

Objectives
Despite decades of research, improving health care safety remains a global priority. Individual studies have demonstrated links between staff engagement and care quality, but until now, any relationship between engagement and patient safety outcomes has been more speculative. This systematic review and meta-analysis therefore assessed this relationship and explored if the way these variables were defined and measured had any differential effect.
Methods
After systematic searches of Medline, CINAHL, PsycInfo, Embase, Cochrane Library, and National Institute for Health Research Journals databases, narrative and random-effects meta-analyses were completed, with pooled effect sizes expressed as Pearson r.
Results
Fourteen studies met the inclusion criteria, 11 of which were suitable for meta-analysis. Meta-analyses indicated a small but consistent, statistically significant relationship between staff engagement and patient safety (all outcomes; 11 studies; r = 0.22; 95% confidence interval [CI], 0.07 to 0.36; n = 30,490) and 2 patient safety outcome categories: patient safety culture (7 studies; r = 0.22; 95% CI, 0.01 to 0.41; n = 27,857) and errors/adverse events (4 studies; r = −0.20; 95% CI, −0.26 to −0.13; n = 2633). The specific approach to conceptualizing engagement did not affect the strength of the findings.
Conclusions
This is the first review to demonstrate a significant relationship between engagement and both safety culture scores and errors/adverse events. Despite a limited and evolving evidence base, we cautiously conclude that increasing staff engagement could be an effective means of enhancing patient safety. Further research is needed to determine causality and clarify the nature of the staff engagement/patient safety relationship at individual and unit/workgroup levels.
Key Words: patient safety, health care staff, engagement, patient outcomes
Improving health care safety is a global priority,1 having been identified as an issue approaching epidemic proportions.2 Despite major technological advances, modern-day health care delivery remains a human endeavor3 and health care safety primarily a function of human behavior and performance.2
Evidence outside health care demonstrates that engaged employees generally perform 20% better than their colleagues.4 Reports based on hospital-level data suggest staff engagement and health care safety performance may be strongly associated,3,5 for example, that engaged staff deliver better quality care,3,6 lower patient mortality,7 and better reporting of errors, near misses and incidents.6 Staff engagement has also been associated with lower staff turnover and reduced absenteeism,8 which are known to affect safety.9,10 Given this and the large variations in staff engagement levels between organizations,7,11,12 generalized interventions to increase staff engagement may be equally, if not more, impactful and cost-effective than local interventions addressing specific risks such as falls or pressure ulcers.
Staff engagement is a broad concept8 characterized by a fragmented and complex literature, with more than 50 definitions identified.11 One systematic review13 identified 6 definition categories. These were personal role engagement, work task or job engagement, multidimensional engagement, engagement as a composite attitudinal and behavioral concept, engagement as management practice, and self-engagement with performance. Definitions broadly fall into 2 overarching categories, one focusing on engagement as a personal state14 and the second on engagement as practice.15 It is important therefore to consider this distinction because it may have a bearing on how this relationship is conceptualized and measured.
Previous reviews have investigated the effectiveness of work engagement interventions,16,17 characteristics of engaged staff,18 how to enhance staff well-being,19 engagement outcomes for other staff groups,13,20 and engagement and care quality21 or have reviewed the association between engagement and safety but not specifically in health care.13,22 Thus, with one notable exception,23 there is a gap in the evidence base on the relationship between staff engagement and patient safety. Mossburg and Dennison-Himmelfarb23 reported a moderately strong positive association between engagement and patient safety culture, but limited evidence on the links between engagement and errors. They did, however, recommend further investigation of this relationship, including exploration of how engagement and patient safety are operationalized in the literature. They also highlighted the opportunity to move away from the traditional, deficit-based focus on burnout. This review addresses both of these gaps.
Before recommending staff engagement interventions as a target for improving patient safety, we must first understand the evidence regarding the nature of the relationship between these 2 constructs (engagement as a personal state versus engagement as practice) and whether this differs depending on the type of staff engagement or how we measure patient safety. This systematic review and meta-analysis therefore set out to answer the following research questions:
What is the strength of the relationship between staff engagement and patient safety outcomes?
Which conceptualization of staff engagement is most associated with patient safety outcomes?
METHODS
This review followed PRISMA guidelines24 (Fig. 1; preregistered at https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=108599).
FIGURE 1.
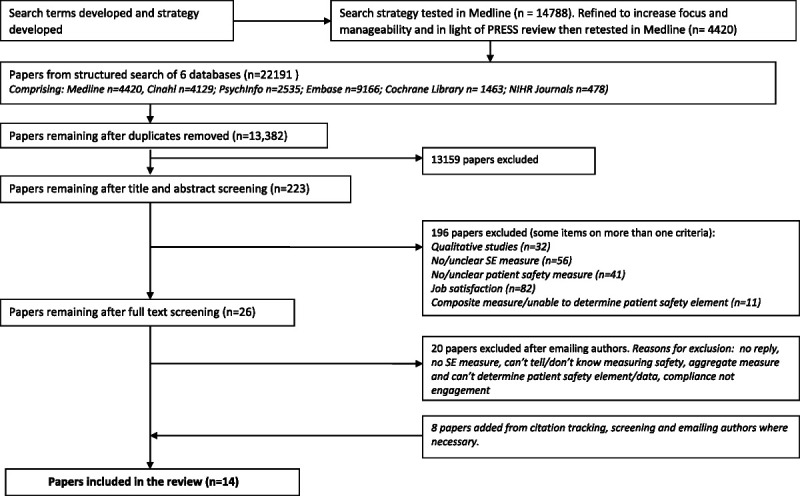
Overview of study selection process (PRISMA diagram).
