

Abstract
Objective
Obesity and chronic pain often co‐occur and exert bidirectional influences on one another. How patients with obesity and chronic pain respond to weight loss treatments, however, remains unclear. This study evaluated body weight, physical activity, and diet outcomes in participants with and without chronic pain in a 2‐year behavioral weight loss trial.
Methods
An analytical cohort of 397 adults was assembled from a Midwestern healthcare system that participated in the larger trial. Participants with chronic pain 1 year prior to, or during, the trial were identified using a validated medical records algorithm. Mixed models were used to estimate changes in outcomes over 24 months.
Results
One‐third of participants (n = 130) had chronic pain. After adjustment for age, sex, body mass index, and trial arm, weight loss was similar in both groups at 6‐months (−7.0 ± 0.8 kg with chronic pain vs. −7.7 ± 0.6 kg without). Participants with chronic pain had significantly less weight loss at 24‐months relative to those without (−3.6 ± 0.5 vs. −5.2 ± 0.4 kg; p = 0.007). Physical activity, screen time, dietary fat, fruit/vegetable consumption, and sugar‐sweetened beverage intake improved similarly in both groups over time.
Conclusions
Participants with chronic pain lost ∼33% less weight over 2 years, which was driven by greater weight regain after the first 6 months. Future research should test tailored weight loss maintenance strategies for individuals with chronic pain.
Keywords: dietary assessment, physical activity, weight loss
1. INTRODUCTION
Chronic pain affects over 116 million people, with costs exceeding over $635 billion dollars annually in the United States. 1 Obesity and chronic pain often occur together. Relative to those at a healthy weight, prevalence rates for self‐reported daily pain are 68%, 136%, and 254% higher for individuals with class I, class II, and class III obesity, respectively. 2
Chronic pain and obesity appear to have bidirectional physiological and behavioral influences on one another. Those with chronic pain tend to release greater amounts of proinflammatory mediators.3, 4 Most notably, interleukin‐6 and C‐reactive protein accumulate, while macrophages also build up in adipose tissue, leading to chronic inflammation. 5 Adults with chronic pain may also display eating patterns that lead to excess caloric intake over time. For example, leptin levels, which signal satiety, have been shown to be particularly elevated in patients with obesity and osteoarthritis.5, 6, 7 As might be expected, those with chronic pain tend to have consistently lower levels of physical activity due to disability and low mood, among other factors.8, 9, 10, 11
How patients with obesity and chronic pain respond to weight loss treatments remains unclear. Short‐term observational studies suggest that patients with chronic pain do tend to lose weight in a lifestyle modification intervention, and those that lose more weight sometimes have greater pain reduction (along with improved leptin and other markers of metabolic function).12, 13, 14 This association is more pronounced in bariatric surgery, as most patients with chronic pain before surgery experience significant improvement in pain symptoms after surgery, which also leads to a more active lifestyle and greater quality of life. 15 An inverse association has been observed between pain severity and weight loss in some programs. 16 Evidence from more rigorous studies, however, is mixed. A 6‐month lifestyle modification intervention in patients who were overweight and had low back pain did not result in significant weight loss or pain control compared to those in a usual care condition. 17 Only two studies compared those with versus without chronic pain within a cohort of weight loss trial participants. Masheb, et al. found that, over 12 months, participants with self‐reported severe pain at baseline lost nearly 2 kg less than those with either moderate or no pain. 18 Another lifestyle modification intervention study, conducted in the United Kingdom's national weight management program, found patients with obesity and severe pain lost 5.1 kg less weight over 1 year relative to those with mild or no pain. 19
The purpose of this study was to compare the effectiveness of a lifestyle modification intervention in trial participants with versus without chronic pain. Body weight, physical activity, and diet outcomes were assessed over a 24‐month timeframe. Our hypothesis was that individuals with chronic pain would lose less weight and have less favorable lifestyle improvements over 24 months relative to those without chronic pain.
