

Abstract
Background
Many diabetic individuals use prescription and non-prescription opioids and opiates. We aimed to investigate the joint effect of diabetes and opiate use on all-cause and cause-specific mortality.
Methods
Golestan Cohort study is a prospective population-based study in Iran. A total of 50 045 people—aged 40–75, 28 811 women, 8487 opiate users, 3548 diabetic patients—were followed during a median of 11.1 years, with over 99% success follow-up. Hazard ratio and 95% confidence intervals (HRs, 95% CIs), and preventable death attributable to each risk factor, were calculated.
Results
After 533 309 person-years, 7060 deaths occurred: 4178 (10.8%) of non-diabetic non-opiate users, 757 (25.3%) diabetic non-users, 1906 (24.0%) non-diabetic opiate users and 219 (39.8%) diabetic opiate users. Compared with non-diabetic non-users, HRs (95% CIs) for all-cause mortality were 2.17 (2.00–2.35) in diabetic non-opiate users, 1.63 (1.53–1.74) in non-diabetic opiate users and 2.76 (2.40–3.17) in diabetic opiate users. Among those who both had diabetes and used opiates, 63.8% (95% CI: 58.3%–68.5%) of all deaths were attributable to these risk factors, compared with 53.9% (95% CI: 50%–57.4%) in people who only had diabetes and 38.7% (95% CI: 34.6%–42.5%) in non-diabetic opiate users. Diabetes was more strongly associated with cardiovascular than cancer mortality. The risk of early mortality in known cases of diabetes did not depend on whether they started opiate use before or after their diagnosis.
Conclusions
Using opiates is detrimental to the health of diabetic patients. Public awareness about the health effects of opiates, and improvement of diabetes care especially among individuals with or at risk of opiate use, are necessary.
Keywords: Causes of death, diabetes mellitus, mortality, opiate addiction, opioids, opium
Key Messages
Although many individuals with diabetes use prescription and non-prescription opioids and opiates, the joint effects of diabetes and long-term opiate use on overall and cause-specific mortality have not been studied.
Patients with diabetes who were chronic opiate users were at increased risk of early mortality, and death due to cardiovascular diseases, cancer and other causes, compared with all other groups, including diabetics who did not use opiates.
Public awareness about the health effects of opiate use and more attention to diabetic complications such as neuropathy and psychological disorders are crucial, as they may be the underlying factors leading to opiate misuse in diabetic patients.
Introduction
Diabetes mellitus and its complications, such as heart attack, stroke, blindness, kidney failure, neuropathy and lower limb amputation, impose a great and rising burden on global health.1,2 In 2017, about 425 million adults (aged 20–79 years) had diabetes mellitus, and this number is estimated to rise to 629 million in 2045.3 This increase will be most noticeable in Africa (156%) and the Middle East (110%).3 Lifestyle modification, social support and medication adherence are important strategies for prevention and management of diabetes and have resulted in improved care in many high-income countries.2,4 However, for low- and middle-income countries, where almost 80% of diabetic adults live,3 such improvements are still not available to many.2 As a result, among diabetic patients, the proportions of death before 60 years in high-, middle- and low-income countries are 36%, 46% and 73%, respectively.3
Opiates (opium and its derivatives) have had medicinal and recreational uses for millennia5 and were among the commonly used treatments for diabetes in Europe before the widespread use of modern antidiabetic medications.5,6 In the modern era, prescription opioids (natural or synthetic products with opiate properties) are used mainly for chronic pain which is unresponsive to other pain-reduction strategies.5 In addition to their medical use, opiates and opioids are misused by as many as 53 million people, more than half using non-synthetic opiates such as opium, morphine and heroin.7 Diabetic patients may use or misuse opioids and opiates for a number of reasons. Diabetic peripheral neuropathic pain is one of these reasons8 and in one study, prescription opioids were the most common agents used to alleviate this pain.9 On the other hand, in places where non-prescription opiates are widely available, they may be used as alternative pain-killers or may still be seen as a traditional remedy for diabetes by some people.10 Limited evidence about short-term hypoglycaemic effects of opiates in type 2 diabetes11 may fuel these traditional beliefs, even among health care professionals.10,12 Finally, the mood elevation experienced by recreational opiate users13 may attract some diabetic patients who are known to be at higher risk of depression and anxiety.14,15 These psychiatric disorders are more prevalent in diabetic opioid users compared with diabetic non-opioid users.16 There is, however, little information on the overall long-term health effects of opioid or opiate use among patients with diabetes.17
South-West Asia (including the Middle East) is among hot spots of the global diabetes epidemic,2,3 and more than 90% of the global illicit opium is produced in this region.7 Diabetes and opiate use have been shown to be two important risk factors in many chronic diseases in this part of the world.18 In this region, the Golestan Cohort Study (GCS) in north-east Iran has followed up more than 50 000 adults since 2004, of whom approximately 8500 are chronic opiate users19 and 3500 have diabetes.20 Therefore, data from this cohort provide a unique opportunity to answer an important question about the joint effects of diabetes and opiate use, using longitudinal data with long-term follow-up.
Methods
Ethics approval and consent to participation
The Golestan Cohort Study protocol was approved by the ethical review committees of the Digestive Disease Research Institute of Tehran University of Medical Sciences, the US National Cancer Institute and the International Agency for Research on Cancer. All participants provided written informed consent.
Study design
The GCS recruited a total of 50 045 general population participants (28 811 women and 21 234 men, aged 40–75 years) between 2004 and 2008 from among adults in Golestan Province, Iran. Urban residents (20% of participants) were randomly selected from Gonbad city, and rural residents (80%) were selected from 326 villages in the region. Details of the study have been described previously.21
Baseline data collection
Trained physicians and nutritionists used a structured questionnaire to collect demographic, medical history and lifestyle information. Blood pressure and anthropometrics were measured using standard protocols. History of physician-diagnosed diabetes mellitus, hypertension, ischaemic heart disease, stroke and cancer, age of diagnosis and any drug consumption were asked and recorded. We defined diabetes as self-reported diagnosis by a physician and/or taking antidiabetic drugs. We have previously shown that self-reported diabetes had 61.5% sensitivity and 97.6% specificity in a random sample of participants.20 In less than 1% of patients, diabetes started before age 35 and needed insulin therapy—likely indicators of type 1 diabetes.22 Questions about opiate, tobacco and alcohol use included type, frequency, time and amount per consumption. Individuals were considered opiate users or tobacco users if they ever used non-prescription opiates or tobacco, respectively, at least once a week for a period of 6 months. We previously tested self-reported opiate use against urinary metabolites and showed the self-report to have high sensitivity and specificity (93% and 89%, respectively).23 The self-report also had excellent reliability (kappa statistic >0.9), using a re-interview after 2 months.23 In order to test dose-response relationships, opiate users were further categorized based on median daily opiate consumption. Nutritional data were collected with a validated food frequency questionnaire.24 Data on intensity, frequency and duration of physical activities were recorded and the metabolic equivalents of each task per minute per week (METs.min/week) were calculated. As a measure of socioeconomic status, wealth score was calculated for each participant based on assets, using multiple correspondence analysis.25 Hypertension was defined as having at least one of these conditions: systolic blood pressure ≥140 mmHg, diastolic blood pressure ≥90 mmHg, being a known case of hypertension or taking antihypertensive drugs.