Scope of the Review
Studies exploring the relationship between staff engagement and patient safety outcomes were included. With no consensus on the definition of staff engagement,13 studies addressing this concept in its broadest sense were considered based on 2 working definitions. The first, commonly used in the organizational psychology literature, conceptualizes engagement as a state:
“A positive, fulfilling, work-related state of mind that is characterized by vigor, dedication and absorption.”14(p74)
The second, broader definition, adopted by the UK National Health Service, emphasizes engagement as practice:
“….a positive attitude held by an employee toward the organisation and its values. An engaged employee is aware of business context and works with colleagues to improve performance within the job for the benefit of the organisation.”15(p4)
The review was limited to studies published in 1999 onward to correspond with the publication of To Err Is Human,5 the major catalyst for developing safer health care. Other inclusion criteria were as follows: peer-reviewed studies, published in English, involving health care staff, using quantitative methods/measures of staff engagement and patient safety, and cross-sectional, prospective, or interventional designs. Exclusion criteria were studies measuring satisfaction or composite quality of care from which patient safety could not be disaggregated.
Medline, CINAHL, PsycInfo, Embase, Cochrane Library, and National Institute for Health Research Journals databases were searched by an academic/health care librarian from January 1999 to February 2020 using 3 blocks of search terms/synonyms (health care staff, staff/employee engagement, patient safety/quality of care). The search strategy was tested in Medline, refined and retested after independent peer review using the Peer Review of Electronic Search Strategies guidelines25 (Supplementary File 1). We completed citation tracking of all included studies to identify additional studies. After the removal of duplicates, G.J. and T.M. independently screened all titles and abstracts, then full texts for potentially relevant records. Any discrepancy or uncertainty at any stage was resolved through full-text review and team discussion (J.J., R.L., L.B.). We contacted 19 authors for clarification of measures or unadjusted or item-level correlations; 1 author26 provided the data requested.
Data extraction and quality assessment templates were developed, piloted on 20% of the included articles (G.J., T.M., L.B.) and then iterated after team discussion. Extracted data comprised the following: author, setting, participant characteristics, staff engagement definition, sample size, study design, outcomes, measures, analysis method, inclusion/exclusion criteria, study limitations, and conclusions. Four reviewers (G.J., T.M., J.J., R.L.) independently categorized the engagement definitions from individual articles and through discussion arrived at a consensus categorization (Table 1). Data were independently extracted then agreed by G.J./T.M. (qualitative) and G.J./L.B. (quantitative). G.J./T.M. independently completed quality assessment for each study. Quality assessment comprised items from the guidance on the assessment of observational studies40 and Cochrane risk of bias tool plus “a priori,” team-defined criteria specific to our review.41 A score of 0 was awarded for criteria where information was indeterminable. Possible scores ranged from 0 to 6. A score of 5 to 6 was considered high; 3 to 4, fair; and 0 to 2, poor quality (Supplementary File 2).
TABLE 1.
Summary of Studies Included in the Review
| Source and Grouping(s) for Analysis | Setting | Professional Group and Sample | Quality Score | Staff Engagement Definition | Staff Engagement Measure | Patient Safety Measure | Summary Findings |
|---|---|---|---|---|---|---|---|
| Arnetz et al27 (United States)*†‡ | Nursing home | Mixed 312 |
3 | NHS (practice, personal) | Quality-Work Competence Questionnaire (employeeship scale: nonpunitive response to error, communication about incidents, compliance with safety procedures) | Nursing Home Survey on Patient Safety Culture | Employeeship and • Nonpunitive response to error (r = 0.21, P < 0.001) • Communication about incidents (r = 0.27, P < 0.001) • Compliance with safety procedures (r = 0.15, P < 0.001) |
| Collier and Fitzpatrick28 (United States)*‡ | Hospital (ITU) | Nurses 26 units |
3 | Gallup Q12 (practice, organizational) | Gallup Q12 | HSOPSC | Engagement and • Total safety scores (r = 0.65, P < 0.01), although big variations in safety scores between units (41%–82%) • All 12 dimensions of SAQ, 9 of which were significant, including • Frequency incident reporting (r = 0.56, P < 0.01) • Overall perceptions safety (r = 0.43, P < 0.05) • Significant result for one hospital-level dimension, teamwork across hospital units (r = 0.46 P < 0.05) |
| Daugherty-Biddison et al29 (United States) *‡ |
Hospital | Mixed 58–68 units ×3 |
3 | Gallup (practice, organizational) | Gallup Q12 | SAQ | Engagement and unit-level safety climate in all 4 domains of SAQ at 3 time points, all P < 0.001: Spearman ρ = 0.69 (58 units, 2009) ρ = 0.57 (68 units, 2011) ρ = 0.43 (59 units, 2013) |
| Georganta et al30 (Europe)*§ | Hospital | Mixed 532 |
4 | Schaufeli (state) | UWES | HSOPSC | Number of events reported and • Vigor: r = 0.06 (n/s) • Dedication: r = 0.13 (P < 0.01) Frequency events reported and • Vigor: r = 0.10 (P < 0.05) • Dedication: r = 0.10 (P < 0.05) |
| Horwitz and Horwitz31 (United States)*‡ | Hospital | Doctors 63 |
1 | NHS (practice, personal) | OCQ (short version) | Patient Safety Climate in Healthcare Organisations | Affective commitment and perception of patient safety culture: r = 0.26 (P < 0.05) |
