
Fig 3.
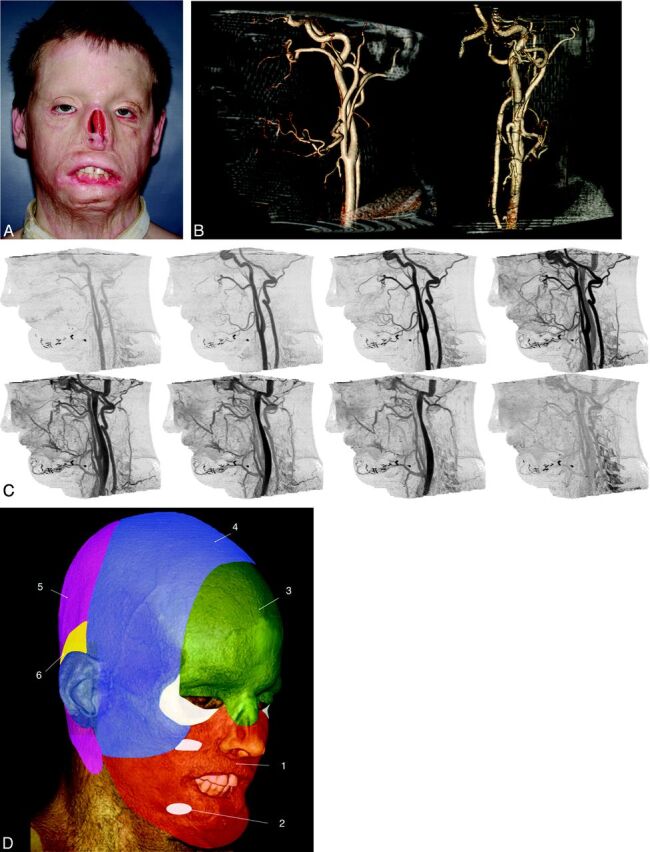
Candidate for full face transplantation. A, After a high-voltage injury, several flap and graft procedures resulted in persistent disfigurement. The patient wore a nasal prosthesis, removed for this photograph. B, Representative sagittal (left) and anteroposterior (right) projections from CT volume rendering. Volumes are viewed from an arbitrary angle to characterize branch and smaller vessels—for example, those from the external carotid artery that may be available for anastomoses. The nasal prosthesis was included in the CT acquisition. C, Sagittal cine CT images provide time resolution and enable separation of arteries and veins so that each dataset can be individually postprocessed. D, Angiosomes of the face overlaid on a volume-rendered CT image, including all soft-tissue components and numbered according to the source artery: 1) facial, 2) internal maxillary, 3) ophthalmic and internal carotid, 4) superficial temporal, 5) vertebral, and 6) posterior auricular. Lower and midface (orange) allografts can be perfused solely by facial arteries. Although the lower two-thirds of the face includes internal maxillary artery angiosomes, this territory can also be perfused by the facial artery via neighboring angiosome collateral vessels. For procedures in which the allograft includes the upper face and scalp (green and blue), the facial and superficial temporal arteries should be included, with the external carotid artery as the source vessel.