
Figure 2.
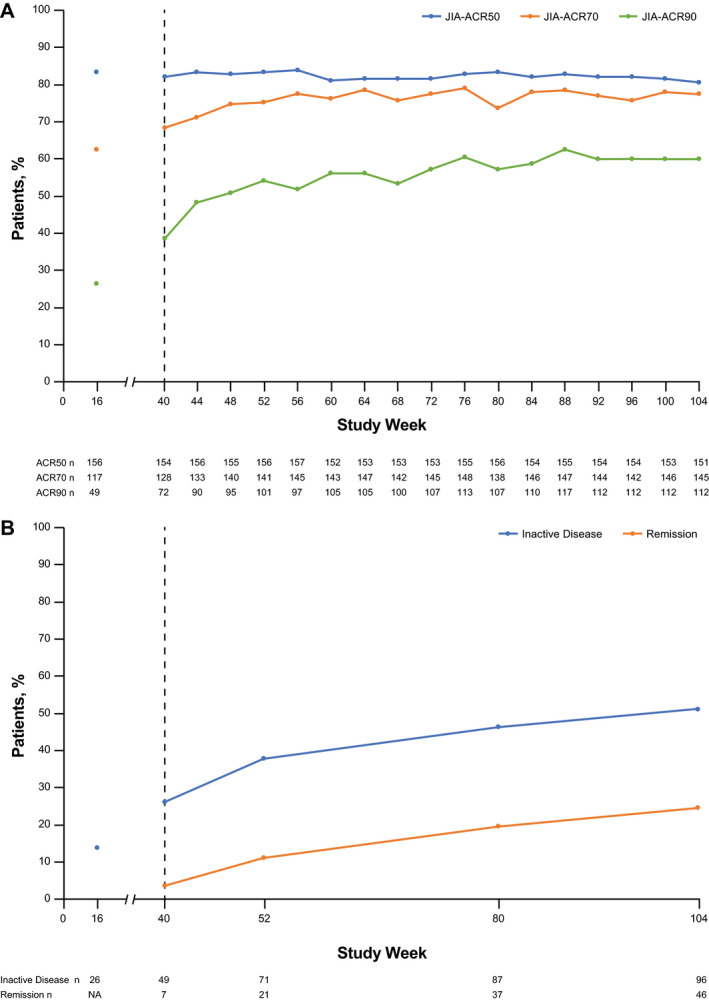
Proportions of patients in the mITT population (n = 188) achieving JIA‐ACR50/70/90 responses (A) and inactive disease and clinical remission (B) through week 104. Responders achieved JIA‐ACR50/70/90 responses or inactive disease/remission relative to baseline. After week 40, patients who were not randomly assigned in part 2 because they did not achieve at least a JIA‐ACR30 response were included and considered nonresponders. Patients who withdrew due to non–safety‐related reasons were included as nonresponders. For patients who withdrew due to safety reasons, last observation carried forward (LOCF) was used. LOCF was applied to missing ACR core components at each visit. Inactive disease was defined as the absence of active joints, no fever or physical examination features (including active uveitis) attributable to polyarticular‐course JIA, a physician global visual analog scale score of ≤10 mm, and a normal erythrocyte sedimentation rate (<20 mm/hour). Clinical remission was defined as meeting the criteria for inactive disease at all visits in the 6 months before and including the assessment day. See Figure 1 for other definitions.