

Abstract
One-third of persons with epilepsy have seizures despite appropriate medical therapy. Drug resistant epilepsy (DRE) is associated with neurocognitive and psychological decline, poor quality of life, increased risk of premature death, and greater economic burden. Epilepsy surgery is an effective and safe treatment for a subset of people with DRE but remains one of the most underutilized evidence-based treatments in modern medicine. The reasons for this quality gap are insufficiently understood. In this comprehensive review, we compile known significant barriers to epilepsy surgery, originating from both patient/family-related factors and physician/health system components. Important patient-related factors include individual and epilepsy characteristics which bias towards continued preferential use of poorly effective medications, as well as patient perspectives and misconceptions of surgical risks and benefits. Health system and physician-related barriers include demonstrable knowledge gaps among physicians, inadequate access to comprehensive epilepsy centers, complex presurgical evaluations, insufficient research, and socioeconomic bias when choosing appropriate surgical candidates
Keywords: Barriers to care, Drug-resistant epilepsy, Epilepsy, Epilepsy surgery, Medically resistant epilepsy, Underutilization
1. Introduction
Approximately one-third of patients with epilepsy have seizures which fail to respond to drug therapy [1]. Drug resistant epilepsy (DRE) is associated with neurocognitive and psychological decline, poor quality of life, increased risk of premature death, and higher societal economic burden. Worldwide, 10 million potential surgical candidates exist out of approximately 50 million persons with epilepsy [2].
High-level evidence supports epilepsy surgery as an effective and safe treatment option for a subset of patients with DRE. In adults with temporal lobe epilepsy, a randomized controlled trial comparing surgical therapy to continued medical management demonstrated after one year only 8% of patients were free of focal impaired seizures in the medical group compared to 58% after epilepsy surgery [3]. In addition, patients in the surgical group had better quality of life. Another multicenter, controlled, parallel-group clinical trial in adults demonstrated early resective surgery (within 2 consecutive years of disabling seizures) in mesial temporal lobe epilepsy was associated with lower probability of continued seizures (11 of 15 were seizure-free during year 2 of follow up) compared to continuing medical therapy (0 of 23 participants became seizure free) [4].
Epilepsy surgery benefits children as well. A single-center randomized trial of surgery for DRE of various etiologies in children demonstrated that 77% were seizure-free in the surgical group compared to 7% in the medical therapy group (p < 0.001) at 12 months with additional improvements in behavior and quality of life in the surgery group [5]. A longitudinal study in intractable temporal lobe epilepsy showed seizure free patients after surgery recovered nonmemory (1 year postoperatively) and memory deficits (performed 2–10 years after the baseline testing) [6]. Epilepsy surgery leading to seizure freedom significantly reduces mortality rate (standardized mortality ratio of 0.45) [7]. Despite high upfront cost, resective epilepsy surgery became cost-effective between 9 and 10 years after surgery in a multi-center French study, and even earlier if all indirect cost were taken under consideration [8].
Disappointingly, despite high-quality evidence supporting improved seizure outcomes, cognitive outcomes, QOL, and higher cost-effectiveness of epilepsy surgery compared to continued medical management of DRE, epilepsy surgery remains one of the most underutilized evidence-based treatments in modern medicine [9–11]. As 25–50% of patients with DRE may be candidates for epilepsy surgery, the number of potential epilepsy surgery candidates globally is between 1 and 7.5 million people [12,13]. The degree of inadequate access to surgical treatment is potentially expected in resource-poor countries; yet, is strikingly elevated in high-income, developed countries with the availability of state-of-the art facilities. A national survey revealed only 3000–4000 epilepsy surgeries occur annually among 100,000–200,000 surgical candidates in the United States [14]. A mean interval of 22 years from the onset of epilepsy to surgical therapy further exasperates this quality gap [15].
Despite mounting clinical evidence, the rate of epilepsy surgery may be declining or static, at best. The American Academy of Neurology practice parameter in 2003 recommended “referral to a surgical epilepsy center on failing appropriate trials of first-line antiepileptic drugs” [9]. A study several years later noted no difference in the referral pattern (diagnosis of seizures to the referral in years: 17.1 ± 10.0 vs 18.6 ± 12.6 years, p = 0.39) when compared between the timeframes of 1995–1998 and 2005–2008 [16]. Jehi et al. reported the evolving pattern of epilepsy surgery between 1991 and 2011 in 9 major epilepsy centers with an overall 25% declining surgical rate with specific decline for mesial temporal lobe procedures [17].
