

Abstract
BACKGROUND AND PURPOSE: In most children with conductive hearing loss, acquired otitis media and/or middle ear effusion are ultimately diagnosed. Congenital conductive hearing loss is a rare condition; absence of the oval window is an unusual pathogenesis for this type of hearing impairment and can be associated with an anomalous horizontal facial nerve canal. Our goal was to describe the imaging features of congenital absence of the oval window, to determine the frequency with which anomalous development of the horizontal facial nerve canal occurs, and to review the developmental error responsible for this malformation.
METHODS: Nine temporal bones in seven patients (5 to 36 years old) were found to have an inadequately formed oval window on high-resolution CT scans; seven ears showed complete lack of oval window formation, and two showed partial absence of the oval window. Records were reviewed for clinical information, and images were examined for associated anomalies.
RESULTS: Six of nine ears with abnormal oval window formation showed malposition of the horizontal facial nerve canal. In each of these, the canal was abnormally low, overlying the expected location of the oval window; three of the canals lacked a visible bony covering. Seven of the nine ears were found to have a dysplastic or absent stapes.
CONCLUSION: Congenital absence of the oval window can be diagnosed on CT studies. In the present series, this anomaly was associated with a grossly aberrant horizontal facial nerve canal in six of nine involved ears. Familiarity with the developmental sequence of oval window formation fosters an understanding of these anomalies. Preoperative recognition is important clinically, as a low facial nerve will block surgical access to the oval window and its presence will alter patient management.
Congenital absence of the oval window is an uncommon embryologic defect. This entity is characterized by the clinical presentation of maximal conductive hearing loss (60 dB) beginning at birth or in early childhood (1), the absence of antecedent inflammatory middle ear disease or persistence of the hearing loss despite maximal medical therapy, and insufficient oval window formation on high-resolution CT scans. Associated with this entity is an extraordinarily high prevalence of anomalous development and malposition of the horizontal facial nerve canal, which makes surgical correction difficult if not contraindicated. Congenital absence of the oval window and its associated abnormalities have been mentioned in the radiologic literature (2–4), but to our knowledge the imaging features have not been fully described.
We report nine ears (in seven patients) in which we found congenital absence of the oval window. We correlate this interesting anomaly with its embryologic derivation, and describe the important associated feature of anomalous facial nerve development. The role of surgical correction is discussed.
Methods
Between January 1, 1995, and December 31, 1998, 2413 high-resolution CT studies of the temporal bone were performed at two associated institutions. From these studies, seven patients were found to have congenital absence of the oval window; five with unilateral involvement and two with bilateral involvement. The patients, five male and two female, ranged in age from 5 to 36 years. Three of the patients were referred for imaging by an otologist as part of a workup for maximal conductive hearing loss and suspected ossicular malformation; two patients were undergoing evaluation for correction of microtia; and two patients were referred by general otolaryngologists for evaluation of conductive hearing loss. None of the adult patients could recall hearing normally from the affected ear, and there was no documentation of normal hearing in the children. Audiometry showed moderate to maximal conductive hearing loss in all patients. One patient, who had a mild-to-moderate sensorineural component to the hearing loss, was noted to have a dilated vestibular aqueduct.
Twenty-five temporal bone CT scans obtained in other patients were reviewed for comparison. These patients, 15 male and 10 female, 7 to 40 years old, were scanned for reasons other than congenital hearing loss. On the coronal scans, a vertical line was drawn from the anterior junction of the lateral and superior semicircular canal, and the relationship of the horizontal facial nerve canal to this line was noted. On the axial scans, the presence of both the anterior and posterior stapedial crura within the oval window was noted.
All scans were obtained in both the axial and direct coronal planes using 1-mm-thick slices at either 1.0- or 0.5-mm intervals. The axial plane scans were obtained parallel to the hard palate, corresponding to a −10° angulation to the canthomeatal baseline and providing optimal visualization of the stapes superstructure and oval window. The coronal plane scans were obtained with a maximal gantry tilt. Images were reconstructed retrospectively using a small field of view (9.6- to 10.0-cm diameter) centered on the cochlear promontory and processed with a bone or sharp imaging algorithm.