Follow-up and outcomes
All participants were followed annually, by phone call or home visit. If a death was reported, all clinical or hospital records were collected and, if needed, a verbal autopsy was completed.26 Using the collected medical documents, two independent internists determined the cause of death based on the 10th version of the International Classification of Diseases (ICD-10) codes. The two codes were compared and if they were different, a third more experienced internist determined the final code. For the current study, the confirmed causes of death were classified as cardiovascular (I00–I99), cancer (C00–C97) or other causes.
Statistical analysis
We constructed Cox proportional hazard models, with age as the underlying time variable, to estimate hazard ratios and 95% confidence intervals (HRs, 95% CIs) for the association between diabetes, opiate use and mortality. The proportional hazard assumption was verified using ‘log-log’ plots. To analyse the joint effects of diabetes and opiate use on mortality, the population was categorized into four subgroups: non-diabetic non-opiate users (as reference), diabetic non-opiate users, non-diabetic opiate users and diabetic opiate users. We further analysed the associations of opiate use with mortality in diabetic and non-diabetic participants. Diabetic opiate users who reported a diagnosis age of diabetes (n = 539), were stratified into two groups: 268 (50%) started opiate use after (n = 178) or at the same age (n = 90) as their diabetes diagnosis, and 271 started it before their diabetes was diagnosed. Participants were followed until the date of death, loss to follow-up or 31 July 2018, whichever came first. Cox models were adjusted for: age at enrolment (years, continuous); sex (male, female); ethnicity (Turkmen, others); marital status (married, non-married); place of residence (rural, urban); educational level (no formal schooling, ≤5 years, >5 years); wealth score (quintiles); physical activity (tertiles); intake of fruit/vegetables (tertiles); body mass index (body weight/height-squared, kg/m2, continuous); cigarette smoking (never, former, or current); alcohol drinking (ever, never); opiate use (ever, never); hypertension (yes, no); and history of ischaemic heart disease (yes, no), stroke (yes, no); and cancer (yes, no), as applicable. There were no missing values for the main exposures (diabetes and opiate use), and for other covariates the number of missing values was relatively small (physical activity, vegetable and fruit consumption, body mass index and hypertension were missing in 0.4%, 1.7%, 0.02% and 0.06% of participants, respectively). In these cases, we used separate missing indicators to keep them in the models. To evaluate the interaction between opiate use and diabetes, we added the multiplicative interaction term in the models. Tests for trend were based on medians across categories.
Population-attributable fractions (PAFs) were calculated based on adjusted models, to show the proportion of all deaths attributable to the different joint groups of diabetes and opiate use, using the following equation:27
We also scaled this proportion to the percentage of deaths in the group, to report the number of additional deaths per 100 (i.e. % of preventable deaths) attributable to diabetes and/or opiates use in each group.27
We conducted a few sensitivity analyses to limit the effects of reverse causality: we excluded participants with history of other chronic diseases (ischaemic heart disease, stroke or cancer) at baseline; we also excluded the first 2 years of follow-up. We also repeated the analysis after exclusion of participants with any history of tobacco and/or alcohol use and those in lowest tertile of vegetable/fruit consumption. To restrict the confounding effects of cigarette smoking, we studied the associations stratified by the history of tobacco use. All statistical analyses were done with Stata statistical software, version 12 (StataCorp, College Station, TX).
Results
Among 50 045 cohort participants, 3444 self-reported physician-diagnosed diabetes, of whom 2346 (68%) used anti-diabetic medications. An additional 104 people used such medications but did not report a diabetes diagnosis; as a result, a total of 3548 participants (7.1%) met our definition for diabetes. Data on antidiabetic drugs used by these patients are shown in the Supplementary Appendix, available as Supplementary data at IJE online. Table 1 compares characteristics of individuals with and without diabetes at baseline. Those with diabetes were more likely to be women, urban residents, hypertensive and obese, with higher wealth scores and lower levels of physical activity. Patients with diabetes were also less likely to smoke cigarettes or use any tobacco product and ate more fruits and vegetables.
Table 1.