The concerning trend in declining epilepsy surgery rates is evident across countries with varied health care systems. A population-based cohort study in the US showed a decreasing epilepsy surgery rate between 1990 and 2008 with decreased hospitalizations in high-volume surgical centers [18]. Another population-based retrospective cohort study in Ontario, Canada showed that only 1.2% of patients underwent epilepsy surgery within 2 years of DRE diagnosis despite 12% of patients dying within the same timeframe [19]. Data from the UK estimated that the occurrence of the annual number of epilepsy surgeries may keep pace with the incident cases added to the surgical pool, but does not address the treatment gap of the preexisting intractable patients [20]. In Germany, the duration of DRE prior to presurgical assessment increased from 1989 to 2009 and presurgical volume increased between 1990 and 2013 yet surgical cases remained stable due to an increasing rate of informed choice against epilepsy surgery [21,22].
A well-defined but poorly understood quality gap exists in DRE treatment with wide range barriers. To allow comprehensive analysis of barriers, we decided to undertake a scoping-review approach (rather than systematic review). With intention of broadly examine the literature on barriers to epilepsy surgery, we identified several research questions to guide (example, how important is patient attitudes and perspectives in uptake of epilepsy surgery?) the scoping review. We identified papers from PubMed and other databases with use of various combinations of the following keywords “epilepsy “and “surgery” or “surgical” or “surgical procedures” or “resecti*” or “disconnecti*”. The references within each article were then reviewed with a ‘snowball sampling’ approach to obtain further relevant articles. After reviewing title and abstracts of all these articles, relevant articles related to barriers to epilepsy surgery were reviewed in detail. Several experts of the surgical subgroup of the Pediatric Epilepsy Research Consortium (PERC) were consulted for in-depth guidance regarding appropriateness of the included references, suggestion for additional references, and provide insight beyond that available in the literature. In this paper, we summarized and reported the known barriers to epilepsy surgery in an effort to identify opportunities to increase epilepsy surgery utilization (Fig. 1). In a subsequent paper (Underutilization of Epilepsy Surgery: Part II: Strategies to Overcome Barriers), we discussed various strategies to overcome these barriers.
Fig. 1.
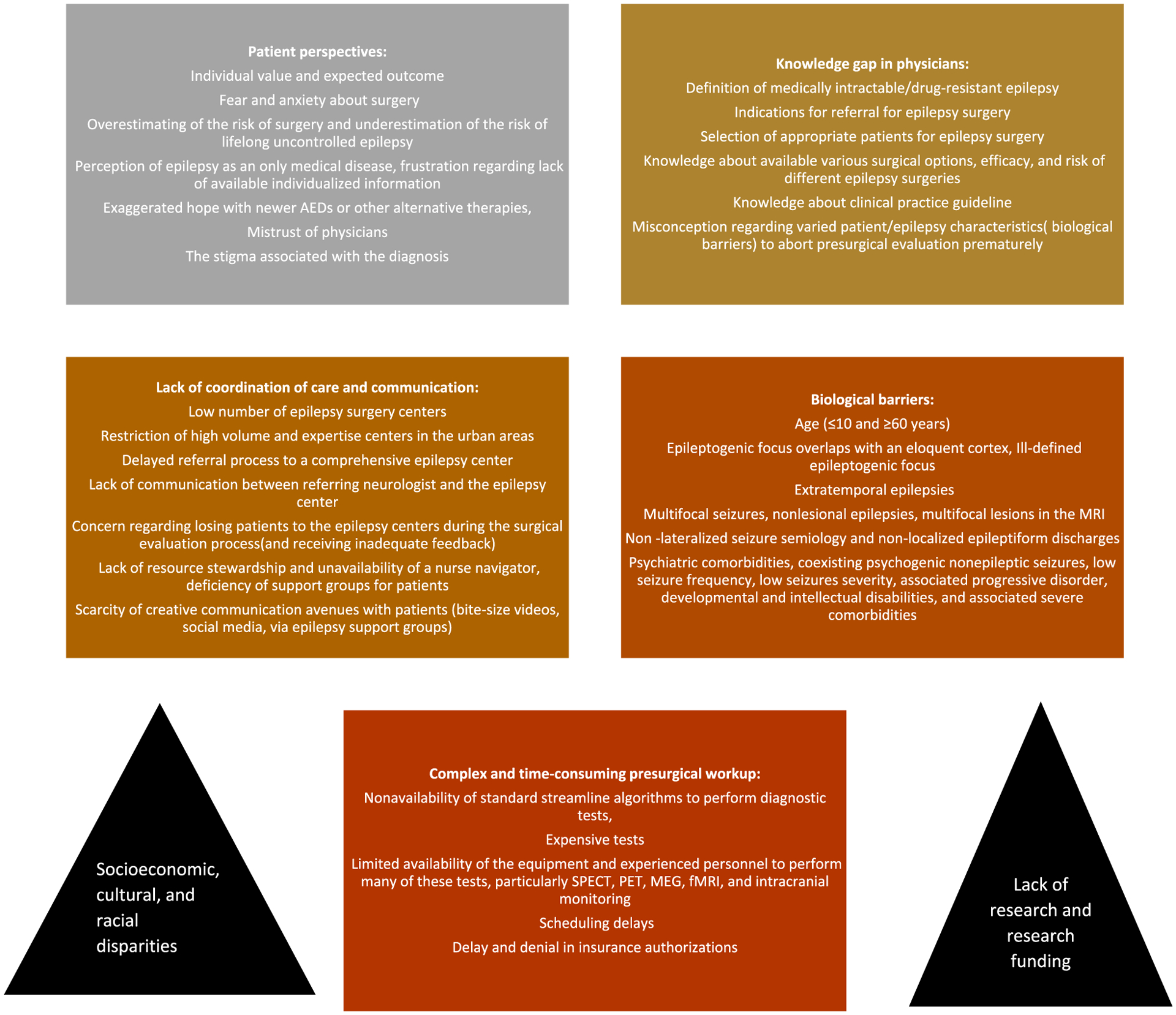
Barriers to epilepsy surgery.
Challenges related to patient attitudes and perspectives (Table 1).
Table 1.
Knowledge and attitudes about epilepsy surgery among patients and families.
| Author | Purpose | Method | Results |
|---|---|---|---|
| Swarztrauber et al. [26] | To understand patient attitudes about the treatment of medically intractable epilepsy and to document potential barriers limiting patient access to the surgical treatment of epilepsy, highlighting the attitudes of adolescents and minorities | Focus groups interviews of adults with intractable epilepsy, adolescents with intractable epilepsy, parents of adolescents with intractable epilepsy, and African-Americans with intractable epilepsy | The perceptions of the risks of the surgical treatment of epilepsy were exaggerated. Patients felt that their health care providers did not provide adequate information about epilepsy and portrayed epilepsy surgery negatively |
| Bower et al. [27] | To compare expectations prior to epilepsy surgery between men and women | Ratings of the importance of 12 potential impacts of resective surgery were analyzed in a seven-center cohort study including 389 adults aged 16 and older who underwent resective epilepsy surgery | Women rated driving, physical activity limitations, and economic worries as less important, and fatigue and pregnancy concerns as more important than men |