Results
Congenital absence of the oval window was diagnosed most readily on the coronal CT scans (see the Table). Coronal images best delineate the size and shape of the oval window as well as the course and integrity of the horizontal facial nerve canal (Fig 1A). Axial images also delineate the oval window and are most useful for assessing the status of the stapes superstructure (head and crura) (Fig 1B). Seven of the nine ears had complete osseous obliteration of the oval window. Bony prominence over the cochlear promontory and under the lateral semicircular canal produced a tapered configuration and a dimplelike depression on the medial wall of the middle ear at the center of the oval window region (Fig 2). One patient had incomplete tapering of the oval window, producing a residual 1-mm central opening (Fig 3). Another patient had flat ossification of the superior half of the oval window without tapering; this patient had complete oval window obliteration on the contralateral ear. These latter two patients were considered to have partial absence of the oval window.
CT features of congenital absence of the oval window
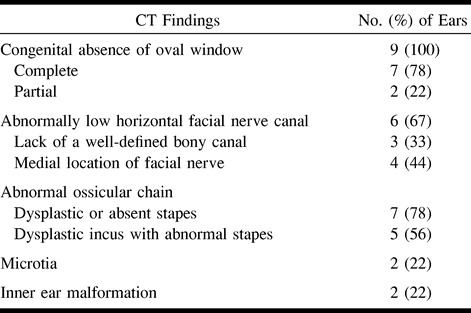
fig 1.
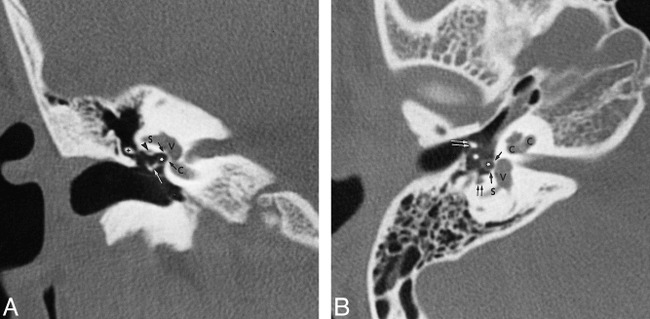
A and B, Normal anatomy of oval window on coronal (A) and axial (B) CT scans. V indicates vestibule; C, cochlea; S, lateral semicircular canal; single black arrows, margin of the oval window; asterisk, obturator foramen between stapes crura, well delineated on the axial scan; in A, arrowhead indicates horizontal facial nerve canal; cross, incudal body; single white arrow, incudal-stapedial articulation between the lenticular process and capitulum; in B, double black arrow indicates sinus tympani; double white arrow, neck of malleus. Posterior to the malleus lies the long process of the incus cut in cross section. Note that the facial nerve (arrowhead, A) is lateral to an imaginary vertical line drawn through the junction of the lateral and superior semicircular canals
fig 2.
