

A primary challenge in combatting the ongoing coronavirus disease 2019 (COVID‐19) pandemic is to clarify the definitions and roles of airborne transmission, contact transmission, and droplet transmission of the causative agent, severe acute respiratory syndrome coronavirus 2 (SARS‐CoV‐2). 1 Confusion about these key aspects exists among both the general population, who are interested in evaluating their own infection risk in different settings, and scientists of different disciplines. Debate over these definitions continues, 2 with many questions, such as the following, being asked. What is the difference between airborne transmission and aerosol transmission? What is the droplet threshold size in droplet transmission? What is the difference between transmission by fomites (contaminated inanimate surfaces or objects) and transmission by contact? If fomite transmission can occur, is transmission from animate surfaces also possible?
There are various definitions for the different routes of transmission of respiratory pathogens (typically viruses), and at least three routes are currently thought to play a role, according to the World Health Organization (WHO) 3 and the US Centers for Disease Control and Prevention (US CDC). 4 Here, we adopt the following definitions from Shiu et al. 1 for discussion.
Contact transmission involves the transfer of virus‐laden respiratory secretions from an infected person to a susceptible person, either directly (via physical contact) or indirectly (via surfaces or objects).
Large‐droplet or droplet transmission involves the expulsion of virus‐laden respiratory droplets from an infected person and the subsequent deposition of these droplets on the mucosal surfaces (eg, eyes, nose, and mouth) of a susceptible person.
Airborne or aerosol transmission involves virus‐laden fine, airborne respiratory droplets being generated by the exhalation of an infected person, or by a medical aerosol‐generating procedure being performed on an infected person, and these droplets subsequently being inhaled by a susceptible person.
Among these, the definition of contact transmission appears to be the most confusing. The term “contact” refers to both direct physical contact between the infected and the susceptible persons, and indirect contact via the touching of intermediate surfaces or objects. The latter is also called the fomite route. The term “intermediate” implies that the surfaces or objects lie “between” the infected and the susceptible persons, that is, the surface or object is contaminated by the infected person, prior to the surface being touched by the susceptible person. However, a surface may also be contaminated by a healthy person's hands in a surface touch network. 5 In addition, the word “contact” can be inferred to mean physical or social contact, which may lead to confusion over the exact definitions of contact transmission. In physical terms, aerosol transmission is also a form of indirect contact via air, while large‐droplet transmission is also a form of indirect contact. The term “droplet transmission” is also confusing, as it implies that all droplets are large and will deposit on mucosal surfaces. Finally, the short‐range aerosol route is not considered, as the aerosol transmission route refers only to long‐range aerosol transmission. In fact, short‐range and long‐range aerosol transmission should not fall under the same category, as they are prevented by different measures. Thus, short‐range aerosol transmission should be considered a type of close‐contact transmission, together with large‐droplet and direct‐contact transmission.
If we consider that categorization is a way to sort different transmission events into groups based on different criteria, then those used for categorizing the three traditional categories of transmission routes appear unclear. We have attempted to use a transmission media–based approach to clarify the existing categorization of the routes of transmission of respiratory pathogens. 6 In reality, there may be multiple layers of intermediate transmission media. Expired droplets are the primary carriers of pathogens after their release from infected persons. Once expired droplets are deposited on or transferred to an inanimate surface or object (fomite), fomites are the transmission media. However, animate surfaces, such as hands and faces, can also be media in indirect transmission, and hands are essential media for fomite transmission. Droplets are transmission media in nearly all of the routes, except for the direct transfer of bodily fluids containing pathogens, for example, via kissing. Air itself cannot transmit pathogens if air does not flow or is not inhaled. Thus, if the transmission media–based criterion is used, aerosol transmission appears to be a better definition than airborne transmission.