Baseline characteristics of the Golestan Cohort Study participants based on diabetes and opiate using status
| Variables | Diabetic participants |
Non-diabetic participants |
||||
|---|---|---|---|---|---|---|
| Opiate users (n = 551) | Non-opiate users (n = 2997) | All (n = 3548) | Opiate users (n = 7936) | Non-opiate users (n = 38 561) | All (n = 46 497) | |
| Age, years | 54.98 (9.0) | 54.53 (8.6) | 54.60 (8.7) | 53.15 (9.2) | 51.60 (8.8) | 51.87 (8.9) |
| Sex, women | 221 (40.1) | 2197 (73.3) | 2418 (68.2) | 2133 (26.9) | 24 260 (62.9) | 26 393 (56.8) |
| Ethnicity, Turkmen | 381 (69.2) | 1889 (63.0) | 2270 (64.0) | 6171 (77.8) | 28 812 (74.7) | 34 983 (75.2) |
| Education | ||||||
| No formal schooling | 380 (69.0) | 2260 (75.4) | 2640 (74.4) | 5248 (66.1) | 27 230 (70.6) | 32 478 (69.9) |
| 1–5 years schooling | 94 (17.1) | 406 (13.6) | 500 (14. 1) | 1606 (20.2) | 6357 (16.5) | 7963 (17.1) |
| >5 years schooling | 77 (14.0) | 331 (11.0) | 408 (11.5) | 1082 (13.6) | 4974 (12.9) | 6056 (13.0) |
| Residency, rural | 441 (80.0) | 2105 (70.2) | 2546 (71.8) | 7044 (88.8) | 30 421 (78.9) | 37 465 (80.6) |
| Marital status, married | 471 (85.5) | 2514 (83.9) | 2985 (84.1) | 7081 (89.2) | 33 889 (87.9) | 40 970 (88.1) |
| Cigarette smoking | ||||||
| Never | 347 (63.0) | 2779 (92.7) | 3126 (88.1) | 3664 (46.2) | 34 593 (89.7) | 38 257 (82.3) |
| Former smoker | 98 (17.8) | 119 (4.0) | 217 (6.1) | 1514 (19.1) | 1482 (3.8) | 2996 (6.4) |
| Current smoker | 106 (19.2) | 99 (3.3) | 205 (5.8) | 2758 (34.8) | 2486 (6.5) | 5244 (11.3) |
| Any tobacco, ever use | 253 (45.9) | 282 (9.4) | 535 (15.1) | 5304 (66.8) | 5028 (13.0) | 10 332 (22.2) |
| Alcohol, ever drink | 58 (10.5) | 58 (1.9) | 116 (3.3) | 867 (10.9) | 746 (1.9) | 1613 (3.5) |
| Wealth score | ||||||
| 1st quintile | 112 (20.3) | 395 (13.2) | 507 (14.3) | 2527 (31.9) | 7712 (20.0) | 10 239 (22.0) |
| 2nd quintile | 111 (20.2) | 482 (16.1) | 593 (16.7) | 1636 (20.6) | 7059 (18.3) | 8695 (18.7) |
| 3rd quintile | 118 (21.4) | 647 (21.6) | 765 (21.6) | 1645 (20.7) | 8464 (22.0) | 10 109 (21.7) |
| 4th quintile | 110 (20.0) | 665 (22.2) | 775 (21.8) | 1224 (15.4) | 7483 (19.4) | 8707 (18.7) |
| 5th quintile | 100 (18.2) | 808 (27.0) | 908 (25.6) | 904 (11.4) | 7843 (20.3) | 8747 (18.8) |
| Physical activity (METs.min/week) | ||||||
| 1st tertile | 366 (66.8) | 1128 (37.7) | 1494 (42.2) | 4199 (53.0) | 11 908 (31.0) | 16 107 (34.7) |
| 2nd tertile | 121 (22.1) | 1107 (37.0) | 1228 (34.7) | 1982 (25.0) | 12 605 (32.8) | 14 587 (31.5) |
| 3rd tertile | 61 (11.1) | 757 (25.3) | 818 (23.1) | 1737 (21.9) | 13 957 (36.3) | 15 694 (33.8) |
| Vegetable/fruit consumption (g/day) | ||||||
| 1st tertile | 157 (28.8) | 780 (26.3) | 937 (26.7) | 2771 (35.6) | 12 682 (33.5) | 15 453 (33.9) |
| 2nd tertile | 158 (29.0) | 968 (32.6) | 1126 (32.0) | 2656 (34.1) | 12 608 (33.3) | 15 264 (33.4) |
| 3rd tertile | 230 (42.2) | 1222 (41.1) | 1452 (41.3) | 2365 (30.3) | 12 573 (33.2) | 14 938 (32.7) |
| Body mass index (kg/m2) | 27.30 (5.5) | 29.34 (5.0) | 29.02 (5.2) | 23.57 (4.8) | 27.09 (5.4) | 26.49 (5.4) |
| Hypertension | 381 (69.2) | 2046 (68.3) | 2427 (68.4) | 3039(38.3) | 17 325 (45.0) | 20 364 (43.8) |
| History of chronic diseases | ||||||
| Ischaemic heart disease | 129 (23.4) | 447 (14.9) | 576 (16.2) | 570 (7.2) | 1898 (4.9) | 2468 (5.3) |
| Stroke | 12 (2.2) | 70 (2.3) | 82 (2.3) | 90 (1.1) | 246 (0.6) | 336 (0.7) |
| Cancers | 3 (0.5) | 18 (0.6) | 21 (0.6) | 26 (0.3) | 112 (0.3) | 138 (0.3) |
Data are mean (SD) or number (%). Percentages were calculated on the basis of participants with available data.
In all the cohort, 8487 (17.0%) had a history of opiate use, including 15.5% of diabetic and 17.1% of non-diabetic participants (Table 1). In both diabetic and non-diabetic opiate users, the most prevalent type of opiate consumption was raw opium and the most common routes of consumption were smoking or eating (Supplementary Appendix). Both diabetic and non-diabetic opiate users were more likely to be male, rural residents, tobacco and alcohol users, with lower wealth scores, physical activity and BMI, compared with non-users. Types and routes of opiates used by diabetic users were largely similar to non-diabetic users, although the diabetic users seemed to have lower daily doses and shorter duration of use and started opiate use later in life (Supplementary Appendix). Among all opiate users, histories of heroin use and intravenous injection were reported only in 99 (1.17%) and 15 (0.18%) individuals, respectively. Nobody reported morphine use.
After a total follow-up of 533 309 person-years (median follow-up 11.1 years), 7060 deaths occurred in the cohort and only 464 (<1%) participants were lost to follow-up. Among the 6299 confirmed causes of death, 2853 were due to cardiovascular diseases, 1396 were due to cancers and 2050 had other causes of death. Mortality rates during follow-up were: 13.1% in non-diabetic participants (10.8% in non-opiate users and 24.0% in opiate users) and 27.5% in diabetic participants (25.3% in non-opiate users and 39.8% in opiate users) (Tables 2 and 3).
Table 2.