| Lotfi et al32 (Tehran)*‡ |
Hospital | Nurses 340 |
3 | NHS (practice, personal) | OCQ | HSOPSC | Affective commitment and perception of patient safety culture: r = 0.08 (P = 0.13, n/s) |
| Lowe26 (Canada)*‡ | Hospital | Mixed 27,018 |
1 | NHS (practice, personal) | Engagement Scale | Patient Safety Culture Scale | • No correlations were published. The narrative outlines a consistently strong relationship between engagement and organizational performance (e.g., errors and near misses, and safety culture) • 58% of highly engaged employees were in top quartile of patient safety culture scores, and only 3% in lowest quartile. Note: Pearson r was calculated for our meta-analysis from unpublished data provided by the author at our request (see Supplementary file 3) |
| Prins et al33 (the Netherlands)†§ | Hospital | Doctors 2,115 |
2 | Schaufeli (state) | UWES | Self-reported error questionnaire | Total engagement score and • Action/inexperience errors: r = −0.07 (P < 0.001) • Errors due to lack of time: r = −0.22 (P < 0.001) Action/inexperience errors and • Vigor: r = −0.09 (n/s) • Dedication: r = −0.07 (n/s) • Absorption: r = −0.03 (n/s) Errors due to lack of time and • Vigor: r = −0.23 (P < 0.001) • Dedication: r = −0.24 (P < 0.001) • Absorption: r = −0.11 (P < 0.001) |
| Rathert et al34 (United States)*ठ|
Hospital | Mixed 252 | 2 | Schaufeli (state) and NHS (practice, personal) | • Adapted Engagement Scale • OCQ |
HSOPSC | Overall patient safety perceptions and • Engagement: r = −0.14 (P < 0.01; note: direction as expected based on the way the items are constructed) • Organizational commitment: r = 0.40 (P < 0.01) |
| Rezaiamin et al35 (Tehran)†‡ |
Hospital (ITU) | Nurses 117 |
4 | NHS (practice, personal) | Work Commitment Scale | Medication errors | Work commitment and medication errors: • Total errors: r = −0.25 (P = 0.006) • IV: r = −0.21, (P = 0.02) • Non-IV: r = −0.27 (P = 0.003) Multiple linear regression (age, sex, etc. adjusted) was consistent: • Total errors β = −0.27 (P = 0.02) • IV errors β = −0.12 (P = 0.06) • Non-IV = β = −0.15 (P = 0.01) |
| Teng et al36 (Taiwan)†‡ |
Hospital | Nurses 284 (as best we can determine) |
5 | NHS (practice, personal) | Professional Commitment Questionnaire | 6 measures of patient safety | Engagement and overall patient safety: r = 0.19 (P < 0.05) Adjusted for nurse working experience, regression showed associations with injuries due to care (β = 0.16, P < 0.05), patient falls (β = 0.12, P < 0.05), nosocomial infections (β = 0.11, P = 0.07), medication errors (β = 0 0.18, P < 0.01), incomplete/incorrect documentations (β = 0.18, P < 0.01), and delayed care and overall patient safety (β = 0.19, P < 0.01) |
| Thorp et al37 (United States)*‡ |
Hospital | Mixed Max 129 units 2009 |
6 | Gallup (practice, organizational) | Gallup Q12 | HSOPSC | Mean engagement scores in 2007 predicted 2009 patient safety scores (β = 0.77, P < 0.001; among other supporting results) |
| Toode38 (Estonia)*†‡ |
Hospital | Nurses 201 |
3 | NHS (practice, personal) | Engagement/empowerment scale (from Healthcare Team Vitality Instrument) | HSOPSC | Engagement and empowerment in the unit and • Overall perceptions of patient safety: r = 0.44 (P < 0.001) • Patient safety grade in unit: r = 0.20 (P < 0.01) • Frequency of events reported in unit: r = 0.23 (P < 0.001) • Self-reported events during last 12 mo: r = 0.24 (P < 0.001) |
| Tsiga et al39 (Greece)†§ |
Hospital | Doctors 117 |
2 | Schaufeli (state) | UWES | Medical Error Checklist | Engagement and errors: Surgeons (n = 117) r = −0.33 (P < 0.001) Internists (n = 66) = not reported Pediatricians (n = 48) = not reported |
*Staff engagement versus patient safety culture.
†Staff engagement versus errors/adverse events.
‡Staff engagement as practice versus patient safety.
§Staff engagement as state versus patient safety.
ITU, intensive therapy unit; OCQ, Organizational Commitment Questionnaire; SAQ, Safety Attitudes Questionnaire: UWES, Utrecht Work Engagement Scale.
Narrative analysis appraised studies according to research design, country, participant group, setting, engagement definition, patient safety outcome, and measures. Study information was systematically tabulated and patterns within and between studies were explored to identify commonalities/differences and potential reasons for these.
Meta-analyses were conducted using random-effects weighting (DerSimonian-Laird) and Fisher z to r back-transformation method, using R Studio (version 3.5.2)42 with the Metacor (https://repo.bppt.go.id/cran/web/packages/metacor/metacor.pdf) package.43 The pooled effect size metric was Pearson r, based on unadjusted correlations where possible. Effects sizes of r = 0.10, 0.30, and 0.50 were considered small, medium, and large, respectively.44 Where other effect metrics (e.g., Spearman ρ) or summary data were reported, r was estimated using conversion formulas (Supplementary File 3). To mitigate violations of statistical independence, average effect across measures was taken for studies with 2 or more measures of interest (e.g., subscales)45; Supplementary File 3).
Aside from overall pooled analyses, studies were pooled separately according to staff engagement definition groups, such as engagement-as-practice and engagement-as-state, and outcome types, such as patient safety culture (a higher positive r was deemed favorable) and self-reported adverse errors/events (a higher negative r was deemed favorable), where effect size directions were altered as appropriate. An exploratory meta-regression analysis assessed whether any of the aforementioned engagement definitions was more highly associated with patient safety.