It is useful to briefly consider the history of the concept of pathogen transmission, as the concepts we use today are based on those established at the dawn of modern science, and it is to be expected that these concepts will evolve with our understanding of the underlying science. Girolamo Fracastoro (1476–1553) “defined a contagion as a precisely similar corruption, developing in the substance of a combination of elements, which passed from one thing to another and was the result of an infection first occurring in the imperceptible particles. There were three different types of contagion, by direct contact, by contact leaving behind ‘fomites’ that preserved the seeds of contagion and [were] infected by them; and at a distance as if by some impetus or poison. In all three, infection was produced not by an unknown ‘occult’ cause, but by seeds (semina, seminaria) of contagion, which varied with the type.” 7 Fracastoro also speculated upon the concept of airborne seeds (or “seedlets” of contagion). However, the erroneous “miasma” theory of pathogen transmission continued to dominate, and Fracastoro's “seed of disease” contagion theory was not accepted until the development of germ theory by Louis Pasteur (1822–1895) and Robert Koch (1843–1910). Pasteur also discovered that microbes were present in air. 8
Carl Flügge (1847–1923) and others first conceptualized the large‐droplet transmission route 9 and observed that the organisms in the expired droplets could not be recovered by sampling plates exposed at distances beyond 1–2 m from the infectious person. Charles Chapin (1856–1941) 9 established that contact transmission is the dominant route of transmission of infection pathogens. He wrote that “Infection by air, if it does take place, as is commonly believed, is so difficult to avoid or guard against, and so universal in its action, that it discourages effort to avoid other sources of danger. If the sick‐room is filled with floating contagium, of what use is it to make much of an effort to guard against contact infection? If it should prove, as I firmly believe, that contact infection is the chief way in which the contagious diseases spread, an exaggerated idea of the importance of airborne infection is most mischievous.” William Wells developed the concept of droplet nuclei and a relatively modern theory of airborne transmission. 10 However, it is often overlooked that he also calculated and suggested that the droplet threshold size was “a tenth of a millimeter” (ie, 100 µm). 10
As reviewed in, 6 Garner 11 was probably the first to suggest the involvement of droplets larger than 5 µm in large‐droplet transmission and to pioneer the concept of transmission‐based precautions against droplet, contact, and inhalation transmission. The 2014 WHO guidelines 3 define droplets as “respiratory aerosols >5 µm in diameter.” However, the threshold diameter is much larger (50–100 µm), as can be shown by calculating the probability of deposition of an expired droplet. 6 , 12 A drop falls (drops) due to its own weight, while a droplet is a very small drop that does not fall easily. The ability for a droplet to become suspended in air also depends on surrounding airflows, with larger droplets being suspended by stronger airflows. This may have a large effect on airborne transmission, given the difference is size between droplets in a jet expired during normal exhalation, at a typical speed of 2 m/s, with those released in a cough, at a typical speed of 20 m/s, into a typical room airflow speed of <0.25 m/s. Thus, it may be better to simply refer to drops rather than large droplets and to use aerosols to refer to droplets that are small enough to remain suspended in air for a certain period of time. It is notable that aerosols in room air are mostly 5 µm or less in diameter, while those in expired jets are much larger (≤50 µm in diameter 12 ).
As a side note, both the WHO and the US CDC consider that precautions against the transmission of respiratory pathogens include those that guard against contact, droplet, and airborne transmission and that these should be implemented in addition to standard precautions. 3 , 4 It is typically stated that it is more important to implement several of these precautions rather than an individual precaution, which attests to the likelihood that multiple routes of transmission can operate, that there is uncertainty over which transmission routes are most prominent, and that there is some ambiguity in the definitions of the routes of transmission. It would therefore be helpful if the routes of transmission could be defined more explicitly, such that more exact precautions could be taken.
The classical categorization as described above is conceptually useful, but it is based on imagination and reasoning, rather than a systematic consideration of the categorization criteria. The new knowledge that has been gained on the generation, release, transport, and routes of exposure to respiratory droplets enables the revision of this categorization. A good categorization of transmission routes should be free of ambiguity or inconsistencies, such that public health experts can develop consistent precaution and prevention policies, and that researchers of multiple disciplines can easily apply and integrate their knowledge into the study of transmission mechanisms and interventions. Transmission route categorizations should also be updated in response to the latest mechanistic understandings on transmission mechanisms, rather than attempting to fit this new knowledge into the existing definitions, as was done during the development of the short‐range aerosol transmission route and the surface touch network transmission routes.