The joint association of diabetes and opiate use with mortality in the Golestan Cohort Study
| DM-, Opiate- (n = 38 561) | DM+, Opiate- (n = 2997) | DM-, Opiate+ (n = 7936) | DM+, Opiate+ (n = 551) | |
|---|---|---|---|---|
| All-cause deaths (n = 7060) | ||||
| No. of deaths (%) | 4178 (10.8) | 757 (25.3) | 1906 (24.0) | 219 (39.8) |
| Crude rate of death/105 person-years | 997 | 2536 | 2395 | 4524 |
| Adjusted HR | 1 | 2.17 (2.00–2.35) | 1.63 (1.53–1.74) | 2.76 (2.40–3.17) |
| PAF (%) | 0 | 5.78 (5.36–6.16) | 10.43 (9.35–11.48) | 1.98 (1.81–2.12) |
| Attributable death/100 deaths | 0 | 53.9 (50.0–57.4) | 38.7 (34.6–42.5) | 63.8 (58.3–68.5) |
| Cardiovascular deaths (n = 2853) | ||||
| No. of deaths (%) | 1653 (4.3) | 382 (12.8) | 707 (8.9) | 111 (20.2) |
| Crude rate of death/105 person-years | 394 | 1280 | 889 | 2293 |
| Adjusted HR | 1 | 2.24 (2.00–2.52) | 1.62 (1.46–1.79) | 2.80 (2.30–3.41) |
| PAF (%) | 0 | 7.41 (6.69–8.08) | 9.48 (7.81–10.94) | 2.50 (2.20–2.75) |
| Attributable death/100 deaths | 0 | 55.4 (50.0–60.3) | 38.3 (31.5–44.1) | 64.3 (56.5–70.7) |
| Cancer deaths (n = 1396) | ||||
| No. of deaths (%) | 918 (2.4) | 89 (3.0) | 363 (4.6) | 26 (4.7) |
| Crude rate of death/105 person-years | 219 | 298 | 456 | 537 |
| Adjusted HR | 1 | 1.36 (1.09–1.70) | 1.34 (1.17–1.54) | 1.83 (1.23–2.72) |
| PAF (%) | 0 | 1.69 (0.53–2.63) | 6.60 (3.78–9.12) | 0.84 (0.35–1.18) |
| Attributable death/100 deaths | 0 | 26.5 (8.3–41.2) | 25.4 (14.5–35.1) | 45.4 (18.7–63.2) |
| Other causes (n = 2050) | ||||
| No. of deaths (%) | 1145 (3.0) | 203 (6.8) | 635 (8.0) | 67 (12.2) |
| Crude rate of death/105 person-years | 273 | 680 | 798 | 1384 |
| Adjusted HR | 1 | 2.45 (2.10–2.86) | 1.85 (1.66–2.07) | 3.48 (2.71–4.48) |
| PAF (%) | 0 | 5.86 (5.19–6.44) | 14.23 (12.32–16.01) | 2.33 (2.06–2.54) |
| Attributable death/100 deaths | 0 | 59.2 (52.4–65.0) | 45.9 (39.8–51.7) | 71.3 (63.1–77.7) |
DM, diabetes mellitus.
DM-, Opiate-, non-diabetic non-opiate users; DM+, Opiate-, diabetic non-opiate users; DM-, Opiate+, non-diabetic opiate users; DM+, Opiate+, diabetic opiate users; HR, hazard ratio; PAF, population-attributable fraction. HR (95% confidence interval) calculated using Cox regression models with age as the time scale, adjusted for age at enrolment, sex, ethnicity, marital status, education, residence, wealth score, cigarette smoking, alcohol drinking, body mass index, hypertension, history of ischaemic heart diseases, history of stroke, history of cancers, physical activity, vegetable/fruit consumption. PAF (%) calculated as (number of subgroup deaths × 100/total deaths) × (HR-1)/HR. Attributable (preventable) deaths/100 deaths, in each group, calculated as PAF × total deaths × 100/ number of subgroup deaths.
Table 3.
Associations of opiate use with mortality in diabetic and non-diabetic participants; sensitivity and subgroup analyses
| Diabetic participants |
Non-diabetic participants |
|||
|---|---|---|---|---|
| HR1 | HR2 | HR1 | HR2 | |
| All-cause mortality | ||||
| Alla | 1.80 (1.55–2.09) | 1.34 (1.13–1.58) | 2.21 (2.10–2.34) | 1.63 (1.53–1.73) |
| Exclusion of chronic diseasesb | 1.92 (1.60–2.29) | 1.41 (1.15–1.72) | 2.27 (2.14–2.41) | 1.68 (1.57–1.79) |
| Further exclusion of the first 2 years of follow-up | 1.75 (1.44–2.13) | 1.36 (1.09–1.69) | 2.21 (2.08–2.35) | 1.68 (1.57–1.81) |
| Exclusion of ever tobacco users and ever alcohol drinkers | 1.81 (1.48–2.23) | 1.43 (1.16–1.77) | 1.95 (1.78–2.14) | 1.71 (1.55–1.88) |
| Further exclusion of the lowest tertile of fruit/vegetable use | 1.89 (1.48–2.42) | 1.44 (1.11–1.86) | 2.09 (1.85–2.35) | 1.80 (1.59–2.03) |
| Opiate use status | ||||
| Ex-users | 1.33 (0.92–1.91) | 1.06 (0.72–1.55) | 1.71 (1.49–1.96) | 1.33 (1.15–1.52) |
| Current users | 1.91 (1.63–2.24) | 1.39 (1.17–1.66) | 2.30 (2.18–2.44) | 1.68 (1.57–1.79) |
| Daily dose | ||||
| <0.6 g | 1.73 (1.46–2.05) | 1.31 (1.08–1.57) | 2.11 (1.98–2.25) | 1.60 (1.49–1.71) |
| >=0.6 g | 2.01 (1.55–2.62)c | 1.44 (1.08–1.91)c | 2.45 (2.25–2.66)c | 1.69 (1.54–1.85)c |
| Route of current use | ||||
| Only smoke | 1.84 (1.53–2.22) | 1.41 (1.15–1.73) | 2.01 (1.87–2.16) | 1.51 (1.40–1.64) |
| Only oral | 2.10 (1.59–2.76) | 1.37 (1.02–1.82) | 2.76 (2.55–2.98) | 1.95 (1.79–2.12) |
| Sex | ||||
| Women | 1.94 (1.54–2.44) | 1.39 (1.08–1.78) | 2.40 (2.17–2.65) | 1.87 (1.68–2.08) |
| Men | 1.40 (1.14–1.73) | 1.26 (1.00–1.60) | 1.84 (1.72–1.96) | 1.50 (1.39–1.62) |
| Age at enrolment | ||||
| <50 years | 2.51 (1.79–3.50) | 1.50 (1.01–2.22) | 2.75 (2.44–3.10) | 1.70 (1.47–1.97) |
| >=50 years | 1.67 (1.41–1.97) | 1.28 (1.06–1.55) | 2.10 (1.97–2.23) | 1.60 (1.49–1.72) |
| Tobacco use | ||||
| Ever tobacco users | 1.37 (1.05–1.80) | 1.10 (0.81–1.50) | 1.63 (1.50–1.77) | 1.44 (1.31–1.57) |
| Never tobacco users | 1.78 (1.45–2.18) | 1.43 (1.16–1.76) | 1.96 (1.79–2.15) | 1.71 (1.55–1.88) |
| Causes of death | ||||
| Cardiovasculara | 1.81 (1.47–2.24) | 1.38 (1.09–1.74) | 2.07 (1.89–2.26) | 1.61 (1.45–1.78) |
| Cancera | 1.80 (1.16–2.79) | 0.96 (0.58–1.58) | 1.93 (1.71–2.18) | 1.38 (1.19–1.58) |
| Othersa | 2.05 (1.55–2.70) | 1.61 (1.18–2.19) | 2.70 (2.45–2.97) | 1.83 (1.63–2.05) |
Data are hazard ratios (95% confidence intervals) with age as the time scale, and non-opiate users as the reference category. HR1, crude hazard ratio; HR2, hazard ratio adjusted for age at enrolment, sex, ethnicity, marital status, education, residence, wealth score, cigarette smoking, alcohol drinking, body mass index, hypertension, history of ischaemic heart diseases, history of stroke, history of cancers, physical activity, vegetable/fruit consumption, if applicable.