2. METHODS
2.1. Design and intervention
This was a retrospective cohort analysis using data from a recently completed cluster‐randomized behavioral weight loss trial. Methods of the broader trial are described in detail elsewhere. 20 Briefly, 36 practices in the Midwestern US each enrolled approximately 40 participants. Each practice (cluster) was randomly assigned to one of three study arms, all of which included an intensive lifestyle modification intervention that differed by delivery mode, including fee‐for‐service (FFS), patient centered medical home (PCMH), and disease management (DM). Counseling sessions were delivered over 24 months and followed a similar schedule in all arms, which was approximately weekly for the first three months, bi‐weekly through Month 6, and monthly thereafter. The FFS arm met individually, in‐person for 15 min sessions, while the PCMH arm met in an in‐person group format, and the DM arm met in a telephone‐based group format for 60 min sessions. As part of each lifestyle modification intervention arm, participants were encouraged to set reasonable weight loss goals (∼10%) and consume a low‐calorie diet that included a personal calorie goal, emphasis on portion control, and regular consumption of high fiber foods such as fruit and vegetables. 20 With the exception of the DM arm, where weight management counseling was delivered by a centralized call center, all lifestyle modification intervention activities were conducted by local clinic staff. Analyses in this paper were limited to a cohort of study participants from 10 practices from the Marshfield Clinic Health System (MCHS) in Wisconsin who participated in the trial. These MCHS practices were selected for this cohort analysis because only MCHS data systems had reasonably complete capture of primary medical care, which was needed to identify participants with and without chronic pain (as defined below).
2.2. Participants
All participants included in this analysis were patients who were medically homed to one of 10 MCHS clinics. There were 403 participants (from across the 10 MCHS clinics) who enrolled in the broader trial, and analytical data were available on 397 of them. The six participants removed from the study were excluded from this analysis (pregnancy [n = 1], major medical contraindications [n = 3], death [n = 2]). Study‐eligible patients needed to be age 20–75 years, have a body mass index (BMI) between 30 and 45 kg/m2, live in a rural ZIP code, 21 have access to a telephone, and read/speak English. All enrollees had medical clearance from their primary care provider to participate in the lifestyle modification intervention trial. 20 Patients were excluded if they had a recent history of myocardial infarction, stroke, or cancer, any history or planned bariatric surgery, were pregnant, lactating or were planning a pregnancy within 2 years. Studies procedures were approved by the Kansas University Medical Center Institutional Review Board, and all participants signed informed consent forms.
2.3. Chronic pain
The primary exposure was chronic pain. Participants were dichotomized as having or not having chronic pain during the weight loss trial. Chronic pain status was established using a modified version of a previously validated electronic health records (EHR) algorithm developed by Tian and colleagues. 22 Specifically, participants with chronic pain had at least one stand‐alone chronic pain diagnostic code or at least two acute pain diagnoses, separated by at least 30 days (and made by a physician or mid‐level provider), and with occurrences between 1 year prior to the participant's enrollment date and 24 months after their enrollment date (specific International Classification of Disease codes from ninth and 10th versions available upon request). In addition to these pain diagnostic codes, the original study by Tian and colleagues electronically screened for high patient self‐ratings of pain or at least 90 days of an active opioid prescription. 22 Such pain self‐ratings are not systematically collected or query‐able within the MCHS EHR system and only one included study participant had a documented long‐term opioid prescription during the study timeframe. However, the diagnostic codes used alone in the Tian, et al. study accurately identified 93% of manually validated chronic pain patients. We conducted an internal validation of the diagnostic code‐based algorithm used in our study. Two investigators (Cody L. Goessl and Jeffrey J. VanWormer) manually validated 22 participants who were algorithmically identified as having chronic pain, as well as 22 additional participants who were identified as not having chronic pain, per sample size guidelines for reliability assessments. 23 A chart review of all medical encounters during the study timeframe was performed for each audited participant, independently by each reviewer. Reliability of manual determinations was 98% between the two raters, and the percent agreement with manually determined status was 95% for those algorithmically identified with chronic pain and 86% for those identified without chronic pain. In the chronic pain group, chart notes indicated the vast majority of participants had rather traditional forms of chronic pain affecting either their limbs, joints, back, or combination thereof. The one discordant rating in the chronic pain group was due to a patient with a chronic pain diagnosis for flank discomfort (which resolved) secondary to endometriosis. The three discordant ratings in the no chronic pain group were due to two patients with chronic foot pain and one patient with recent onset low back pain that did not receive pain diagnoses.