| Bower Baca et al. [27] | To explore racial differences in patient expectations prior to resective epilepsy surgery | A structured face-to-face interview was administered by trained research associates among 396 adults and adolescents with refractory epilepsy | Among 391 respondents, the two most frequently endorsed expectations (any rank order) were driving (62%) and job/school (43%). When only the most important (first-ranked) expectation was analyzed, driving (53%) and cognition (17%) were most frequently offered. Nonwhites endorsed job/school and cognition more frequently and driving less frequently than whites |
| Prus et al. [28] | To assess beliefs about epilepsy and brain surgery and the use of alternative epilepsy treatments in a culturally diverse population of people with epilepsy | Data were obtained from a structured questionnaire administered to 109 epilepsy patients treated at a single epilepsy center | Brain surgery was rated as having a mean dangerousness of 8.3 (on a scale of 1–10) among the 94 patients with no history of neurosurgery. In addition, 51% of these patients would not consider surgical treatment even if it were guaranteed to stop their seizures without causing deficits. Death and memory loss were both endorsed by 60 (55%) patients as “frequent negative outcomes” of brain surgery. Other perceived negative outcomes were paralysis 39(36%), stroke 28(26%), and personality change 26%(24%) |
| Choi et al. [30] | To understand patient’s decision-making process about temporal lobe epilepsy (TLE) surgery | Five focus group interviews to understand the information patients needed to make informed decisions about TLE surgery. Twenty patients who had undergone TLE surgery described the information used in their decision-making process and evaluated the potential for a patient decision aid to assist other patients who are considering surgery | Patients endorsed not receiving adequate information about surgical options from their physicians. Consequently, most patients in the study sought information independently and arrived at the epilepsy surgery center through the word-of-mouth of family and friends. Reasons for seeking a second opinion were often specific events such as loss of one’s driver’s license, the emergence of a more severe seizure type (i.e., secondarily generalized seizures), or having seizures at work |
| Erba et al. [33] | To clarify how “ready” parents of children with epilepsy may be to consider and accept an unfamiliar, risky treatment such as surgery and how the doctors prepare them for such a decision | Ad hoc questionnaires to parents of children with epilepsy scheduled for regular follow-up appointments at six pediatric epilepsy centers | Among 138 parents of pediatric patients with epilepsy, 25.2%were opposed to epilepsy surgery. However, upon completing the questionnaire that contained factual information about surgery, 50.4% of the responders stated that they had become more favorable vs. 3.3% more hesitant, and 46.3% unchanged |
| Hrzadil et al. [24] | To understand patient knowledge and perceptions regarding epilepsy surgery | A 5-min questionnaire was administered to consecutive adults with focal epilepsy seen in the epilepsy clinic in a large Canadian health region | Most participants (82.9%) were aware that surgery might be an option; however, only 51.9% knew of their own surgical candidacy. The most common information source for epilepsy surgery was the patient’s neurologist or neurosurgeon (65.4%), 21.9% had previously been discouraged from having brain surgery for their epilepsy, this advice most commonly came from a treating neurologist (65.2% of the time). Many patients (55.4%) perceived epilepsy surgery to be very or moderately dangerous. 64.7% rather take part in a nonsurgical research study prior to epilepsy surgery. 61.0% considered brain surgery as a last resort. 14% would decline surgery even if they could be guaranteed seizure freedom without neurological damage. 60% of patients incorrectly identified the risk of overall serious side effects from epilepsy surgery to be over 10%, with the risk of death (17.7%), stroke (32.0%), vision loss (37.4%), personality change (42%), paralysis (42.3%), difficulties in speaking (42.9%), or memory loss(60.4%) Only 44.3% considered uncontrolled seizure more dangerous than epilepsy surgery |