The existing concepts of aerosol, fomite, and large‐droplet transmission are based on where pathogenic particles are positioned (ie, in the air, on fomites, or in/or droplets), not how they are transferred (transmitted). Both large‐droplet transmission and close‐contact transmission were proposed before the theory of air jets was developed, and the latter has now been widely used to understand the airflows expired during respiratory activities, such as coughing and normal breathing. Furthermore, the concept of airborne transmission of droplet nuclei 10 was developed well before it was possible to distinguish air‐distribution patterns in buildings.
Below, we suggest a set of transfer process–focused criteria for categorizing the basic routes of transmission of respiratory viruses. The media involved are shown in brackets, and we adopt a “media + transfer” structure in this new categorization.
(Drop) spray transmission refers to respiratory viruses that are transmitted by the spray of virus‐laden drops expelled from an infected person being deposited on the mucosal surfaces (eg, eyes, nose, and mouth) of a susceptible person. Thus, only drops that move can transmit a virus by this process, where this movement is due to the momentum gained at the point of release, for example, at the mouth. Due to the nature of expired airflows, such drop spray transmission will only be possible within a certain proximity. Chapin 9 wrote that “most diseases are not likely to be dust‐borne, and they are spray‐borne only for two or three feet, a phenomenon which, after all, resembles contact infection more than it does aerial infection as ordinarily understood.” Drop spray transmission is identical to traditional large‐droplet transmission, but avoids the use of the ambiguous “droplets” term, and the word “spray” enhances understanding: It is easy to visualize a face shield being used to block a spray, or a face mask being used to block drops.
(Aerosol) inhalation transmission refers to air‐suspended virus‐laden respiratory droplets being exhaled by an infected person and inhaled by a susceptible person. Aerosol inhalation can occur over the short range and long range. The risk of transmission by aerosol inhalation is greater when a susceptible person is in close proximity to an infected person, that is, within 1–2 m. Flowing air can transport respiratory aerosols around, but unmoving air cannot. However, a person may inhale virus‐containing aerosols from a room containing unmoving air, as inhalation is itself an airflow process.
(Surface) touch transmission refers to animate (eg, skin) or inanimate (fomite) surface‐dwelling virus‐laden respiratory drops or droplets being transferred by a person hand touching such a surface and subsequently touching his/her mucosa, resulting in self‐inoculation.
These three newly defined routes may be considered as the three basic viral transmission routes. Obviously, the fourth transmission route is the direct transfer of bodily fluids containing pathogens (eg, kissing). While spray transmission can only occur during close contact, both inhalation and touch transmission can occur over a long distance. These three basic transmission processes also satisfy one of the basic principles of categorization, that is, cognitive economy, which means “to provide the maximum information with the least cognitive effort.” 13 These processes may be adaptable to categorize transmission of aerosols generated by other mechanisms (eg, medical aerosols or fecal aerosols), if they are shown to play a role in the transmission of a specific pathogen.
It may be possible to further classify the transmission routes according to common relations or attributes, such as infection settings, distances between the infected and the susceptible persons, transmission media, or the origin of virus‐laden droplets or aerosols.
With respect to distance, there are two types of transmission: close‐contact transmission (proximity or short distance, ie, within 1–2 m from the infected person) and distant transmission (long distance, ie, >1–2 m from the infected person) (Figure 1). Crucially, our definitions clarify that all three basic routes of virus transmission, that is, spray, inhalation, and touch transmission, can be involved in close‐contact transmission. Proximity inhalation transmission has been referred to as “short‐range aerosol transmission” in the literature, while proximity touch transmission has been denoted as the “immediate surface” route. 6 However, with respect to close‐contact transmission, the US CDC and WHO transmission‐based precaution approach 3 , 4 does not consider the proximity inhalation route, despite this being likely to occur and possible dominates. Inhalation and touch‐based transmission are both possible forms of distant transmission. Finally, aerosols involved in proximity inhalation are larger than those involved in distant inhalation.
FIGURE 1.