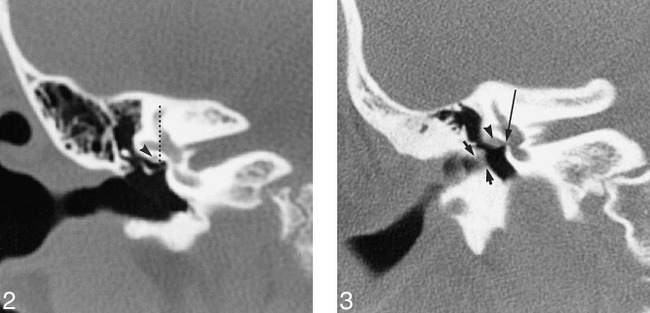
Congenital absence of the oval window, normal facial nerve canal, on coronal CT scan. The oval window is obliterated by a thick bony plate tapering to a central depression. The horizontal facial nerve canal, however, is normal in location (arrowhead), lying lateral to the vertical line drawn through the anterior junction of the lateral and superior semicircular canals.fig 3. Partial absence of the oval window with a large facial nerve on coronal CT scan. This patient with microtia and external canal stenosis (short arrows) has an unusually large horizontal facial nerve (arrowhead). The bone beneath the lateral semicircular canal is thick. The bony facial nerve canal is not well delineated and the nerve overlies the atretic oval window (long arrow)
In three ears, the horizontal facial nerve canal was well formed and located along the cephalic margin of the oval window. To the eye, these canals appeared more medial than normal (ie, closer to the oval window), owing to the abnormal thickness of the oval window. However, these nerves were located lateral to the vertical line drawn through the anterior junction of the lateral and superior semicircular canal, and therefore were considered to be normal in location (Fig 2). In six ears, the canal ran in an abnormal, inferior plane at the center of the oval window or at its inferior border or just below it (Fig 4). Of these six malpositioned canals, three lacked a well-defined bony canal (Fig 3) and four were medial in location (ie, closer to the oval window and medial to the vertical line drawn through the anterior junction of the lateral and superior semicircular canal on the coronal scan) (Figs 4 and 5). One of the low facial nerves was unusually large, and essentially blocked access to the oval window (Fig 3); this was in a patient with microtia in whom a future ossicular reconstruction was contemplated then dismissed on the grounds that the CT findings showed a high potential for facial nerve injury. All patients had normal labyrinthine and geniculate facial nerve canals, and all except those with microtia had normal descending facial nerve canals. Therefore, six of nine ears with congenital absence of the oval window had an abnormality of the horizontal facial nerve canal that was considered to be clinically significant in that the nerve was at some risk for injury during a surgical procedure.
fig 4.
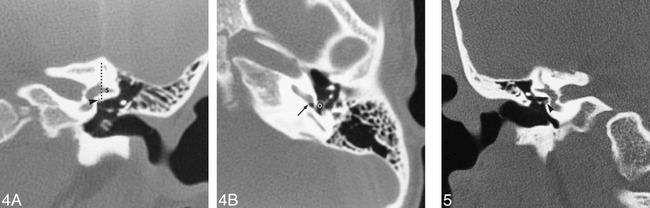
A and B, Congenital absence of the oval window on coronal (A) and axial (B) CT scans. The oval window is completely obliterated. In A, the horizontal facial nerve canal is intact (arrowhead) but is low in position, directly lateral to the oval window. The canal lies medial to the vertical line drawn through the anterior junction of the lateral and superior semicircular canals. The bone below the lateral semicircular canal (S) is extremely thick. Note the myringotomy tube placed for serous otitis media that had no effect on the patient's maximal conductive hearing loss. In B, there is posterior and inferior displacement of a well-formed stapes arch, now located at the level of the round window (arrow), straddling the sinus tympani. O indicates the obturator foramen between the stapes crura.fig 5. Congenital absence of the oval window with a dysplastic stapes on coronal CT scan. The oval window is completely obliterated. The bone below the lateral semicircular canal is intact and solid, lacking the facial nerve canal. The nerve is aberrant, found along the lower border of the oval window (arrowhead) and could be followed anteriorly to the geniculate ganglion (not shown). The stapes is dysplastic and one crus extends onto the facial nerve. Note that the nerve is medial in location
Seven ears had dysplastic or absent stapes; in two of these, one or both crura appeared to surround the horizontal facial nerve (Fig 5). The two normal stapes were displaced inferiorly and posteriorly, away from the obliterated oval window (Fig 4B). In three ears, dysplasia of the incus was identified along with a malformed stapes. The malleus was normal in all patients without microtia.
Two patients had microtia. One had atresia of the external auditory canal and the typical ossicular malformation of this deformity: a clumped malleus and incus fused to the atresia plate. In the other patient with microtia, external canal stenosis with dysplastic changes of the long and lenticular incudal processes were found. Neither of these patients had an identifiable stapes.
