

Abstract
The use of eponyms adds a valuable historical context to the art of medicine, and shall hence be encouraged, nevertheless their use must always reflect an appropriate historical and medical terminology. A bizarre narration concerns the widespread term “St. Anthony’s fire”, which has been used for denoting not less than three distinct diseases. In this article we underscore that at least three distinct diseases, one toxic (i.e., ergotism) and two infectious (i.e., erysipelas and herpes zoster) have been called, in different times and countries, with the same eponym term of “St. Anthony’s fire”, whilst some other diseases may have also been comprised under this “umbrella” definition. It is possible, for example, that even some cases of plague may have been misclassified as “St. Anthony’s fire”. This article also deals with the importance of this topic in the history of art. Several important artists in different periods, in particular painters, were inspired from the history of St. Anthony, who is generally represented in association with fire (representing the burning pain of the diseases), pig (symbolizing the fat of pigs used in the past for relieving skin symptoms), and different “temptations” (devils, food, gold, jewelry, etc.). A literary masterwork is also cited and discussed. (www.actabiomedica.it)
Keywords: St. Anthony’s fire, ergotism, erysipelas, herpes zoster, plague
Introduction
Although the use of eponyms adds a valuable historical context to the art of medicine, and shall hence be encouraged, their use must always reflect an appropriate historical and medical terminology. A bizarre narration concerns the widespread term “St. Anthony’s fire”, which has been used for denoting not less than three distinct diseases.
In the first century BC, the Roman poet and philosopher Lucretius referred to outbreaks of skin acute disease (erysipelas?) as “ignis sacer” (holy fire), describing the burning sensation that was associated with infection (1). According to the following historical evolution of epidemiology and terminology, it appears rather certain that the terms “ignis sacer” (holy fire) and “St. Anthony fire” are not synonyms, although a certain degree of overlap may exist.
St. Anthony of Egypt was born in 251 AD. At the age of 20 he sold all his possessions, gave his wealth to the poor and needy, and disappeared in the desert for living an unblemished life, fasting for long periods (the probable reason for visions and temptations he is said to have experienced), and carrying a monastic life of prayer. He was indeed one of the founders of Christian monachism. He has been involved in a number of healings and exorcisms during his permanence in the desert, so that his name has been originally associated with the sacred art of healing. After his death, at the notable age of 105 years, his burial place was kept secret until the 532 AD, when his bones were moved to Alexandria in Egypt (2), then conveyed to Constantinople by the Saracens after the sack of the city more than a century later, and finally arrived - after adventurous journeys - in Europe. Several countries, cathedrals and monasteries came then into competition for retaining and exposing the relics of the Saint, and at least three “bodies of St. Anthony” have been present in Europe for centuries. One of the bodies was preserved in France, at La Motte St. Didier, in the neighborhoods of Vienne. Here, in the year 1095, a community of monks has been founded. They dedicated themselves to caring sick people, becoming renowned even out of their region, until Pope Bonifacius VIII instituted the Ordo Hospitalierum Sancti Antonii Abbas in Vienne (Hospitaller Order of St. Anthony the Abbot in Vienne) in the year 1297 (3). The modern term “hospital” takes its origin in these aforementioned facts. Several “hospitals” were then built across Europe, especially along the pilgrim’s ways. Skin diseases were extremely common throughout the antiquity, at least until modern hygiene, lifestyle changes and antibiotics have been developed. The combination of poor hygienic conditions, infrequent changes of clothing, rare hand-washing and overcrowded living facilities contributed to make skin affections commonplace in previous centuries. Since no explanations or effective therapies were available at that time, asking Divine assistance for healing was rather frequent. In Catholic countries, a prayer to St. Anthony has been made by the common folk, in order to obtain a cure for acute skin affections. It was generally believed that St. Anthony have cured people with various skin diseases using pork fat, which was effective to mitigate inflammation and itching. The term “St. Anthony’s fire” became thus always more popular, and was used for defining several distinct diseases which share the so-called “burning skin” sensation. After several centuries, due to the fact that “Hospitallers” have gained enormous power and money, Pope Pius VI suppressed the Order in the year 1776, which was merged in the Order of Knights of Malta, also devoted to hospital assistance (4).
