
Fig. 1.
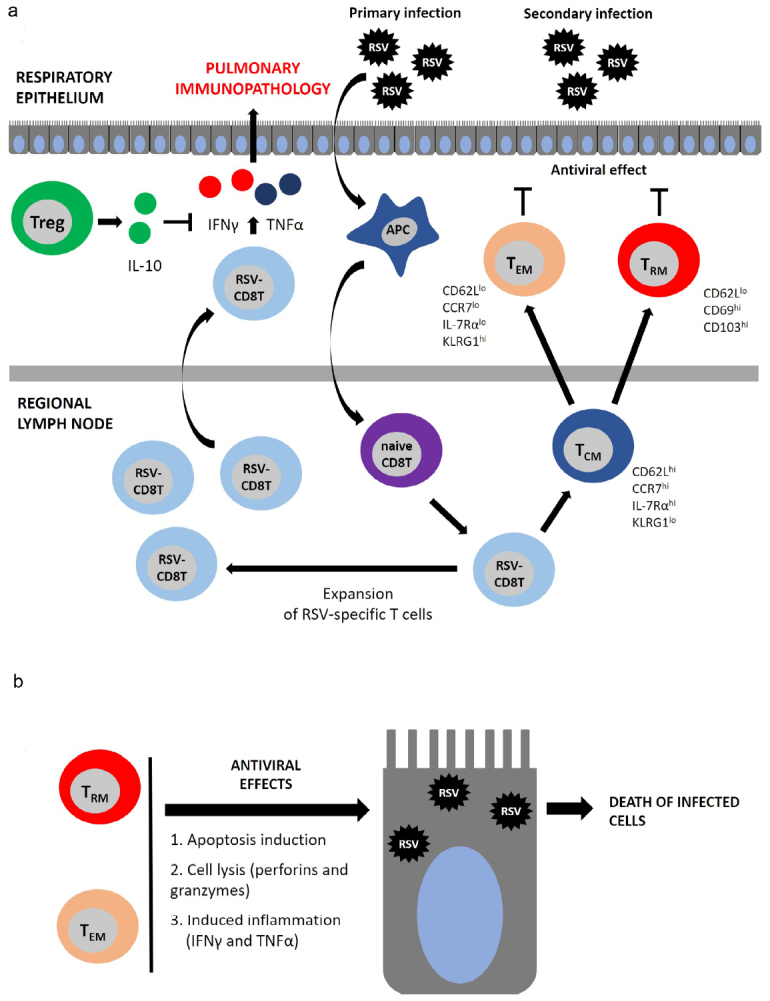
The role of T cells in the antiviral defense and pulmonary immunopathology. a) CD8 T cell-mediated response develops after primary RSV infection. Viral antigens are presented by the antigen-presenting cells (APCs), most commonly, by DCs. Naïve CD8 T cells (naive CD8 T) become activated and differentiate into RSV-specific CD8 T cells (RSV-CD8 T), which then proliferate peaking on days 8-10 post-infection. RSV-CD8 T cells produce large amounts of pro-inflammatory cytokines IFNγ and TNFα, which mediate pulmonary immunopathology. After reaching the plateau, the number of RSV-CD8 T cells declines and they give rise to the memory T cells represented by several phenotypic subsets: 1) TCM – central memory T cells (CD62Lhi/CCR7hi/IL-7Rαhi/KLRG1l°) circulate in the bloodstream and accumulate in the secondary lymphoid tissues; 2) TEM – effector memory T cells (CD62Ll°/CCR7l°/IL-7Rαl°/KLRG1hi) are mainly located in the lungs, but can circulate in the bloodstream; 3) TRM – tissue-resident memory T cells (CD62Ll°/CD69hi/CD103hi) are found solely in the lungs and are unable to exit into the circulation. b) TEM and TRM exert protective antiviral response by triggering apoptosis and direct lysis of infected cells.