2.4. Outcomes
Anthropometric. Height and weight were measured at baseline and used to calculate BMI (kg/m2). Body weight was measured in‐person again at the 6‐, 18‐, and 24‐month follow‐ups. Weight was measured using a standardized protocol that included participants wearing light clothing and in a fasting state, and using a calibrated digital scale (Befour MX‐115, Inc.). Height was measured with a stadiometer.
Physical activity. Participants reported their level of daily physical activity using the validated Past Week Modifiable Activity Questionnaire (PWMAQ). 24 The PWMAQ evaluates moderate to vigorous physical activities (MVPA) based on a self‐reported list of 38 common activities, and their frequencies and durations, over the course of 1 week. Time active is then multiplied by the Compendium of Physical Activities (2011) recommended metabolic equivalent time (MET) values to create a summary estimate of MET hours per week.23, 24 Screen time was evaluated with a single item assessing hours per day spent on a computer or watching television. These questions were administered at baseline, 6, 12, and 24 months.
Diet. Dietary outcomes included the percent energy from fat, fruit/vegetable servings per day, and sugar‐sweetened beverages per day. These measures were captured in three validated instruments, including 25 : National Cancer Institute's Quick Food Scan, 26 US Centers for Disease Control and Prevention's Behavioral Risk Factor Surveillance System—Sugar Sweetened Beverage Intake Questionnaire, and 1 National Cancer Institute's two‐item Fruit and Vegetable Screener.27, 28, 29, 30 All dietary instruments were administered at baseline, 6, 12, and 24 months.
2.5. Analyses
Baseline characteristics were compared between the chronic pain and no chronic pain exposure groups using t‐tests and chi‐square tests. Body weight, physical activity, and diet outcomes were estimated at each follow‐up time and compared between groups using general linear mixed models, controlling for age, gender, baseline BMI, study arm. For the physical activity and diet outcomes, further adjustments were made for the baseline quintiles of MET hours per week, screen time, percent energy from fat, fruit and vegetable consumption, and sugar‐sweetened beverage intake. An intent‐to‐treat framework was used whereby all participants with available data were included, with no imputation for missing follow‐up values (maximum likelihood). Changes from baseline in body weight, physical activity, and diet measures were estimated from the full model using differences in least square means, and were compared between the two groups using Estimate statements (SAS Institute, Inc., Cary, North Carolina).
3. RESULTS
Among the 397 participants included in this analysis, 130 (33%) were identified as having chronic pain. The most common pain diagnoses (not mutually exclusive) were for “Other chronic pain” (338.29, G89.29—72%), “Pain in limb” (729.5, M79.6xx—26%), and “Joint pain in lower leg/knee” (719.46, M25.56x, M45.x—25%). As outlined in Table 1, the sample was typical for weight loss trials in that 72% were female and the average age was 58 years. Baseline BMI was (mean ± SD) 36.5 ± 4.1 kg/m2. The two groups were fairly balanced at baseline, but those with chronic pain were more likely to have public‐assisted healthcare coverage.
TABLE 1.
Descriptive characteristics of RE‐POWER participants
| Chronic pain | No chronic pain | ||
|---|---|---|---|
| (n = 130) | (n = 267) | P | |
| Gender | |||
| Male | 41 (32) | 70 (26) | 0.29 |
| Female | 89 (69) | 197 (74) | |
| Age (y) | 57.9 (11.0) | 57.3 (11.1) | 0.62 |
| Body mass index (kg/m2) | 37.0 (3.9) | 36.4 (4.3) | 0.10 |
| Years living in rural setting | 30.2 (19.1) | 30.3 (18.8) | 0.94 |
| Race | |||
| White | 128 (98) | 262 (98) | 0.69 |
| Not White | 2 (2) | 4(2) | |
| Marital status | |||
| Married | 92 (71) | 216 (81) | 0.19 |
| Not married | 38 (29) | 50 (19) | |
| Healthcare coverage | |||
| Medicare | 53 (41) | 78 (29) | 0.02 |
| Medicaid | 20 (15) | 15 (6) | 0.00 |
| Military | 2 (1) | 12 (3) | 0.13 |
| Private insurance | 68 (17) | 170 (43) | 0.04 |
| No insurance | 0 (0) | 4 (1) | 0.16 |
Note: Values are reported as mean (±SD) or frequency count (%).