Ergotism
St. Anthony had no direct connection with ergotism throughout his lifetime. Nevertheless, Anthony’s name and life story were linked to the disease, whereby his own name was endorsed by the Order of Hospitallers, who were credited with many cures. Ergotism in humans has been very common during the Middle Ages (5), causing many epidemics of mass poisoning (it was indeed one of the scourges at those times), although the nature and underlying cause of disease were still elusive.
Ergot is the alkaloid-containing product of a fungus, Claviceps purpurea, which grows on grains, especially rye. The fungal spores are carried by the wind to the ovaries of young rye, where they germinate into hyphal filaments. These grow deeply into the rye, forming a dense tissue which progressively takes over the grain and hardens into a purple curved spur or sclerotium (“ergot” is derived from “argot”, Old French for the cock’s spur).
Several grass species are vulnerable to ergot infection, but ergot in grain species is what really matters in human pathology. Various grain species, including for example wheat (Triticum aestivum), rice (Oryza sativa) and maize (Zea mays), are the most important sources of human food on a global scale (6). However, rye (Secale cereale) is by far the most vulnerable to Claviceps Pupurea, and most European episodes of mass poisoning have been caused by ergot-infected rye. Rye grows well in cooler areas with poor drainage and acid soils (i.e., the area where wheat does not grow well). Unfortunately, Claviceps purpurea also thrives in constantly damp conditions.
There is a couple of very early references on ergot. One probably refers to the “noxious pustule in the ear of grain” noted on an Assyrian cuneiform tablet of around 600 BC, whilst the second can be found in one of the sacred books of Parsees (400 BC to 300 BC), as “grasses that cause pregnant women to drop the womb and die in childbirth” (7). The Romans regarded rye as an inferior grain, and perhaps for good reasons. In the second century AD, Galen commented on rye bread from the Balkans as being black, with a bad smell (8). Pliny, in his Historia Naturalis dated first century AD, regarded rye as an inferior cereal, with a harsh taste (9). Both comments may raise suspicion of “poisonous” nature of this plant.
It was not until the Christian era that rye has been introduced in western Europe, and it was hence not until the Middle Ages that written traces of ergot poisoning can be found (10). The first mention to a gangrenous ergotism plague in Europe appeared in the year 857, in Germany. Several other records of epidemics then emerged in France, Germany and Scandinavia (11). Overall, as many as 83 ergotism epidemics have been reported in various parts of Europe from 945 AD onwards, and this list is certainly incomplete (12). The German physician Wendelin Thelius, who described an epidemic developed in the year 1596 in the Kingdom of Hesse, was the very first to identify ergotism as the underlying cause (11). In 1676 it was finally established that ergotism was caused by rye infected by the fungus Claviceps Purpurea (13), though the first measures for facing ergot poisoning were only developed in the late 18th century. More specifically, the French physician Tessier observed a huge epidemic in the year 1778 in Sologne (France), during which more than 8000 people died, and was hence persuaded to recommend drainage of fields, compulsory cleaning of grain and replacement of infected grain with potatoes (11).
Ergotism had two main essential clinical manifestations, entailing gangrene (referred to as chronic ergotism) and convulsions (acute ergotism). The former (i.e., the type known for centuries as St Anthony’s Fire) was characterized by intense burning pain and gangrene of feet, hands and whole limbs. In severe cases, the affected tissues became dry and black, and mummified limbs dropped off without loss of blood.
The chemical composition of ergot is complex and variable (11, 14). The pharmacological properties have been recognized for centuries, although they were not well studied and publicized until the early 20th century. Ergot alkaloids, structurally similar to serotonin, act as serotonin agonists. They also interact with a number of adrenergic receptors, thus causing vasoconstriction, blood flow reduction and eventually terminal necrosis of extremities. Ergot also stimulates the central nervous system, thus promoting a variety of mental states (depending of interaction with dopaminergic, serotonergic and adrenergic pathways) including hallucinations, but even depression and, occasionally, coma up to death. Notably, the pharmacological effects are variable among different alkaloids, with various strains of Claviceps purpurea and soils predictably generating diverse ergot alkaloid compositions. A whole range of ergot alkaloids has been detected, several of which are poisonous, whilst others are psychoactive.
