
Fig 1.
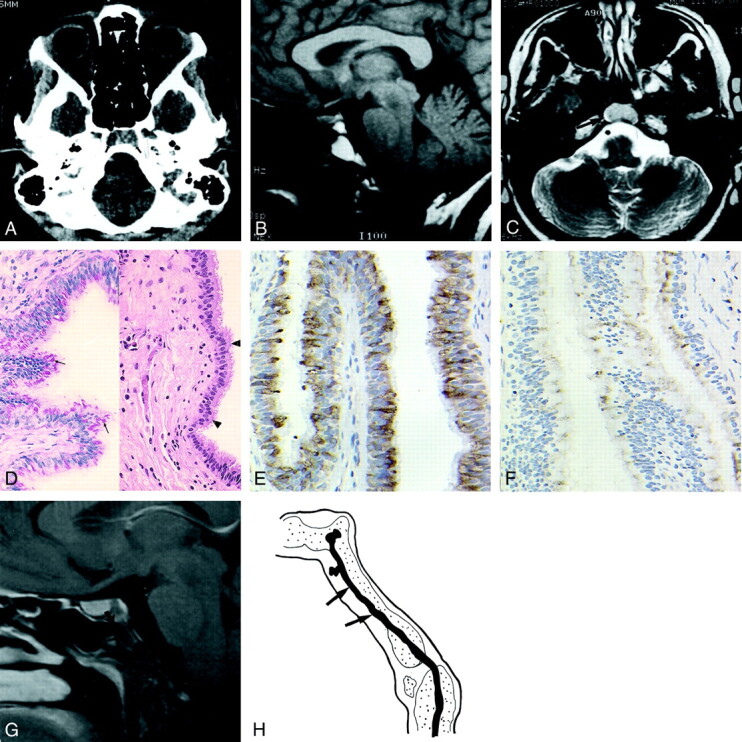
Images obtained in a 28-year-old woman who presented with left-sided frontotemporal headache lasting 6 wk.
A, Axial CT scan of the skull base shows a lytic lesion in the clivus, with no cortical break (arrows). No calcification is seen within the lesion.
B, Sagittal T1-weighted (500/14) image of the brain shows a mass (arrow) in the clivus that is hyperintense relative to the gray matter. The pituitary (arrowhead) is separate from the lesion.
C, Axial T2-weighted (6000/98) obtained at the level of the skull base shows that the lesion (arrow) is isointense to the gray matter.
D, Photomicrographs show the cyst lining composed of a pseudostratified (arrowheads) ciliated columnar epithelium (right image; hematoxylin-eosin, original magnification ×100) and cytoplasmic mucin and Goblet cells (arrows in left image; PASD, original magnification ×100).
E, Photomicrograph shows strong positive immunohistochemical staining within the lining epithelium (EMA, original magnification ×200).
F, Photomicrograph shows focal positive immunohistochemical staining within the lining epithelium (monoclonal CEA, original magnification ×200).
G, Sagittal contrast-enhanced T1-weighted brain MR (615/12) image obtained at 1-y follow-up shows a typical surgical defect in the anterior wall of the clivus (arrow), with no recurrence of the cyst.
H, Sagittal view through the clivus at approximately 3 wk of embryonic development shows the notochord (arrows), which obliquely traverses the occipital plate.