3.1. Weight loss
After adjustment for age, sex, trial arm, and baseline BMI, there was a significant group by time interaction at the 24‐month follow‐up. As shown in Figure 1, mean (±SE) weight loss at 6‐months was similar for participants with (−7.0 ± 0.9 kg) or without (−7.7 kg ± 0.6 kg) chronic pain. Thereafter, the rate of weight regain became steadily greater in the chronic pain group. At the 24‐month follow‐up, participants with chronic pain had lost 3.6 ± 0.5 kg since baseline, whereas those without chronic pain lost 5.2 ± 0.3 kg (weight change differential = 1.6 ± 0.6 kg, p = 0.007).
FIGURE 1.
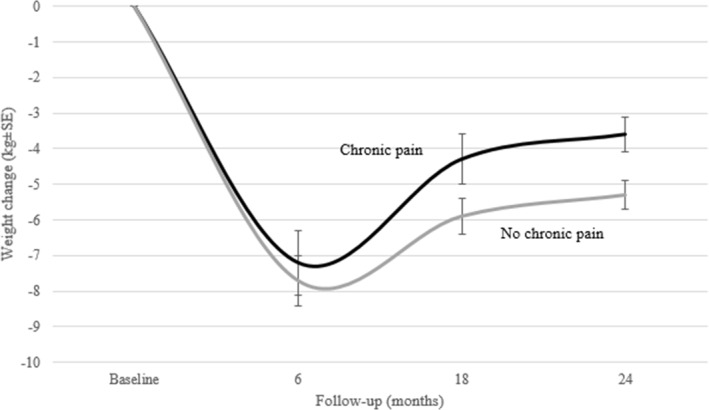
Weight changes by chronic pain status
3.2. Physical activity and diet
There were no significant group by time interactions for any physical activity or diet outcomes. Relative to baseline, there were significant improvements in all physical activity and diet outcomes at each follow‐up time (particularly for MVPA), but the magnitude of these lifestyle improvements were statistically indistinguishable between participants with or without chronic pain (Table 2).
TABLE 2.
Changes in lifestyle outcomes by chronic pain status
| Chronic pain | No chronic pain | ||
|---|---|---|---|
| (n = 130) | (n = 267) | p | |
| Moderate and vigorous physical activities (metabolic equivalent time hours per week) | |||
| Baseline | 7.3 (1.2) | 7.7 (0.9) | 0.79 |
| Change at 6 months | +7.0 (1.7) | +10.3 (1.2) | 0.12 |
| Change at 12 months | +5.2 (1.7) | +6.3 (1.2) | 0.61 |
| Change at 24 months | +4.2 (1.5) | +5.8 (1.0) | 0.38 |
| Screen time (hours per day) | |||
| Baseline | 3.7 (0.2) | 3.6 (0.1) | 0.46 |
| Change at 6 months | −0.5 (0.2) | −0.4 (0.1) | 0.74 |
| Change at 12 months | −0.6 (0.2) | −0.6 (0.1) | 0.80 |
| Change at 24 months | −0.4 (0.2) | −0.5 (0.1) | 0.59 |
| Energy from dietary fat (%) | |||
| Baseline | 32.9 (0.3) | 33.2 (0.2) | 0.34 |
| Change at 6 months | −1.6 (0.4) | −2.0 (0.3) | 0.40 |
| Change at 12 months | −1.7 (0.4) | −1.9 (0.3) | 0.70 |
| Change at 24 months | −1.3 (0.4) | −1.5 (0.2) | 0.64 |
| Fruits and vegetables (servings per day) | |||
| Baseline | 2.0 (0.1) | 2.2 (0.1) | 0.36 |
| Change at 6 months | +1.5 (0.2) | +1.6 (0.1) | 0.46 |
| Change at 12 months | +1.3 (0.2) | +1.2 (0.1) | 0.68 |
| Change at 24 months | +0.8 (0.1) | +0.9 (0.1) | 0.71 |
| Sugar‐sweetened beverages (beverages per day) | |||
| Baseline | 0.5 (0.1) | 0.5 (0.0) | 0.59 |
| Change at 6 months | −0.3 (0.1) | −0.3 (0.1) | 0.85 |
| Change at 12 months | −0.3 (0.1) | −0.3 (0.1) | 0.89 |
| Change at 24 months | −0.2 (0.1) | −0.2 (0.0) | 0.43 |
Notes: Values are reported as mean (±SE).
