenting with GI motility disorders. Patients either received AFT testing and result-guided therapy or symptom-based medical therapy without AFT. In the AFT arm total symptom score (TSS) improved 35% (vs 0% in the non-AFT arm) and symptom improvement was 65% (vs 0% in the non-AFT arm) assessed over a long-term period of 24 to 42 months.31
In a similar study of patients with symptoms of GI motility disorders AFT revealed various abnormalities in over 90% patients. Based on AFT results, individualized therapeutic recommendations (e.g. drugs, devices, and/or behavior) were given for each patient. At follow-up, obtained at a mean of 5.4 +/− 0.5 (range 1 to 12) months, the TSS for these patients decreased from 10.3+/−0.8 at baseline to 7.5 +/− 0.8 (p<0.001). The authors concluded autonomic testing may provide useful information that impacts clinical care.32
Drug therapy of Nausea and Vomiting
Dopamine Receptor Antagonists (DRA)
Dopamine is involved in emesis by stimulating the CTZ. A variety of dopamine receptors have been identified in the nucleus tractus solitarius and the area postrema.33 Inhibition of the dopaminergic D2 receptors in the area postrema inhibits vomiting.34 However, the actual origin of the dopamine required to stimulate these receptors remains unknown. Most clinically used DRAs have no receptor selectivity. Most of the dopamine receptor antagonists (DRAs) cross the blood-brain barrier (BBB) and can block other dopaminergic pathways in the brain producing extrapyramidal symptoms like akathisia, tremor, dyskinesia and drug induced Parkinsonism. They can also cause hyperprolactinemia. Available DRAs include prochlorperazine (Compazine), metoclopramide (Reglan) and domperidone (Limited availability in US)
Metoclopramide (Reglan)
Metoclopramide is a dopamine D2 receptor antagonist, that, in addition to functioning as an anti-emetic agent, also stimulates 5HT4 receptors and stimulates gastric motility. Dopamine has been shown to decrease lower esophageal sphincter (LES) pressure and gastroduodenal motility.35 By blocking these actions of dopamine, metoclopramide augments LES pressure and coordinates antro-duodenal motility. Additionally, it also exhibits some antagonism to the 5HT3 receptors. Thus, the clinical effect is due to a combination of antiemetic and promotility actions.
Metoclopramide is available in oral, suppository and injectable forms. Oral form is available as tablets, liquids and orally dissolving (Metozolv ODT) preparations. Though the latter is orally dissolving, it is still absorbed in the small intestine. Subcutaneous route of administration provides an easy way for patients to self-administer this at home providing plasma levels 80% of the intravenous route.36
A nasally administered form of metoclopramide is also being developed. This would have the obvious benefit of easy drug delivery when nausea and vomiting preclude oral drug intake without having to resort to parenteral administration of the drug; however, the drug’s many side effects would remain.
A randomized, open-label study of patients with diabetic gastroparesis, compared the efficacy and safety of 10 or 20 mg nasal spray or 10 mg tablet and found both doses of the nasal preparation to be significantly better than the oral formulation at reducing the total symptom score (TSS) between baseline and week 6.37 A later study in similar diabetic gastroparesis patients found gastroparesis symptoms of nausea, bloating, early satiety and upper abdominal pain to be significantly reduced in female patients receiving the drug but not in male patients suggesting gender difference in response to nasal metoclopramide.38
The main adverse effect of metoclopramide relates to its extrapyramidal effects which include dyskinesia, dystonia, convulsions, hypertonia, tremors and tardive dyskinesia. In 2009, the US Food and Drug Administration issued a black box warning for metoclopramide and risk of tardive dyskinesia; an irreversible extrapyramidal disorder, which increases with the duration and cumulative dose of treatment. The risk of this developing was found to be greater in patients who took it for more than three months. Although metoclopramide remains the only drug approved for the treatment and symptom relief of acute and recurrent diabetic gastroparesis, the FDA advised against use for longer than 12 weeks in all but exceptional cases.
A head to head trial in 1999 compared domperidone and metoclopramide for efficacy and side effects. In this double-blind, multicenter, randomized study, insulin-dependent diabetes patients with at least three months’ history of gastroparesis symptoms were divided into two groups with half receiving domperidone 20 mg 4 times daily, and half receiving metoclopramide 10 mg 4 times daily. Symptoms of nausea, vomiting, bloating/distension, and early satiety as well as central nervous system (CNS) side effects of somnolence, akathisia, asthenia, anxiety, depression, and reduced mental acuity were evaluated at 2 and 4 weeks. Both drugs were equally effective in alleviating gastrointestinal symptoms, however CNS side effects were more severe and common with metoclopramide.39
Domperidone
Domperidone is closely related to metoclopramide having both central antiemetic and gastric prokinetic effects. However, unlike metoclopramide it crosses the BBB poorly and is virtually devoid of the extrapyramidal side effects. It also does not stimulate the 5HT4 receptor.
Though studies have found conflicting results, domperidone has been implicated in causing QT prolongation, ventricular arrhythmias and sudden cardiac death.40–46
In 2014 the Pharmacovigilance Risk Assessment Committee (PRAC) of the European Medicines Agency (EMA) restricted the use of Domperidone concluding that it posed a significant risk of QT prolongation, cardiac dysrhythmias, and sudden cardiac death (SCD) and made the recommendations to limit the maximum doses of domperidone in adults to 30 mg/ day and use be restricted to less than 1 week.47 Likewise, the U.S. FDA has limited access to this drug through an IND protocol due to the possible risks of cardiac arrhythmias, cardiac arrest, and sudden death.
Domperidone initially became available in 1978. In the 1980s there were multiple case reports of QT prolongation and adverse cardiac events (cardiac arrests/sudden deaths) following administration of high dose parenteral domperidone for N/V prophylaxis in chemotherapy patients.48–52 Some of these patients had hypokalemia. Based on these case reports IV Domperidone was withdrawn from the market globally.
The International Committee on Harmonization (ICH) E14 Guidance on Clinical QT Studies provides guidance on studying a drug’s potential for causing QT prolongation. The thorough QT/QTc (TQT) study is used to determine the values for QT prolongation. TQT studies are conducted in healthy volunteers and use a positive control group (pharmacological or non-pharmacological). A thorough QT/QTc study of domperidone was conducted in a single-center, double-blind, four-way crossover study. Healthy participants were randomized to one of four treatment protocols lasting four days and separated by a 4–9 day washout. The treatment sequence consisted of oral domperidone 10 four times a day, oral domperidone 20 mg four times a day, matching placebo four times a day, or single-dose moxifloxacin 400 mg (positive control)/placebo four times a day. Domperidone at doses up to 80 mg/day was not found to cause clinically relevant QTc interval prolongation.41
Another randomized, placebo-controlled, double-blind, crossover study looked at the QT effects of placebo or oral domperidone alone, ketoconazole alone and combination of domperidone and Ketoconazole on healthy subjects. Medications (domperidone 10 mg, four doses/day at 4 hours’ interval, ketoconazole 200 mg every 12hours) were given orally for 7 days followed by a washout period of 15 days. ECGs recordings were taken on the day before study and at multiple times on day 1, 5, 6 and 7 and RR and QT interval were calculated. Though domperidone was found to cause a significant prolongation of QTC compared to placebo in men, this was clinically not significant. (Overall mean increase in QTC 4.2ms). In women no difference in QTC was seen.53
Another retrospective chart review looked at patients with nausea and vomiting receiving domperidone from 2009 to 2013 under an IND protocol. Doses ranged from 40 to 120 mg/day with 90% receiving 80 to 120 mg/day. Mean duration of therapy was 8 months (range, 3 months to 4 years). Patients had follow-up electrocardiograms available which showed non-significant change in QTc. Just over one fourth of these patients had prolonged QTc at F/U but no cardiovascular complaints. No cases of cardiac arrhythmias were seen. Clinically meaningful symptom improvement was seen in 73% of the patients receiving chronic high dose domperidone treatment.42
Domperidone can also cause hyperprolactinemia which may result in gynecomastia, breast tenderness and menstrual irregularities. The usual starting dose is 20 mg four times a day with a maximum recommended dose of 120mg/day. Although generally unavailable in the US, patients have been known to obtain oral domperidone from outside countries such as Canada. Given the concern for adverse cardiac effects they should be counselled about these risks and a baseline EKG should be performed. Patients with a known prolonged QTc should be counselled to avoid this drug.
Haloperidol
Haloperidol is a DRA similar to metoclopramide in terms of its mechanism of action and adverse effect profile. A recent study in 2017 looked at the efficacy of haloperidol in the treatment of gastroparesis flare with nausea, vomiting and abdominal pain.54 This double blind randomized controlled trial was conducted over a 2-year period and included patients with GP who presented to the emergency department (ED). Patients who were less than 18 years, who had past or current evidence of QT prolongation, hypotension, presence of other acute abdominal conditions, allergy to haloperidol, pregnancy or were unable to provide informed consent were excluded. Patients were assigned to a 5mg intravenous dose of haloperidol in addition to conventional treatment at the discretion of the physician while the control group received placebo in combination with conventional therapy. The severity of nausea (5-point scale) and abdominal pain (10-point scale) were assessed in each patient at baseline and at 15 minutes’ interval for a total of one hour. Adverse effects were also recorded.
It was found that haloperidol in combination with conventional treatment was significantly superior to conventional treatment alone in relieving nausea and abdominal pain in the acute setting and led to a decreased number of hospital admissions in the treatment group. No adverse effects were noted in the study arm. The authors concluded that the study suggested that haloperidol is an effective agent in combination with other conventional analgesic and antiemetic agents for the treatment of gastroparesis in the ED with the caveat that further larger studies were needed to confirm the findings from their study. Follow-up data regarding later adverse effects of participants in this study was not obtained. A 2015 Cochrane review of eight trials including patients treated for acute nausea and vomiting in the emergency setting showed no definitive evidence to support the superiority of one drug over another including metoclopramide, ondansetron, prochlorperazine and promethazine over placebo. This finding suggests that, in the acute setting, nausea will likely improve with supportive treatment regardless of medication selection. The quality of evidence of this review, however, was noted to be low.55 The side effects of haloperidol include hypotension, extrapyramidal movements, akathisia, neuroleptic malignant syndrome, and QT interval prolongation.
CIN-102
A novel dopamine receptor drug, CIN-102, is currently undergoing phase 2 clinical trials. CIN-102 is a peripherally selective dopamine (D2/D3) receptor antagonist. The drug is structurally similar to domperidone, but with the substitution of deuterium atoms allowing for a more stable bond with carbon than non-deuterated domperidone. This substitution is suggested to improve efficacy and tolerability while increasing plasma concentration and half-life. Two phase 1 placebo-controlled studies were completed, which identified no safety concerns. Side effect profiles have been found to be similar to that of non-deuterated Domperidone.
Metopimazine
Metopimazine is a highly potent and selective dopamine D2/D3 receptor antagonist. Metopimazine has dual mechanisms of action: central antagonism of D2 receptors in the area postrema, resulting in the antiemetic and antinauseant properties, and antagonism of D2 receptors in the gut resulting in increased motility. The drug is an established antiemetic that has been approved and marketed for many years in Europe for the treatment of acute conditions. In 2014, preclinical data showed increased amplitude and frequency of antral contractions in dogs, whereas in rats, it showed an increase in gastric emptying of solid foods. In contrast to metoclopramide, metopimazine does not readily cross the blood-brain barrier and does not interact with 5-HT3 or 5-HT4 receptors. Further, unlike domperidone it does not antagonize hERG channels, suggesting a favorable cardiovascular profile. Repurposed metopimazine (NG101) is currently being studied as a potential safer oral alternative to metoclopramide and domperidone for the treatment of gastroparesis.56
Histamine Receptor Antagonists (HRA)
Prochlorperazine (Phenergan) is the most commonly used HRA to treat N/V. Other drugs in this class include diphenhydramine (Benadryl), cyclizine (Cyclivert), dimenhydrinate (Dramamine), doxylamine (in combination with pyridoxine in nausea of pregnancy), and meclizine (Bonnine). These agents work by blocking the histamine (H1) receptors in the emetic area.57,58 They also have central antimuscarinic (M1 receptor) activity, which may contribute to antiemetic effects, but can lead to dry mouth, urinary retention, and drowsiness.
Muscarinic Receptor Antagonists
Muscarinic receptor activity is involved in generation of emetic signals in the emetic center.59 A commonly used antimuscarinic agent is Hyoscine (scopolamine); a belladonna alkaloid which is available in the US as parenteral and transdermal forms. The transdermal patch provides slow release to provide prolonged effects for 72 hours. This drug is routinely used in the prophylaxis and treatment of motion sickness and post-operative nausea and vomiting. Side effects of MRA’s include dry mouth, decreased sweating, blurred vision, tachycardia and urinary retention.
Trimethobenzamide
Trimethobenzamide (Tigan) is an antiemetic with unknown exact mechanism of action, but which acts centrally to directly inhibit the medullary chemoreceptor trigger zone by blocking emetic impulses to the vomiting center. Trimethobenzamide is available as an oral capsule, oral solution, or IM injection. It is approved for CINV, PONV. Diarrhea is one of the main side effects. Although uncommon, some severe CNS effects have been reported, including coma, disorientation, seizure, and some extrapyramidal side effects.
5-HT3 Receptor Antagonists
The discovery of the first 5HT3 antagonist, Ondansetron, in the 1980s ushered in a new era in the treatment of CINV. The highly emetogenic side effects of chemotherapeutic agents like cisplatin, which was only partially controlled by available antiemetic agents like DRA, was significantly more controlled with Ondansetron. In fact, 5HT3RA’s remain the cornerstone of management of CINV in combination with corticosteroids and/or NK1RB and are also extensively used in PONV.
5HT3RA’s, include ondansetron (Zofran), granisetron (Kytril), tropisetron (Navoban), dolasetron (Anzamet), ramosetron (Nasea) and palonasetron (Aloxi) and come in oral, IV and sublingual formulations. Granisetron is also available as a transdermal patch but widespread use has been limited due to cost.
More than 80% of the body’s store of 5-Hydroxytryptamine (5HT, also known as serotonin) is in the gastrointestinal tract, predominantly in the enterochromaffin cells. A variety of stimuli (toxins, chemicals, and distention) cause release of 5HT from the enterochromaffin cells which then acts on 5HT3 receptors found on the vagus nerve terminal, the emetic center and the CTZ.