Abnormalities of the otic capsule were found in two patients: one patient, with microtia, had mild dilatation of the vestibule; the other, with complete congenital absence of the oval window, had mild dilatation of the vestibular aqueduct.
On coronal CT scans in the control group, the horizontal facial nerve canal was found to lie lateral to a vertical line drawn through the anterior junction of the lateral and superior semicircular canal in 48 of 50 ears. The vertical line traversed the horizontal facial nerve canal in two of these normal ears. Therefore, a lateral location of the nerve in relation to the vertical line was thought to be a reliable indicator of a normally positioned horizontal facial nerve canal. Both anterior and posterior stapes crura were well delineated on the axial CT scans in 40 of 50 normal ears. Of the 10 middle ears in which the stapes was poorly visualized, two had fenestral otosclerosis and seven had partial or complete middle ear opacification. In only one otherwise normal middle ear was the stapes not well seen. Therefore, failure to visualize the stapes crura in an aerated middle ear on an axial CT scan is thought to be a reliable indicator of stapes absence or dysplasia.
Discussion
Conductive hearing loss in the pediatric population is usually found to be caused by acquired middle ear disease, such as acute otitis media, acute otitis media with effusion, and chronic otitis media (5). Congenital conductive hearing loss is a far less common entity, and must necessarily be due to a developmental anomaly of the ear along the conductive pathway from the external auditory canal to the oval window. External canal atresia or stenosis accounts for most cases of congenital conductive hearing loss, with only a small percentage of cases caused by isolated dysplasia of the ossicular chain and/or the oval window (6). Congenital absence of the oval window is considered to be a rare anomaly of temporal bone development and has an important association with anomalous facial nerve development (7). Many otologists believe that congenital absence of the oval window is more frequently seen in practice than the literature would suggest (7). The diagnosis of congenital absence of the oval window can be made on routine, high-resolution CT studies of the temporal bone, and provides invaluable information to the clinician. Identifying this malformation may sway an otologist away from performing a middle ear exploration, particularly if there is a potential for facial nerve injury.
The normal oval window niche is a rectangular, medial recess of the middle ear cavity that can be seen on all CT scans of the temporal bone, both axial and coronal (see Fig 1). The oval window is bordered superiorly by the lateral semicircular canal and its bony encasement, medially by the vestibule, and inferomedially by the basilar turn of the cochlea and the bone of the cochlear promontory. The horizontal or tympanic segment of the facial nerve canal runs in the bone of the otic capsule immediately below the lateral semicircular canal, along the superior margin of the window. Anterior to the oval window is the wedge of otic capsule between the vestibule and the middle turn of the cochlea. Posteriorly lies the orifice of the sinus tympani. The oval-shaped stapes footplate and its circumferential annular ligament close the oval window. The footplate normally measures 0.25 mm in thickness (8), and may be seen as a thin white line traversing the oval window; occasionally, it is not seen on the CT scan. The more lateral components of the stapes consist of the anterior and posterior crura and the head or capitulum, which articulates with the cup-shaped lenticular process of the incus. The stapes is oriented in the horizontal plane and is therefore best appreciated in the axial imaging plane.
The oval window is an anatomic and developmental junction zone forming the interface between the middle and the inner ear. Formation of the oval window is intimately related to development of the stapes footplate, the annular ligament, the horizontal segment of the facial nerve canal, and the vestibular component of the otic capsule. As early as the fifth week of gestation, the blastemal mass of the stapes becomes recognizable as a ring-shaped structure around the stapedial artery. This rudimentary stapes grows medially, then contacts and indents the developing otic capsule at the future oval window during the seventh week of gestation. The tissue in this depression fuses with the stapedial ring to form the stapes footplate (7, 9). By 14 weeks, the stapes crura are recognizable; at 18 weeks, ossification begins; and by 32 weeks, the stapes appears in its infant form (9). Once the base of the stapes has fully developed, dedifferentiation of the oval window cartilage occurs, and a rim of fibrous tissue forms, producing the annular ligament. The stapes is thus adult in configuration at 35 weeks (9). When the primitive stapes fails to fuse with the primitive vestibule, the oval window cannot develop, resulting in its congenital absence. Malformation of the stapes is an expected concomitant finding given the close relationship of the stapes to the oval window during this developmental sequence. Failure of the annular ligament to completely form produces congenital fixation of the stapes footplate, the opposite end of this spectrum (9), an entity without radiologic findings. Partial absence or hypoplasia of the oval window represents a malformation of intermediate severity, as seen in two of our patients.
