
Fig 4.
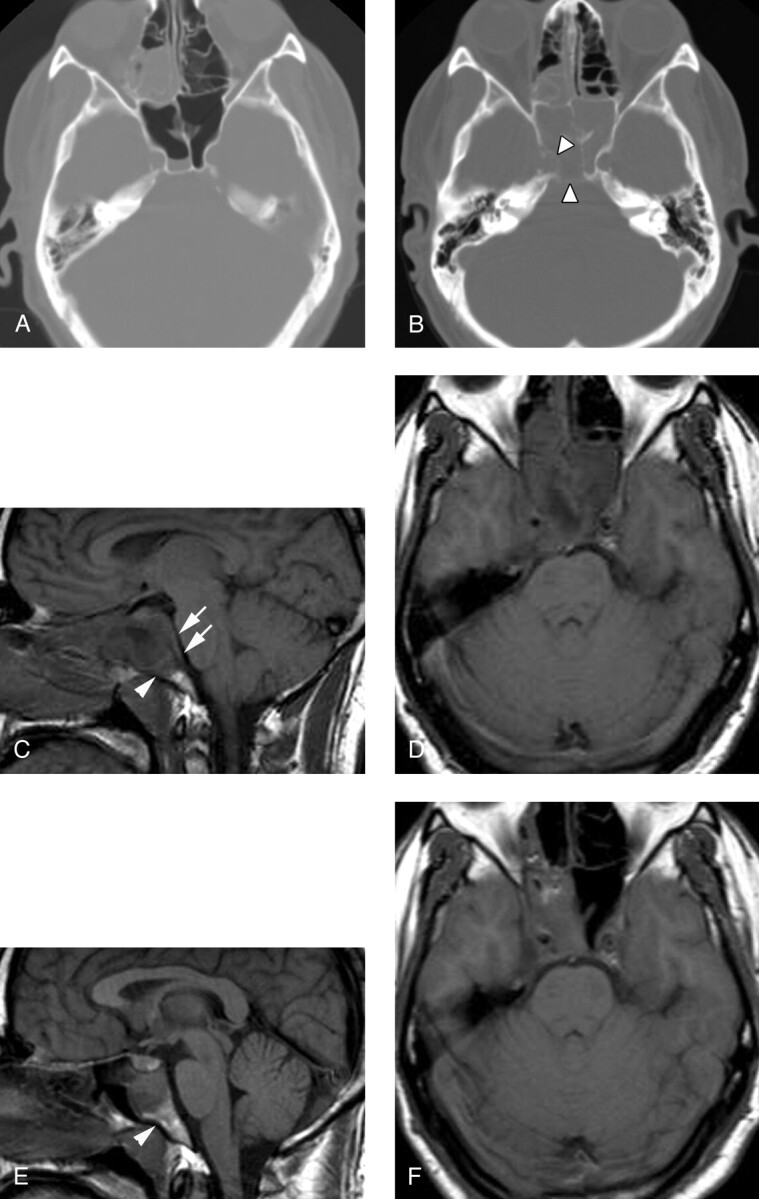
Patient 5, a 33-year-old man presenting with severe headache and sinus congestion.
A, Unenhanced axial CT image (bone window) demonstrates mucosal thickening in the right ethmoid sinus and an air-fluid level in the right sphenoid sinus. The bony walls of the sphenoid sinus are normal. Diagnosis of acute-on-chronic sinusitis was made and Septra and a decongestant were prescribed for the patient.
B, Three weeks later, the patient returned with continued headache and new diplopia on right lateral gaze. Unenhanced axial CT image (bone window) demonstrates segmental erosion of the bony wall of a completely opacified sphenoid sinus (arrowheads).
C, Sagittal T1-weighted spin-echo image (600/11/2) demonstrates abnormal hypointense signal intensity in the upper clivus (arrowhead) and thickening of the retroclival dura (arrows). The sphenoid sinus is filled with fluid and soft tissue.
D, Axial T1-weighted image (600/11/2) demonstrates abnormal soft tissue in the right cavernous sinus, with preservation of the right carotid flow void. Abnormal clival hypointensity is present, as is extensive inflammatory disease of the sphenoid and posterior ethmoid sinuses.
E, Sagittal T1-weighted spin-echo image (600/11/2) after 1 month of intravenous antibiotic therapy demonstrates normalization of signal intensity in the clivus (arrowhead), as well as a reduction in inflammatory sinus disease and resolution of the retroclival dural thickening.
F, Axial T1-weighted spin-echo image (600/11/2) from the same follow-up examination also demonstrates improvement in sinus disease. Abnormal soft tissue persists in the right cavernous sinus but is reduced in volume. The patient’s CN VI palsy had resolved by the time of this follow-up examination.