5HT3 agents all possess similar mechanisms of action but differ in their chemical structures. They are all metabolized in the liver through the CYP2D6 system, with the exception of granisetron (via CYP3A). As the CYP2D6 system exhibits genetic polymorphism, individual patients can exhibit varying response to these drugs.60
5HT3 antagonists have been associated with prolongation of the QT interval on EKG. In one study, Ondansetron, but not Granisetron, was found to cause QT prolongation.61 In another study, though the median QT interval was higher after Palonosetron administration compared to baseline, the difference was not statistically significant.62
A study examined the electrocardiographic and cardiovascular effects of 5HT3RA’s in healthy volunteers and in patients undergoing chemotherapy or surgery by reviewing studies and preclinical data published between 1963 and 2002. The study subjects received either a single parenteral dose alone or a single parenteral dose followed by a short daily course of these agents. 5HT3RA as a class were found to have effects on EKG parameters. However, these changes were small, reversible clinically insignificant and independent of the patient population studied. No serious cardiac events, including torsades, were attributed to the use of 5HT3RA.63
In another study of perioperative use of ondansetron or dolasetron, no difference in QTc was noted in the patients who received or did not receive 5HT3 antagonists.64
In 2012 the FDA issued a safety warning of ECG changes including QT interval prolongation in some patients receiving Ondansetron. It recommended ondansetron be avoided in patients with congenital long QT syndrome and advised ECG monitoring in patients with electrolyte abnormalities, congestive heart failure, bradyarrhythmia, or patients taking other medications that prolong the QT interval.
At the request of the FDA, the manufacturer of Zofran (ondansetron), GlaxoSmithKline (GSK), conducted a randomized, double blinded, single-dose, period-balanced, crossover, placebo-controlled study to investigate the effect of a single IV dose of Zofran on QT interval in healthy volunteers given Zofran at two different doses (8mg or 32 mg) and compared to placebo and Moxifloxacin.65 This study demonstrated that a single 32-mg IV dose increased the QT interval by 20 msec. These findings led to the removal of the single 32-mg IV dose and a change in use of the IV formulation for the management of CINV. However, no changes were made to the oral or IV dosing recommendations for the prevention of PONV.
In a patient in whom there is concern for cardiac adverse effects (e.g. patients with baseline high normal QT intervals, congestive heart failure and acute coronary syndrome) it may be prudent to follow closely with serial EKG monitoring.
5-HT4 Receptor agonists
Serotonin receptors of the 5HT4 family play one of the key roles in the serotonin effects on the GI tract functioning. Research has shown that activation of the 5HT4 receptors of the stomach and intestine stimulates the peristaltic reflex and secretion. Therefore, 5HT4 agonists can be used clinically as a prokinetic agent for diseases associated with decreased motility. There is additional research suggesting the ability of some of these agents to suppress intestinal hypersensitivity. Similar to 5-HT3 receptors, these G-protein coupled receptors are found in the GI tract and modulate release of many neurotransmitters and hormones. The serotonin receptors influence various biologic and neurologic processes. The analgesic effects of some of these agents is partly related to action of 5HT4 receptors of intestinal afferents and spinal sensory neurons.
Cisapride
Cisapride is a 5-HT4 receptor agonist which facilitates acetylcholine release from myenteric neurons through a 5-HT4 receptor-mediated effect. Cisapride is the prototype of serotonergic agonists promoting esophageal peristalsis, augmenting lower esophageal sphincter pressure, and accelerating gastric emptying and colonic transit. In clinical trials cisapride demonstrated variable efficacy in both short- and long-term therapy of gastroparesis and dyspepsia as well as gastroesophageal reflux disease, chronic constipation and chronic intestinal pseudo-obstruction.66 Serious cardiac arrhythmias related to QT interval prolongation were reported by Health Canada beginning in 1996 with warnings issued by the US Food and Drug Administration shortly after in 1998. Cisapride was taken off the US market by 2000 which cast a negative light over the entire drug class until newer and safer options have more recently become available.67
Tegaserod
Tegaserod is a 5-HT4 receptor partial agonist, which exerts its effect by stimulating the release of neurotransmitters thereby increasing the peristaltic reflex and decreasing visceral sensitivity. This helps to accelerate small bowel and colonic transit. Tegaserod is especially helpful in improving bloating, abdominal pain, and constipation, and may also be helpful as a prokinetic/antiemetic when nausea is related to poor GI motility.
Tegaserod is available only as an oral tablet and is rapidly absorbed following oral administration with peak plasma concentrations reached after approximately 1 hour. Absolute bioavailability is about 10% under fasted conditions. Food reduces the bioavailability of tegaserod by 40 to 65% and the C(max) by 20 to 40%. The most common side effects are diarrhea and flatulence, but in a large double blind RCT only 1.6% of patients discontinued the drug due to these side effects.68 Tegaserod was withdrawn in 2007 due to concerns over an increased risks of cardiovascular adverse effects. The manufacturer denied this claim, because pre-existing cardiovascular disease or risk factors were attributed to all affected patients. Thus, no causal relationship between tegaserod use and cardiovascular events was clearly shown. A matched case-control study of tegaserod-treated with untreated patients found no association between tegaserod and adverse cardiovascular outcomes. Tegaserod was resubmitted to the Food and Drug Administration in 2018 for use in a low-risk population and is now available again the US.69
Prucalopride
Prucalopride is a 5-HT4 receptor agonist, which activates the 5-HT4 receptors via intraluminal drug and increases propulsive motor activity in a graded manner. Stimulation of 5-HT4 receptors by 5-HT or drug such as prucalopride is essential for normal bowel motor pattern generation. Prucalopride functions to increase intestinal and colonic motility and has additionally demonstrated promise in the treatment of gastroparesis, post-op ileus, and opiate induced constipation.70 Prucalopride is available only as an oral tablet, with a bioavailablity of >90%, and peak plasma time of 2–3 hours. Prucalopride was introduced to market in 2009 and had been used in Europe since 2010, Canada since 2011, and was recently approved in December 2018 for use in US for chronic idiopathic constipation.71 Unlike previously available 5-HT4 receptor agonists such as cisapride and tegaserod, prucalopride does not interact with the cardiac hERG potassium channels or other serotonergic receptors in blood vessels and is not reported to be associated with an increase in major adverse cardiovascular events.72 In clinical trials, suicide, suicide attempts, and suicide ideation have been reported, though no causal relationship could be established. Headache, abdominal pain, nausea, and diarrhea were the most common adverse effects reported in the clinical trials.
Velusetrag
Velusetrag is a potent, highly selective 5-HT4 agonist, which has preferential binding to the 5-HT4 receptor compared with all other 5-HT receptor subtypes with selectivity greater than 500-fold. Velusetrag functions to activate 5-HT4 receptors on gastrointestinal motor neurons, release excitatory neurotransmitters such as acetylcholine and substance P which promotes propulsion of contents along the gastrointestinal tract. Velusetrag is associated with accelerated colonic and orocecal transit with single dosing in healthy subjects as well as significant effects on gastric and colonic transit with multiple dosing.73 A recent phase 2b study showed significant improvement in gastric emptying (defined as <10% reduction in GES hour-4 retention) compared to placebo. The most commonly reported adverse events reported were diarrhea, nausea and headache with higher rates in groups receiving 15 or 30 mg dosing compared to 5 mg. There was no difference in the number of cardiac adverse events in velusetrag treated subjects compared with placebo in the clinical trial.74
Neurokinin 1 receptor antagonists (NK1RA)
In the early 2000s NK1 blockers were introduced in clinical practice and proved to be extremely useful in the management of CINV, though also were effective in PONV. In CINV NK1RA have proved beneficial in the delayed phase N/V where 5HT3RA are less effective. Neurokinin receptors have been found in the CNS neurocircuits as well as in the peripheral vagal afferents.75–77 Perhaps because of their central site of action where multiple inputs converge, in animal studies NK1RA have been found to be a more effective antiemetic against a variety of emetogenic stimuli arising from abdominal afferents, CTZ and vestibular area.78
Aprepitant
Aprepitant (Emend) is an oral NK1 receptor antagonist and is currently available in the United States for CINV and PONV. Case reports have described successful use of Aprepitant in gastroparesis associated nausea and vomiting.79,80 The APRON Trial (Aprepitant for the Relief of Nausea in Patients with Chronic Nausea and Vomiting of Presumed Gastric Origin Trial) compared aprepitant (125 mg orally daily) with placebo for symptomatic relief of patients with nausea and vomiting of suspected gastric dysfunction. This 4-week multicenter, parallel-group, double-blinded, masked, randomized clinical trial randomized patients to either aprepitant or placebo. Over half of the patients had delayed gastric emptying and the rest had normal or rapid emptying with symptoms of gastroparesis. The primary endpoint of improvement of nausea with aprepitant vs. placebo was not met. (46% with aprepitant vs. 40% with placebo; RIR=1.2, 95% CI: 0.8–1.7; P=0.43). However compared with placebo, aprepitant use resulted in a greater decline in mean 4-week daily hours of nausea (−2.5 vs. −1.2 hrs; P=0.03), mean 4-week Gastroparesis Cardinal Symptom Index (GCSI) score (−1.3 vs −0.7; P=0.001), and greater improvement in multiple other Patient Assessment of Gastrointestinal Disorders Symptom Severity Index (PAGI-SYM) and Gastrointestinal Symptom Rating Scale (GSRS) measures.81
Tradipidant
Other NK1 receptor antagonists are now undergoing clinical trials in the US. Tradipidant, is another such NK1RA, which underwent a phase II clinical trial in 2018. Patients with gastroparesis were followed over a period of 4 weeks. Tradipitant resulted in statistically significant improvement in nausea scores, as well as improvement in number of nausea free days, and improvement in most of the symptom severity scales. Tradipitant met the primary endpoint of the study of change in nausea score as measured by patient daily diaries (change of −1.2 for Tradipitant versus −0.7 for placebo, p=0.0099) and also met the related endpoint of improvement in the number of nausea free days (an addition of 28.8% of days for tradipitant versus 15.0% for placebo, p=0.0160.82,83 A phase III trial evaluating the effectiveness of tradipitant in the treatment of motion sickness is currently underway.
Ghrelin Receptor Agonists
Due to the lack of approved agents research has continued exploring a number of molecular targets which can help accelerate GI motility. One such target, Ghrelin, is an amino acid peptide and neurohumoral transmitter, which functions as a natural ligand for the grehlin or growth hormone secretagogue (GHS-1a) receptor. Grehlin has been studied due to its important physiologic role in the regulation of body weight and appetite. Stimulating grehlin receptors stimulates increased growth hormone, prolactin, and cortisol levels, and increases appetite. This naturally occurring peptide is found predominantly in the stomach, but is present in most GI organs, and grehlin receptors are expressed throughout the GI tract as well as in the CNS. Ghrelin receptors are also located on the nodose ganglion cells in vagal afferent pathways, and animal models have shown that administration of grehlin reduced the vagal afferent firing, while ghrelin receptor antagonists reverse the effect. Other studies demonstrate that grehlin exerts prokinetic effects in the stomach, and accelerates gastric emptying, as well as reducing meal related symptoms in patients with gastroparesis.84 Proof of this concept was provided by studies on fasting motility in humans, and gastric emptying in patients with idiopathic gastroparesis. There is also pharmacological evidence for expression of the GHS-1a receptor in the GI tract.85 These beneficial effects have led to interest in the development of ghrelin-like drugs for the treatment of gastroparesis, as well as colonic dysmotility.
Relamorelin
Relamorelin is an example of a ghrelin agonist and is a synthetic pentapeptide and selective agonist of ghrelin and growth hormone secretagogue receptor. It has similar characteristics to native ghrelin, but has improved stability and longer half-life, and binds to the GHS-1a receptor with three times greater potency affinity than natural Ghrelin. Relamorelin is centrally penetrant and has been shown to accelerate gastric emptying and improve symptoms in patients with diabetic gastroparesis. A phase IIB study was conducted in patients with diabetic gastroparesis and showed a 75% reduction in vomiting frequency across all doses tested. This was not statistically significant result due to high placebo response, however four common symptoms of GP were significantly reduced over the study period in all dose groups, compared to placebo. Relamorelin also accelerated gastric emptying at all three doses compared to placebo.86 However, a dose-related worsening of glycemic control was noted in 14.5% of patients receiving relamorelin with some requiring insulin or other antidiabetic medication dose adjustments.87 Phase III trials studying the 10ug twice daily and placebo dosing in progress now will likely involve closer monitoring of glycemic control as well as proactive glycemic management.88
Motilin Receptor Agonists
Structurally similar to ghrelin, motilin is a peptide that is synthesized and released in the duodenum and jejunum, with smaller amounts in the gastric antrum, during fasting and post-prandial phases. While fasting motilin is released in association with phase III of the Motor Migrating Complex (MMC). During this phase, high-amplitude propulsive contractions are believed to help clear the stomach and intestine from undigested material. Following its discovery, the macrolide antibiotic, erythromycin, was found to activate the motilin receptor inducing these high-amplitude gastric propulsive contractions as well as stimulating gastric fundic contractility and increasing gastric emptying. Another macrolide, azithromycin, has also demonstrated activity as a motilin receptor agonist, but clinical trial data is limited. These antibiotics are thought to have no central antiemetic effect, so reductions in nausea and vomiting are attributed to its motor stimulation properties.89 Although not FDA approved for this indication, erythromycin has been widely used in the treatment of gastroparesis. The IV formulation has been found to be more effective than oral form and can be effectively utilized in the acute and hospital settings. Long-term use of erythromycin is often not recommended due to tachyphylaxis, poor bioavailability of oral formulation, risk of antibiotic resistance, ability to prolong QT interval and its interactions with other medications metabolized by cytochrome P450 3A4.90
Camicinal
Camicinal (GSK962040) is a first-in-class small molecule (non-macrolide) motilin receptor agonist with potential use in nausea and vomiting secondary to delayed gastric emptying. Camicinal was designed with greater specificity for the recombinant human motilin receptor which would potentially decrease the negative effects seen with more nonspecific structures. Early studies have shown increased solid food emptying in healthy volunteers with type 1 diabetes and symptoms of gastroparesis. Another 2014 phase II study demonstrated observed symptom improvements in diabetic patients with gastroparesis and has been well tolerated.91 Further studies are needed to evaluate the safety profile of camicinal.
Pterins
Pterins are cyclic compounds all derived from guanosine triphosphate (GTP). GTP can be metabolized to tetrahydrobiopterin (BH4), which is a cofactor in the production of monoamine neurotransmitters and nitric oxide and can be oxidized to potent antioxidants such as dihydrobiopterin and biopterin. Measurement and quantification of pterins and oxidized/catabolized forms provides direct evidence of immune system inflammation and may represent a set of biomarkers that are sensitive and effective at quantifying stress. Tetrahydrobiopterin (BH4) is a cofactor in the production of various signaling molecules, including nitric oxide, dopamine, adrenaline, and noradrenaline. BH4 levels are critical for processes associated with cardiovascular function, inflammation, mood, pain, and neurotransmission. There is increasing evidence suggesting that BH4 is upregulated in chronic pain conditions. Drugs that can affect BH4 metabolism could therefore be helpful in chronic pain conditions.