P for interaction for HR1 and HR2 were 0.008 and 0.002 for all-cause mortality; 0.226 and 0.028 for cardiovascular mortality; 0.782 and 0.990 for cancer mortality; and 0.056 and 0.076 for other causes of death, respectively.
History of ischaemic heart disease, stroke, cancers at baseline.
P for trend <0.01, based on median of categories.
Table 2 shows the adjusted HRs, PAFs and numbers of attributable deaths in four categories of participants, based on baseline diabetes diagnosis and opiate use, and Figure 1 shows survival curves for these four categories. Compared with individuals who did not have diabetes and did not use opiates, people with a diabetes diagnosis but no opiate use had more than double the adjusted risk of premature mortality (HR = 2.17; 95% CI: 2.00–2.35). In opiate users without diabetes, the HR was 1.63 (95% CI: 1.53–1.74) and in opiate users with diabetes, this rate increased further to 2.76 (95% CI: 2.40–3.17). Table 2 also shows death rates (per 100 000) in each group, which increased from 997 in non-diabetic non-opiate users, to 2536 in diabetic participants, 2395 in opiate users, and 4524 in diabetic participants who used opiates. As a result, among those who both had diabetes and used opiates, 63.8% (95% CI: 58.3%–68.5%) of all deaths were attributable to these risk factors, compared with 53.9% (95% CI: 50%–57.4%) of deaths in people who only had diabetes, and 38.7% (95% CI: 34.6%–42.5%) in non-diabetic participants who used opiates. A large proportion of cardiovascular deaths was attributable to diabetes (with or without opiate use), whereas for cancer deaths, diabetes and opiates seemed to have similar attributable proportions.
Figure 1.
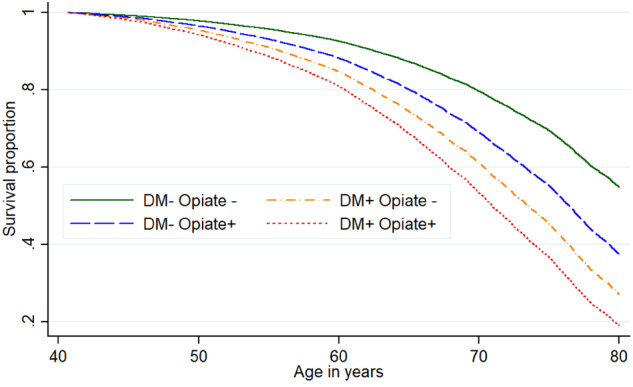
Survival of the participants in the Golestan Cohort Study. The curves are based on Cox regression models adjusted for age at enrolment, sex, ethnicity, marital status, education, residence, wealth score, cigarette smoking, alcohol drinking, body mass index, hypertension, history of ischaemic heart disease, history of stroke, history of cancers, physical activity and vegetable/fruit consumption. DM, diabetes mellitus; DM- Opiate-, non-diabetic individuals who did not use opiates; DM+ Opiate-, diabetic patients who did not use opiates; DM- Opiate+, non-diabetic individuals who used opiates; and DM+ opiate+, diabetic patients who used opiates
Table 3 further explores the association of opiate use with mortality among diabetic and non-diabetic groups. Opiate use was positively associated with all-cause mortality among both diabetic and non-diabetic participants, with adjusted HRs (95% CI) of 1.34 (1.13–1.58) and 1.63 (1.53–1.73), respectively. These associations changed little after stepwise exclusion of: participants with chronic diseases; the first 2 years of follow-up; those with tobacco and alcohol use; and those with low intake of fruits and vegetables. The associations were stronger in both diabetic and non-diabetic participants who never used tobacco products. There was an increase in mortality risk by the average dose of opiate used (P for trend <0.01 in both diabetic and non-diabetic participants). Subgroup analyses revealed that the associations between opiate consumption with mortality were consistent in both sexes and across age groups. Compared with cancer death, cardiovascular mortality was more strongly associated with opiate use.
Finally, we stratified the patients with diabetes into those who started opiate use after or in the same year of diabetes diagnosis (n = 268) and those who used opiates before the diagnosis of diabetes (n = 271), and compared each stratum with diabetic participants without a history of opiate use (n = 2997). Opiate use after diabetes diagnosis was associated with an increased risk of mortality [crude and adjusted HRs (95% CIs) of 1.79 (1.46–2.20) and 1.36 (1.09–1.69), respectively]. The proportion of deaths attributed to opiate use after diabetes diagnosis was 26.5% (95% CI: 0–40.9), in the adjusted model. HRs (95% CIs) of association between opiate use and mortality in diabetic participants who already used opiates before diagnosis with diabetes, compared with diabetic non-opiate users, were similar [HR = 1.78 (95% CI: 1.46–2.17) and HR = 1.28 (95% CI: 1.03–1.60), in crude and adjusted models, respectively], with an attributable death proportion of 21.9% (95% CI: 2.9–37.5) in the adjusted model.