4. DISCUSSION
This is one of the few studies to directly compare weight loss outcomes in adults with obesity and with versus without chronic pain. Clinician evaluated chronic pain was fairly common in this obesity‐treatment seeking sample, and participants with chronic pain initially lost about the same amount of weight over 6 months as those without. After that point, however, participants with chronic pain regained more weight and, by the 24‐month follow‐up, had a net weight loss that was about 33% less than their counterparts without chronic pain. Weight regain is predictable in most all lifestyle modification interventions, 31 and our findings were consistent with prior studies by Masheb, et al., as well as Ryan and colleagues and Wachholtz, et al., in that participants with chronic pain lost less weight than those without.16, 18, 19 These prior studies did not have long‐term follow‐up though, and usually reported weight only at the beginning and end of follow‐up, thus our study may be the first to show that the main difference in adults with obesity and chronic pain is that they tend to regain weight faster after their initial (6‐month) weight loss. Though not assessed in this analysis, such outcomes may negatively impact quality of life for patients with obesity and chronic pain as they near completion of a weight loss intervention.
Reasons for the greater weight regain observed in our sample of participants with chronic pain are unclear. It did not seem to be driven by any obviously greater erosion of behaviors supportive of weight loss maintenance, as those with or without chronic pain had a relatively similar profile of change in dietary and physical activity measures. Our sample was underpowered, however, to examine whether associations between lifestyle changes and weight change differed in adults with versus without chronic pain, a potentially important area of future research. This lack of a clear adherence differentiation between the two groups, which was consistent with findings on dietary intake by Masheb and colleagues, could partially be explained by the known imprecision of self‐reported lifestyle metrics.18, 32, 33, 34 It may also indicate that there are at least some physiological barriers to weight loss that persist in patients with chronic pain. In our study, individuals with chronic pain had all received recent medical recognition of their pain, which may be an indicator of more severe underlying injuries or conditions that can foster chronic inflammatory states, insulin resistance, and metabolic or hypothalamus‐pituitary axis dysfunction that impedes weight loss.12, 35, 36 Future research should examine how such biological factors contribute to weight regain in patients with obesity and chronic pain. In addition, exploring how chronic pain may interact with severe mental health conditions (e.g., depression, post‐traumatic stress disorder) may be an important area to understand potential mediating roles between mental health, lifestyle changes, and weight loss in patients with chronic pain.
Future lifestyle modification interventions should also consider integrating pain management directly alongside weight management. Like our trial, prior lifestyle modification intervention studies in this area were designed to target weight loss, and weight loss and associated increases in activity could also have pain reduction benefits.12, 13, 14, 15, 16, 17, 18, 19 Only one lifestyle modification intervention tested healthy lifestyle coaching combined with an educational curriculum aimed to reduce fears about pain and minimize lifestyle risks that drive pain intensity, but reported null findings compared to a control group. 15 However, integrating such pain‐specific cognitive retraining procedures alongside more intense strategies for weight loss maintenance, such as increased physical activity, daily self‐weighing, and dietary restraint, 37 may help those with obesity and chronic pain be more successful over the long‐term. This could also include adaptive strategies, similar to daily self‐weighing, that evaluate pain levels more frequently, with alerts provided to clinicians regarding the need for further pain control. Other weight management components that could be integrated into programs for patients with obesity and chronic pain may include more specific health education techniques like teach‐to‐goal methods that reinforce program objectives and strategies, pain coping skills techniques, along with combined behavioral and pharmaceutical therapies, which have demonstrated some benefits in prior lifestyle modification interventional studies.13, 37, 38, 39, 40, 41, 42, 43
Strengths of this study included the 24 months of available follow‐up and objective assessment of chronic pain using a validated EHR method. Limitations included the cohort (vs. random) design of the analysis, which could increase the risk of confounding by unmeasured exposures. Also, the identification of chronic pain status via recent clinician evaluation could increase the risk of exposure misclassification because it does not delineate those with moderate pain symptoms that do not require medical attention, nor does it provide an appraisal of pain duration or impacts on function. Furthermore, we dichotomized participants with any versus no chronic pain diagnoses, which could increase the risk of residual confounding as it does not permit examination of how specific chronic pain types (e.g., central, joints, and back) may differentially influence weight loss. More detailed sub‐classification of pain, along with multivariable analyses to identify underlying pain mechanisms for outcome responses, would be more optimal, but would likely require a much larger sample size and detailed chart review/adjudication of complex pain patients. Our sample was also limited to rural MCHS patients only, whom we had reasonably complete capture of prior medical history on, but this limits generalizability across all chronic pain patients in other parts of the United States and in urban areas. Finally, lifestyle habits were self‐reported using validated surveys, but are subject to recall and self‐presentation biases.