Like the stapes, the facial nerve develops from the second branchial arch. The horizontal segment of the facial nerve is recognized by the sixth week of gestation when it passes between the developing membranous labyrinth and the primitive stapes (10). By week 8, soon after the stapes blastema reaches the otic capsule, a sulcus forms within the lateral margin of the cartilaginous otic capsule, initiating formation of the horizontal facial nerve canal; this groove forms by week 10. If this canal is deep and well formed, the facial nerve will be “locked in” to its normal anatomic position against the otic capsule (10). The facial nerve groove will begin to enclose the facial nerve in the fourth gestational month. Ossification of the canal is completed during or shortly after the first year of life (11).
The developmental processes of the stapes, oval window, and facial nerve are clearly related both temporally and spatially. One widely accepted explanation for congenital absence of the oval window proposes that during the fifth and sixth weeks of gestation, the developing facial nerve becomes anteriorly displaced and interposed between the otic capsule and the stapes blastema. As a result, contact between the stapes and otic capsule required to initiate development of the oval window is prevented (10, 12, 13). Both the oval window and the stapes will be malformed (10).
The imaging features of congenital absence of the oval window reflect this developmental aberration. Failure of the oval window to develop results in its osseous obliteration either by a concentric narrowing that produces a dimplelike depression along the medial tympanic wall or by a thick bony plate. In either case, the rectangular shape of the oval window niche is obliterated. An abnormal appearance of the stapes is frequently associated with congenital absence of the oval window, and is characterized by failure to identify both stapes crura in the oval window on the axial CT scan. A normally formed stapes may be displaced out of the oval window niche (see Fig 4). In our series, seven of nine stapes were absent or malformed, and three of these were associated with malformation of the incus as well.
Based on the embryologic derivation, dysplasia of the stapes superstructure (crura and capitulum) is expected, and this association is substantiated in the surgical otology literature. In 1976, Jarsdoerfer (7) reviewed the literature and found a total of 45 ears with congenital absence of the oval window; in addition, he had six of his own cases, and by combining these data, he published a report on 51 ears with congenital absence of the oval window documented at surgery. In his series, only 4% of the patients had a normal stapes, 43% of middle ears had no stapes, and 41% had a malformed stapes. In another surgical publication, Lambert (13) reported on seven patients with congenital absence of the oval window and noted that the stapes was either absent or severely abnormal in all. The spectrum of abnormalities found at surgery includes a small and rudimentary stapes lacking footplate or crura, a loop-shaped stapes, an amorphous ossicle, fibrous connection of the stapes to the facial nerve canal, a stapes embedded in an uncovered facial nerve, and aplasia (13).
Even more important from a surgical standpoint is the association of congenital absence of the oval window with anomalous development of the horizontal facial nerve canal. In our series, the abnormalities encountered were low-lying canals within or below the expected location of the oval window, canals without an identifiable bony covering, and a large facial nerve. The labyrinthine and geniculate portions of the canal were normal in all patients, while the descending segment was abnormal in the two patients with external canal atresia, reflecting the facial nerve malformations typically encountered in that entity.
The surgical otology literature substantiates these radiologic findings. In Jahrsdoerfer's series of 51 ears (7), 76% of the patients with congenital absence of the oval window had malformation of the facial nerve canal; in 12% the canal was normal and in 12% morphology was not mentioned. In Lambert's series (13), four of seven facial nerve canals were abnormal. The most common abnormalities encountered in these surgical reports were low-lying canals running within the region of the oval window and grossly dehiscent canals, similar to the findings in our series. Less commonly reported were stapes embedded within a dehiscent facial nerve, an absent horizontal facial nerve canal with a large chorda tympani presumed to be carrying all the facial nerve fibers, a hypoplastic facial nerve, a bifurcated horizontal canal, and a persistent stapedial artery (7, 13–15).