CNSA-001 (Sepiapterin)
Tetrahydrobiopterin is an essential cofactor for nitric oxide synthetase, as well as of aromatic amino acid hydroxylases of phenylalanine, tyrosine, and tryptophan. Neuronal nitric oxide synthase (nNOS) is expressed by many nerves throughout the GI tract which helps to generate nitric oxide, a key regulator of motility. In diabetes, synthesis of BH4 is decreased resulting in NOS uncoupling and overproduction of superoxide instead of NO. This may result in reduced postprandial accommodation and symptoms of bloating, fullness, nausea and vomiting. CNSA-001, a natural precursor of BH4, has been shown to increase circulating levels in humans and is thought to correct nNOS coupling and restore NO production to help improve gastric accommodation in patients with diabetic gastroparesis. It is a more stable molecule and transported more efficiently across cellular membranes than BH4.92 A recent Phase II trial showed that CNSA-001 improved gastric accommodation and early satiety in women with diabetic gastroparesis compared to placebo.93
Tricyclic Antidepressants
Tricyclic antidepressants (TCAs) have been associated with moderate symptom reduction in chronic nausea and vomiting related to functional disorders such as cyclical vomiting syndrome and chronic functional nausea. The main drugs in this class used for the treatment of nausea and vomiting are nortriptyline, amitriptyline, imipramine and desipramine, although others have shown benefit, as well. TCAs have antihistaminic and antimuscarinic activity which help block these receptors in the emetic center. In a retrospective study of patients with chronic functional nausea, 51% of patients had a complete response and 33% had moderate reduction in symptoms with low dose TCAs.94 TCAs in low doses have also been used in the treatment of nausea, vomiting and abdominal pain associated with gastroparesis although there is little evidence to support this. The NORIG (Nortriptyline for Idiopathic Gastroparesis) trial, a multicenter, parallel-group, placebo-controlled, double-masked, randomized clinical trial showed no primary symptomatic improvement outcome between patients randomized to nortriptyline vs placebo.95 Cardiovascular, anticholinergic and neurologic side effects are associated with TCAs and may present as fatal arrhythmias, fever, dry mouth, urinary retention or altered mental status which may limit their use.
In practice patients with chronic or recurrent N/V may not have adequate relief with use of a single drug. Thus, combination of drugs is used which are more effective due to inhibition of multiple pathways involved in N/V. One commonly used combination is a 5HT3 antagonist with promethazine, sometimes with the addition of scopolamine patch. In a pilot study (“ZAP”) published as an abstract the use of ondansetron (Zofran), additional fluids and promethazine (Phenergan) showed continued control of vomiting, nausea, and GI total symptoms, statistically significant by ANOVA (p < 0.01).96 This retrospective study looked at the long term efficacy and safety of either promethazine alone, ondansetron alone or combination of the two. The cohort included idiopathic gastroparetic symptom patients (IGp) and diabetic gastroparetic symptom patients (DGp) and were followed up on a short-term (1 month to 1 year) and long-term (4 years to 10 years) basis. Patients had short and long-term improvement in N/V and symptom scores with ondansetron and/or promethazine. However, patients in this long-term study were found to have noticeable mortality. In the IGp group cause of death was sepsis in one patient and cardiopulmonary (often thrombotic) causes in the remaining three. In the DGp group all deaths were due to cardiopulmonary causes either myocardial infarction of pulmonary emboli.
Immunotherapy for Nausea and Vomiting
Immune mediated autonomic disorders (autoimmune dysautonomia) may present with manifestation of gastrointestinal dysmotility only and is known as both autoimmune gastrointestinal dysmotility (AGID) and gastrointestinal autoimmune neuropathy (GAIN).97 This may be an idiopathic condition or occur as a result of a paraneoplastic condition.98,99 Common manifestations include gastroparesis, intestinal pseudo-obstruction and colonic inertia. Various antibodies have been linked with this condition and some of these include type 1 antineuronal nuclear autoantibody (ANNA-1, also called “anti-Hu”), ganglionic nicotinic acetylcholine receptors (AChR), voltage-gated neuronal potassium channel-complex (VGKC) and glutamic acid.97,99,100 In the case of gastroparesis, evidence of immune mediated damage has been shown in full thickness gastric biopsy specimens. These have shown increased CD-45 immunofluorescence in the myenteric plexus and increased CD-68 in the muscle layer.101 Decreased numbers of interstitial cells of Cajal and nerve fibers have also been demonstrated in these biopsies.
Immunotherapy has emerged as a promising avenue of treatment for these conditions. Immunotherapy has been evaluated as an aid to diagnosing autoimmune gastrointestinal dysmotility in a recent retrospective study.102 Inclusion criteria was defined by prominent gastrointestinal dysmotility symptoms with objective abnormalities on scintigraphy–manometry, presence of serum neural autoantibodies or personal/family history of autoimmune disease and having undergone treatment with immunotherapy on a trial basis (intravenous immune globulin, methylprednisolone, or both). After a 6 to 12-week trial of immunotherapy, 74% had improvement. Of these, 29% had both symptomatic and scintigraphic improvement, 47% had symptomatic improvement alone and 24% had scintigraphic improvement alone. Of the responders who underwent retesting with autonomic testing or manometry, the majority had improvement.
Another pilot retrospective case series looked at the effects of immunotherapy using different agents in female gastroparesis patients.103 These patients had experienced suboptimal response to medical therapy and/or gastric bio-electrical stimulation. All had undergone full thickness gastric biopsies showing presence of inflammatory markers and positive GAD-65 antibodies. Treatment consisted of mycophenolate alone, combination of mycophenolate and methylprednisolone or Intravenous Immunoglobulin (IVIG) alone. IVIG was given weekly for 8 to 12 weeks, Mycophenolate daily for 12 weeks and combination of mycophenolate and methylprednisolone was given daily for 8 to 12 weeks. As a whole group, 55% had improvement in vomiting and 45% had improvements in nausea, abdominal pain and bloating. TSS improved in 55% of patients. Maximum improvement was seen in the patients receiving IVIG. The authors concluded that while randomized controlled and blinded trials are needed to further validate the potential clinical benefit, immunotherapy should be considered as a part of the armamentarium against gastroparesis.
Other studies have looked to demonstrate an immune system pathology (presence of autoantibodies) underlying some of the idiopathic gastroparesis patients and their responses to IVIG regimens.104 Patients with idiopathic gastroparesis refractory to medical and/or gastric enteral stimulation therapy with positive serological markers received IVIG infusions weekly for 12 weeks. Response was defined as 20% reduction in Total Symptom Score (TSS). 64% of the patients who received IVIG infusions for 12 weeks responded to treatment. Symptom scores for nausea, vomiting, anorexia and abdominal pain decreased significantly for the treatment patient group. The authors emphasized the importance of conducting an autoimmune serology panel on patients with gastroparesis symptoms in order to identify patients who would benefit from immunotherapy.
Device Therapy of Chronic Nausea and Vomiting
The study of electrical stimulation of nerves as a therapeutic treatment, also known as bioelectric neuromodulation, is being trialed in various ranges of human disease. The benefits of treatment using neuromodulation is well-known in conditions such as Parkinson’s Disease, psychiatric disease, and pain control. Emerging research is showing that similar therapies may benefit patients with gastrointestinal disorders as well. A 2018 review of the neurologic pathways and currently available neuromodulation treatments discussed the opportunity for further introductions of disease-modifying bioelectric therapy throughout the central nervous system via the vagus nerve, thoracolumbar connections, sacral nerves and organ-specific treatments.105 Studies involving gastric electrical stimulation and placement of electrodes into the muscle wall and serosal surfaces of the stomach have shown significant benefit in symptoms of gastroparesis and frequency of vomiting.106,107
Electrical Stimulation of the Stomach
Animal studies in the 1960s showed that application of electric current to isolated stomachs produced gastric contractions leading to gastric emptying.108 Around the same time, clinical studies were conducted to stimulate the human gastrointestinal tract in an attempt to treat post-operative ileus.109 While initial results were promising, later studies failed to show any effect on GI tract motility.110,111 Continued research in this area found that stimulation could improve gastric emptying and alleviate nausea and vomiting in patients with gastroparesis, using both high and low energy devices.106,112
In the various studies of GES, different patterns of waveforms have been applied. The pulse of the current varied from microseconds to a few hundred milliseconds. Likewise, the frequency varied from few cycles/min to the hertz frequency (cycles/second). Different patterns of electrical stimulation (frequency, amplitude, pulse) were found to result in different patterns of gastric myoelectric activities and clinical effects.
At least two types of GES have been studied to treat gastroparesis with others proposed or in development.
Low frequency/high energy stimulation
This form of stimulation uses long pulse duration (few hundred milliseconds) at a slower frequency of a few cycles per minute. Low frequency stimulation has been shown to normalize gastric dysrhythmias and entrain gastric slow waves and accelerate gastric emptying with minimal effects on subjective nausea and vomiting. This high energy system never received FDA approval.113
High frequency/low energy Stimulation
High frequency stimulation has demonstrated little to no effect on gastric emptying but has been shown to significantly reduce symptoms of nausea and vomiting in gastroparetic patients. This form of stimulation employs short pulse duration at a higher frequency and can be delivered either continuously or at intervals while utilizing less energy. The lower energy consumption and thus the longer battery life of this form of stimulation made it a practical choice for an implantable permanent device. The Enterra system (Medtronic) uses this form of stimulation and is the only device that is available for clinical use. It is FDA approved, albeit on a humanitarian device exemption basis, for treatment of gastroparesis refractory to maximal medical therapy. However, since approval allows for use of this device within its programmable ranges, many patients receive much higher than normal energies, and some therapies have been labelled as ‘medium energy’ as there is no current consensus on terminology for bioelectric devices.
Permanent GES
As discussed in previous sections, high-frequency/low-energy GES significantly decreases vomiting frequency and gastrointestinal symptoms in patients with severe gastroparesis. While temporary GES is placed endoscopically, insertion of the Enterra GES is placed surgically under general anesthesia via laparotomy or minimally invasive techniques. Two stimulation leads are inserted in the gastric muscularis propria along the greater curve proximal to the pylorus. These leads are connected to a neurostimulator that is placed into a subcutaneous pocket and sutured to the underlying fascia. Complications of permanent GES placement include skin erosion/wound dehiscence, device migration/flipping and although rare, perforation and erosion of the leads or intestinal obstruction.114
Since permanent GES placement requires surgery, is expensive and is not universally effective, temporary GES has been used to predict response to more permanent stimulation.115 Varying approaches have been used to access the stomach to place temporary GES stimulating leads and all require endoscopy for placement. The technique used in the U of MS study named ENDOStim employs the orogastric or nasogastric approach.116,117 The leads are placed using endoscopy in a manner similar to placing a nasojejunal tube. The tips of the electrode are embedded in the submucosa (active fixation) or on top of the mucosa (passive fixation) and in both cases held in place with endoclips. Another method of placement utilizes a previously matured PEG tract via the gastric mucosa.116 In another temporary percutaneous GES (TPGES) method, the electrodes are inserted using a method similar to placing a PEG tube but without penetrating the gastric mucosa via creation of a saline submucosal pillow. The uninsulated portion of the electrodes stimulate the muscularis propria of the gastric wall.118
Mechanism of effect of GES
While a variety of effects of GES have been thought to be responsible for the clinical effects, the exact mechanism remains unknown.119,120 The Enterra system has demonstrated improvement in symptoms of gastroparesis, however the gastric dysrhythmias remain and results on gastric emptying have been variable with some studies showing improvement and others not.121–124 A 2009 meta-analysis identified 13 studies which were suitable for inclusion.125 Of these, four studies had data on gastric emptying at two hours showing highly variable changes in the rate of gastric emptying. Five other studies showed a highly significant improvement in gastric emptying at four hours after GES and the change was strongly consistent between these studies. A recent review of patients undergoing temporary GES (tGES) showed that those patients who were delayed were accelerated by tGES and those that were non delayed in solid emptying at baseline slowed.126 Three broad possible classes of mechanisms may be involved; local enteric, central and autonomic.115 A combination of these and perhaps other effects may be responsible for the clinical effect. A recent study listed 16 potential specific mechanisms and further studies are underway.127
Results of Enterra System
Multiple studies have looked at the efficacy of Enterra system and all have consistently shown a beneficial effect on symptoms of nausea, vomiting and quality of life, in patients with gastroparesis and in those with N/V attributed to other causes.
Outcomes of patients at three US centers implanted with the Enterra system for drug refractory gastroparesis were reviewed. Patients were followed for a median 4 years and found to have a significant improvement in vomiting frequency score (VFS), total gastrointestinal symptom score (TSS), and a Medicare derived HRQOL measure (IDIOMS) before and after gastric electrical stimulation (GES).128 Another study reported single center outcomes of the Enterra system for up to 8 years after placement.129 Total Symptom Score comprising of functional (nausea, vomiting, early satiety, bloating and postprandial fullness) and pain (chest pain or burning, epigastric pain or burning) symptoms were available at one year and also at four to eight years. All of these symptoms were significantly improved at all times during the study. Although GES has been shown to significantly improve refractory nausea and vomiting in patients with or without gastroparesis, it does not improve gastric emptying.130
Gastric Electric Stimulation (GES) has also been found to be effective in nausea and vomiting of non-gastroparesis etiology. A study of GES in patients with intractable nausea and vomiting but with normal gastric emptying showed significant improvement in nausea, vomiting and quality of life as well as other symptoms like abdominal pain, regurgitation and appetite.131 Andersson et. al. studied the outcomes of temporary percutaneously placed GES in patients with diverse causes of nausea and vomiting ranging from functional dyspepsia to chronic intestinal pseudo obstruction irrespective of gastric emptying (nonconventional indications for GES). All patients had symptoms refractory to maximal medical management. 81% of the patients had at least a 50% reduction in the main symptoms of nausea or vomiting. Responders were then selected for permanent GES and 91% had significant improvement in symptoms at 6 months and at time of last follow up. (Mean time, 21 months, range 6 to 48 months).118 Thus, the efficacy of the Enterra System is not limited to patients to gastroparesis only and is also durable. GES has recently been shown, in a small pilot study, to be effective in malignancy related gastroparesis (MAG)132 and for patients with the symptoms of gastroparesis who have co-existent inflammatory bowel disease.133
Other Interventional Therapies for Nausea and Vomiting
There are a few studies which have studied electrocranial stimulation in healthy volunteers as a method to reduce nausea. Most of these studies are focused on the vestibular system/motion sickness but are suggestive that electrical stimulation to the left parietal cortex can delay the onset of nausea symptoms (increased time to develop symptoms), as well as increase the speed of recovery from nausea episodes.134 Recent studies also suggest that transcortical electrical stimulation can decrease the sensitivity to developing nausea, and therefore could be useful in other types of nausea and vomiting as well.
