
FIG 1.
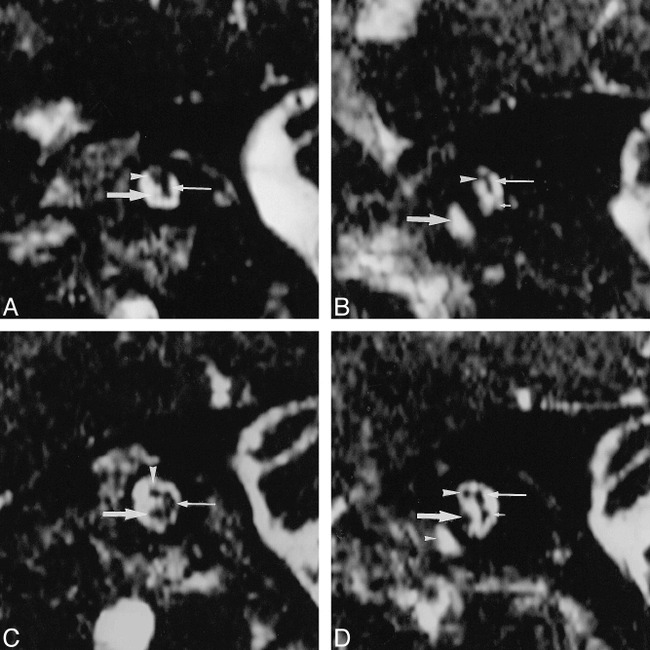
Images from the case of a 12-year-old female patient who presented at our institute with unilateral hearing impairment.
A, Abnormal left ear. Parasagittal 3DFT-CISS (12.3/5.9/1; flip angle, 70°) reconstruction images obtained perpendicular to the IAC at the midportion in the affected left side. The facial nerve is depicted in the superior and anterior position in the IAC (arrowhead). The common vestibular nerve is identified (thin arrow). A thin cochlear branch arises (arrow) from the VCN.
B, Abnormal left ear. Parasagittal 3DFT-CISS reconstruction images obtained perpendicular to the IAC at the lateral portion. The common vestibular nerve (not identified on this image) divides into the superior vestibular branch (thin arrow) and the inferior vestibular branch (short arrow) (poorly visualized). The cochlear branch is not visualized. The IAC seems to be slightly narrow compared with that on the right side (see panel D). The facial nerve is identified (arrowhead). The basal turn of the cochlea is shown (arrow). The vestibular branches also seem to be small in comparison with those on the right side (see panel D). Any vestibular abnormality, however, could be detected in the patient.
C, Normal right ear. Parasagittal 3DFT-CISS (12.3/5.9/1; flip angle, 70°) reconstruction images obtained perpendicular to the IAC at the midportion in the normal right side. The cochlear branch (arrow) is larger than the facial nerve (arrowhead). The common vestibular nerve is shown (thin arrow).
D, Normal right ear. Parasagittal 3DFT-CISS reconstruction images obtained perpendicular to the IAC at the lateral portion. The common vestibular nerve divides into the superior vestibular branch (thin arrow) and the inferior vestibular branch (short arrow). The cochlear branch (arrow) is larger than the facial nerve (arrowhead). Small arrowhead, the cochlea.