Heterogeneity was assessed with Cochran Q statistic and related I2 statistic. Funnel plots were generated and used to provide some insight into small study bias (an indicator of publication bias), alongside Kendall τ, Egger regression, and failsafe N (Orwin method) statistics. All analyses were subject to leave-one-out sensitivity analyses.46
RESULTS
Systematic searching yielded 13,382 records after the removal of duplicates. Study selection (Fig. 1) resulted in 14 studies eligible for the overall review and 11 for meta-analysis. Table 1 summarizes the studies included in the review. Seven were from North America/Canada,26–29,31,34,37 4 from Europe30,32,38,39 and 3 from the Middle/Far East.32,35,36 Thirteen were cross-sectional, and 1 was non–cross-sectional.37 All but 1 study27 were hospital based. Six involved mixed staff groups26,27,29,30,34,37; 5, nurses only28,32,35,36,38; and 3, doctors only.31,33,39 The relationship between our variables of interest was a secondary or incidental objective in half of the eligible studies.30,31,34,35,37–39 Only 2 studies were deemed of high quality (scoring 5–6 in the quality assessment)36,37; 7, fair (scoring 3–4)27–30,32,35,38; and 5, poor (scoring 0–2)26,31,33,34,39 (Supplementary File 2). Samples ranged from 63 (doctors only)31 to 27,0181 (mixed staff group)26 for participant-level data and from 26 (nurses only groups)28 to 68 (mixed staff groups)29 for unit-level data. Ten studies measured patient safety culture, and 4 measured the number of errors/adverse events. Of the studies included, 3 used the Hospital Survey of Patient Safety Culture (HSOPSC) measure and reported subscale scores. One subscale of this questionnaire assesses the frequency of errors/events reporting. This was considered a safety culture rather than adverse events measure because it reflects reporting culture rather than the frequency of events occurring.
The main and subgroup analyses are reported by research question.
Question 1: What is the strength of the relationship between staff engagement and patient safety outcomes?
All 14 studies reported a relationship between staff engagement and patient safety in the predicted direction except for one engagement measure in a dual-measure study.34 All results were statistically significant except 1 study32 and 1 subscale (the number of reported events) in a multioutcome study.30 Eleven of the 14 were suitable for inclusion in a meta-analysis of studies measuring any patient safety outcome and any definition of engagement. Random-effects meta-analysis suggested a small to medium positive, significant relationship between engagement and patient safety (r = 0.22; 95% confidence interval [CI], 0.07–0.36; n = 30,490) with considerable heterogeneity (P < 0.01; I2 = 98%; Fig. 2).
FIGURE 2.
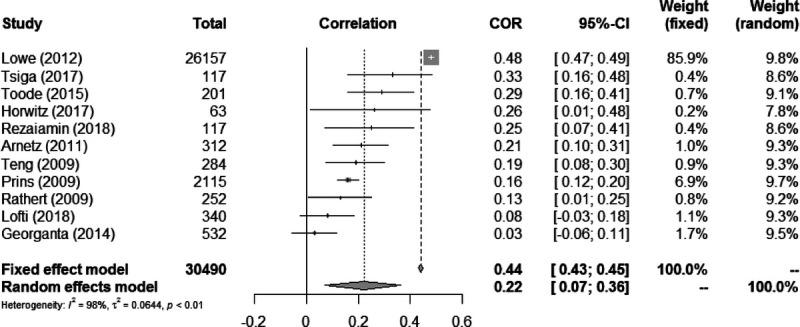
Patient safety and staff engagement (n = 11).
Three studies28,29,37 were excluded from all meta-analyses because they reported unit-level analyses (pooling unit and participant-level data would bias the meta-analyses by artificially lending more weight to participant-level studies that had much higher n values). Their findings were consistent with the aforementioned meta-analysis. Two reported stronger effects than the individual-level studies: r = 0.65 (for patent safety culture), r = 0.56 (for frequency of incident reporting (both P < 0.01),28 and Spearman ρ = 0.69, 0.57, and 0.44 (P < 0.001; for patient safety culture at 3 time points).29 The third also supported the meta-analysis findings (β = 0.75, P < 0.001)37 (see Supplementary File 3 for small, unit-level–only meta-analysis).
The Relationship Between Staff Engagement and Patient Safety by Outcome Group
Safety outcomes were broadly categorized as follows: patient safety culture and errors/adverse events. Three studies28,30,38 reported on both these outcomes.
Staff Engagement and Patient Safety Culture
Ten studies explored this relationship; 6 included mixed staff groups,26,27,29,30,34,37 3 included nurses only,28,32,38 and 1 included doctors only.31 The most frequent patient safety culture measure, used by half of these 10 studies, was the HSOPSC. Nine of the 10 reported positive, statistically significant correlations. The 7 studies suitable for meta-analysis showed a small positive, significant association (r = 0.22; 95% CI, 0.01–0.41; n = 27,857) with considerable heterogeneity (P < 0.01; I2 = 98%; Fig. 3).
FIGURE 3.
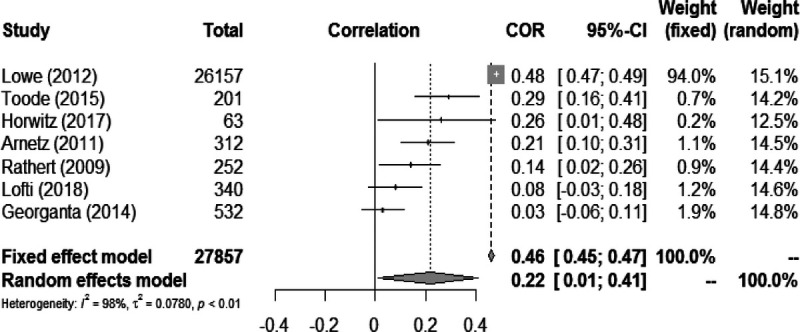
Engagement × patient safety culture (n = 7).