| Anderson et al. [29] | To explore the socio cultural, medical, personal, and psychological differences between candidates who chose (n = 23) and those who declined surgical intervention (n = 9) | A novel questionnaire addressing a range of possible factors important in patient decision making | It was found that patients who declined surgery were less bothered by their epilepsy (despite comparable severity), more anxious about surgery, and less likely to listen to their doctors (and others) and had more comorbid psychiatric diseases. Patients who chose surgery were more embarrassed by their seizures, more interested in being ”seizure-free,” and less anxious about specific aspects of surgery |
| Pieters et al. [70] | To describe experiences during the arduous time before the epilepsy surgery referral and the parent reported facilitators that helped them move forward through this slow time | Individual semi-structured interviews with 37 parents of children who had previously undergone epilepsy surgery | Parental decision-making was facilitated when parents eventually received a presurgical referral and navigated to a multidisciplinary team that they trusted to care for their child with medically refractory epilepsy |
| Ladino et al. [25] | To assess knowledge and attitudes toward epilepsy surgery among patients with epilepsy and identify barriers that might delay the treatment | A 10-minute questionnaire was administered to patients with epilepsy in Colombia | More than half of the patients (56%) were not aware that surgery might be an option. Apprehension about epilepsy surgery was evident; 60% of patients perceived epilepsy surgery to be very or moderately dangerous. A large proportion of patients believe death (41%), stroke (47%), vision loss (56%), personality change (56%), paralysis (62%), difficulties in speaking (69%), and memory loss (60%) were frequent side effects. The majority of patients (62%) consider the surgical procedure as the last option of treatment |
1.1. Misconceptions regarding surgery, lack of self-exploration, lack of individualized information
Patient attitudes and perspectives regarding epilepsy surgery are founded in social and education background and further developed by experience with healthcare systems and information or misinformation from providers, the internet, social media, and community resources. Regrettably, the misconception that epilepsy is a purely pharmacologically-treated disease is prevalent [23]. Many patients consider epilepsy surgery as an experimental procedure despite use for more than 100 years. Though general awareness regarding epilepsy surgery is increasing, many patients with intractable epilepsy (51.9–56%) are unaware if they are candidates for surgical evaluation [24,25]. Additionally, patients’ negative attitudes and perspectives about epilepsy can act as a major barrier; patients may refuse surgery if they perceive their epilepsy is not “severe” (may not correlate with objective assessment), experience excessive anxiety about surgery, are not adherent with healthcare providers’ advice, and suffer from comorbid psychiatric disease [25–29]. Patients and families may develop negative attitudes towards epilepsy surgery if exposed to healthcare professionals with bias against surgery or if various providers provide inconsistent information.