Discussion
Patients with diabetes who took opiates were at increased risk of early mortality compared with all other groups, including diabetic participants who did not use opiates. The risk of early mortality in known cases of diabetes did not depend on whether they started opiate use before or after their diabetes diagnosis. Opiate use also showed a dose-dependent association with increased mortality rate in both diabetic and non-diabetic participants. These associations were present in both sexes, younger and older ages, after exclusion of participants with chronic diseases and the first 2 years of follow-up and after exclusion of those with tobacco and alcohol use and those with low intake of fruits and vegetables.
Diabetes increases the risk of mortality from cardiovascular diseases, cancers and other causes2,28 and this excess risk largely depends on the quality of diabetes care.22,29 For example, in high-income countries, diabetes less than doubles the rate of all-cause mortality,28 whereas in Mexico, a middle-income country, this excess risk is almost 4-fold.22 In our study, diabetes increased the risk of early death more than twice, and we showed that this risk was further aggravated by opiate use. The fact that diabetic patients who take opiates are at even higher risk of mortality has an important public health message, especially for places where opiates are widely available and sometimes may even be recommended to diabetic patients. A study from Isfahan, Iran, indicated that 32% (911 out of 2854) of urban adults believed that opium decreases blood sugar.30 In another study, 78.3% of addicted participants believed that opiates have beneficial effects on glycaemic control.31 Although we did not evaluate the attitudes of participants towards opiate effects on diabetes, almost 50% of diabetic patients who used opiates had started opiate misuse after or at the same time as their diabetes diagnosis. This may indicate that many at least did not consider opiates to be harmful to their disease.
Although opioid drugs are not the first- or second-line agents recommended in painful diabetic neuropathy, they are still among the drugs used for this condition.8 In places where non-prescription opiates are widely available, patients may use them as convenient alternative pain medications. The prevalence of painful diabetic neuropathy is estimated to be 10–25%,32,33 but there are studies which estimate that as many as 65% of diabetic adults may suffer from this complication.34 We had no data about painful diabetic neuropathy; however, studies from high-income countries showed high levels of unawareness35,36 and mismanagement,36–38 even in diabetes clinics.39 This is probably also true in low- and middle-income countries such as Iran. The analgesic property of opiates might mask the symptoms of painful complications such as diabetic neuropathy, diabetic foot or even angina pectoris, so these patients may delay seeking health care.12
Potential mechanisms that may link opiates with chronic diseases and death have been reported previously.12,19,40,41 Opiate users (even exclusive users who do not use tobacco) are exposed to high levels of toxicant and carcinogenic compounds. In a previous study using urinary biomarkers, opiate use was the main source of many metabolites of polycyclic aromatic hydrocarbons and volatile organic compounds. For example, the concentrations of phenanthrene and acrylamide metabolites were 2 to 5 times higher in the urine samples from exclusive opiate users compared with exclusive cigarette smokers, and 5–8 times higher compared with tobacco non-users. Many of the parent compounds for these metabolites are included in the Food and Drug Administration’s (FDA’s) list of Harmful and Potentially Harmful Constituents in Tobacco Products and Tobacco Smoke for their carcinogenicity or respiratory or cardiac toxicity.42 In addition to these mechanisms, long-term opiate use may have specific effects on glycaemic control, and diabetic complications. Morphine and insulin can activate similar signalling cascades, because of a direct cross-talk between downstream signalling pathways of the mu-opioid receptors and insulin receptors.43 Thus, morphine can induce desensitization of insulin receptor signalling.43 Long-term opioid administration may also induce insulin resistance via the induction of hypogonadism in both sexes, mediated mainly by inhibiting hypothalamic gonadotropin-releasing hormone secretion.44 For example in men, long-term opioid use, regardless of the administration route, can lead to a very high prevalence (85–90%) of hypogonadism44 and subsequently a higher risk of insulin resistance and metabolic syndrome.44,45 The chronic use of opiates in diabetic patients can also lead to the development of substance use disorders,14 a dangerous and understudied combination,17 which can adversely influence self-management and diabetes care.12,16,17 For example, a retrospective cohort study of more than 900 000 diabetic patients receiving care in the US Department of Veterans Affairs showed that chronic opioid therapy (at least six prescriptions for opioids in a year) was associated with poorer diabetic care (i.e. lower frequency of testing haemoglobin A1C and cholesterol levels and fewer eye examinations), in a dose-dependent manner.16 In another retrospective cohort study among Massachusetts beneficiaries of Medicare and/or Medicaid, diabetic patients with drug use disorders had a higher risk of diabetes-related hospitalization and lower limb amputation.46
To our knowledge, this is the first prospective population-based study to investigate the joint effects of opiate use and diabetes on overall and cause-specific mortality. We adjusted our models for many covariates and confounders such as socioeconomic factors, physical activity and tobacco use. We also stratified the models in both diabetic and non-diabetic participants by important covariates to reduce the effect of residual confounding, particularly due to cigarette smoking, which highly correlates with opiate use. Based on our previous validation study,20 about 38% of diabetic participants were unaware of their condition, and were classified as non-diabetic participants, so the risks of diabetes-associated mortality in our study might be underestimated. Also, our estimates of the association between opiate use and mortality in patients with diabetes might be underestimated because the duration and amount of opiates used by this group were lower than those used by non-diabetic participants. In this study, opiate users had lower socioeconomic levels and higher prevalence of risk factors such as tobacco and alcohol use compared with non-users. Despite extensive adjustments for these potential confounders, residual confounding from these or other unmeasured confounders cannot be completely ruled out. However, these conditions are unlikely to completely explain high mortality rates among opiate users, because the results remained unchanged after several steps of sensitivity analysis excluding individuals with chronic diseases, tobacco use, alcohol use and poor diet. Finally, our population used special types of non-prescription, mainly natural, opiates. Further studies should be directed towards other types of opiates, and towards prescription opioids in type 2 diabetes.
Conclusions
Co-existence of opiate use and diabetes aggravated, overall, cardiovascular, cancer and other causes of mortality compared with each of these risk factors alone. Also opiates increased mortality equally in those who started taking them before or after the diagnosis of diabetes. Improving guideline adherence for detecting and treating neuropathy and psychological disorders in diabetic patients is recommended.