5. CONCLUSION
Chronic pain is a common comorbidity in patients with obesity. 2 Our findings support previous research suggesting that chronic pain inhibits weight loss in behavioral weight management program, and this seems to be driven by greater weight regain following the initial 6‐month weight loss. Researchers and clinicians should seek to identify more comprehensive, team‐based approaches that simultaneously address weight and pain management, especially after the initial weight loss phase of a lifestyle modification intervention.
CONFLICT OF INTEREST
The authors declared no conflict of interest.
AUTHOR'S CONTRIBUTIONS
All authors equally contributed to the development, revisions and approval of this manuscript. Jeffrey J. VanWormer and Cody L. Goessl internally validated the pain algorithm against participant's medical records and conducted all statistical analyses, as well.
ACKNOWLEDGEMENTS
The study team would like to thank the staffs of Marshfield Clinic Research Institute, Center for Clinical Epidemiology and Population Health and University of Kansas Medical Center, Department of Population Health, for their diligent work on this trial and cohort study. All individual data, other documents, data or analyses will be not be available to anyone beyond the study team. This trial was funded by Patient‐Centered Outcomes Research Institute. Clinical trial registration: Clinicaltrials.gov identifier NCT02456636.
REFERENCES
- 1. Institute of Medicine (US) Committee on Advancing Pain Research, Care, and Education . Relieving Pain in America: A Blueprint for Transforming Prevention, Care, Education, and Research. Washington, DC: National Academies Press (US); 2011. [PubMed] [Google Scholar]
- 2. Stone AA, Broderick JE. Obesity and pain are associated in the United States. Obesity. 2012;20:1491‐1495. [DOI] [PubMed] [Google Scholar]
- 3. Omoigui S. The biochemical origin of pain–proposing a new law of pain: the origin of all pain is inflammation and the inflammatory response. Part 1 of 3–A unifying law of pain. Med Hypotheses. 2007;69:70‐82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Omoigui S. The biochemical origin of pain: the origin of all pain is inflammation and the inflammatory response. Part 2 of 3–inflammatory profile of pain syndromes. Med Hypotheses. 2007;69:1169‐1178. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Okifuji A, Hare BD. The association between chronic pain and obesity. J Pain Res. 2015;8:399. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Considine RV. Human leptin: an adipocyte hormone with weight‐regulatory and endocrine functions. Semin Vasc Med. 2005;5:15‐24. [DOI] [PubMed] [Google Scholar]
- 7. Lübbeke A, Finckh A, Puskas GJ, et al. Do synovial leptin levels correlate with pain in end stage arthritis? Int J Orthop. 2013;37:2071‐2079. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Amy EA, Kozak AT. “The more pain I have, the more I want to eat”: obesity in the context of chronic pain. Obesity. 2012;20:2027‐2034. [DOI] [PubMed] [Google Scholar]
- 9. Lake JK, Power C, Cole TJ. Back pain and obesity in the 1958 British birth cohort: cause or effect? J Clin Epidemiol. 2000;53:245‐250. [DOI] [PubMed] [Google Scholar]
- 10. Marcus DA. Obesity and the impact of chronic pain. Clin J Pain. 2004;20:186‐191. [DOI] [PubMed] [Google Scholar]
- 11. Chin S‐H, Huang W‐L, Akter S, Binks M. Obesity and pain: a systematic review. Int J Obes. 2020;44:969‐979. [DOI] [PubMed] [Google Scholar]