A request for epilepsy surgery from the patient and family is more likely to occur after a specific life event such as loss of a driver’s license or prolonged/convulsive seizure, rather than after systematic exploration of options early in the disease course [30]. Self-exploration for epilepsy surgery may be a reflection of education, empowerment, and ownership of healthcare decisions and dependent on the patient’s values, outcome expectation, education, and socioeconomic status.
Measuring patient-reported determinants of health and wellbeing is particularly crucial when counseling about treatment, and expected outcomes may be significantly different between genders and races [27]. Unfortunately, a standardized instrument to evaluate a patient’s expectations for epilepsy surgery and expected outcomes does not exist, although some researchers have suggested using the Patient Reported Implementation Science model [31]. Rather than receiving generic information about efficacy and success, many patients prefer individualized outcomes data related to their specific situation in order to make an informed decision [30]. Lack of a descriptive summary of various possible complications (e.g., impact of functional deficits) make patients anxious and may cause delay or a refusal for surgery. Finally, the stigma associated with epilepsy and mistrust of physicians are other barriers which may lead to delayed care, including consideration of epilepsy surgery.
1.2. Fear and misconceptions about surgical risk and inappropriate hope regarding nonsurgical treatments
An alarming fear of surgery exists, with a majority (55.4–60%) of patients considering epilepsy surgery as a moderate to very high-risk intervention. Several studies identified an overestimation of surgery risks with a large proportion of patients having anxiety about death (41–55%), memory loss (60%), stroke (26–47%), paralysis (36–62%), and personality change (24–56%) [24,25,32]. Surprisingly, patients (14.2–51%) are willing to refuse surgery even if guaranteed seizure freedom without any neurologic deficits [24,32] and approximately one-fourth to one-third of patients refuse surgery despite their physician’s recommendation [33].
We postulate several reasons behind these miscalculations. Many patients underestimate the risks associated with lifelong uncontrolled epilepsy with a significant tolerance of disability, thus considering epilepsy surgery as a ‘last-ditch effort’ only. Despite lack of evidence, patients may have unfounded expectation of becoming seizure-free with the addition of new AEDs, other alternative nonsurgical therapies, or participation in research studies. Thanks to improving side effect profiles of newer AEDs, patients may be willing to tolerate multiple AED trials given reduced burden of side effects. Additionally, some patients and families may assume a disability mindset secondary to chronic epilepsy diagnosis and fear an uncertain future if seizure freedom leads to the loss of disadvantaged/sick status.
2. Physician specific barriers (Table 2)
Table 2.
Knowledge and attitudes about epilepsy surgery among physicians.