One of the hypothesized mechanisms of gastric electrical stimulation is through a central vagus nerve stimulation.135 Prior methods of vagus nerve stimulation have required invasive therapy, including gastric stimulator placement or surgical intervention. Recent studies have looked at non-invasive vagus nerve stimulation (nVNS) as an alternative to eliminate the safety risks of GES or surgical intervention. A recent open-label pilot study assessed nVNS in patients with mild to moderate idiopathic gastroparesis. Patients self-administered a non-invasive vagal nerve stimulator for 4 weeks and were found to have improvement in gastroparesis cardinal symptom index as well as reduction in gastric emptying.136
Surgical and Endoscopic Therapies for Nausea and Vomiting.
For patients with nausea and vomiting secondary to refractory gastroparesis several endoscopic and surgical treatment options exist. As many of these procedures carry inherent risks and complications, invasive therapy is reserved for patients with unmanageable symptoms who remain symptomatic despite treatment interventions with dietary and lifestyle management, antiemetic and prokinetic agents. These include permanent gastric electric stimulation, endoscopic botulinum toxin injection, gastric peroral endoscopic pyloromyotomy (G-POEM), laparoscopic pyloroplasty (LP), and gastrostomy and jejunostomy tube Placement. All of these are reviewed below.
Endoscopic Botulinum Toxin Injection
Endoscopic intrasphincteric injection of the pylorus with botulinum toxin-A (BT-A) decreases smooth muscle contractions induced by acetylcholine. By decreasing pyloric contraction, BT-A enhances gastric emptying providing symptomatic relief. Botulinum toxin injection was previously widely used as many open label trials have reported intrapyloric BT-A injection to be useful in symptomatic management. However, a 2008 randomized, double-blind, placebo-controlled trial did not show superiority in symptomatic improvement compared to placebo.137 Skill of the endoscopist and risk of misplaced injections must also be taken into consideration when determining effectiveness.
Functional luminal imaging probe (FLIP) technology uses balloon-based impedance planimetry to measure the cross-sectional area and pressure of segments of the GI tract, which allows for calculation of distensibility. It was originally used for esophageal measurements but has more recently been used to assess the relationship between pyloric pathophysiology and gastroparesis. A 2015 study using FLIP in patients with gastroparesis showed that early satiety and postprandial fullness were inversely correlated with diameter and cross-sectional area of the pyloric sphincter.138 Desprez et al. used this technology to study the effects of intrasphincteric botulinum injection in patients with gastroparesis, all whom had FLI measurements prior to injection. They found that patients with impaired pyloric compliance had decreased total symptom score at 3 months compared with patients with normal pyloric distensibility.139 This may provide information in the future regarding what patients may benefit from intrapyloric BT-A injection for gastroparesis symptoms in the future.
Gastric Peroral Endoscopic Pyloromyotomy (G-POEM)
G-POEM, also known as per oral endoscopic pyloromyotomy (POP), is a novel and minimally invasive treatment option emerging as a feasible option for treatment of refractory gastroparesis. Although new, with the first procedure performed in 2013, early results on therapeutic benefit and safety profile have been promising. This endoscopic submucosal tunneling technique involves myotomy of the inner circular and oblique muscle bundles 2–5 cm proximal to the pylorus on the greater curvature of the stomach extending into the duodenal bulb followed by full thickness pyloromyotomy.140 A 2018 retrospective single-center study of patients with refractory gastroparesis who underwent G-POEM showed technical success in 100% of the patients and long-term clinical response at 14.5 months in 81% of patients. There was significant reduction in the Gastroparesis Cardinal Symptom Index (GCSI) as well as gastric emptying scintigraphy.141 As this was a small study, involving only 16 patients, caution must be taken when extrapolating information and larger reviews are necessary.
Laparoscopic Pyloroplasty
Laparoscopic pyloroplasty (LP) is a minimally invasive surgery which involves making an incision extending from the gastric antrum to the duodenum, widening the pyloric opening. Recent studies have shown that LP improved or normalized gastric emptying in nearly 90% of patients with low morbidity.142 There were significant improvements in nausea, vomiting, bloating as well as abdominal pain. LP and G-POEM have similar, significant rates of improvement in GCSI score and objective gastric emptying. However, LP is associated with longer average length of hospital stay, operative time, estimated blood loss and more post-operative complications such as surgical site infection and unplanned ICU admission when compared with G-POEM.143 More head to head data regarding the long term benefits vs risks of the two procedures is needed.
Combination GES and Pyloric Therapy
Gastric electrical stimulation is thought to benefit patients with gastroparesis in part through vagus nerve stimulation which inhibits the chemo-receptor trigger zone in the hypothalamus. Pyloric surgical intervention, on the other hand, has a more pronounced effect on gastric emptying. Combination of GES and pyloroplasty has been shown to improve gastric emptying and gastroparesis symptoms in drug refractory gastroparesis.144 Comparisons of clinical outcomes of gastric electrical stimulation, pyloric surgery (PS) or a combination of the two in patients with refractory gastroparesis has shown mixed results. Some studies have shown that GES and combination of GES + PS significantly improves nausea and vomiting compared to PS alone.145 However, others have found that combination of GES + PS does not offer clinically significant advantage over GES or PS alone.146
Gastrostomy and Jejunostomy Tube Placement
Percutaneous insertion of gastrostomy tube (G-tube) through the abdominal wall is a common procedure performed safely with endoscope-assisted transillumination. Although G-tube or jejunostomy tube (J-tube) placement does not treat the underlying disorder causing N/V they play important roles in improving quality of life.147 G-tube may allow for decompression of gastric contents which allows prevention of frequent vomiting. J-tube placement can be performed percutaneously (similar to G-tubes), laparoscopically or surgically via laparotomy. J-tubes are inserted directly into the small intestine and allow for enteral nutrition to provide adequate caloric intake for patients unable to maintain nutrition with peroral intake. An additional aspect of enteral tube placement is that in some cases full thickness GI biopsies, for neuro-muscular analysis, can be obtained.148
Complementary and Alternative Therapies in Nausea and Vomiting
Complementary and alternative medical therapies (CAM) are increasingly being used by patients for a variety of conditions including nausea and vomiting. These may be for refractory symptoms or by patients who wish to avoid allopathic treatment. CAM therapies for nausea and vomiting may include use of herbs, behavioral therapies including hypnosis and acupuncture and acupressure. While details of these therapies are beyond the scope of this review, a summary of some of the important interventions is presented.
Ginger
Ginger has been studied for the treatment of nausea and vomiting resulting from various conditions including motion sickness, PONV, CINV and N/V associated with pregnancy.149 The antiemetic effects of ginger in N/V is mediated by its constituent chemicals gingerol, shogaol, and zingerone, which act through serotonin and NK1 receptors in the central and peripheral pathways of N/V.150,151 Ginger also has an intestinal antispasmodic and gastric prokinetic effect increasing gastroduodenal motility as well as gastric emptying.152–155 It has also been shown to have antiarrhythmic effects in the stomach.156,157
Clinical studies of ginger for the treatment of nausea and/or vomiting have produced conflicting results. In functional dyspepsia, though physiological effects (gastric emptying and antral contractions) were seen, there was no significant symptom improvement. Studies in motion sickness have also yielded conflicting results with one study showing no benefit and another showing delay in nausea onset which was less severe.156,158 In nausea and vomiting of pregnancy and hyperemesis gravidarum, systematic reviews of studies have found that ginger may yield a small beneficial effect over placebo.159,160 Ginger has also been studied in CINV. A double-blind multicenter trial in which patients were randomized to receive either different doses of standardized ginger constituents or placebo found that all doses of ginger significantly reduced the incidence of acute, but not delayed, nausea.161
Another systematic review of randomized controlled trials and crossover trials found seven studies that met the inclusion criteria.162 Five of these studies used ginger along with standard anti CINV antiemetics and two used ginger as a stand-alone therapy. Three of these studies showed a favorable effect, and two showed no effect on measures of CINV. Two studies were also favorable, but the authors indicated the caveat that due to lack of a placebo group the significance was difficult to determine. Studies of the efficacy of ginger in PONV, have shown inconsistent findings.163
Acupuncture and Electro-acupuncture
Acupuncture is a part of Traditional Chinese Medicine (TCM) system and is believed to have arisen in 100 BC. Acupuncture embraces the ancient Chinese philosophy of health and disease is based on the concept of balance between the Yin and Yang energies. Disease is believed to occur when there is an imbalance in these energies and treatment is directed at bringing back this balance by stimulating energy centers called meridians. Despite its popularity and persistence, scientific evidence supporting its efficacy is lacking.
Acupuncture is performed by inserting thin needles at various condition-specific locations known as meridians. For nausea and vomiting these are commonly directed at the P6 center and the auricular center. Acupuncture may also be performed by the application of electric currents between pairs of acupuncture needles (electro-acupuncture). Acupressure, also known as shiatsu, is the application of pressure to specific points but without the use of needles or puncturing of skin involved in acupuncture.https://en.wikipedia.org/wiki/Acupressure
While scientific studies on the benefits of acupuncture have provided inconsistent results, a Cochrane review found it may be useful in CINV and PONV.164–166 The Cochrane review of acupuncture in PONV was most recently updated in 2015.167 This review included 59 trials and found that compared to placebo, PC6 stimulation significantly reduced the incidence of nausea, vomiting and the need for rescue antiemetics. However due to the high level of heterogeneity among trials the quality if evidence was rated as low. When PC6 acupoint stimulation was compared to antiemetic drugs there was no difference in the incidence of nausea, vomiting or the need for rescue antiemetics. The quality of evidence was rated as moderate. When compared to antiemetic medicines, the combination of acupuncture and medications was found to reduce the incidence of vomiting but not nausea. The quality of evidence was rated as very low.
Acupuncture (including acupressure and electroacupuncture) has been explored as an adjunctive therapy in multiple studies in CINV. An updated systematic review of integrative therapies in breast cancer patients recommended acupressure and electroacupuncture as a grade B recommendation, i.e. high certainty that the net benefit is moderate or there is moderate certainty that the net benefit is moderate to substantial.168 Acupressure therapy was found to produce significant decreases in nausea, retching, and vomiting (P < .05) in a meta-analysis across three randomized control trials.
Another systematic review of one quasi-experimental and nine randomized clinical trials, which included two specific acupressure modalities (acupressure band and finger acupressure) in different kinds of cancer concluded that acupressure was strongly suggestive to be effective in controlling acute and delayed nausea and vomiting.169
Acupuncture and acupressure have been explored in gastroparesis patients. A systematic review of randomized controlled trials (RCTs) evaluated the efficacy of acupuncture in improving dyspeptic symptoms and gastric emptying in diabetic gastroparesis (DGP).170 While this review found that acupuncture might be effective to improve dyspeptic symptoms in DGP, a definite conclusion could not be made due to the low quality of trials and possibility of publication bias.
A crossover blinded study investigated the effects of chronic electrical stimulation at acupuncture points in dyspeptic symptoms in DGP patients. Patients were blindly treated at home with 4-week ES and 4-week sham-ES in a randomized order. 4-wk ES, not sham-ES, significantly improved nausea, vomiting, abdominal fullness, bloating and retching.4-week ES, not sham-ES, increased percentage of normal slow waves in both fasting and fed states.171
A study looked at central and peripheral effects of needleless transcutaneous electrical acupuncture (TEA) treatment for nausea in patients with diabetic gastroparesis (DGP).172 Electroencephalography (EEG) and electrogastrography (EGG) recordings were used to investigate the central and peripheral responses of TEA. The severity of nausea was compared at baseline, during visual stimulation (VS) to provoke nausea, during active VS together with TEA, and TEA alone. TEA was found to improve gastric dysrhythmia and ameliorate nausea. TEA treatment of nausea provoked by VS was found to cause change of dominance from right to left inferior frontal lobe activity.
Several recent studies have demonstrated the effectiveness of nerve electrical stimulation (NES) for treating CINV. A 2018 randomized controlled trial evaluated the effectiveness of NES for the treatment of CINV in patients with advanced gastric cancer.173 Patients were divided equally between the NES group and the sham group. Gel pads were placed at bilateral acupoints for 30 minutes daily for 1 week. In the treatment group, electrical stimulation was applied to these points while the sham group did not receive electrical stimulation. Patients in the NES group reduced nausea, vomiting and improved appetite compared to sham group, but there was no significant difference in quality of life and functional impairment. Future studies are still needed to assess the long-term efficacy and safety of NES treatment for the treatment of CINV.
Behavioral Therapy
A few studies have explored behavioral therapy in the treatment of nausea and vomiting.
A study of bone marrow transplant patients randomly assigned them to either hypnosis training, cognitive behavioral therapy (CBT), therapist contact control (TC) or control prior to beginning transplantation conditioning. It was found that nausea, emesis and opioid use did not differ significantly between the treatment groups.174 Another study explored the effect of music therapy and visual imagery on chemotherapy-induced anxiety and nausea-vomiting.175 Patients receiving chemotherapy received training in guided visual imagery consisting of viewing five nature paintings and listening to music between their second and third rounds of chemotherapy. Music therapy and visual imagery was found to reduce the severity and duration of chemotherapy-induced nausea and vomiting significantly (p < 0·05).
Another study applied autonomic training (AT) with directed imagery (verbal instructions) to patients with chronic nausea and vomiting. After treatment, gastrointestinal symptoms decreased by >30% in 58% of the treated patients. It was found that baseline measures of gastric emptying and autonomic function predicted treatment outcome.176
Conclusions:
Nausea and vomiting are common conditions seen in ambulatory and hospital environments that can lead to significant decline in patient’s quality of life and increased cost of medical care from emergency visits and repeated hospitalizations. This comprehensive review has discussed the pathophysiology of nausea and vomiting, pharmacotherapy, surgical interventions, bioelectric neuromodulatory techniques (including gastric electrical stimulation), behavioral and alternative and complimentary medicine treatments. Improved understandings of pathophysiology of nausea and vomiting and future developments are needed to develop optimal therapies.
Table 1-.
