
Figure 3.
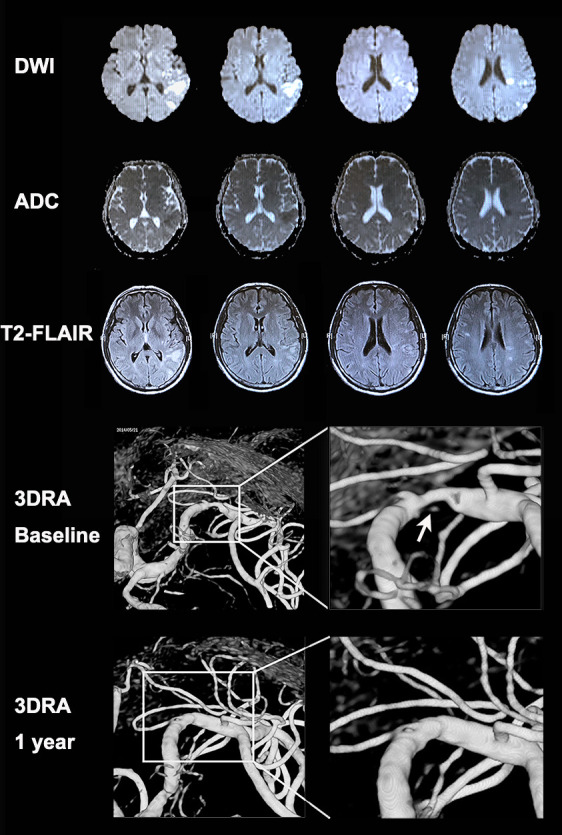
MRI and 3DRA images of a patient with an ulcerative MCA-M1 plaque and coexisting acute and chronic infarcts in cortical and subcortical regions. A patient with a history of hypertension presented with sudden onset of expressive dysphasia. The MRI exam conducted 1 day after symptom onset showed a cluster of early infarcts (high signal in DWI and low signal in apparent diffusion coefficient maps) at left posterior corona radiata (internal borderzone) and left temporal–parietal cortical and subcortical regions (including the posterior borderzone). There were also older small infarcts (high signal in T2 fluid-attenuated inversion recovery imaging and iso-intensity signal in apparent diffusion coefficient maps) in the same regions. The 3DRA exam conducted 4 weeks after the index stroke showed 80% stenosis of the left MCA-M1 with an ulcer in the plaque surface, that is, contrast appearing beneath the surface outline of the plaque (arrow). The patient received aspirin and clopidogrel treatment for 4 weeks since admission followed by lifelong aspirin treatment, in conjunction with stringent vascular risk factor control. The patient had no recurrent ischaemic stroke within 1 year after the index stroke. A repeated 3DRA exam at 1 year showed healing of the previously ulcerated MCA-M1 plaque. 3DRA, 3-dimensional rotational angiography; DWI, diffusion-weighted imaging; MCA-M1, M1 middle cerebral artery.