
Figure 2.
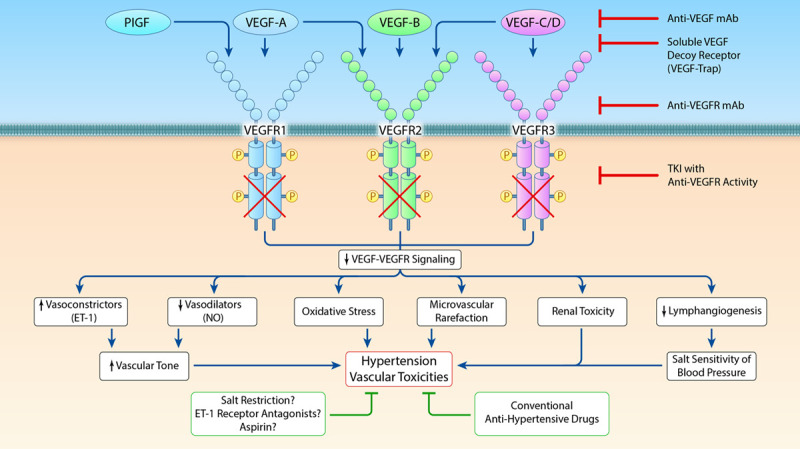
Pathophysiological mechanisms underlying VEGF (vascular endothelial growth factor) inhibitor (VEGFI)-induced hypertension and possible therapeutic interventions. Clinically, four different major classes of agents to inhibit VEGF signaling can be distinguished: (1) monoclonal antibodies directed against circulating VEGF; (2) soluble decoy receptors (VEGF-traps), scavenging freely available VEGF; (3) monoclonal antibodies against the vascular endothelial growth factor receptor (VEGFR); (4) TKI with anti-VEGFR activity that act on the intracellular tyrosine kinase domains of VEGFR to inhibit their activation. Multiple mechanisms contribute to VEGFI-induced hypertension, including an imbalance between vasoconstrictor (ET-1 [endothelin-1]) and vasodilator factors (nitric oxide [NO]), oxidative stress, microvascular rarefaction, renal injury, and decreased lymphangiogenesis. Conventional antihypertensive drugs, including calcium channel blockers and angiotensin-converting enzyme inhibitors / angiotensin II receptor blockers can be used in the treatment of VEGFI-induced hypertension. Additional potential treatment options include salt restriction, ET-1 receptor antagonists and aspirin. However, ET-1 receptor antagonists are currently not registered for the treatment of systemic hypertension. mAb indicates monoclonal antibody; PlGF, placental growth factor; and TKI, tyrosine kinase inhibitor (Illustration credit: Ben Smith).