Three unit-level studies were excluded from this meta-analysis. Two involved mixed staff groups. The first and highest-quality study in the review37 reported a positive association of engagement with a validated index of patient safety culture (β = 0.75, P < 0.001). The second29 found strong, significant correlations between staff engagement and all 4 domains of the Safety Attitudes Questionnaire (mean Spearman ρ = 0.69 [in 2009], 0.57 [in 2011], 0.43 [in 2013]; P < 0.001). The third, smaller study of nurses in 26 units28 found a strong, positive relationship between staff engagement and total patient safety culture scores (r = 0.65, P < 0.01) and with 9 of the 12 safety dimensions of the HSOPSC (Table 1).
Staff Engagement and Errors/Adverse Events
Seven studies examined this relationship. All were cross-sectional. Five were of good or fair quality,28,30,35,36,38 and 2 were of poor quality.33,39 More than half involved only nurses28,35,36,38; 2, only doctors33,39; and 1, a mixed staff group.30 Three studies used the HSOPSC self-reported events subscale and so were not included in this meta-analysis. This is because the HSOPSC measures reporting culture rather than incident rates and would therefore be hypothesized as positively related to staff engagement, whereas incident rates are predicted to be correlated in a negative direction. Pooled analysis of the 4 studies measuring the number of errors/adverse events indicated that higher engagement had a small, inverse relationship with errors/events (r = −0.20; 95% CI, −0.26 to −0.13; n = 2633) with low heterogeneity (P = 0.22; I2 = 32%; Fig. 4).
FIGURE 4.
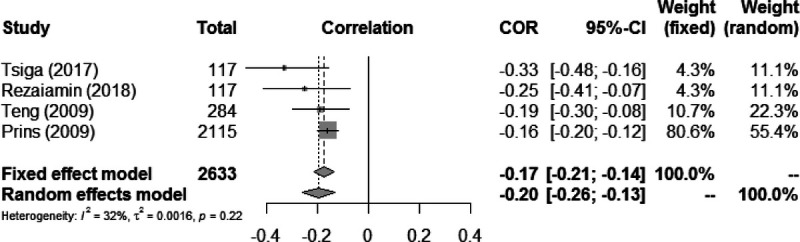
Engagement × errors/events/incidents (n = 4).
Question 2: Which conceptualization of staff engagement is most closely associated with patient safety outcomes?
Studies conceptualized staff engagement in 2 main ways: engagement-as-practice (n = 11) and engagement-as-state (n = 4), although one reflected both.34 Of the 11 adopting an engagement-as-practice approach, 8 reflected the definition of engagement-as-personal-practice.26,27,31,32,34–36,38 The other 3 had an engagement-as-organizational-practice focus28,29,37 and used the Gallup Q12 questionnaire.4
Engagement-as-Practice and Patient Safety Outcomes
Pooled analysis of 8 studies indicated that staff engagement-as-practice showed a small, significant positive association with patient safety (r = 0.21, 95% CI, 0.01–0.39; n = 27,726) with high heterogeneity (P < 0.01, I2 = 97%; Supplementary File 3). The 3 unit-level studies unsuitable for meta-analysis consistently supported these findings, all reporting highly significant, moderate to strong correlations of r = 0.65 (safety culture) and 0.56 (frequency of incident reporting; P < 0.01)28; r = 0.69, 0.57, and 0.44 (safety culture at 3 time points; P < 0.001)29; and β = 0.75 (safety culture; P < 0.001).37
Engagement-as-State and Patient Safety Outcomes
Four studies addressed this relationship, with 2 using mixed staff groups30,34 and 2 using doctors only.33,39 One was of fair30 and the other 3 were of poor quality.33,34,39 All were suitable for meta-analysis. The pooled effect showed a small, positive correlation (r = 0.22; 95% CI, 0.08–0.36; n = 3016) and high heterogeneity (P < 0.01, I2 = 90%; Supplementary File 3).
A meta-regression assessed whether the 2 definitions of engagement had differential effects on patient safety. One study measuring staff engagement in both ways34 was excluded from this analysis (to mitigate dependency), and meta-regression showed no significant differences (β = 0.09; 95% CI, −0.17 to 0.34; P = 0.50).
Sensitivity Analyses
Although there was some evidence of small study bias, the overall pooled analysis was robust in leave-one-out analyses. When stratified by outcome type, the significance of the effect size of pooled errors outcome was unaffected in leave-one-out analyses, but the safety culture outcome became marginally nonsignificant when excluding 3 studies.27,31,38 When studies were stratified by engagement concept, leave-one out analyses rendered the pooled effect sizes for engagement-as-state marginally nonsignificant when 1 study33 was excluded and similarly for engagement-as-practice in respect of 5 studies.27,31,35,36,38 All leave-one-out analyses effects were in the same direction as the main analyses; thus, lack of significance may have been driven by type II error given the small number of studies and moderate effect sizes. Full details are given in Supplementary File 3.
DISCUSSION
Extensive research has demonstrated links between staff engagement and work performance in non–health care4,11 and health care settings.7,47 There is also compelling evidence of links between staff engagement and care quality.48–50 However, links between staff engagement and patient safety specifically have been more speculative.23 This systematic review and meta-analysis therefore explored whether the beneficial relationship between staff engagement and safety outcomes identified in other sectors was evident in health care and whether how these concepts were defined and measured made any difference.
This review is only the second exploring this relationship and the first to demonstrate a consistent, statistically significant relationship between reported engagement and both safety culture scores and errors/events. The previous review23 explored relationships between burnout and staff engagement with patient and staff safety outcomes. We used a more comprehensive search strategy and focused specifically on patient safety outcomes. We identified more eligible studies but excluded 2 they included. This could partly explain why this review reports a smaller though consistent relationship with both safety outcomes, whereas its forerunner23 found inconsistent findings regarding engagement and errors.