Drug Classes and mechanism of action
| Drug Class | Mechanism of Action | Drug Names in this class | Adverse Effects |
|---|---|---|---|
| Dopamine receptor antagonist |
|
Metoclopramine, Domperidone, Haloperidol, CIN-102, Metopimazine | Extrapyramidal symptoms (black box warning for tardive dyskinesia), QT prolongation, hyperprolactinemia |
| 5-HT-3 receptor antagonist |
|
Ondansetron, other ‘setrons | QT prolongation (dose dependent), headache, constipation, serotonin syndrome |
| 5-HT-4 receptor agonist |
|
Cisapride, Velusetrag, Tegaserod, Prucalopride | QT prolongation (Cisapride), headache, abd pain, diarrhea. Previously withdrawn due to increased risk of heart attack or stroke (Tegaserod) |
| Histamine receptor antagonist |
|
Promethazine, Prochlorperazine, Cyclizine, Meclizine, Dimenhydrinate, Scopolamine Doxylamine (in combination with pyridoxine) | Anticholinergic effects, sedation |
| NK1 Receptor antagonist |
|
Aprepitant, Tradipitant | Headache, constipation, diarrhea, hiccups; inducer of CYP3A4 |
| Ghrelin agonist |
|
Relamorelin | Hyperglycemia, LFT elevation, diarrhea |
| Motilin Agonist |
|
Erythromycin, Azithryomycin, Camicinal | Risk of antibiotic resistance (Erythromycin, Azithryomycin), tachyphylaxis, QT prolongation (Erythromycin), drug interactions due to CYP450 3A4 inhibition |
| Tetrahydrobiopterin |
|
Sapropterin | Headache, runny nose, diarrhea |
| Tricyclic Antidepressants |
|
Nortriptyline, Amitriptyline, Imipramine, Desipramine, Doxepin | Anticholinergic effects, sedation, QT prolongation, cardiac arrhythmia |
Table 2-.
Individual Drugs, Effects, Route of Administration and Adverse Effects
| Drug Name | Mechanism of Action | Drug Effects | Route of administration | Adverse effects |
|---|---|---|---|---|
| Metoclopramide | Dopamine receptor antagonist (high dose), and 5-HT4 receptor agonist |
|
Oral, IV, IM | Extrapyramidal symptoms (black box warning for tardive dyskinesia) |
| Domperidone | Dopamine D2 and D3 receptor antagonist |
|
Oral, IM, rectal | QT prolongation, hyperprolactinemia (breast and menstrual symptoms), dry mouth, diarrhea |
| Haloperidol (Haldol) | Dopamine receptor antagonist, acts on numerous other serotonin receptors |
|
Oral, IM, IV | Extrapyramidal side effects, anticholinergic side effects, somnolence, QT prolongation |
| CIN-102 | Dopamine receptor antagonist (D2/D3) |
|
Oral | Under investigation |
| Metopimazine (NG101) | Dopamine receptor antagonist (D2/D3) |
|
Oral | Under investigation |
| Promethazine (Phenergan) | Histamine receptor antagonist + antimuscarinic |
|
Oral, IV, IM, rectal | Anticholinergic side effects, drowsiness |
| Prochlorperazine (Compazine) | D2 receptor antagonist |
|
Oral, IV, IM, rectal | Agitation, insomnia, anticholinergic effects, constipation |
| Cyclizine | Histamine receptor antagonist + antimuscarinic |
|
Oral, IV, IM | Drowsiness, xerostomia, headache, nausea urinary retention |
| Meclizine | Histamine receptor antagonist + antimuscarinic |
|
Oral | Drowsiness, blurred vision, dry mouth, urinary retentioni |
| Scopolamine | Antimuscarinic |
|
Oral, skin patch, IV, IM, rectal | Anticholinergic side effects, drowsiness, tachycardia |
| Trimethobenzamide | Unknown |
|
Oral, IM | Diarrhea; CNS effects including coma, disorientation, seizure, extrapyramidal effects |
| Ondansetron (Zofran) | 5-HT3 receptor antagonist |
|
Oral, IV, IM, rectal | headache, fatigue, constipation, QT prolongation |
| Other -setrons | 5-HT3 receptor antagonist |
|
Oral, IV, IM, rectal, transdermal | Headache, constipation, diarrhea, drowsiness, asthenia |
| Cisapride | 5-HT4 receptor agonist |
|
Oral | QT prolongation, cardiac arrhythmia, sudden cardiac death |
| Velusetrag | 5-HT4 receptor agonist |
|
Oral | Headache, diarrhea, nausea |
| Prucalopride (Motegrity) | 5-HT4 receptor agonist |
|
Oral | Headache, diarrhea, nausea, dizziness, abdominal distension |
| Tegaserod (Zelnorm) | 5-HT4 receptor partial agonist |
|
Oral | Headache, abdominal pain, nausea, diarrhea, flatulence, dizziness |
| Aprepitant (Emend) | NK1 receptor antagonist |
|
Oral | Headache, constipation, diarrhea, hiccups, dizziness, |
| Tradipitant | NK1 receptor antagonist |
|
Oral | Somnolence, diarrhea, fatigue |
| Sapropterin (Kuvan) | BH4 |
|
Oral | Rhinorrhea, headache, diarrhea, cough, nausea |
| CNSA-001 (Sepiapterin) | BH4 precursor |
|
Oral | |
| Relamorelin | Ghrelin agonist |
|
Subcutaneous | Hyperglycemia, DKA, LFT elevation, diarrhea, nausea |
| Erythromycin | Motilin Receptor Agonist |
|
Oral, IV | Tachyphylaxis, antibiotic resistance, QT prolongation, drug interactions due to CYP450 3A4 inhibition |
| Camicinal | Motilin Receptor Agonist |
|
Oral | Headache, flatulence, vomiting, constipation, decreased blood glucose |
| Nortriptyline | Serotonin and Norepinephrine Reuptake Inhibitor; Histamine and Muscarinic Antagonist |
|
Oral | Anticholinergic effects, sedation, QT prolongation, cardiac arrhythmia |
| Amitriptyline | Serotonin and Norepinephrine Reuptake Inhibitor; Histamine and Muscarinic Antagonist |
|
Oral, IM | Anticholinergic effects, sedation, QT prolongation, cardiac arrhythmia |
Table 3-.
Surgical and Endoscopic Treatment Options
| Procedure | Procedure Description | Mechanism | Risks |
|---|---|---|---|
| Permanent GES Placement | Surgical insertion of 2 stimulation leads in gastric muscle connected to a neurostimulator placed into a subcutaneous pocket |
|
|
| Laparoscopic Pyloroplasty | Minimally invasive surgical incision extending from the gastric antrum to the duodenum widening the pyloric opening |
|
|
| Gastric Peroral Endoscopic Myotomy (G-POEM) | Endoscopic submucosal tunneling from gastric antrum into the duodenal bulb followed by full thickness pyloromyotomy, widening the pyloric opening |
|
|
| Combination GES and Pyloric Therapy | Combination of insertion of gastric electric stimulator as well as pyloric surgical intervention as above |
|
|
| Endoscopic Botulinum Toxin Injection | Endoscopic intrapyloric injection of botulinum toxin-A (BT-A) |
|
|
| Gastrostomy Tube Placement | Percutaneous insertion through the abdominal wall into the stomach via endoscope-assisted transillumination (Can be done endoscopically or surgically) |
|
|
| Jejunostomy Tube Placement | Percutaneous insertion through the abdominal wall into the small intestine via endoscope-assisted transillumination (Can be done endoscopically or surgically) |
|
|
Table 4-.
Complementary and Alternative Therapies
| Treatment | Mechanism | Therapeutic Effects | Risks and Side Effects |
|---|---|---|---|
| Acupuncture and electro-puncture. |
|
Reduction of swelling, pain, and improvement in peripheral blood flow. Demonstrated benefit in post-operative nausea and vomiting with treatment applied to the P6 meridian. |
|
| Acupressure (Shiatsu) |
|
Similar to acupuncture | Pain and bruising at site of application. Less common side effects include dizziness, fainting, nerve damage, and rarely, organ damage. |
| Ginger | Inhibitory effects of 6-shogaol, 6-gingerol, and zingerone (metabolic by-products of ginger) of the 5-HT3 receptors and human gut enteric neurons | Reduction of nausea and vomiting. May have synergistic anti-emetic effects in combination with other 5-HT antagonists. | mild gastrointestinal complications including pyrosis (heartburn or reflux) and eructation (belching) |
Acknowledgments:
The authors would like to thank Catherine McBride for manuscript preparation.
Financial support for this work: none
Footnotes
Disclosures:
Dr. Heckroth - None
Dr. Luckett - None
Dr. Moser - None
Dr. Parajuli – None
Dr. Abell
Main funding: NIH GpCRC.
Investigator: Allergan, Vanda, Censa, Cin-dome
Consultant: Censa, Nuvaira, Takeda
Speaker: Takeda, Medtronic
Editorial:
GI writer-Medstudy
GI-Neuromodulation
GES-Wikistim
Reviewer: UpToDate
Other: Founder of ADEPT-GI: Holder of IP from the University of Mississippi on gastric electrical stimulation and on autonomic & enteric predications of medical conditions.
Contributor Information
Matthew Heckroth, Department of Medicine, University of Louisville, Louisville, KY, USA..
R. Tyler Luckett, Division of Gastroenterology, Hepatology & Nutrition, Department of Medicine, University of Louisville, Louisville, KY, USA..
Chris Moser, Department of Medicine, University of Louisville, Louisville, KY, USA..
Dipendra Parajuli, Division of Gastroenterology, Hepatology & Nutrition, Department of Medicine, University of Louisville, Louisville, KY, USA.; Robley Rex VAMC, Louisville, KY, USA.
Thomas L. Abell, Professor of Medicine, Arthur M Schoen MD Chair in Gastroenterology, Division of Gastroenterology, Hepatology & Nutrition, Department of Medicine, University of Louisville, Louisville, KY, USA.
References
- 1.Pasricha PJ, Colvin R, Yates K, et al. Characteristics of Patients With Chronic Unexplained Nausea and Vomiting and Normal Gastric Emptying. Clin Gastroenterol Hepatol. Published online 2011. doi: 10.1016/j.cgh.2011.03.003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Warr DG, Hesketh PJ, Gralla RJ, et al. Efficacy and tolerability of aprepitant for the prevention of chemotherapy-induced nausea and vomiting in patients with breast cancer after moderately emetogenic chemotherapy. J Clin Oncol. Published online 2005. doi: 10.1200/JCO.2005.09.050 [DOI] [PubMed] [Google Scholar]
- 3.Roila F, Molassiotis A, Herrstedt J, et al. 2016 MASCC and ESMO guideline update for the prevention of chemotherapy- and radiotherapy-induced nausea and vomiting and of nausea and vomiting in advanced cancer patients. Ann Oncol. Published online 2016. doi: 10.1093/annonc/mdw270 [DOI] [PubMed] [Google Scholar]
- 4.Sanger GJ, Andrews PLR. Treatment of nausea and vomiting: Gaps in our knowledge. Auton Neurosci Basic Clin. Published online 2006. doi: 10.1016/j.autneu.2006.07.009 [DOI] [PubMed] [Google Scholar]
- 5.Foubert J, Vaessen G. Nausea: The neglected symptom? Eur J Oncol Nurs. Published online 2005. doi: 10.1016/j.ejon.2004.03.006 [DOI] [PubMed] [Google Scholar]
- 6.Guyton Khonsary S. and Hall: Textbook of Medical Physiology. Surg Neurol Int. Published online 2017. doi: 10.4103/sni.sni_327_17 [DOI] [Google Scholar]
- 7.Abell TL, Parajuli D. Nausea and vomiting related to autonomic nervous system disorders. In: Nausea and Vomiting: Diagnosis and Treatment. ; 2016. doi: 10.1007/978-3-319-34076-0_7 [DOI] [Google Scholar]
- 8.Gershon MD. Roles played by 5-hydroxytryptamine in the physiology of the bowel. In: Alimentary Pharmacology and Therapeutics, Supplement. ; 1999. doi: 10.1046/j.1365-2036.1999.00002.x-i2 [DOI] [PubMed] [Google Scholar]
- 9.Racké K, Reimann A, Schwörer H, Kilbinger H. Regulation of 5-HT release from enterochromaffin cells. Behav Brain Res. Published online 1995. doi: 10.1016/0166-4328(96)00075-7 [DOI] [PubMed] [Google Scholar]
- 10.Abell TL, Kedar A, Stocker A, et al. Pathophysiology of Gastroparesis Syndromes Includes Anatomic and Physiologic Abnormalities. Dig Dis Sci. Published online 2020. doi: 10.1007/s10620-020-06259-6 [DOI] [PubMed] [Google Scholar]
- 11.Roila F, Herrstedt J, Aapro M, et al. Guideline update for MASCC and ESMO in the prevention of chemotherapy-and radiotherapy-induced nausea and vomiting: Results of the Perugia consensus conference. Ann Oncol. Published online 2010. doi: 10.1093/annonc/mdq194 [DOI] [PubMed] [Google Scholar]
- 12.O’Brien BJ, Rusthoven J, Rocchi A, et al. Impact of chemotherapy-associated nausea and vomiting on patients’ functional status and on costs: Survey of five Canadian centres. CMAJ. Published online 1993. [PMC free article] [PubMed] [Google Scholar]
- 13.Osoba D, Zee B, Warr D, Latreille J, Kaizer L, Pater J. Effect of postchemotherapy nausea and vomiting on health-related quality of life. Support Care Cancer. Published online 1997. doi: 10.1007/s005200050078 [DOI] [PubMed] [Google Scholar]
- 14.Wood GJ, Shega JW, Lynch B, Von Roenn JH. Management of intractable nausea and vomiting in patients at the end of life: “I was feeling nauseous all of the time… nothing was working.” J Am Med Assoc. Published online 2007. doi: 10.1001/jama.298.10.1196 [DOI] [PubMed] [Google Scholar]
- 15.Talley NJ. What Causes Functional Gastrointestinal Disorders? A Proposed Disease Model. Am J Gastroenterol. Published online 2020. doi: 10.14309/ajg.0000000000000485 [DOI] [PubMed] [Google Scholar]
- 16.Nguyen L, Wilson LA, Miriel L, et al. Autonomic function in gastroparesis and chronic unexplained nausea and vomiting: Relationship with etiology, gastric emptying, and symptom severity. Neurogastroenterol Motil. Published online 2020. doi: 10.1111/nmo.13810 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Sandroni P, Opfer-Gehrking TL, McPhee BR, Low PA. Postural tachycardia syndrome: Clinical features and follow-up study. Mayo Clin Proc. Published online 1999. doi: 10.4065/74.11.1106 [DOI] [PubMed] [Google Scholar]
- 18.Schondorf R, Low PA. Idiopathic postural orthostatic tachycardia syndrome: An attenuated form of acute pandysautonomia? Neurology. Published online 1993. doi: 10.1212/wnl.43.1_part_1.132 [DOI] [PubMed] [Google Scholar]
- 19.Weimer LH, Williams O. Syncope and orthostatic intolerance. Med Clin North Am. Published online 2003. doi: 10.1016/S0025-7125(03)00007-5 [DOI] [PubMed] [Google Scholar]