Implications
We showed that the increased mortality among diabetic patients is further increased by chronic use of opiates. Public awareness and better education of both medical staff members and diabetic patients about the health effects of opiate use is necessary. In clinics, more attention to diabetic complications such as neuropathy and psychological disorders is crucial, as they may be the underlying factors leading to opiate misuse in these patients.
Data accessibility
The datasets generated and/or analyed during the current study are not publicly available but are available from the corresponding author on reasonable request.
Supplementary data
Supplementary data are available at IJE online.
Funding
This work was supported by the National Institute for Medical Research Development (NIMAD, Elite Grant number: 977283), Tehran University of Medical Sciences (grant number: 81/15), Cancer Research UK (grant number: C20/A5860), the National Institute of General Medical Sciences/National Institutes of Health (grant number: UL1 GM118973) and in part by the National Cancer Institute/National Institutes of Health, Intramural Research Program, and various collaborative research agreements with International Agency for Research on Cancer. The funding sources had no role in study design, data collection, data analysis, data interpretation or writing of the report.
Supplementary Material
Acknowledgements
We thank the study participants and the Behvarzes for their long-term cooperation. We gratefully acknowledge Professor Barry I Graubard, from the Biostatistics Branch, Division of Cancer Epidemiology and Genetics, National Cancer Institute, for his thoughtful and helpful comments and suggestions. We also thank the local authorities, Golestan University of Medical Sciences officials, local physicians, elders and religious leaders as well as the general physicians, nurses and nutritionists in the enrolment teams for their collaboration.
Author contributions
Design of the study: M.N., F.K., P.Br., P.Bo., S.M.D., C.C.A., R.M., A.E.; data acquisition: H.P., A.P., G.R., M.K., S.G., M.Z., A.No., M.So., A.Ni., R.M., A.E.; data interpretation and analysis: M.N., M.K., F.K., M.Sh., A.E.; writing the manuscript: M.N., A.E.; all authors reviewed and commented on drafts, approved the final version to be published and agreed to be accountable for all aspects of the paper. R.M. is the guarantor.
Conflict of interest
None declared.
References
- 1.World Health Organization. Diabetes. 2018. http://www.who.int/en/news-room/fact-sheets/detail/diabetes (1 June 2019, date last accessed).
- 2. Zheng Y, Ley SH, Hu FB.. Global aetiology and epidemiology of type 2 diabetes mellitus and its complications. Nat Rev Endocrinol 2018;14:88–98. [DOI] [PubMed] [Google Scholar]
- 3.International Diabetes Federation. IDF Diabetes Atlas, Eighth Edition 2017. 2018. https://www.idf.org/aboutdiabetes/what-is-diabetes/facts-figures.html (1 June 2019, date last accessed). [PubMed]
- 4. Gregg EW, Cheng YJ, Srinivasan M. et al. Trends in cause-specific mortality among adults with and without diagnosed diabetes in the USA: an epidemiological analysis of linked national survey and vital statistics data. Lancet 2018;391:2430–40. [DOI] [PubMed] [Google Scholar]
- 5.National Academies of Sciences, Engineering, and Medicine. Pain Management and the Opioid Epidemic: Balancing Societal and Individual Benefits and Risks of Prescription Opioid Use. Washington, DC: National Academies Press, 2017. [PubMed] [Google Scholar]
- 6. Helmstadter A. Antidiabetic drugs used in Europe prior to the discovery of insulin. Pharmazie 2007;62:717–20. [PubMed] [Google Scholar]
- 7.United Nations Organization. World Drug Report (United Nations publication, Sales No. E.19.XI.8). New York, NY: UNO, 2019.
- 8. Pop-Busui R, Boulton AJ, Feldman EL. et al. Diabetic neuropathy: a position statement by the American Diabetes Association. Diabetes Care 2017;40:136–54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Patil PR, Wolfe J, Said Q, Thomas J, Martin BC.. Opioid use in the management of diabetic peripheral neuropathy (DPN) in a large commercially insured population. Clin J Pain 2015;31:414–24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Najafipour H, Beik A.. The impact of opium consumption on blood glucose, serum lipids and blood pressure, and related mechanisms. Front Physiol 2016;7:436. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Ceriello A, Giugliano D, Quatraro A, Russo PD, Torella R.. Blood glucose may condition factor VII levels in diabetic and normal subjects. Metab Regul Diabetol 1988;31:3–15. [DOI] [PubMed] [Google Scholar]
- 12. Masoudkabir F, Sarrafzadegan N, Eisenberg MJ.. Effects of opium consumption on cardiometabolic diseases. Nat Rev Cardiol 2013;10:733–40. [DOI] [PubMed] [Google Scholar]
- 13. Kalant H. Opium revisited: a brief review of its nature, composition, non-medical use and relative risks. Addiction 1997;92:267–77. [PubMed] [Google Scholar]
- 14. Wu L-T, Ghitza UE, Batch BC. et al. Substance use and mental diagnoses among adults with and without type 2 diabetes: results from electronic health records data. Drug Alcohol Depend 2015;156:162–69. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Najafipour H, Sanjari M, Shokoohi M. et al. Epidemiology of diabetes mellitus, pre-diabetes, undiagnosed and uncontrolled diabetes and its predictors in general population aged 15 to 75 years: a community-based study (KERCADRS) in southeastern Iran. J Diabetes 2015;7:613–21. [DOI] [PubMed] [Google Scholar]
- 16. Rose AJ, Hermos JA, Frayne SM, Pogach LM, Berlowitz DR, Miller DR.. Does opioid therapy affect quality of care for diabetes mellitus? Am J Manag Care 2009;15:217–24. [PubMed] [Google Scholar]
- 17. Walter KN, Wagner JA, Cengiz E, Tamborlane WV, Petry NM.. Substance use disorders among patients with type 2 diabetes: a dangerous but understudied combination. Curr Diab Rep 2017;17:2. [DOI] [PubMed] [Google Scholar]
- 18. Sadeghian S, Graili P, Salarifar M, Karimi AA, Darvish S, Abbasi SH.. Opium consumption in men and diabetes mellitus in women are the most important risk factors of premature coronary artery disease in Iran. Int J Cardiol 2010;141:116–18. [DOI] [PubMed] [Google Scholar]