According to European records, convulsive ergotism was more frequent in areas on the east side of Rhine (e.g. Germany), whereas the gangrenous type was more widespread in France and in other areas in the west side of Rhine (15). This geographical pattern reflects variations in ergot alkaloid composition, which are at least partially attributable to different conditions during the growth season (e.g. weather) and host plant parasitized (5, 16). It has been recently suggested that Claviceps populations are not specialized in terms of hosts, but rather in terms of habitats, which are obviously interconnected with climatic conditions (17). After harvesting, toxicity may be dependent on storage and transport conditions, since ergot alkaloids tend to undergo degradation over time (e.g., ~18 months) (17).
The history interplays with agriculture and medicine. In Norway, for example, rye was introduced in Rogaland (south-west Norway) and in Vestfold (south-east Norway) in the fifth century AD (18, 19). The Rogaland toponymal itself, as well as the name of the people living there (ryger), may in fact originate from an Indo-European stem for rye (8, 20).
Epidemics of ergotism continued to occur sporadically in Europe until the first half of the 20th century (an epidemic occurred in the year 1951 in France, accounting for nearly 250 victims). Since then, although some outbreaks occurred in less-developed countries, ergotism has been confined to individual cases of ergotamine overdosage in the more-developed world (13, 15, 21).
The dramatic symptoms and signs of ergotism attracted the interest of many artists, particularly in the late Middle Ages. The German painter Matthias Grünewald, a contemporary of Albrecht Dürer and Lucas Cranach, depicted figures with abnormal postures and skin eruptions, probably modelled from patients with ergotism in the monastery (Fig. 1) (22).
Figure 1.
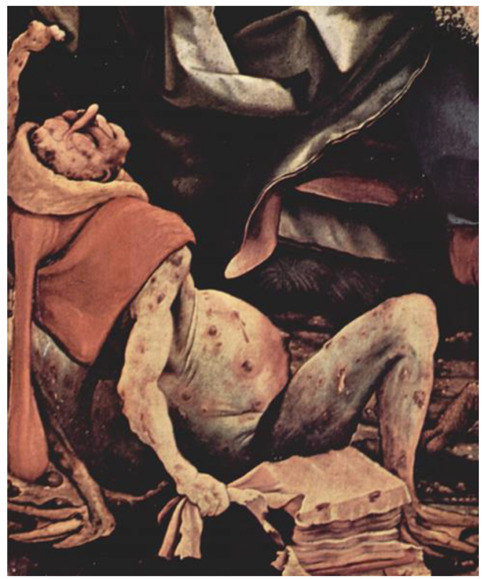
Mathias Grünewald (1480-1528): St. Anthony temptations (particular, showing skin manifestation of St. Anthony’s fire)
There are also several mentions in the Norse-Icelandic sagas of a human disease for which ergot poisoning was the possible underlying cause. Some descriptions are highly evocative of “holy fire”, underlining that sufferers were tormented by an invisible flame burning inside their body. People thought that it destroyed the limbs, occasionally leaving only the head and torso (23).
The psychiatric symptoms of ergotism (hallucinations, namely) persuaded people to think at them as having “diabolic nature”. The affected people were hence accused of witchcraft in many countries. For example, the Salem Witch Trials of 1692 represents a dark time in colonial America, but also a curious medical mystery. The trials began when several young girls in Salem, Massachusetts, fell ill and developed unexplained symptoms, including temporary blindness, skin lesions, convulsions and hallucinations. The local doctor, uncertain of the real cause of their sickness, diagnosed these girls as having “bewitchment” (24). This clinical judgment caused persecution and subsequent prosecution of suspected subjects. The preexisting culture of superstition, along with ongoing warfare against surrounding villages and fear of attack from Native Americans, contributed to the hysteria anticipating the witch hunt (24). Following the trials, many scholars theorized about the true cause of the mysterious illness, and a plausible explanation was convulsive ergotism. The enigmatic epidemic that swept throughout the Salem village, along with the following witch hunt, is a notable example of how medicine and history are often intertwined. The dermatological findings in the victims of the Salem Witch Trials are invaluable in unraveling the truth behind what was once thought to be the workings of witches.