The broadly consistent and statistically significant beneficial relationship we found between staff engagement and patient safety (all outcomes) and both safety outcome categories (i.e., patient safety culture and errors/adverse events) indicates that the relationship previously identified elsewhere is also present in health care. Although the relationship was small for the individual-level studies, the 3 unit-level studies28,29,37 consistently reported strong correlations, which may warrant further research. A large study,51 although not specific to health care or safety, found that group-level performance outcomes were positively related to group-level engagement, which itself was positively related to but distinct from individual engagement, pointing to nuanced relationships between these concepts. The unit-level studies in our review all featured an “engagement as organizational practice” approach using the Gallup Q12 tool52 but indicate this nuanced relationship could also be true in health care settings; therefore, research to determine if and how patient safety outcomes are influenced by specific, yet unknown, group-level engagement may be warranted. This is particularly so given the complex, interprofessional and collaborative nature of health care.
Regarding the review’s second aim, it seems the way staff engagement was conceptualized did not differentially affect safety outcomes. There was a small positive association between patient safety (all outcomes) and both conceptions of staff engagement (i.e., engagement-as-practice and engagement-as-state). Contrary to the dominance of the psychological state definition previously reported,7 the majority of studies we reviewed investigated engagement as practice. Our review also identified that only 2 of the 6 engagement categories identified by a cross-sector review13 have been studied in relation to patient safety, indicating potential gaps in health research regarding the other 4: personal role engagement, multidimensional engagement, engagement as management practice, self-engagement with performance.
Nevertheless, the findings indicate that this may be a very important area of focus for safety interventions in the future. They support expert opinion that engaging staff by enabling them to raise concerns and contribute to service improvement can prevent poor-quality care.26,53,54 They also illustrate the potential of staff engagement as a strategy for building safety into health care, as has repeatedly been advocated.2,5,6 Furthermore, our findings are consistent with others arguing that effective systems and processes alone cannot improve safety5,7; therefore “…accelerated evolution…” and evaluation of the impact of organizational models on staff engagement and outcomes are also needed.6(p42) Thus, although staff engagement is nuanced in nature12 and varies between organizations3,50 developing this broader approach to patient safety has the potential for significant gains and provides unprecedented opportunities for achieving multiple, complementary benefits at scale.
Improving patient safety remains a global policy priority, but the human-centric nature of health care delivery means achieving this is dependent on an appropriately skilled and engaged workforce of sufficient number. This review provides the foundation for a potentially fruitful yet underexplored research and policy agenda to support the achievement of this aim. Further research is needed to clarify the nature and confirm the magnitude of the relationship between staff engagement and patient safety outcomes identified. The call for longitudinal studies, made more than a decade ago,4 to help determine causality remains unanswered. In addition, exploring the impact of generalized staff engagement interventions on patient safety outcomes compared with the traditional focus on safety interventions to address specific risks, for example, falls or pressure ulcers, is likely to prove fruitful. Finally, studies in a broader range of health care settings, involving a wider range of staff groups at unit/team and individual levels, would inform the effective development and testing of safety improvement interventions.
Including a broad range of relevant databases, terms and independent peer review enabled a robust and comprehensive but focused review. This was important given the lack of consensus on the definition of engagement and broad range of patient safety outcomes in use. Independent screening and data extraction by 2 reviewers and consensus decision making within the review team enhanced rigor.
LIMITATIONS
These findings must be interpreted in the context of the limited evidence base, with few studies specifically addressing the relationship between staff engagement and patient safety outcomes. In addition, the varied safety outcomes and measurement tools used makes direct comparison challenging. Current evidence is primarily correlational, so causality cannot be inferred. There is also a focus on hospital settings involving mainly doctors and nurses. This limits transferability to other parts of the health system, with different characteristics and priorities potentially affecting the staff engagement/patient safety relationship. Thus, our findings support a previous call12 for multicenter studies across health services.
The quality assessment tool was designed for this study. Although based on validated sources, it was not previously tested. The review includes 2 high-quality studies36,37 but study quality overall was only fair. All studies used self-reporting that features inherent risk of bias compared with objective measurement. The correlational nature of the eligible studies prevented any inference of causality. Exclusion of qualitative studies and gray literature means useful insights may be missing, particularly as the peer-reviewed literature is relatively limited. In addition, several analyses exhibited high heterogeneity, which may be due to the varied study quality, sample characteristics, measurement tools, outcome measures, and conceptions of engagement used. This reflects the conceptual ambiguities in the developing engagement/safety literature.13,23
CONCLUSIONS
The review identified a small but consistent and significant relationship between staff engagement and both patient safety culture and errors/events, the strength and certainty of which vary between contexts and specific outcome measures. Although the findings need cautious interpretation, increasing staff engagement could offer an impactful and cost-effective means of enhancing a range of patient safety outcomes.
ACKNOWLEDGMENT
This research was funded by the National Institute for Health Research (NIHR) Yorkshire and Humber Patient Safety Translational Research Centre (NIHR YH PSTRC). The views expressed in this article are those of the authors and not necessarily those of the NHS, the NIHR, or the Department of Health and Social Care.
We would like to thank Dr Max McLean, Ms Federica Bianchini/Ms Kirstine McDermid, and Dr Jonathan Benn for their contribution to the development of the review aims, execution of searches, and peer review of the search strategy, respectively.
For the meta-analysis, this was higher because the data set provided to us from the author included more participants.
The authors disclose no conflict of interest.
Contributor Information
Thomas Mills, Email: tom.mills@york.ac.uk.
Luke Budworth, Email: Luke.Budworth@bthft.nhs.uk.