- 12. Doury‐Panchout F, Metivier J‐C, Nardoux J, Fouquet B. Visceral obesity and chronic pain: effect of a 4‐week rehabilitation program on adipokines and insulin resistance. J Exerc Rehabil. 2017;13:464‐471. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Schrepf A, Harte SE, Miller N, et al. Improvement in the spatial distribution of pain, somatic symptoms, and depression after a weight loss intervention. J Pain. 2017;18:1542‐1550. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Cooper L, Ryan C, Ells LJ, et al. Weight loss interventions for adults with overweight/obesity and chronic musculoskeletal pain: a mixed methods systematic review. Obes Rev. 2018;19:989‐1007. [DOI] [PubMed] [Google Scholar]
- 15. Speck RM, Bond DS, Sarwer DB, Farrar JT. A systematic review of musculoskeletal pain among bariatric surgery patients: implications for physical activity and exercise. Surg Obes Relat Dis. 2014;10:161‐170. [DOI] [PubMed] [Google Scholar]
- 16. Wachholtz A, Binks M, Eisenson H, Kolotkin R, Suzuki A. Does pain predict interference with daily functioning and weight loss in an obese residential treatment‐seeking population? Int J Behav Med. 2010;17:118‐124. [DOI] [PubMed] [Google Scholar]
- 17. Williams A, Wiggers J, O'Brien KM, et al. Effectiveness of a healthy lifestyle lifestyle modification intervention for chronic low back pain: a randomised controlled trial. Pain. 2018;159:1137‐1146. [DOI] [PubMed] [Google Scholar]
- 18. Masheb RM, Lutes LD, Kim HM, et al. Weight loss outcomes in patients with pain. Obesity. 2015;23:1778‐1784. [DOI] [PubMed] [Google Scholar]
- 19. Ryan CG, Vijayaraman A, Denny V, et al. The association between baseline persistent pain and weight change in patients attending a specialist weight management service. PLoS One. 2017;12: e0179227. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Befort CA, VanWormer JJ, DeSouza C, et al. Protocol for the rural engagement in primary care for optimizing weight reduction (RE‐POWER) trial: comparing three obesity treatment models in rural primary care. Contemp Clin Trials. 2016;47:304‐314. [DOI] [PubMed] [Google Scholar]
- 21. United States Department of Agriculture . Rural‐Urban Commuting Area Codes; 2020. Updated October 24, 2019. Accessed. https://www.ers.usda.gov/data-products/rural-urban-commuting-area-code6s.aspx January 27. [Google Scholar]
- 22. Tian TY, Zlateva I, Anderson DR. Using electronic health records data to identify patients with chronic pain in a primary care setting. JAMIA Open. 2013;20:e275‐e280. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Ainsworth BE, Haskell WL, Herrmann SD, et al. Compendium of Physical Activities: a second update of codes and MET values. Med Sci Sports Exerc. 2011;43(2011):1575‐1581. [DOI] [PubMed] [Google Scholar]
- 24. Gabriel KP, McClain JJ, Schmid KK, Storti KL, Ainsworth BE. Reliability and convergent validity of the past‐week Modifiable Activity Questionnaire. Publ Health Nutr. 2011;14:435‐442. [DOI] [PubMed] [Google Scholar]
- 25. National Institute of Diabetes, Digestive and Kidney Disorders . Type 2 Diabetes; 2020. Updated May 1, 2017. Accessed. https://www.niddk.nih.gov/health-information/diabetes/overview/what-is-diabetes/type-2-diabetes January 22. [Google Scholar]
- 26. Centers for Disease Control and Prevention . Type 2 Diabetes; 2020. Updated May 30, 2019. Accessed. https://www.cdc.gov/diabetes/basics/type2.html January 22. [Google Scholar]