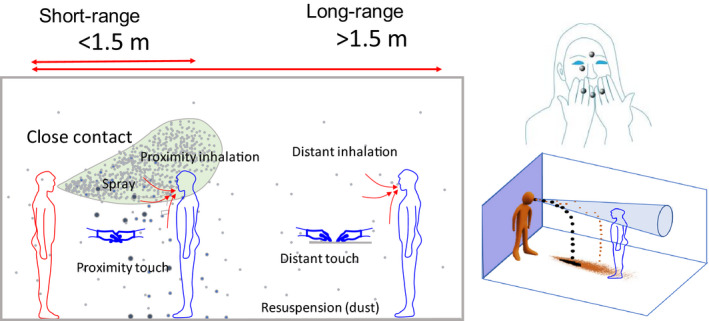
An illustration of the three basic short‐distance transmission routes—spray, inhalation, and touch—and long‐distance transmission (inhalation and touch) in a room. The expired jet range is shown in light green, the infected person is shown in red, and the susceptible person is shown in blue (modified from 14 ). The drops are shown as large black circles, and the aerosols, as small black circles
Peer Review
The peer review history for this article is available at https://publons.com/publon/10.1111/ina.12786.
ACKNOWLEDGEMENTS
The author is grateful to Dr Donald Milton for discussions, especially for his suggestion to use the aerosol inhalation definition suggested by Dr Lindsey Marr. This work was been supported by The Hong Kong RGC GRF project (No. 17202719).
REFERENCES
- 1. Shiu EY, Leung NH, Cowling BJ. Controversy around airborne versus droplet transmission of respiratory viruses: implication for infection prevention. Curr Opin Infect Dis. 2019;32(4):372‐379. [DOI] [PubMed] [Google Scholar]
- 2. Tellier R, Li Y, Cowling BJ, Tang JW. Recognition of aerosol transmission of infectious agents: a commentary. BMC Infect Dis. 2019;19(1):101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. World Health Organization . Infection prevention and control of epidemic‐ and pandemic prone acute respiratory infections in healthcare – WHO guidelines. 2014. http://www.who.int/csr/bioriskreduction/infection_control/publication/en/. (Accessed 14 October 2020). [PubMed]
- 4. Siegel JD, Rhinehart E, Jackson M, et al. Guideline for isolation precautions: preventing transmission of infectious agents in healthcare settings. Centers for Disease Control and Prevention. 2007. https://www.cdc.gov/infectioncontrol/guidelines/isolation/index.htm. (Accessed 14 October 2020). [DOI] [PMC free article] [PubMed]
- 5. Lei H, Li Y, Xiao S, et al. Logistic growth of a surface contamination network and its role in disease spread. Sci Rep. 2017;7:14826. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Zhang N, Chen W, Chan PTJ, et al. Close contact behaviour in indoor environment and transmission of respiratory infection. Indoor Air. 2020;30(4):645‐661. 10.1111/ina.12673 [DOI] [PubMed] [Google Scholar]
- 7. Nutton V. The seeds of disease: an explanation of contagion and infection from the Greeks to the Renaissance. Med Hist. 1983;27(1):1‐34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Ariatti A, Comtois P. Louis Pasteur: the first experimental aerobiologist. Aerobiologia. 1993;9(1):5‐14. [Google Scholar]
- 9. Chapin CV. The Sources and Modes of Infection. New York, NY: John Wiley and Sons; 1912. [Google Scholar]
- 10. Wells WF. On air‐borne infection study: II – droplets and droplet nuclei. Am J Epidemiol. 1934;20:611‐618. [Google Scholar]
- 11. Garner JS. Hospital infection control practices advisory committee. Guideline for isolation precautions in hospitals. Infect Control Hosp Epidemiol. 1996;17:54‐80. [DOI] [PubMed] [Google Scholar]
- 12. Chen W, Zhang N, Wei J, et al. Short‐range airborne route dominates exposure of respiratory infection during close contact. Build Environ. 2020;176:106859. [Google Scholar]
- 13. Rosch E. Principles of categorization. In: Levitin DJ, ed. Foundations of Cognitive Psychology: Core Readings. Cambridge, MA: MIT Press; 2002:251‐270. [Google Scholar]
- 14. Wei J, Li Y. Airborne spread of infectious agents in the indoor environment. Am J Infect Control. 2016;44(9 Suppl):102‐108. [DOI] [PMC free article] [PubMed] [Google Scholar]