- 20.Sullivan SD, Hanauer J, Rowe PC, Barron DF, Darbari A, Oliva-Hemker M. Gastrointestinal symptoms associated with orthostatic intolerance. J Pediatr Gastroenterol Nutr. Published online 2005. doi: 10.1097/01.MPG.0000157914.40088.31 [DOI] [PubMed] [Google Scholar]
- 21.Camilleri M, Bharucha AE. Gastrointestinal dysfunction in neurologic disease. Semin Neurol. Published online 1996. doi: 10.1055/s-2008-1040977 [DOI] [PubMed] [Google Scholar]
- 22.Hammam E, Dawood T, Macefield VG. Low-frequency galvanic vestibular stimulation evokes two peaks of modulation in skin sympathetic nerve activity. Exp Brain Res. Published online 2012. doi: 10.1007/s00221-012-3090-z [DOI] [PubMed] [Google Scholar]
- 23.Himi N, Koga T, Nakamura E, Kobashi M, Yamane M, Tsujioka K. Differences in autonomic responses between subjects with and without nausea while watching an irregularly oscillating video. Auton Neurosci Basic Clin. Published online 2004. doi: 10.1016/j.autneu.2004.08.008 [DOI] [PubMed] [Google Scholar]
- 24.Morrow GR, Hickok JT, Dubeshter B, Lipshultz SE. Changes in clinical measures of autonomic nervous system function related to cancer chemotherapy-induced nausea. J Auton Nerv Syst. Published online 1999. doi: 10.1016/S0165-1838(99)00053-3 [DOI] [PubMed] [Google Scholar]
- 25.Morrow GR. The effect of a susceptibility to motion sickness on the side effects of cancer chemotherapy. Cancer. Published online 1985. doi: 10.1002/1097-0142(19850615)55:12<2766::AID-CNCR2820551207>3.0.CO;2-7 [DOI] [PubMed] [Google Scholar]
- 26.Chelimsky G, Boyle JT, Tusing L, Chelimsky TC. Autonomic abnormalities in children with functional abdominal pain: Coincidence or etiology? J Pediatr Gastroenterol Nutr. Published online 2001. doi: 10.1097/00005176-200107000-00008 [DOI] [PubMed] [Google Scholar]
- 27.Alshekhlee A, Guerch M, Ridha F, Mcneeley K, Chelimsky TC. Postural tachycardia syndrome with asystole on head-up tilt. Clin Auton Res. Published online 2008. doi: 10.1007/s10286-007-0445-9 [DOI] [PubMed] [Google Scholar]
- 28.Hejazi RA, Lavenbarg TH, Pasnoor M, et al. Autonomic nerve function in adult patients with cyclic vomiting syndrome. Neurogastroenterol Motil. Published online 2011. doi: 10.1111/j.1365-2982.2011.01679.x [DOI] [PubMed] [Google Scholar]
- 29.Aslam N, Kedar A, Nagarajarao HS, et al. Serum Catecholamines and Dysautonomia in Diabetic Gastroparesis and Liver Cirrhosis. Am J Med Sci. Published online 2015. doi: 10.1097/MAJ.0000000000000523 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Stocker A, Abell TL, Rashed H, Kedar A, Boatright B, Chen J. Autonomic Evaluation of Patients With Gastroparesis and Neurostimulation: Comparisons of Direct/Systemic and Indirect/Cardiac Measures. Gastroenterol Res. Published online 2016. doi: 10.14740/gr667w [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Oubre B, Al-Juburi A, Rashed HM, Abell TL. Evaluation of autonomic and enteric nervous system may affect the outcome of therapy in patients with GI motility disorders. Gastroenterology. Published online 2003. doi: 10.1016/s0016-5085(03)82567-2 [DOI] [Google Scholar]
- 32.Daboul I, Taleb N, Rashed HM, Alkheshen MM, Abell TL. Evaluation of autonomic and enteric measures can affect clinical care of patients with GI motility disorders. Gastroenterology. Published online 2000. doi: 10.1016/s0016-5085(00)80126-2 [DOI] [Google Scholar]
- 33.Hyde TM, Knable MB, Murray AM. Distribution of dopamine D1-D4 receptor subtypes in human dorsal vagal complex. Synapse. Published online 1996. doi: 10.1002/(SICI)1098-2396(199611)24:3<224::AID-SYN4>3.0.CO;2-G [DOI] [PubMed] [Google Scholar]
- 34.Mitchelson F Pharmacological Agents Affecting Emesis: A Review (Part I). Drugs. Published online 1992. doi: 10.2165/00003495-199243030-00002 [DOI] [PubMed] [Google Scholar]
- 35.Valenzuela JE, Dooley CP. Dopamine antagonists in the upper gastrointestinal tract. Scand J Gastroenterol Suppl. Published online 1984. [PubMed] [Google Scholar]
- 36.McCallum RW, Valenzuela G, Polepalle S, Spyker D. Subcutaneous metoclopramide in the treatment of symptomatic gastroparesis: Clinical efficacy and pharmacokinetics. J Pharmacol Exp Ther. Published online 1991. [PubMed] [Google Scholar]
- 37.Parkman HP, Carlson MR, Gonyer D. Metoclopramide nasal spray is effective in symptoms of gastroparesis in diabetics compared to conventional oral tablet. Neurogastroenterol Motil. Published online 2014. doi: 10.1111/nmo.12296 [DOI] [PubMed] [Google Scholar]
- 38.Parkman HP, Carlson MR, Gonyer D. Metoclopramide nasal spray reduces symptoms of gastroparesis in women, but not men, with diabetes: Results of a phase 2b randomized study. Clin Gastroenterol Hepatol. Published online 2015. doi: 10.1016/j.cgh.2014.12.030 [DOI] [PubMed] [Google Scholar]
- 39.Patterson D, Abell T, Rothstein R, Koch K, Barnett J. A Double-Blind Multicenter Comparison of Domperidone and Metoclopramide in The Treatment of Diabetic Patients With Symptoms of Gastroparesis Fig. 1. Am J Gastroenterol. Published online 1999. doi: 10.1111/j.1572-0241.1999.00456.x [DOI] [PubMed] [Google Scholar]
- 40.Rossi M, Giorgi G. Domperidone and Long QT Syndrome. Curr Drug Saf. Published online 2010. doi: 10.2174/157488610791698334 [DOI] [PubMed] [Google Scholar]
- 41.Biewenga J, Keung C, Solanki B, et al. Absence of QTc prolongation with domperidone: A randomized, double-blind, placebo- and positive-controlled thorough QT/QTc study in healthy volunteers. Clin Pharmacol Drug Dev. Published online 2015. doi: 10.1002/cpdd.126 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Ortiz A, Cooper CJ, Alvarez A, Gomez Y, Sarosiek I, McCallum RW. Cardiovascular safety profile and clinical experience with high-dose domperidone therapy for nausea and vomiting. In: American Journal of the Medical Sciences. ; 2015. doi: 10.1097/MAJ.0000000000000439 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Marzi M, Weitz D, Avila A, Molina G, Caraballo L, Piskulic L. Cardiac adverse effects of domperidone in adult patients: A systematic review. Rev Med Chil. Published online 2015. doi: 10.4067/S0034-98872015000100002 [DOI] [PubMed] [Google Scholar]
- 44.Hill C, Nicot P, Piette C, Le Gleut K, Durand G, Toussaint B. Estimating the number of sudden cardiac deaths attributable to the use of domperidone in France. Pharmacoepidemiol Drug Saf. Published online 2015. doi: 10.1002/pds.3771 [DOI] [PubMed] [Google Scholar]
- 45.Buffery PJ, Matthew Strother R. Domperidone safety: A mini-review of the science of QT prolongation and clinical implications of recent global regulatory recommendations. N Z Med J. Published online 2015. [PubMed] [Google Scholar]
- 46.Hondeghem LM. Domperidone: Limited benefits with significant risk for sudden cardiac death. J Cardiovasc Pharmacol. Published online 2013. doi: 10.1097/FJC.0b013e31827afd0d [DOI] [PubMed] [Google Scholar]
- 47.Group C, Recognition M, Procedures D, et al. Restrictions on the use of domperidone-containing medicines. Eur Med Agency. Published online 2014. [Google Scholar]
- 48.Giaccone G, Bertetto O, Calciati A. TWO SUDDEN DEATHS DURING PROPHYLACTIC ANTIEMETIC TREATMENT WITH HIGH DOSES OF DOMPERIDONE AND METHYLPREDNISOLONE. Lancet. Published online 1984. doi: 10.1016/S0140-6736(84)90841-9 [DOI] [PubMed] [Google Scholar]
- 49.Joss RA, Goldhirsch A, Brunner KW, Galeazzi RL. SUDDEN DEATH IN CANCER PATIENT ON HIGH-DOSE DOMPERIDONE. Lancet. Published online 1982. doi: 10.1016/S0140-6736(82)92016-5 [DOI] [PubMed] [Google Scholar]
- 50.Osborne RJ, Slevin ML, Hunter RW, Hamer J. Cardiac Arrhythmias during Cytotoxic Chemotherapy: Role of Domperidone. Hum Exp Toxicol. Published online 1985. doi: 10.1177/096032718500400608 [DOI] [PubMed] [Google Scholar]
- 51.Bruera E, Villamayor R, Roca E, Barugel M, Tronge J, Chacon R. Q-T interval prolongation and ventricular fibrillation with iv domperidone. Cancer Treat Rep. Published online 1986. [PubMed] [Google Scholar]
- 52.Roussak JB, Carey P, Parry H. Cardiac arrest after treatment with intravenous domperidone. Br Med J. Published online 1984. doi: 10.1136/bmj.289.6458.1579 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Boyce MJ, Baisley KJ, Warrington SJ. Pharmacokinetic interaction between domperidone and ketoconazole leads to QT prolongation in healthy volunteers: A randomized, placebo-controlled, double-blind, crossover study. Br J Clin Pharmacol. Published online 2012. doi: 10.1111/j.1365-2125.2011.04093.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Roldan CJ, Chambers KA, Paniagua L, Patel S, Cardenas-Turanzas M, Chathampally Y. Randomized Controlled Double-blind Trial Comparing Haloperidol Combined With Conventional Therapy to Conventional Therapy Alone in Patients With Symptomatic Gastroparesis. Acad Emerg Med. Published online 2017. doi: 10.1111/acem.13245 [DOI] [PubMed] [Google Scholar]
- 55.Furyk JS, Meek RA, Egerton-Warburton D. Drugs for the treatment of nausea and vomiting in adults in the emergency department setting. Cochrane Database Syst Rev. Published online 2015. doi: 10.1002/14651858.CD010106.pub2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.De Colle C, van der Hart M, Chen J, Rassoulpour A, Pasricha PJ. 1079 NG101: A Potent and Selective Dopamine D2 Receptor Antagonist as a Potential Alternative to Metoclopramide and Domperidone for the Treatment of Gastroparesis. Gastroenterology. Published online 2016. doi: 10.1016/s0016-5085(16)30794-6 [DOI] [Google Scholar]
- 57.Flake ZA, Scalley RD, Bailey AG. Practical Selection of Antiemetics. Am Fam Physician. Published online 2004. [PubMed] [Google Scholar]
- 58.Chepyala P, Olden KW. Nausea and vomiting. Curr Treat Options Gastroenterol. Published online 2008. doi: 10.1007/s11938-008-0026-6 [DOI] [PubMed] [Google Scholar]
- 59.Golding JF, Stott JRR. Comparison of the effects of a selective muscarinic receptor antagonist and hyoscine (scopolamine) on motion sickness, skin conductance and heart rate. Br J Clin Pharmacol. Published online 1997. doi: 10.1046/j.1365-2125.1997.00606.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Kaiser R, Sezer O, Papies A, et al. Patient-tailored antiemetic treatment with 5-hydroxytryptamine type 3 receptor antagonists according to cytochrome P-450 2D6 genotypes. J Clin Oncol. Published online 2002. doi: 10.1200/JCO.2002.09.064 [DOI] [PubMed] [Google Scholar]
- 61.Boike SC, Ilson B, Zariffa N, Jorkasky DK. Cardiovascular effects of i.v. granisetron at two administration rates and of ondansetron in healthy adults. Am J Heal Pharm. Published online 1997. doi: 10.1093/ajhp/54.10.1172 [DOI] [PubMed] [Google Scholar]
- 62.Yavas C, Dogan U, Yavas G, Araz M, Yavas Ata O. Acute effect of palonosetron on electrocardiographic parameters in cancer patients: A prospective study. Support Care Cancer. Published online 2012. doi: 10.1007/s00520-011-1348-9 [DOI] [PubMed] [Google Scholar]
- 63.Navari RM, Koeller JM. Electrocardiographic and cardiovascular effects of the 5-hydroxytryptamine3 receptor antagonists. Ann Pharmacother. Published online 2003. doi: 10.1345/aph.1C510 [DOI] [PubMed] [Google Scholar]
- 64.Obal D, Yang D, Sessler DI. Perioperative doses of ondansetron or dolasetron do not lengthen the qt interval. Mayo Clin Proc. Published online 2014. doi: 10.1016/j.mayocp.2013.10.008 [DOI] [PubMed] [Google Scholar]
- 65.Zuo P, Haberer LJ, Fang L, Hunt TL, Ridgway D, Russo MW. Integration of modeling and simulation to support changes to ondansetron dosing following a randomized, double-blind, placebo-, and active-controlled thorough QT study. J Clin Pharmacol. Published online 2014. doi: 10.1002/jcph.322 [DOI] [PubMed] [Google Scholar]
- 66.Tack J, Coremans G, Janssens J. A Risk-Benefit Assessment of Cisapride in the Treatment of Gastrointestinal Disorders. Drug Saf. Published online 1995. doi: 10.2165/00002018-199512060-00004 [DOI] [PubMed] [Google Scholar]
- 67.Quigley EM. Cisapride: What can we learn from the rise and fall of a prokinetic? J Dig Dis. Published online 2011. doi: 10.1111/j.1751-2980.2011.00491.x [DOI] [PubMed] [Google Scholar]
- 68.Hasler WL, Schoenfeld P. Safety profile of tegaserod, a 5-HT4 receptor agonist, for the treatment of irritable bowel syndrome. Drug Saf. Published online 2004. doi: 10.2165/00002018-200427090-00001 [DOI] [PubMed] [Google Scholar]
- 69.Marciniak TA, Serebruany V. Should We Use Tegaserod for Irritable Bowel Syndrome? Am J Ther. Published online 2019. doi: 10.1097/MJT.0000000000000947 [DOI] [PubMed] [Google Scholar]
- 70.Shokrollahi M, Chen JH, Huizinga JD. Intraluminal prucalopride increases propulsive motor activities via luminal 5-HT4 receptors in the rabbit colon. Neurogastroenterol Motil. Published online 2019. doi: 10.1111/nmo.13598 [DOI] [PubMed] [Google Scholar]
- 71.Mahajan R Prucalopride: A Recently Approved Drug by the Food and Drug Administration for Chronic Idiopathic Constipation. Int J Appl basic Med Res. 2019;9(1):1–2. doi: 10.4103/ijabmr.IJABMR_412_18 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Vijayvargiya P, Camilleri M. Use of prucalopride in adults with chronic idiopathic constipation. Expert Rev Clin Pharmacol. Published online 2019. doi: 10.1080/17512433.2019.1620104 [DOI] [PubMed] [Google Scholar]