Erysipelas
The term “erysipelas” is conventionally used by doctors for describing a skin infection limited to legs, arms or face (25). The infection mainly involves the upper dermis and superficial lymphatics, and is typically caused by beta-hemolytic group A Streptococci, beginning from mild wounds, stings or scratches. In several cases, however, the site of entrance of the microorganism cannot be clearly identified. Erysipelas is more superficial than cellulitis, and typically more raised and demarcated.
The original writings of Hippocrates, from the 4th century BC, describe the disease erysipelas (ἐρυσίπελας, i.e., red skin) (26) and, in fact, streptococcal diseases have been known for centuries, though their delineation in separate disease entities has not occurred until the 16th century AD. Until the 19th century AD several severe skin infections were classified under the term “erysipelas”, including what we now classify as pyoderma gangrenosum, necrotizing fasciitis, Fournier’s gangrene and, probably, toxic shock syndrome (27). In the seminal article of Corbin, we can read that “phlegmonous erysipelas is frequently complicated with gangrene”, “mortification of the skin is generally consecutive to destruction of subcutaneous cellular tissue”, “the external integuments are destroyed, and the muscles or aponeuroses are laid bare”, “in erysipelas of the legs, in nine cases out of ten, gangrene takes place after the suppuration and destruction of the cellular tissue”, “we frequently see pure phlegmonous erysipelas arise in the scrotum, and a part of it destroyed by mortification”, and so forth (27). It seems thus obvious that we are now using the same term only for a subgroup of diseases earlier classified as “erysipelas”.
The first description of streptococcal infection can be attributed to the Austrian surgeon Theodor Billroth, in 1874, when he identified some organisms responsible of erysipelas and wound infections (28, 29). He described that these “small organisms (Kettenkokken) can be found either isolated or arranged in pairs, sometimes in chains of four to twenty or more links. He also proposed the name Streptococcus (strepto, a chain, and coccus, a berry)”. The true significance and formal appearance of Streptococci in history started in 1879, when Louis Pasteur isolated the microorganism from uteruses and blood of women with puerperal fever (30). He further demonstrated that the Streptococcus was the underlying pathogen of the disease causing the highest mortality rates of women and newborns at that time. Additional refinement of the name Streptococcus came from Friedrich Julius Rosenbach, in 1884, who examined bacteria isolated from suppurative lesions, and the species was hence named Streptococcus pyogenes (Gr., pyo, pus, and genes, forming) (31). Fehleisen previously isolated Streptococci from a patient with erysipelas, whilst Rosenbach named the microorganism Streptococcus erysepaltis (31, 32). It was later shown that no particular characteristic was associated with organisms isolated from specific diseases, so that Andrewes and Christie suggested that the proposed species names of pyogenes, erysepaltis, scarlatinae and puerperalis should have been all included in the single name of Streptococcus pyogenes (31,33).
Prior to antibiotics, only skin cleaning and cool dressing were used to treat these infections, with largely unsatisfactory outcomes, and this explains the attribution of a “holy” origin to this condition. “St Anthony’s fire” is in fact the name that is still given to streptococcal erysipelas in many Anglo-Saxon European countries, as well as in the United States. Erysipelas have killed saints, popes, kings, soldiers and writers, throughout mankind history. Famous casualties of erysipelas include St. John of the Cross (dead in 1591), Pope Gregory XVI (dead in 1846), Queen Anne (dead in 1714), Princess Amelia of Great Britain (dead in 1810), Queen Christine of Sweden (dead in 1679), King Frederick VII of Denmark (dead in 1873). The German composer Richard Wagner also suffered from erysipelas, but he was cured and then died in 1883 for a heart attack (34).
Herpes zoster
Herpes zoster (HZ), a viral disease sustained by reactivation of latent varicella-zoster virus (VZV) is also known as St. Anthony’s fire especially in Italy, France and Spain. VZV is a herpes virus which causes chickenpox, or varicella, in childhood. Although the distribution is virtually ubiquitous, it is more prevalent in temperate climates and the disease develops most frequently during late winter and spring (35). After resolution of acute phase, residual provirus segments travel from sensory nerve endings up sensory fibers, eventually lodging in cranial or dorsal root ganglia. Once inside neuronal nucleus, the virus remains in a latent form, although always retaining the capability to revert to infectious state (36). The mechanisms leading to reactivation of VZV are still largely unclear. Although some risk factors have been identified (i.e., age, immunocompromised state, immunosuppressive drugs, HIV infection, cancer, psychologic stress, trauma, among others), reactivation mostly occurs when cell-mediated immunity decreases below a crucial level (35).