The prevalence of inner ear malformations associated with congenital absence of the oval window is surprisingly low. In our series of nine ears, one had a slightly dilated vestibular aqueduct and another had a mildly dilated vestibule. This observation lends support to the mechanical theory of congenital absence of the oval window, in which failure of the developing stapes to physically contact the otic capsule explains lack of development of the oval window. A toxic insult occurring at the time of contact between the primitive stapes and otic capsule would occur at approximately 7 weeks gestational age and should affect all regional tissues with equal frequency. An arrest of inner ear development at 7 weeks could produce several types of inner ear dysplasia, including incomplete septation of the cochlea (classic Mondini malformation), a dilated vestibule incorporating the lateral semicircular canal, a dilated lateral semicircular canal, and a dilated vestibular aqueduct (16).
None of our patients had a middle ear exploration to confirm the impression of congenital absence of the oval window, because our otology service currently chooses not to correct this type of hearing loss surgically. When imaging features are subtle, the clinical data become even more important. A history of maximal conductive hearing loss from birth without prior episodes of otitis media, normal findings at otoscopic examination, and suggestive radiologic findings make the diagnosis of congenital absence of the oval window highly likely. An aberrant horizontal facial nerve canal confirms the diagnosis. Clearly, however, there is a threshold of abnormal findings below which the diagnosis cannot be made with certainty.
The differential diagnosis of congenital absence of the oval window is limited to fenestral otosclerosis and tympanosclerosis. Each of these entities has a distinctly different clinical presentation than congenital absence of the oval window and should not create diagnostic confusion. Onset of otosclerosis in childhood is unusual, but it has been reported (8, 17). The CT scan initially shows poorly mineralized radiolucent bone building up anterior to the oval window, eventually encroaching into it. With time, this spongiotic bone fully ossifies, and in the absence of any clinical history, could appear similar to congenital absence of the oval window on the CT scan. The CT scan of tympanosclerosis may show osseous obliteration of the oval window identical to that in congenital absence of the oval window. However, associated inflammatory changes of the middle ear will invariably be present, including partial or complete middle ear opacification and typical inflammatory ossicular erosion and/or fixation (18). When complete osseous obliteration of the oval window is seen with a malpositioned horizontal facial nerve canal, the diagnosis of congenital absence of the oval window is favored over these two entities.
Surgical repair of a congenitally absent oval window is technically difficult, and outcomes have been variable (1, 7, 13). A malpositioned and/or exposed facial nerve is at great risk for injury (7, 19). Surgical vestibulotomy or fenestration of the lateral semicircular canal could be complicated by a perilymphatic fistula, and result in a nonhearing ear. Jahrsdoerfer (7) and Sterkers and Sterkers (1) reported some degree of hearing improvement after vestibulotomy. In Lambert's series of seven patients (13), six had surgical correction, with no sustained improvement in hearing at the 1-year follow-up. Detection of congenital absence of the oval window on high-resolution CT scans will allow the surgeon to select cases worthy of an attempt at correction and suggest hearing aids for those in whom the risk is too great. Surgical patients could be referred to a more experienced team without the need for an initial middle ear exploration to uncover the anomaly.
Conclusion
Congenital absence of the oval window is a rare but important cause of maximal conductive hearing loss. The diagnosis is often suspected by the otologist and can be confirmed on routine high-resolution temporal bone CT scans. The common association of congenital absence of the oval window with anomalous tympanic facial nerve development can be explained on an embryologic basis. The radiologist must therefore understand the spectrum of abnormal facial nerve development and have a high index of suspicion for a malpositioned or exposed horizontal facial nerve. Similarly, when an occluded oval window is seen in association with an anomalous horizontal facial nerve canal on a temporal bone CT scan, the diagnosis of congenital absence of the oval window may be suggested.