- 73.Manini ML, Camilleri M, Goldberg M, et al. Effects of Velusetrag (TD-5108) on gastrointestinal transit and bowel function in health and pharmacokinetics in health and constipation. Neurogastroenterol Motil. Published online 2010. doi: 10.1111/j.1365-2982.2009.01378.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Abell T, Kuo B, Esfandyari T, et al. 784 – Velusetrag Improves Gastoparesis Both in Symptoms and Gastric Emptying in Patients with Diabetic Or Idiopathic Gastroparesis in a 12-Week Global Phase 2B Study. Gastroenterology. Published online 2019. doi: 10.1016/s0016-5085(19)37201-4 [DOI] [Google Scholar]
- 75.Darmani NA, Ray AP. Evidence for a re-evaluation of the neurochemical and anatomical bases of chemotherapy-induced vomiting. Chem Rev. Published online 2009. doi: 10.1021/cr900117p [DOI] [PubMed] [Google Scholar]
- 76.Endo T, Minami M, Hirafuji M, et al. Neurochemistry and neuropharmacology of emesis - The role of serotonin. Toxicology. Published online 2000. doi: 10.1016/S0300-483X(00)00314-0 [DOI] [PubMed] [Google Scholar]
- 77.Saito R, Takano Y, Kamiya HO. Roles of substance P and NK1 receptor in the brainstem in the development of emesis. J Pharmacol Sci. Published online 2003. doi: 10.1254/jphs.91.87 [DOI] [PubMed] [Google Scholar]
- 78.Andrews PLR, Rudd JA. The Role of Tachykinins and the Tachykinin NK1 Receptor in Nausea and Emesis. In: ; 2004. doi: 10.1007/978-3-642-18891-6_12 [DOI] [Google Scholar]
- 79.Chong K, Dhatariya K. A case of severe, refractory diabetic gastroparesis managed by prolonged use of aprepitant. Nat Rev Endocrinol. Published online 2009. doi: 10.1038/nrendo.2009.50 [DOI] [PubMed] [Google Scholar]
- 80.Fahler J, Wall GC, Leman BI. Gastroparesis-associated refractory nausea treated with aprepitant. Ann Pharmacother. Published online 2012. doi: 10.1345/aph.1R484 [DOI] [PubMed] [Google Scholar]
- 81.Pasricha PJ, Yates K, Sarosiek I, et al. Aprepitant for Symptoms of Gastroparesis and Related Disorders: The APRON Randomized Clinical Trial. Am J Gastroenterol. Published online 2016. doi: 10.1038/ajg.2016.363 [DOI] [Google Scholar]
- 82.Carlin JL, Lieberman VR, Dahal A, et al. Tradipitant Complete Responder Analysis in Gastroparesis Patients. Am J Gastroenterol. Published online 2019. doi: 10.14309/01.ajg.0000594480.04971.10 [DOI] [Google Scholar]
- 83.Carlin JL, Lieberman VR, Dahal A, et al. Efficacy and Safety of Tradipitant in Patients With Diabetic and Idiopathic Gastroparesis in a Randomized, Placebo-Controlled Trial. Gastroenterology. Published online 2020. doi: 10.1053/j.gastro.2020.07.029 [DOI] [PubMed] [Google Scholar]
- 84.Murray CDR, Martin NM, Patterson M, et al. Ghrelin enhances gastric emptying in diabetic gastroparesis: A double blind, placebo controlled, crossover study. Gut. Published online 2005. doi: 10.1136/gut.2005.069088 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.Pradhan G, Samson SL, Sun Y. Ghrelin: Much more than a hunger hormone. Curr Opin Clin Nutr Metab Care. Published online 2013. doi: 10.1097/MCO.0b013e328365b9be [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Chedid V, Camilleri M. Relamorelin for the treatment of gastrointestinal motility disorders. Expert Opin Investig Drugs. Published online 2017. doi: 10.1080/13543784.2017.1373088 [DOI] [PubMed] [Google Scholar]
- 87.Camilleri M, McCallum RW, Tack J, Spence SC, Gottesdiener K, Fiedorek FT. Efficacy and Safety of Relamorelin in Diabetics With Symptoms of Gastroparesis: A Randomized, Placebo-Controlled Study. Gastroenterology Published online 2017. doi: 10.1053/j.gastro.2017.07.035 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88.Camilleri M, Lembo A, McCallum R, et al. Overall safety of relamorelin in adults with diabetic gastroparesis: Analysis of phase 2a and 2b trial data. Aliment Pharmacol Ther. Published online 2020. doi: 10.1111/apt.15711 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Sanger GJ, Wang Y, Hobson A, Broad J. Motilin: Towards a new understanding of the gastrointestinal neuropharmacology and therapeutic use of motilin receptor agonists. Br J Pharmacol. Published online 2013. doi: 10.1111/bph.12075 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Hasler WL. Newest Drugs for Chronic Unexplained Nausea and Vomiting. Curr Treat Options Gastroenterol. Published online 2016. doi: 10.1007/s11938-016-0110-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.Barton ME, Otiker T, Vasist Johnson L, et al. 70 A Randomized, Double-Blind, Placebo-Controlled Phase II Study (MOT114479) to Evaluate the Safety and Efficacy and Dose Response of 28 Days of Orally Administered Camicinal, a Motilin Receptor Agonist, in Diabetics With Gastroparesis. Vol 146.; 2014. doi: 10.1016/S0016-5085(14)60070-6 [DOI] [Google Scholar]
- 92.Smith N, Longo N, Levert K, Hyland K, Blau N. Phase I clinical evaluation of CNSA-001 (sepiapterin), a novel pharmacological treatment for phenylketonuria and tetrahydrobiopterin deficiencies, in healthy volunteers. Mol Genet Metab. Published online 2019. doi: 10.1016/j.ymgme.2019.02.001 [DOI] [PubMed] [Google Scholar]
- 93.Abell TL, Garcia LM, Wiener GJ, Wo JM, Bulat RS, Smith N. Improved Gastric Accommodation in Women With Moderate or Severe Diabetic Gastroparesis Randomized to Oral CNSA-001 ( Sepiapterin ) versus Placebo. 2020;001:2020. [DOI] [PubMed] [Google Scholar]
- 94.Singh P, Yoon SS, Kuo B. Nausea: A review of pathophysiology and therapeutics. Therap Adv Gastroenterol. Published online 2016. doi: 10.1177/1756283X15618131 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95.Parkman HP, Van Natta ML, Abell TL, et al. Effect of nortriptyline on symptoms of idiopathic gastroparesis: The NORIG randomized clinical trial. JAMA - J Am Med Assoc. Published online 2013. doi: 10.1001/jama.2013.282833 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.BLANCHARD K Long term anti-emetic therapy with zofran and phenergren (ZAP): does zap loose its zip? Am J Gastroenterol. Published online 2002. doi: 10.1016/s0002-9270(02)05350-9 [DOI] [Google Scholar]
- 97.D R, T KM, P SJ, A. F-O, B E, L. VA Serologic Profiles Aiding the Diagnosis of Autoimmune Gastrointestinal Dysmotility. Clin Gastroenterol Hepatol. Published online 2008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98.Pasha SF, Lunsford TN, Lennon VA. Autoimmune Gastrointestinal Dysmotility Treated Successfully With Pyridostigmine. Gastroenterology. Published online 2006. doi: 10.1053/j.gastro.2006.06.018 [DOI] [PubMed] [Google Scholar]
- 99.Lennon VA, Sas DF, Busk MF, et al. Enteric neuronal autoantibodies in pseudoobstruction with small-cell lung carcinoma. Gastroenterology. Published online 1991. doi: 10.1016/0016-5085(91)90593-a [DOI] [PubMed] [Google Scholar]
- 100.Lennon VA, Ermilov LG, Szurszewski JH, Vernino S. Immunization with neuronal nicotinic acetylcholine receptor induces neurological autoimmune disease. J Clin Invest. Published online 2003. doi: 10.1172/JCI17429 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 101.Grover M, Farrugia G, Lurken MS, et al. Cellular changes in diabetic and idiopathic gastroparesis. Gastroenterology. Published online 2011. doi: 10.1053/j.gastro.2011.01.046 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102.Flanagan EP, Saito YA, Lennon VA, et al. Immunotherapy trial as diagnostic test in evaluating patients with presumed autoimmune gastrointestinal dysmotility. Neurogastroenterol Motil. Published online 2014. doi: 10.1111/nmo.12391 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 103.Soota K, Kedar A, Nikitina Y, Arendale E, Vedanarayanan V, Abell TL. Immunomodulation for treatment of drug and device refractory gastroparesis. Results Immunol. Published online 2016. doi: 10.1016/j.rinim.2016.02.001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 104.Ashat M, Lewis A, Liaquat H, et al. Intravenous immunoglobulin in drug and device refractory patients with the symptoms of gastroparesis—an open-label study. Neurogastroenterol Motil. Published online 2018. doi: 10.1111/nmo.13256 [DOI] [PubMed] [Google Scholar]
- 105.Payne SC, Furness JB, Stebbing MJ. Bioelectric neuromodulation for gastrointestinal disorders: effectiveness and mechanisms. Nat Rev Gastroenterol Hepatol. Published online 2019. doi: 10.1038/s41575-018-0078-6 [DOI] [PubMed] [Google Scholar]
- 106.McCallum RW, Chen JDZ, Lin Z, et al. Gastric pacing improves emptying and symptoms in patients with gastroparesis. Gastroenterology. Published online 1998. doi: 10.1016/S0016-5085(98)70528-1 [DOI] [PubMed] [Google Scholar]
- 107.McCallum RW, Snape W, Brody F, Wo J, Parkman HP, Nowak T. Gastric electrical stimulation with enterra therapy improves symptoms from diabetic gastroparesis in a prospective study. Clin Gastroenterol Hepatol. Published online 2010. doi: 10.1016/j.cgh.2010.05.020 [DOI] [PubMed] [Google Scholar]
- 108.Paton WDM, Vane JR. An analysis of the responses of the isolated stomach to electrical stimulation and to drugs. J Physiol. Published online 1963. doi: 10.1113/jphysiol.1963.sp007040 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 109.BILGUTAY AM, LILLEHEI CW, WINGROVE R, GRIFFEN WO, BONNABEAU RC. GASTROINTESTINAL PACING: A NEW CONCEPT IN THE TREATMENT OF ILEUS. Biomed Sci Instrum. Published online 1963. [PubMed] [Google Scholar]
- 110.QUAST DC, BEALL AC, DEBAKEY ME CLINICAL EVALUATION OF THE GASTROINTESTINAL PACER. Surg Gynecol Obstet. Published online 1965. [PubMed] [Google Scholar]
- 111.Berger T, Kewenter J, Kock NG. Response to gastrointestinal pacing: antral, duodenal and jejunal motility in control and postoperative patients. Ann Surg. Published online 1966. doi: 10.1097/00000658-196607000-00015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 112.Familoni BO, Abell TL, Voeller G, Salem A, Gaber O. Electrical stimulation at a frequency higher than basal rate in human stomach. Dig Dis Sci. Published online 1997. doi: 10.1023/A:1018852011857 [DOI] [PubMed] [Google Scholar]
- 113.Lin Z, Forster J, Sarosiek I, McCallum RW. Treatment of gastroparesis with electrical stimulation. Dig Dis Sci. 2003;48(5):837–848. doi: 10.1023/a:1023099206939 [DOI] [PubMed] [Google Scholar]
- 114.Zoll B, Jehangir A, Malik Z, Edwards MA, Petrov RV, Parkman HR. Gastric Electric Stimulation for Refractory Gastroparesis. J Clin Outcomes Manag. Published online 2019. [PMC free article] [PubMed] [Google Scholar]
- 115.Abell TL, Chen J, Emmanuel A, Jolley C, Sarela AI, Törnblom H. Neurostimulation of the gastrointestinal tract: Review of recent developments. Neuromodulation. Published online 2015. doi: 10.1111/ner.12260 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 116.Ayinala S, Batista O, Goyal A, et al. Temporary gastric electrical stimulation with orally or PEG-placed electrodes in patients with drug refractory gastroparesis. Gastrointest Endosc. Published online 2005. doi: 10.1016/S0016-5107(05)00076-3 [DOI] [PubMed] [Google Scholar]
- 117.Daram SR, Tang SJ, Abell TL. Temporary gastric electrical stimulation for gastroparesis: Endoscopic placement of electrodes (ENDOstim). Surg Endosc. Published online 2011. doi: 10.1007/s00464-011-1710-5 [DOI] [PubMed] [Google Scholar]
- 118.Andersson S, Ringström G, Elfvin A, Simrén M, Lönroth H, Abrahamsson H. Temporary percutaneous gastric electrical stimulation: A novel technique tested in patients with non-established indications for gastric electrical stimulation. Digestion. Published online 2010. doi: 10.1159/000291905 [DOI] [PubMed] [Google Scholar]
- 119.Soffer E, Abell T, Lin Z, et al. Review article: Gastric electrical stimulation for gastroparesis - Physiological foundations, technical aspects and clinical implications. Aliment Pharmacol Ther. Published online 2009. doi: 10.1111/j.1365-2036.2009.04082.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 120.Yin J, Abell TD, McCallum RW, Chen JDZ. Gastric neuromodulation with Enterra system for nausea and vomiting in patients with gastroparesis. Neuromodulation. Published online 2012. doi: 10.1111/j.1525-1403.2012.00429.x [DOI] [PubMed] [Google Scholar]
- 121.Chen JDZ, Qian L, Ouyang H, Yin J. Gastric electrical stimulation with short pulses reduces vomiting but not dysrhythmias in dogs. Gastroenterology. Published online 2003. doi: 10.1053/gast.2003.50048 [DOI] [PubMed] [Google Scholar]
- 122.Lin Z, Forster J, Sarosiek I, McCallum RW. Treatment of Diabetic Gastroparesis by High-Frequency Gastric Electrical Stimulation. Diabetes Care. Published online 2004. doi: 10.2337/diacare.27.5.1071 [DOI] [PubMed] [Google Scholar]
- 123.Abell TL, Van Cutsem E, Abrahamsson H, et al. Gastric electrical stimulation in intractable symptomatic gastroparesis. Digestion. Published online 2002. doi: 10.1159/000068359 [DOI] [PubMed] [Google Scholar]
- 124.Abell T, McCallum RW, Hocking M, et al. Gastric electrical stimulation for medically refractory gastroparesis. Gastroenterology. Published online 2003. doi: 10.1016/S0016-5085(03)00878-3 [DOI] [PubMed] [Google Scholar]