- 19. Khademi H, Malekzadeh R, Pourshams A. et al. Opium use and mortality in Golestan Cohort Study: prospective cohort study of 50,000 adults in Iran. BMJ 2012;344:e2502. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Golozar A, Khademi H, Kamangar F. et al. Diabetes mellitus and its correlates in an Iranian adult population. PLoS One 2011;6:e26725. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Pourshams A, Khademi H, Malekshah AF. et al. Cohort Profile: The Golestan Cohort Study—a prospective study of oesophageal cancer in northern Iran. Int J Epidemiol 2010;39:52–59. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Alegre-Diaz J, Herrington W, Lopez-Cervantes M. et al. Diabetes and cause-specific mortality in Mexico City. N Engl J Med 2016;375:1961–71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Abnet CC, Saadatian-Elahi M, Pourshams A. et al. Reliability and validity of opiate use self-report in a population at high risk for esophageal cancer in Golestan, Iran. Cancer Epidemiol Biomarkers Prev 2004;13:1068–70. [PubMed] [Google Scholar]
- 24. Malekshah AF, Kimiagar M, Saadatian-Elahi M. et al. Validity and reliability of a new food frequency questionnaire compared to 24 h recalls and biochemical measurements: pilot phase of Golestan cohort study of esophageal cancer. Eur J Clin Nutr 2006;60:971–77. [DOI] [PubMed] [Google Scholar]
- 25. Islami F, Kamangar F, Nasrollahzadeh D. et al. Socio-economic status and oesophageal cancer: results from a population-based case-control study in a high-risk area. Int J Epidemiol 2009;38:978–88. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Khademi H, Etemadi A, Kamangar F. et al. Verbal autopsy: reliability and validity estimates for causes of death in the Golestan Cohort Study in Iran. PLoS One 2010;5:e11183. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Rockhill B, Newman B, Weinberg C.. Use and misuse of population attributable fractions. Am J Public Health 1998;88:15–19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Rao Kondapally Seshasai S, Kaptoge S, Thompson A. et al. Diabetes mellitus, fasting glucose, and risk of cause-specific death. N Engl J Med 2011;364:829–41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Rawshani A, Rawshani A, Franzen S. et al. Risk factors, mortality, and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med 2018;379:633–44. [DOI] [PubMed] [Google Scholar]
- 30. Roohafza H, Talaei M, Sadeghi M, Haghani P, Shokouh P, Sarrafzadegan N.. Opium decreases the age at myocardial infarction and sudden cardiac death: a long- and short-term outcome evaluation. Arch Iran Med 2013;16:154–60. [PubMed] [Google Scholar]
- 31. Azod L, Rashidi M, Afkhami-Ardekani M, Kiani G, Khoshkam F.. Effect of opium addiction on diabetes. Am J Drug Alcohol Abuse 2008;34:383–88. [DOI] [PubMed] [Google Scholar]
- 32. Vinik AI. Clinical practice, diabetic sensory and motor neuropathy. N Engl J Med 2016;374:1455–64. [DOI] [PubMed] [Google Scholar]
- 33. Ziegler D, Fonseca V.. From guideline to patient: a review of recent recommendations for pharmacotherapy of painful diabetic neuropathy. J Diabetes Complications 2015;29:146–56. [DOI] [PubMed] [Google Scholar]
- 34. Halawa MR, Karawagh A, Zeidan A, Mahmoud AE, Sakr M, Hegazy A.. Prevalence of painful diabetic peripheral neuropathy among patients suffering from diabetes mellitus in Saudi Arabia. Curr Med Res Opin 2010;26:337–43. [DOI] [PubMed] [Google Scholar]
- 35. Veresiu AI, Bondor CI, Florea B, Vinik EJ, Vinik AI, Gâvan NA.. Detection of undisclosed neuropathy and assessment of its impact on quality of life: a survey in 25,000 Romanian patients with diabetes. J Diabetes Complications 2015;29:644–49. [DOI] [PubMed] [Google Scholar]
- 36. Daousi C, MacFarlane IA, Woodward A, Nurmikko TJ, Bundred PE, Benbow SJ.. Chronic painful peripheral neuropathy in an urban community: a controlled comparison of people with and without diabetes. Diabet Med 2004;21:976–82. [DOI] [PubMed] [Google Scholar]
- 37. Gore M, Dukes E, Rowbotham DJ, Tai KS, Leslie D.. Clinical characteristics and pain management among patients with painful peripheral neuropathic disorders in general practice settings. Eur J Pain 2007;11:652–64. [DOI] [PubMed] [Google Scholar]
- 38. Yang M, Qian C, Liu Y.. Suboptimal treatment of diabetic peripheral neuropathic pain in the United States. Pain Med 2015;16:2075–83. [DOI] [PubMed] [Google Scholar]
- 39. Van Acker K, Bouhassira D, De Bacquer D. et al. Prevalence and impact on quality of life of peripheral neuropathy with or without neuropathic pain in type 1 and type 2 diabetic patients attending hospital outpatients clinics. Diabetes Metab 2009;35:206–13. [DOI] [PubMed] [Google Scholar]
- 40. Kamangar F, Shakeri R, Malekzadeh R, Islami F.. Opium use: an emerging risk factor for cancer?. Lancet Oncol 2014;15:e69–77. [DOI] [PubMed] [Google Scholar]
- 41. Khademi H, Kamangar F, Brennan P, Malekzadeh R.. Opioid therapy and its side effects: a review. Arch Iran Med 2016;19:870–76. [DOI] [PubMed] [Google Scholar]
- 42. Etemadi A, Poustchi H, Calafat AM. et al. Opiate and tobacco use and exposure to carcinogens and toxicants in the Golestan Cohort Study. Cancer Epidemiol Biomarkers Prev 2020;29:650–58. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Li Y, Eitan S, Wu J. et al. Morphine induces desensitization of insulin receptor signaling. Mol Cell Biol 2003;23:6255–66. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44. Vuong C, Van Uum SH, O'Dell LE, Lutfy K, Friedman TC.. The effects of opioids and opioid analogs on animal and human endocrine systems. Endocr Rev 2010;31:98–132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45. Gevi F, Fanelli G, Zolla L.. Metabolic patterns in insulin-resistant male hypogonadism. Cell Death Dis 2018;9:671. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46. Leung G, Zhang J, Lin WC, Clark RE.. Behavioral disorders and diabetes-related outcomes among Massachusetts Medicare and Medicaid beneficiaries. Psychiatr Serv 2011;62:659–65. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
The datasets generated and/or analyed during the current study are not publicly available but are available from the corresponding author on reasonable request.