HZ, or shingles, predominantly affects older people, occurring in consequence of aging-related waning of cell-mediated immunity to VZV, which is dormant in everyone who has ever had chickenpox (37). Approximately 50% of HZ cases develop in people aged 50 years or older (38), with incidence increasing in parallel with ageing, from 1.1- 2.9 cases per 1000 person-years in people aged ≤50 years, to 9.5 and 10.9 cases per 1000 person-years in age groups of 70-79 and ≥80 years, respectively (39).
VZV injuries neurons and satellite cells, with neurologic damage beginning even before appearance of the characteristic zoster rash (40). Postherpetic neuralgia is the most frequent complication of HZ, which may cause debilitating pain (often continuing for long after the rash resolves and despite aggressive antiviral and/or pain therapy) and impaired quality of life in otherwise healthy older people (41).
Another disabling complication occurs when HZ infections involves the first division of trigeminal nerve, thus leading to developing herpes zoster ophthalmicus and the consequent risk of long-term vision complications due to inflammation or nerve damage (42, 43).
Historically, a relationship between the etiologies of varicella and herpes zoster has been first suggested by von Bòkay in 1892, who observed that young children often developed varicella after contacts with adults suffering from herpes zoster (44). Microorganism transmissibility has then been demonstrated by inoculation of fluid recovered from herpes zoster lesions in children with no history of varicella; all these children developed varicella, and secondary transmission could be documented (45). Garland and Hope-Simpson first suggested that herpes zoster was caused by reactivation of a latent virus, acquired during varicella (36). Afterwards, Goodpasture and Anderson detected multinucleated giant cells in a human skin/chorioallantois membrane culture system infected with herpes zoster lesion fluid in the year 1944 (46), and infectious VZV was finally isolated in tissue culture by Weller and Stoddard in 1953 (47).
The burning nature of the pain caused by HZ gives a reasonable explanation for this third disease also named as St. Anthony’s fire.
Discussion
In this article we have underscored that at least three distinct diseases, one toxic (i.e., ergotism) and two infectious (i.e., erysipelas and herpes zoster) have been called with the same eponym term of “St. Anthony’s fire”, whilst some other diseases may have also been comprised under this “umbrella” definition, as earlier discussed. It is possible, for example, that even some cases of plague may have been misclassified as “St. Anthony’s fire”. The plague has dramatically ravaged Italy during the 16th century, especially Venice. Many prayers were raised in the Venetian churches, and also privately addressed to St. Anthony, with the hope of preventing plague contagion and finding an effective treatment. Although the etiology of the bubonic plague was Yersinia pestis (and not ergot alkaloids, Streptococcus pyogenes or VZV), the plague generated enlarged ulcerated lymph nodes and severe skin involvement, so that it was classified as a different type of St. Anthony’s fire.
Several important artists in different periods, in particular painters, were inspired from the history of St. Anthony, who is generally represented in association with fire (representing the burning pain of the diseases), pig (symbolizing the fat of pigs used by the Hospitallers for relieving skin symptoms), and different “temptations” (devils, food, gold, jewelry, etc.). The most famous certainly include Hieronymus Bosch (1450-1516), Giovanni Girolamo Savoldo (1480-1548), Michelangelo Buonarroti (1475-1564), the aforementioned Matthias Grünewald (1480-1528), Pieter Huys (1519-1584), Paolo Caliari “the Veronese” (1528-1588), Pieter Brueghel the Elder (1525/1530-1569), Salvator Rosa (1615-1673), Fèlicien Rops (1833-1898), Paul Cézanne (1839-1906), Max Ernst (1891-1976), Salvador Dalí (1904-1989). Figures 2-4 displays some examples of these paintings. Among these celebrated artists, Hieronymus Bosch made the temptations of St. Anthony one of his favorite subjects, and up to five paintings on this subject are attributed, totally or partially, to him. He depicted the Saint himself and sufferers from various forms of ergotism with strange flying objects which reproduce hallucinations (11).