- 125.O’Grady G, Egbuji JU, Du P, Cheng LK, Pullan AJ, Windsor JA. High-frequency gastric electrical stimulation for the treatment of gastroparesis: A meta-analysis. World J Surg. Published online 2009. doi: 10.1007/s00268-009-0096-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 126.Singh S, McCrary J, Kedar A, et al. Temporary endoscopic stimulation in gastroparesis-like syndrome. J Neurogastroenterol Motil. Published online 2015. doi: 10.5056/jnm15046 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 127.Shine A, Abell TL. Role of Gastric Electrical Stimulation in the Treatment of Gastroparesis. Gastrointest Disord. 2020;2(1):12–26. doi: 10.3390/gidisord2010003 [DOI] [Google Scholar]
- 128.Anand C, Al-Juburi A, Familoni B, et al. Gastric electrical stimulation is safe and effective: A long-term study in patients with drug-refractory gastroparesis in three regional centers. Digestion. Published online 2007. doi: 10.1159/000102961 [DOI] [PubMed] [Google Scholar]
- 129.Brody F, Zettervall SL, Richards NG, et al. Follow-up after gastric electrical stimulation for gastroparesis. In: Journal of the American College of Surgeons. ; 2015. doi: 10.1016/j.jamcollsurg.2014.10.001 [DOI] [PubMed] [Google Scholar]
- 130.Ducrotte P, Coffin B, Bonaz B, et al. Gastric Electrical Stimulation Reduces Refractory Vomiting in a Randomized Crossover Trial. Gastroenterology. Published online 2020. doi: 10.1053/j.gastro.2019.10.018 [DOI] [PubMed] [Google Scholar]
- 131.Gourcerol G, Leblanc I, Leroi AM, Denis P, Ducrotte P. Gastric electrical stimulation in medically refractory nausea and vomiting. Eur J Gastroenterol Hepatol. Published online 2007. doi: 10.1097/01.meg.0000250584.15490.b4 [DOI] [PubMed] [Google Scholar]
- 132.Shah H, Wendorf G, Ahmed S, et al. Treating an oft-unrecognized and troublesome entity: using gastric electrical stimulation to reduce symptoms of malignancy-associated gastroparesis. Support Care Cancer. Published online 2017. doi: 10.1007/s00520-016-3375-z [DOI] [PubMed] [Google Scholar]
- 133.Bhatti S, Jaafar I, Hassan H, et al. Effects of Gastric Neuromodulation on Crohn’s Disease in Patients With Coexisting Symptoms of Gastroparesis. Neuromodulation. Published online 2020. doi: 10.1111/ner.13118 [DOI] [PubMed] [Google Scholar]
- 134.Arshad Q, Cerchiai N, Goga U, et al. Electrocortical therapy for motion sickness. Neurology. Published online 2015. doi: 10.1212/WNL.0000000000001989 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 135.Paulon E, Nastou D, Jaboli F, Marin J, Liebler E, Epstein O. Proof of concept: Short-term noninvasive cervical vagus nerve stimulation in patients with drugrefractory gastroparesis. Frontline Gastroenterol. Published online 2017. doi: 10.1136/flgastro-2017-100809 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 136.Gottfried-Blackmore A, Adler EP, Fernandez-Becker N, Clarke J, Habtezion A, Nguyen L. Open-label pilot study: Non-invasive vagal nerve stimulation improves symptoms and gastric emptying in patients with idiopathic gastroparesis. Neurogastroenterol Motil. Published online 2020. doi: 10.1111/nmo.13769 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 137.Friedenberg FK, Palit A, Parkman HP, Hanlon A, Nelson DB. Botulinum toxin A for the treatment of delayed gastric emptying. Am J Gastroenterol. Published online 2008. doi: 10.1111/j.1572-0241.2007.01676.x [DOI] [PubMed] [Google Scholar]
- 138.Malik Z, Sankineni A, Parkman HP. Assessing pyloric sphincter pathophysiology using EndoFLIP in patients with gastroparesis. Neurogastroenterol Motil. Published online 2015. doi: 10.1111/nmo.12522 [DOI] [PubMed] [Google Scholar]
- 139.Desprez C, Melchior C, Wuestenberghs F, et al. Pyloric distensibility measurement predicts symptomatic response to intrapyloric botulinum toxin injection. Gastrointest Endosc. Published online 2019. doi: 10.1016/j.gie.2019.04.228 [DOI] [PubMed] [Google Scholar]
- 140.Podboy A, Hwang JH, Nguyen LA, et al. Gastric per-oral endoscopic myotomy: Current status and future directions. World J Gastroenterol. Published online 2019. doi: 10.3748/wjg.v25.i21.2581 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 141.Xu J, Chen T, Elkholy S, et al. Gastric Peroral Endoscopic Myotomy (G-POEM) as a Treatment for Refractory Gastroparesis: Long-Term Outcomes. Can J Gastroenterol Hepatol. Published online 2018. doi: 10.1155/2018/6409698 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 142.Shada AL, Dunst CM, Pescarus R, et al. Laparoscopic pyloroplasty is a safe and effective first-line surgical therapy for refractory gastroparesis. Surg Endosc. Published online 2016. doi: 10.1007/s00464-015-4385-5 [DOI] [PubMed] [Google Scholar]
- 143.Landreneau JP, Strong AT, El-Hayek K, et al. Laparoscopic pyloroplasty versus endoscopic per-oral pyloromyotomy for the treatment of gastroparesis. Surg Endosc. Published online 2019. doi: 10.1007/s00464-018-6342-6 [DOI] [PubMed] [Google Scholar]
- 144.Davis BR, Sarosiek I, Bashashati M, Alvarado B, McCallum RW. The Long-Term Efficacy and Safety of Pyloroplasty Combined with Gastric Electrical Stimulation Therapy in Gastroparesis. J Gastrointest Surg. Published online 2017. doi: 10.1007/s11605-016-3327-4 [DOI] [PubMed] [Google Scholar]
- 145.Zoll B, Jehangir A, Edwards MA, et al. Surgical Treatment for Refractory Gastroparesis: Stimulator, Pyloric Surgery, or Both? J Gastrointest Surg. Published online 2019. doi: 10.1007/s11605-019-04391-x [DOI] [PubMed] [Google Scholar]
- 146.Marowski S, Xu Y, Greenberg J, Funk L, Lidor A, Shada A. Both gastric electrical stimulation and pyloric surgery offer long-term symptom improvement in patients with gastroparesis. Surg Endosc. Published online 2020. doi: 10.1007/s00464-020-07960-3 [DOI] [PubMed] [Google Scholar]
- 147.Myint AS, Rieders B, Tashkandi M, et al. Current and emerging therapeutic options for gastroparesis. Gastroenterol Hepatol. Published online 2018. [PMC free article] [PubMed] [Google Scholar]
- 148.Abell TL, Familoni B, Voeller G, et al. Electrophysiologic, morphologic, and serologic features of chronic unexplained nausea and vomiting: Lessons learned from 121 consecutive patients. Surgery. Published online 2009. doi: 10.1016/j.surg.2008.12.006 [DOI] [PubMed] [Google Scholar]
- 149.Palatty PL, Haniadka R, Valder B, Arora R, Baliga MS. Ginger in the Prevention of Nausea and Vomiting: A Review. Crit Rev Food Sci Nutr. Published online 2013. doi: 10.1080/10408398.2011.553751 [DOI] [PubMed] [Google Scholar]
- 150.Qian QH, Yue W, Chen WH, Yang ZH, Liu ZT, Wang YX. Effect of gingerol on substance P and NK1 receptor expression in a vomiting model of mink. Chin Med J (Engl). Published online 2010. doi: 10.3760/cma.j.issn.0366-6999.2010.04.017 [DOI] [PubMed] [Google Scholar]
- 151.Jin Z, Lee G, Kim S, Park CS, Park YS, Jin YH. Ginger and its pungent constituents non-competitively inhibit serotonin currents on visceral afferent neurons. Korean J Physiol Pharmacol. Published online 2014. doi: 10.4196/kjpp.2014.18.2.149 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 152.Abdel-Aziz H, Windeck T, Ploch M, Verspohl EJ. Mode of action of gingerols and shogaols on 5-HT3 receptors: Binding studies, cation uptake by the receptor channel and contraction of isolated guinea-pig ileum. Eur J Pharmacol. Published online 2006. doi: 10.1016/j.ejphar.2005.10.049 [DOI] [PubMed] [Google Scholar]
- 153.Ghayur MN, Gilani AH. Pharmacological basis for the medicinal use of ginger in gastrointestinal disorders. Dig Dis Sci. Published online 2005. doi: 10.1007/s10620-005-2957-2 [DOI] [PubMed] [Google Scholar]
- 154.Micklefield GH, Redeker Y, Meister V, Jung O, Greving I, May B. Effects of ginger on gastroduodenal motility. Int J Clin Pharmacol Ther. Published online 1999. [PubMed] [Google Scholar]
- 155.Wu KL, Rayner CK, Chuah SK, et al. Effects of ginger on gastric emptying and motility in healthy humans. Eur J Gastroenterol Hepatol. Published online 2008. doi: 10.1097/MEG.0b013e3282f4b224 [DOI] [PubMed] [Google Scholar]
- 156.Lien HC, Sun WM, Chen YH, Kim H, Hasler W, Owyang C. Effects of ginger on motion sickness and gastric slow-wave dysrhythmias induced by circular vection. Am J Physiol - Gastrointest Liver Physiol. Published online 2003. doi: 10.1152/ajpgi.00164.2002 [DOI] [PubMed] [Google Scholar]
- 157.Gonlachanvit S, Chen YH, Hasler WL, Sun WM, Owyang C. Ginger Reduces Hyperglycemia-Evoked Gastric Dysrhythmias in Healthy Humans: Possible Role of Endogenous Prostaglandins. J Pharmacol Exp Ther. Published online 2003. doi: 10.1124/jpet.103.053421 [DOI] [PubMed] [Google Scholar]
- 158.Stewart JJ, Wood MJ, Wood CD, Mims ME. Effects of ginger on motion sickness susceptibility and gastric function. Pharmacology. Published online 1991. doi: 10.1159/000138781 [DOI] [PubMed] [Google Scholar]
- 159.O’Donnell A, McParlin C, Robson SC, et al. Treatments for hyperemesis gravidarum and nausea and vomiting in pregnancy: A systematic review and economic assessment. Health Technol Assess (Rockv). Published online 2016. doi: 10.3310/hta20740 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 160.Matthews A, Haas DM, O’Mathúna DP, Dowswell T. Interventions for nausea and vomiting in early pregnancy. Cochrane Database Syst Rev. Published online 2015. doi: 10.1002/14651858.CD007575.pub4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 161.Ryan JL, Heckler CE, Roscoe JA, et al. Ginger (Zingiber officinale) reduces acute chemotherapy-induced nausea: A URCC CCOP study of 576 patients. Support Care Cancer. Published online 2012. doi: 10.1007/s00520-011-1236-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 162.Marx WM, Teleni L, Mccarthy AL, et al. Ginger (Zingiber officinale) and chemotherapy-induced nausea and vomiting: A systematic literature review. Nutr Rev. Published online 2013. doi: 10.1111/nure.12016 [DOI] [PubMed] [Google Scholar]
- 163.Nguyen LA, Lee L. Complementary and alternative medicine for nausea and vomiting. In: Nausea and Vomiting: Diagnosis and Treatment. Springer International Publishing; 2016:165–173. doi: 10.1007/978-3-319-34076-0_12 [DOI] [Google Scholar]
- 164.Ernst E Acupuncture- A critical analysis. J Intern Med. Published online 2006. doi: 10.1111/j.1365-2796.2005.01584.x [DOI] [PubMed] [Google Scholar]
- 165.Ernst E, Lee MS, Choi TY. Acupuncture: Does it alleviate pain and are there serious risks? A review of reviews. Pain Published online 2011. doi: 10.1016/j.pain.2010.11.004 [DOI] [PubMed] [Google Scholar]
- 166.Ernst E Acupuncture: What Does the Most Reliable Evidence Tell Us? J Pain Symptom Manage. Published online 2009. doi: 10.1016/j.jpainsymman.2008.04.009 [DOI] [PubMed] [Google Scholar]
- 167.Lee A, Chan SKC, Fan LTY. Stimulation of the wrist acupuncture point PC6 for preventing postoperative nausea and vomiting. Cochrane Database Syst Rev. Published online 2015. doi: 10.1002/14651858.CD003281.pub4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 168.Greenlee H, DuPont-Reyes MJ, Balneaves LG, et al. Clinical practice guidelines on the evidence-based use of integrative therapies during and after breast cancer treatment. CA Cancer J Clin. Published online 2017. doi: 10.3322/caac.21397 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 169.Lee J, Dodd M, Dibble S, Abrams D. Review of Acupressure Studies for Chemotherapy-Induced Nausea and Vomiting Control. J Pain Symptom Manage. Published online 2008. doi: 10.1016/j.jpainsymman.2007.10.019 [DOI] [PubMed] [Google Scholar]
- 170.Yang M, Li X, Liu S, et al. Meta-analysis of acupuncture for relieving non-organic dyspeptic symptoms suggestive of diabetic gastroparesis. BMC Complement Altern Med. Published online 2013. doi: 10.1186/1472-6882-13-311 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 171.Chen J, Sarosiek I, McCallum R, et al. Chronic Electrical Stimulation at Acupuncture Points Improves Dyspeptic Symptoms in Patients with Diabetic Gastroparesis. Am J Gastroenterol. Published online 2012. doi: 10.14309/00000434-201210001-00135 [DOI] [Google Scholar]
- 172.Sarosiek I, Song G, Sun Y, et al. Central and peripheral effects of transcutaneous acupuncture treatment for nausea in patients with diabetic gastroparesis. J Neurogastroenterol Motil. Published online 2017. doi: 10.5056/jnm16097 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 173.cheng Guo W, Wang F Effect of nerve electrical stimulation for treating chemotherapy-induced nausea and vomiting in patients with advanced gastric cancer: A randomized controlled trial. Med (United States). Published online 2018. doi: 10.1097/MD.0000000000013620 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 174.Syrjala KL, Cummings C, Donaldson GW. Hypnosis or cognitive behavioral training for the reduction of pain and nausea during cancer treatment: a controlled clinical trial. Pain. Published online 1992. doi: 10.1016/0304-3959(92)90049-H [DOI] [PubMed] [Google Scholar]
- 175.Karagozoglu S, Tekyasar F, Yilmaz FA. Effects of music therapy and guided visual imagery on chemotherapy-induced anxiety and nausea-vomiting. J Clin Nurs. Published online 2013. doi: 10.1111/jocn.12030 [DOI] [PubMed] [Google Scholar]
- 176.Rashed H, Cutts T, Abell T, et al. Predictors of response to a behavioral treatment in patients with chronic gastric motility disorders. Dig Dis Sci. Published online 2002. doi: 10.1023/A:1015029805498 [DOI] [PubMed] [Google Scholar]