Judith Johnson, Email: j.johnson@leeds.ac.uk.
Rebecca Lawton, Email: r.j.lawton@leeds.ac.uk.
REFERENCES
- 1.WHO Director General . Patient Safety: Global Action on Patient Safety [Internet]. 72nd World Health Assembly. 2019. Available at: http://apps.who.int/gb/ebwha/pdf_files/WHA72/A72_26-en.pdf. Accessed May 1, 2020.
- 2.Flott K, Fontana G, Darzi A. The Global State of Patient Safety. London, UK: Imperial College London; 2019. [Google Scholar]
- 3.The Kings Fund . Staff Engagement: Six Building Blocks for Harnessing the Creativity and Enthusiasm of NHS Staff. London, UK: The Kings Fund; 2015. [Google Scholar]
- 4.Robertson-Smith G, Marwick C. Employee Engagement: A Review of Current Thinking. Brighton: Institute for Employment Studies; 2009. [Google Scholar]
- 5.Institute of Medicine . Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: National Academy Press; 2001. [Google Scholar]
- 6.Ham C. Improving NHS Care by Engaging Staff and Devolving Decision-Making: Report of the Review of Staff Engagement and Empowerment in the NHS. London, UK: The Kings Fund; 2014. [Google Scholar]
- 7.West MA, Dawson JF. Employee Engagement and NHS Performance. London, UK: The King’s Fund; 2012. [Google Scholar]
- 8.West M Dawson J, et al. NHS Staff Management and Health Service Quality. Birmingham: Aston Business School; 2011. Available at: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/215455/dh_129656.pdf. Accessed May 1, 2020. [Google Scholar]
- 9.Griffiths P Ball J Drennan J, et al. Nurse staffing and patient outcomes: strengths and limitations of the evidence to inform policy and practice. A review and discussion paper based on evidence reviewed for the National Institute for Health and Care Excellence Safe Staffing guideline development. Int J Nurs Stud. 2016;63:213–225. [DOI] [PubMed] [Google Scholar]
- 10.Griffiths P Ball J Drennan J, et al. The Association Between Patient Safety Outcomes and Nurse/Healthcare Assistant Skill Mix and Staffing Levels & Factors That May Influence Staffing Requirements. Southampton, England: University of Southampton, Centre for Innovation and Leadership in Health Sciences; 2014. [Google Scholar]
- 11.MacLeod D, Clarke N. Engaging for Success: Enhancing Performance Through Employee Engagement. London, UK: Crown; 2009. [Google Scholar]
- 12.Jeve YB, Oppenheimer C, Konje J. Employee engagement within the NHS: a cross-sectional study. Int J Health Policy Manag. 2015;4:85–90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Bailey C Madden A Alfes K, et al. The meaning, antecedents and outcomes of employee engagement: a narrative synthesis. Int J Manag Rev. 2017;19:31–35. [Google Scholar]
- 14.Schaufeli WB Salanova M Gonzalez-Roma V, et al. The measurement of engagement and burnout: a two sample confirmatory factor analytic approach. J Happiness Stud. 2002;3:71–92. [Google Scholar]
- 15.Robinson D, Perryman S, Hayday S. The Drivers of Employee Engagement. IES Report 408. Brighton, UK: Institute of Employment Studies; 2004. [Google Scholar]
- 16.Carolan S, Harris PR, Cavanagh K. Improving employee well-being and effectiveness: systematic review and meta-analysis of web-based psychological interventions delivered in the workplace. J Med Internet Res. 2017;19:e271. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Knight C, Patterson M, Dawson J. Building work engagement: a systematic review and meta-analysis investigating the effectiveness of work engagement interventions. J Organ Behav. 2017;38:792–812. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Bakker AB Schaufeli WB Leiter MP, et al. Work engagement: an emerging concept in occupational health psychology. Work Stress. 2008;22:187–200. [PubMed] [Google Scholar]
- 19.Bailey C Madden A Alfes K, et al. Evaluating the Evidence on Employee Engagement and Its Potential Benefits to NHS Staff: A Narrative Synthesis of the Literature. Southampton, UK: NIHR Journals Library. NIHR funded: Health Services and Delivery Research, 12/5004/01—Enhancing and Embedding Staff Engagement in the NHS: Putting Theory Into Practice; 2015. [PubMed] [Google Scholar]
- 20.Keyko K Cummings GG Yonge O, et al. Work engagement in professional nursing practice: a systematic review. Int J Nurs Stud. 2016;61:142–164. [DOI] [PubMed] [Google Scholar]
- 21.Garcia-Sierra R, Fernandez-Castry J, Martinez-Zaragoza F. Work engagement in nursing: an integrative review of the literature. J Nurs Manag. 2015;24:E101–E111. [DOI] [PubMed] [Google Scholar]
- 22.Nahrgang JD, Morgeson FP, Hoffmann DA. Safety at work: a meta-analytic investigation of the link between job demands, job resources, burnout, engagement, and safety outcomes. J Appl Psychol. 2011;96:71–94. [DOI] [PubMed] [Google Scholar]
- 23.Mossburg S, Dennison-Himmelfarb C. The association between professional burnout and engagement with patient safety culture and outcomes: a systematic review. J Patient Saf. 2018. [DOI] [PubMed] [Google Scholar]
- 24.Moher D Librati A Tetzlaff J, et al. Preferred reporting items for systematic reviews and meta-analyses the PRISMA statement. PLoS Med. 2009;6:e1000097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.McGowan J Sampson M Salzwedel DM, et al. PRESS peer review of electronic search strategies: 2015 guideline statement. J Clin Epidemiol. 2016;75:40e46. [DOI] [PubMed] [Google Scholar]
