
Figure 1.
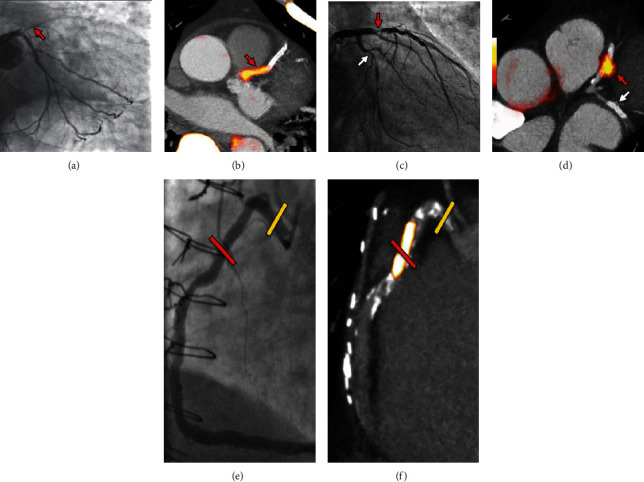
Focal 18F-NaF in patients with myocardial infarction and stable angina. A patient with acute ST-segment elevation myocardial infarction with (a) proximal occlusion (red arrow) of the left anterior descending artery on invasive coronary angiography and (b) intense focal 18F-NaF (tissue-to-background ratios, culprit 2.27 vs. reference segment 1.09 (108% increase)) uptake (yellow-red) at the site of the culprit plaque (red arrow) on the combined PET and CT. A patient with anterior non-ST-segment elevation MI with (c) culprit (red arrow; left anterior descending artery) and bystander nonculprit (white arrow; circumflex artery) lesions on invasive coronary angiography that were both stented during the index admission. Only the culprit lesion had increased 18F-NaF uptake (tissue-to-background ratios, culprit 2.03 vs. reference segment 1.08 (88% increase)) on PET-CT (d) after percutaneous coronary intervention. In a patient with stable angina with previous coronary artery bypass grafting, (e) invasive coronary angiography showed nonobstructive disease in the right coronary artery. (f) Corresponding PET-CT scan showed a region of increased 18F-NaF activity (positive lesion, red line) in the midright coronary artery (tissue-to-background ratio, 3.13) and a region without increased uptake in the proximal vessel (negative lesion, yellow line). This figure was originally published in the Lancet under the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/) (data from Joshi et al. [20]).