- 27. Lundeen EA, Park S, Pan L, Blanck HM. Daily intake of sugar‐sweetened beverages among US adults in 9 states, by state and sociodemographic and behavioral characteristics. Prev Chronic Dis. 2016;15(2018):E154. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Thompson FE, Midthune D, Subar AF, Kipnis V, Kahle LL, Schatzkin A. Development and evaluation of a short instrument to estimate usual dietary intake of percentage energy from fat. J Am Diet Assoc. 2007;107:760‐767. [DOI] [PubMed] [Google Scholar]
- 29. Thompson FE, Midthune D, Williams GC, et al. Evaluation of a short dietary assessment instrument for percentage energy from fat in an lifestyle modification intervention study. J Nutr. 2008;138:193s‐199s. [DOI] [PubMed] [Google Scholar]
- 30. Yaroch AL, Tooze J, Thompson FE, et al. Evaluation of three short dietary instruments to assess fruit and vegetable intake: the National Cancer Institute's food attitudes and behaviors survey. J Acad Nutr Diet. 2012;112:1570‐1577. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Franz MJ, VanWormer JJ, Crain AL, et al. Weight‐loss outcomes: a systematic review and meta‐analysis of weight‐loss clinical trials with a minimum 1‐year follow‐up. J Am Diet Assoc. 2007;107:1755‐1767. [DOI] [PubMed] [Google Scholar]
- 32. Celis‐Morales CA, Perez‐Bravo F, Ibañez L, Salas C, Bailey ME, Gill JM. Objective vs. self‐reported physical activity and sedentary time: effects of measurement method on relationships with risk biomarkers. PloS One. 2012;7:e36345. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Kant AK. Dietary patterns: biomarkers and chronic disease risk. Appl Physiol Nutr Metabol. 2010;35:199‐206. [DOI] [PubMed] [Google Scholar]
- 34. Satija A, Yu E, Willett WC, Hu FB. Understanding nutritional Epidemiology and its role in policy. Adv Nutr. 2015;6:5‐18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Ray L, Lipton RB, Zimmerman ME, Katz MJ, Derby CA. Mechanisms of association between obesity and chronic pain in the elderly. Pain. 2011;152:53‐59. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Loevinger BL, Muller D, Alonso C, Coe CL. Metabolic syndrome in women with chronic pain. Metabol Open. 2007;56:87‐93. [DOI] [PubMed] [Google Scholar]
- 37. Wadden TA, Berkowitz RI, Vogt RA, Steen SN, Stunkard AJ, Foster GD. Lifestyle modification in the pharmacologic treatment of obesity: a pilot investigation of a potential primary care approach. Obes Res. 1997;5:218‐226. [DOI] [PubMed] [Google Scholar]
- 38. Williams GC, Grow VM, Freedman ZR, Ryan RM, Deci EL. Motivational predictors of weight loss and weight‐loss maintenance. J Pers Soc Psychol. 1996;70:115. [DOI] [PubMed] [Google Scholar]
- 39. Gatzounis R, Schrooten MG, Crombez G, Vlaeyen JW. Operant learning theory in pain and chronic pain rehabilitation. Curr Pain Headache Rep. 2012;16:117‐126. [DOI] [PubMed] [Google Scholar]
- 40. Hauptman J, Lucas C, Boldrin MN, Collins H, Segal KR. Orlistat in the long‐term treatment of obesity in primary care settings. Arch Fam Med. 2000;9:160. [DOI] [PubMed] [Google Scholar]
- 41. Poston W, Haddock C, Pinkston M, et al. Evaluation of a primary care‐oriented brief counselling lifestyle modification intervention for obesity with and without orlistat. J Intern Med. 2006;260:388‐398. [DOI] [PubMed] [Google Scholar]
- 42. Goessl CL. Health Literacy Changes In a Technology‐Enhanced Diabetes Prevention Program [dissertation]. Omaha, NE: University of Nebraska Medical Center; 2019. [Google Scholar]
- 43. Somers TJ, Blumenthal JA, Guilak F, et al. Pain coping skills training and lifestyle behavioral weight management in patients with knee osteoarthritis: a randomized controlled study. Pain. 2012;153(6):1199‐1209. [DOI] [PMC free article] [PubMed] [Google Scholar]