- 26.Lowe G. How employee engagement matters for hospital performance. Healthc Q. 2012;15:29–39. [DOI] [PubMed] [Google Scholar]
- 27.Arnetz JE Zhdanova LS Elsouhag D, et al. Organizational climate determinants of resident safety culture in nursing homes. Gerontologist. 2011;51:739–749. [DOI] [PubMed] [Google Scholar]
- 28.Collier SL, Fitzpatrick JJ. Employee engagement and a culture of safety in the intensive care unit. J Nurs Adm. 2016;46:49–54. [DOI] [PubMed] [Google Scholar]
- 29.Daugherty-Biddison EL Paine L Murakami P, et al. Associations between safety culture and employee engagement over time: a retrospective analysis. BMJ Qual Saf. 2016;25:31–37. [DOI] [PubMed] [Google Scholar]
- 30.Georganta K, Panagopoulou E, Montgomery A. Talking behind their backs: negative gossip and burnout in hospitals. Burn Res. 2014;1:76–81. [Google Scholar]
- 31.Horwitz SK, Horwitz IB. The effects of organizational commitment and structural empowerment on patient safety culture. J Health Organ Manag. 2017;31:10–27. [DOI] [PubMed] [Google Scholar]
- 32.Lotfi Z Atashzadeh-Shoorideh F Mohtashami J, et al. Relationship between ethical leadership and organisational commitment of nurses with perception of patient safety culture. J Nurs Manag. 2018;26:726–734. [DOI] [PubMed] [Google Scholar]
- 33.Prins JT van der Haijden FMMA Hoekstra-Weebers JEHM, et al. Burnout, engagement and resident physicians’ self-reported errors. Psychol Health Med. 2009;16:654–666. [DOI] [PubMed] [Google Scholar]
- 34.Rathert C, Ishqaidef G, May DR. Improving work environments in health care: test of a theoretical framework. Health Care Manage Rev. 2009;34:334–343. [DOI] [PubMed] [Google Scholar]
- 35.Rezaiamin A Pazokian M Tafreshi MZ, et al. The relationship between work commitment, dynamic, and medication error. Clin Nurs Res. 2018;27:660–674. [DOI] [PubMed] [Google Scholar]
- 36.Teng C-I Dai Y-TD Shyu Y-IL, et al. Professional commitment, patient safety and patient-perceived care quality. J Nurs Scholarsh. 2009;41:301–309. [DOI] [PubMed] [Google Scholar]
- 37.Thorp J Baqai W Witters D, et al. Workplace engagement and workers’ compensation claims as predictors for patient safety culture. J Patient Saf. 2012;8:194–201. [DOI] [PubMed] [Google Scholar]
- 38.Toode K. Hospital nurses’ working conditions in relation to motivation and patient safety. Nurs Manag (Harrow). 2015;21:31–41. [DOI] [PubMed] [Google Scholar]
- 39.Tsiga E, Panagopoulou E, Montgomery A. Examining the link. between burnout and medical error: A checklist approach. Burn Res. 2017;6:1–8. [Google Scholar]
- 40.Thomas BH Ciliska D Dobbins M, et al. A process for systematically reviewing the literature: providing the research evidence for public health nursing interventions—worldviews on evidence-based nursing: Sigma Theta Tau International. Honor Soc Nurs. 2004;1:176–184. [DOI] [PubMed] [Google Scholar]
- 41.Hall L Johnson J Watt I, et al. Healthcare staff wellbeing, burnout, and patient safety: a systematic review. PLoS One. 2016;11:e0159015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.R Core Team . R: A Language and Environment for Statistical Computing. Vienna, Austria: R Foundation for Statistical Computing; 2019. Available at: https://www.R-project.org/. Accessed May 1, 2020. [Google Scholar]
- 43.Metacor package [computer programme]. Available at: https://repo.bppt.go.id/cran/web/packages/metacor/metacor.pdf. Accessed May 1, 2020.
- 44.Cohen J. A power primer. Psychol Bull. 1992;112:155–159. [DOI] [PubMed] [Google Scholar]
- 45.Scammacca N, Roberts G, Stuebing KK. Meta-analysis with complex research designs: dealing with dependence from multiple measures and multiple group comparisons. Rev Educ Res. 2014;84:328–364. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Higgins JP Thompson SG Deeks J, et al. Measuring inconsistency in meta-analyses. BMJ. 2003;327:557–560. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Simpson MR. Engagement at work: a review of the literature. Int J Nurs Stud. 2009;46:1012–1034. [DOI] [PubMed] [Google Scholar]
- 48.NHS Improvement . Interim NHS People Plan. London, UK: NHS Improvement; 2019. [Google Scholar]
- 49.The Kings Fund. In: Closing the Gap: Key Areas for Action on the Health and care Workforce. London, UK: The Kings Fund; 2019. [Google Scholar]
- 50.The Kings Fund. In: Leadership and Engagement for Improvement in the NHS: Together We Can. London, UK: The Kings Fund; 2012. [Google Scholar]
- 51.Luth MT, May DR. Toward a multilevel framework of engagement and performance at work. Acad Manag Proc. 2012;1. Published Online: November 30 2017. Available at: 10.5465/AMBPP.2012.14. Accessed May 7, 2020. [DOI] [Google Scholar]
- 52.Harter JK Schmidt FL Killham EA, et al. Q12 Meta-analysis: The Relationship Between Engagement at Work and Organisational Outcomes. Washington, DC: Gallup Inc; 2009. [Google Scholar]
- 53.Francis R. Report of the Mid Staffordshire NHS Foundation Trust Public Inquiry. London, UK: Crown; 2013. [Google Scholar]
- 54.Berwick D. A Promise to Learn–—A Commitment to Act. London, UK: Crown; 2013. [Google Scholar]