Footnotes
Address reprint requests to Barbara Zeifer, MD, The New York Eye & Ear Infirmary, 310 E 14th St, New York, NY 10003.
References
- 1.Sterkers J-M, Sterkers O. Surgical management of congenital absence of the oval window with malposition of the facial nerve. Adv Otol Rhinol Laryngol 1988;40:33-37 [DOI] [PubMed] [Google Scholar]
- 2.Weissman JL. Hearing loss. Radiology 1996;199:593-611 [DOI] [PubMed] [Google Scholar]
- 3.Mayer TE, Brueckmann H, Siegert R, Witt A, Weerda H. High-resolution CT of the temporal bone in dysplasia of the auricle and external auditory canal. AJNR Am J Neuroradiol 1997;18:53-65 [PMC free article] [PubMed] [Google Scholar]
- 4.Swartz JD, Glazer AU, Faerber EN, Capitanio MA, Popky GL. Congenital middle-ear deafness: CT study. Radiology 1986;159:187-190 [DOI] [PubMed] [Google Scholar]
- 5.Briggs RJS, Luxford WM. Correction of conductive hearing loss in children. Otolaryngol Clin North Am 1994;27:607-619 [PubMed] [Google Scholar]
- 6.Stewart JM, Downs MP. Congenital conductive hearing loss: the need for early identification and intervention. Pediatrics 1993;91:355-359 [PubMed] [Google Scholar]
- 7.Jahrsdoerfer RA. Congenital absence of the oval window. ORL J Otorhinolaryngol Relat Spec 1977;84:904-914 [Google Scholar]
- 8.House JW. Otosclerosis. In: Hughes GB, Pensak ML, eds. Clinical Otology. 2nd ed. New York: Thieme; 1997:241–249
- 9.Harada T, Black FO, Sand OI, Singleton GT. Temporal bone histopathologic findings in congenital anomalies of the oval window. Otolaryngol Head Neck Surg 1980;88:275-287 [DOI] [PubMed] [Google Scholar]
- 10.Jahrsdoerfer RA. Embryology of the facial nerve. Am J Otol 1988;9:423-426 [PubMed] [Google Scholar]
- 11.Nager GT, Proctor B. Anatomical variations and anomalies involving the facial canal. Otolaryngol Clin North Am 1991;24:531-553 [PubMed] [Google Scholar]
- 12.Gerhardt HJ, Otto HD. The intratemporal course of the facial nerve and its influence on the development of the ossicular chain. Acta Otolaryngol 1981;91:567-573 [DOI] [PubMed] [Google Scholar]
- 13.Lambert PR. Congenital absence of the oval window. Laryngoscope 1990;100:37-40 [DOI] [PubMed] [Google Scholar]
- 14.Teunissen EB, Cremers Cor WRJ. Classification of congenital middle ear anomalies. Ann Otol Rhinol Laryngol 1993;102:606-612 [DOI] [PubMed] [Google Scholar]
- 15.Magnuson T, Har-El G. Middle ear anomalies. Otolaryngol Head Neck Surg 1994;111:853-854 [DOI] [PubMed] [Google Scholar]
- 16.Jackler RK, Luxford WM, House WF. Congenital malformations of the inner ear: a classification based on embryogenesis. Laryngoscope 1987;97: (Suppl 40) 2-24 [DOI] [PubMed] [Google Scholar]
- 17.Robinson M. Juvenile otosclerosis. Ann Otol Rhinol Laryngol 1983;92:561-565 [DOI] [PubMed] [Google Scholar]
- 18.Swartz JD, Harnsberger HR. The middle ear and mastoid. In: Swartz JD, Harnsberger, HR eds. Imaging of the Temporal Bone. 3rd ed. New York: Thieme; 1998: 47–169
- 19.Pou JW. Congenital anomalies of the middle ear. Laryngoscope 1976: 251–254 [DOI] [PubMed]