Figure 2.

Giovanni Gerolamo Savoldo (1480-1548): St. Anthony temptations
Figure 4.
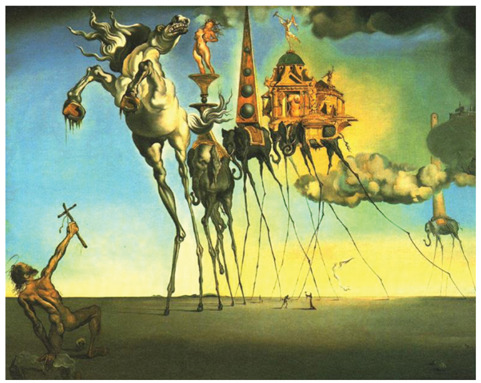
Salvador Dalí (1904-1989): St. Anthony temptations
Figure 3.

Michelangelo Buonarroti (1475-1564): St. Anthony temptations
In literature, Gustave Flaubert’s novel “La tentation de Saint Antoine” (1874) represents the most famous example. In this book the old St. Anthony, while remembering the ancient temptations, is newly captivated by power, luxury and pursuit of pleasure. In the meanwhile, one of his disciples, Ilarion, presents to the holy man “all the Gods, the rites, the prayers and the oracles”, emphasizing the contradictions of the Holy Scriptures (48).
In conclusion, for several centuries each affection capable of provoking a burning pain in the skin was named St. Anthony’s fire. The time and the local epidemiology have selected and “distilled” only three of these diseases as perfect candidates for the eponym: ergotism, erysipelas, and herpes zoster. Probably three in Medicine is by far too much. Physicians should then be careful when they diagnose a case of St. Anthony fire: are they dealing with a toxic, viral or bacterial disease?
Disclosures:
The images of the paintings are freely available on the internet. They have been published, according with Italian law, in low resolution format, only for scientific and didactic purposes, without any lucrative aim.
Conflict of interest:
Each author declares that he or she has no commercial associations (e.g. consultancies, stock ownership, equity interest, patent/licensing arrangement etc.) that might pose a conflict of interest in connection with the submitted article
References
- 1.Leider M. New York: McGraw-Hill; 1968. A Dictionary of Dermatologic Words, Terms and Phrases. [Google Scholar]
- 2.Farrer D. Oxford: Clarendon; 1978. The Oxford dictionary of saints. [Google Scholar]
- 3.Athanasius. Life of Antony. In: White C, editor. Early Christian Lives. London, England: Penguin Books; 1998. [Google Scholar]
- 4.A History of the Knights of Malta London. Longman, Brown, Green; 1858. Whitworth Porter. [Google Scholar]
- 5.Matossian MK. Yale University Press; 1989. Poisons of the Past. Molds, Epidemics, and History. New Haven, CT, and London. [Google Scholar]
- 6.van Wyk BE. Food Plants of the World. An Illustrated Guide. Portland, or: Timber Press. 2005 [Google Scholar]
- 7.Thoms H. John Stearns and pulvis parturiens. Am J Obstet Gynecol. 1931;22:418–423. [Google Scholar]
- 8.Behre KE. The history of rye cultivation in Europe. Vegetation History and Archaeobotany. 1992;1:141–156. [Google Scholar]
- 9.Cambridge, MA and London: Harvard University Press; 1950. Pliny: Natural History (Rackham H. transl.). Books XVII-XIX. [Google Scholar]
- 10.Clark BJ. The versatile ergot of rye. In: Parnham MJ, Bruinvels J, editors. Discoveries in pharmacology: haemodynamics, hormones, and inflammation. Amsterdam: Elsevier; 1984. pp. 3–33. [Google Scholar]
- 11.van Dongen PW, de Groot AN. History of ergot alkaloids from ergotism to ergometrine. Eur J Obstet Gynecol Reprod Biol. 1995;60:109–116. doi: 10.1016/0028-2243(95)02104-z. [DOI] [PubMed] [Google Scholar]
- 12.Heusinger TO Studien über den Ergotismus, insbesondere sein Auftreten im neunzehnten Jahrhundert; aus Anlass einer Epidemie in Oberhessen im Winter 1855/56. Marburg: Koch, 1856 [Google Scholar]
- 13.Tanner JR. St Anthony’s Fire, then and now: a Case Report and Historical Review. Can J Surg. 1987;30:291–293. [PubMed] [Google Scholar]
- 14.Haarmann T, Rolke Y, Goesbert S, et al. Ergot; from witchcraft to biotechnology. Molecular Plant Pathology. 2009;10:563–577. doi: 10.1111/j.1364-3703.2009.00548.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Barger G. Ergot and Ergotism. A Monograph. London, Edinburgh: Gurney and Jackson. 1931 [Google Scholar]
- 16.Pažotouvá S, Parberry DP. The taxononomy and phyogeny of Claviceps. In: Křen V, Cvak L, editors. Ergot. The Genus Claviceps. Amsterdam: Harwood Academic Publishers; 1999. [Google Scholar]
- 17.Pažoutová S, Olšovská J, Linka M, et al. Chemoraces and habitat specialization of Claviceps purpurea populations. Appl Environ Microbiol. 2000;66:5419–5425. doi: 10.1128/aem.66.12.5419-5425.2000. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Larsen Ø. Ergotisme - en svøpe gjennom århundrer [Ergotism: a plague throughout centuries] Liv og helse. 1965;5:106–109. [Google Scholar]
- 19.Myhre B, Øye I. Norges landbrukshistorie I. 4000 f. Kr. - 1350 e. Kr. Jorda blir levevei [Norwegian Agricultural History I. 4000 BC - 1350 ad. The Soil becomes a Way of Living]. Oslo: Det norske samlaget. 2002 [Google Scholar]
- 20.Holm T. Leiver frå soga um rugdbraudet og rygene [Slices of the history of rye bread and rygene [the people of Rogland]]. Norsk årbok, andre rekkja. 2008:47–95. [Google Scholar]
- 21.King B. Outbreak of ergotism in Wollo, Ethiopia. Lancet. 1979;2:1411. doi: 10.1016/s0140-6736(79)92050-6. [DOI] [PubMed] [Google Scholar]
- 22.Garcia de Yebenes J, Garcia de Yebenes P. Dystonia in the painting of Matias Grunewald. Epidemic ergotism in the late Middle Ages. Arch Neurobiol. 1991;54:37–40. [PubMed] [Google Scholar]
- 23.Reichborn-Kjennerud I. Vår gamle trolldomsmedisin. III [Our old witchcraft medicine. III]. Skrifter utgitt av Det norske videnskabs-akademi Oslo. II. Historisk-filosofisk klasse. 1940 [Google Scholar]
- 24.Caporael LR. Ergotism: the Satan loosed in Salem? Science. 1976;192:21–26. doi: 10.1126/science.769159. [DOI] [PubMed] [Google Scholar]
- 25.Bisno AL, Stevens DL. Streptococcal infections of skin and soft tissues. N Engl J Med. 1996;334:240–245. doi: 10.1056/NEJM199601253340407. [DOI] [PubMed] [Google Scholar]
- 26.Adams F. The genuine works of Hippocrates: translated from the Greek with a preliminary discourse and annotations. London: Sydenham Society; 1849. [Google Scholar]
- 27.Corbin. Remarks Tending to Elucidate the History of Erysipelas, and Especially of Phlegmonous Erysipelas. Lond Med Phys J. 1831;11:116–121. [PMC free article] [PubMed] [Google Scholar]
- 28.Billroth T. Untersuchungen über die Vegetationsformen von Coccobacteria septica und der Antheil, welchen sie an der Entstehung und Verbreitung der accidentellen Wundkrankheiten haben. Berlin: G. Reimer. 1874 [Google Scholar]
- 29.Billroth T. London: The New Sydenham Society; 1877. Lectures on surgical pathology and therapeutics. [Google Scholar]
- 30.Alouf JE, Horaud T. Streptococcal Research at Pasteur Institute from Louis Pasteur’s time to date. Adv Exper Med Biol. 1997;418:7–14. doi: 10.1007/978-1-4899-1825-3_4. [DOI] [PubMed] [Google Scholar]
- 31.Evans AC. Studies on Hemolytic Streptococci: II. Streptococcus pyogenes. J Bacteriol. 1936;31:611–624. doi: 10.1128/jb.31.6.611-624.1936. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Rosenbach FJ. Wiesbaden: Bergmann; 1884. Mikro-organismen bei den Wund-Infections-Krankheiten des Menschen. [Google Scholar]
- 33.Andrewes FW, Christie EM. The haemolytic streptococci: their grouping by agglutination. London: H.M. Stationery Office; 1932. [Google Scholar]
- 34.Asensi V, Asensi JM. St. Anthony’s fire. JAMA Dermatology. 2016;152:850. doi: 10.1001/jamadermatol.2015.5476. [DOI] [PubMed] [Google Scholar]
- 35.Weinberg JM. Herpes zoster: Epidemiology, natural history, and common complications. J Am Acad Dermatol. 2007;57:S130–S135. doi: 10.1016/j.jaad.2007.08.046. [DOI] [PubMed] [Google Scholar]
- 36.Hope-Simpson RE. The nature of herpes zoster: a long-term study and a new hypothesis. Proc R Soc Med. 1965;58:9–20. doi: 10.1177/003591576505800106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Arvin A. Aging, immunity, and the varicella-zoster virus. N Engl J Med. 2005;352:2266–2277. doi: 10.1056/NEJMp058091. [DOI] [PubMed] [Google Scholar]
- 38.Oxman MN, Levin MJ, Johnson GR, et al. for the Shingles Prevention Study Group. A vaccine to prevent herpes zoster and postherpetic neuralgia in older adults. N Engl J Med. 2005;352:2271–2284. doi: 10.1056/NEJMoa051016. [DOI] [PubMed] [Google Scholar]
- 39.Insinga RP, Itzler RF, Pellissier JM, et al. The incidence of herpes zoster in a United States administrative database. J Gen Intern Med. 2005;20:748–753. doi: 10.1111/j.1525-1497.2005.0150.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Gilden DH, Kleinschmidt-DeMasters BK, LaGuardia JJ, et al. Neurologic complications of the reactivation of varicella-zoster virus. N Engl J Med. 2000;342:635–645. doi: 10.1056/NEJM200003023420906. [DOI] [PubMed] [Google Scholar]
- 41.Schmader KE. Epidemiology and impact on quality of life of postherpetic neuralgia and painful diabetic neuropathy. Clin J Pain. 2002;18:350–354. doi: 10.1097/00002508-200211000-00002. [DOI] [PubMed] [Google Scholar]
- 42.Weller TH. Varicella and herpes zoster: changing concepts of the natural history, control, and importance of a not-so-benign virus. N Engl J Med. 1983;309:1362–1368. doi: 10.1056/NEJM198312013092205. [DOI] [PubMed] [Google Scholar]
- 43.Gnann JW, Jr, Whitley RJ. Clinical practice: herpes zoster. N Engl J Med. 2002;347:340–346. doi: 10.1056/NEJMcp013211. [DOI] [PubMed] [Google Scholar]
- 44.von Bòkay J. Über den ätiologischen Zusammenhang der Varizellen mit gewissen Fällen von Herpes. Zoster. Wien. Klin. Wochenschr. 1909;22:1323–1326. [Google Scholar]
- 45.Kundratitz K. Über die Ätiologie des Zoster and über seine Beziehungen zu Varizellen. Wien. Klin. Wochenschr. 1925;38:502–503. [Google Scholar]
- 46.Goodpasture EW, Anderson K. Infection of human skin, grafted on the chorioallantois of chick embryos with the virus of herpes zoster. Am J Pathol. 1944;20:447–455. [PMC free article] [PubMed] [Google Scholar]
- 47.Weller TH. Varicella and herpes zoster: a perspective and overview. J Infect Dis. 1992;166:S1–S7. [PubMed] [Google Scholar]
- 48.Flaubert G. La tentation de Saint Antoine. Paris, Charpentier & Cie. 1874 [Google Scholar]