| Author | Purpose | Method | Results |
|---|---|---|---|
| Hakimi et al. [34] | To describe the different views held by neurologists regarding refractory epilepsy that may contribute to the delay in referring patients for epilepsy surgery | Neurologists in Michigan were mailed a 10-item survey inquiring about their definition of medically refractory epilepsy and their decision-making process in referring patients for epilepsy surgery | The majority of neurologists defined medically refractory epilepsy as failure of three monotherapy antiepileptic drug (AEDs) trials and at least two polytherapy trials. Nineteen percent responded that all approved AEDs had to fail before a patient could be defined as medically refractory. Eighty-two percent of the respondents had referred patients for epilepsy surgery. Almost 50% were not satisfied with the level of communication from epilepsy centers. One-third reported serious complications resulting from surgery |
| Kumlien et al. [35] | To investigate Swedish neurologists’ views and criteria for referral for epilepsy surgery | A survey was sent out to neurologists who treat patients with epilepsy. | Sixty-one percent of respondents considered that epilepsy surgery reduced seizure frequency and 53% that it improved quality of life. Surgical treatment was thought to be cost-effective by 90% of respondents. Referral for surgery was considered if three or more antiepileptic drugs had failed. Seizure frequency and severity and the patient’s own wishes were regarded as the most important criteria for surgical referral. MRI and EEG findings were also important, whereas the duration of illness was considered less important. Age below 65 years and lack of intellectual impairment were important for considering referral |
| Hall-Patch et al. [35] | To explore UK pediatric neurologists’ views regarding resective surgery for medically refractory epilepsies in children. | Cross-sectional survey methodology | The majority (84%; 31/37) felt that surgery was under-recommended Those working in epilepsy surgery centers showed a slight but non-significant tendency to fit more closely to the published guidance of failure of two AED monotherapy trials, no polytherapy failure needed, and did not need to fail ketogenic diet. 56% (14/25) had o experienced problems with liaison and information provision with the referring center. A minority (16%; 4/25) had the experience of a patient not being returned to their care in an appropriate time frame |
| Erba et al. [33] | To assess how pediatric neurologists approach the issue of epilepsy surgery | Physicians were surveyed with a 14 item questionnaire based on the theory of planned behavior | Out of 60 child neurologists who provided all responses, point of view of 24 (40%) were aligned with the opinion leaders, whereas viewpoint of the remaining 36 (60%) laid outside the 5th percentile of the experts’ curve indicating disagreement. |
| Cothros et al. [40] | Knowledge and Attitudes About Epilepsy Surgery Among Family Doctors in Ontario | Physicians were surveyed regarding demographics, referral practices, and general knowledge about epilepsy surgery | The majority of family physicians (81%) always referred patients with epilepsy, most often to neurologists. General knowledge of epilepsy was mixed, with 53.7% feeling that surgery should be considered in selected cases for the treatment of epilepsy, though 53.2% did not know what type of epilepsy could be surgically treated. 3.5% reported that surgery should never be considered and 14.9% that surgery should be considered only as a last resort. The largest percentage of responses (43.8%) did not have knowledge about surgical risk, and nearly 50% felt surgery constituted a moderate to very high risk |
| Erba et al. [41] | To assess knowledge and attitudes toward epilepsy surgery among practicing neurologists and identify the barriers that delay the treatment | 183 Italian adult and child neurologists were surveyed with an ad hoc questionnaire exploring physicians’ willingness to refer patients for epilepsy surgery when such treatment may be indicated | The majority of Italian neurologists have highly variable attitudes toward epilepsy surgery, reflecting ambivalence and uncertainty toward this type of treatment. About two-thirds of responders are nonaligned with the opinion leaders, mainly due to differences in handling pharmacologic treatment and information regarding epilepsy surgery, which affect their attitudes and, ultimately, patient management. |
| Roberts et al. [37] | To assess potential neurologist-related barriers to epilepsy surgery among Canadian neurologists | A 29-item, pilot-tested questionnaire was mailed to all neurologists registered to practice in Canada | More than half (56.6%) of neurologists required patients to be drug-resistant and to have at least one seizure per year before considering surgery, and nearly half (48.6%) failed to correctly define drug-resistant epilepsy. Other barriers were to fail to consider surgery in patients with generalized epilepsy, epileptic encephalopathy, psychiatric comorbidities, non-lesional focal epilepsy, and developmental delay. 45% of participants were not aware of AAN clinical practice guidelines on the temporal lobe and localized neocortical resections for Epilepsy and 30% considered epilepsy surgery as a last resort treatment for epilepsy |
| Uijl et al. [38] | To quantify under referral for epilepsy surgery in the Netherlands, and reveal its causes | Medical records of medically refractory epilepsy patients were judged by an expert panel whether epilepsy surgery referral should have been done according to published Dutch guidelines and the treating neurologists were approached to understand the reasons behind non-referral | Approximately 25% of the reasons were considered valid, such as Type/classification of epilepsy, type of seizures, contra-indication for surgery, comorbidity, low seizure frequency, the low burden of seizures (judgement of patient), and patient’s refusal 75% of total reasons were considered not valid, such as the low burden of seizures (judgment of neurologist), psychogenic seizures apart from epileptic seizures, psychiatric comorbidity, referral to screening program >5 yrs. ago |
2.1. Knowledge gaps, lack of access to practical guidelines, and lack of adequate hands-on training
A patient with DRE receives care from primary care providers, emergency room physicians, neurologists, epileptologists, and occasionally neurosurgeons. As previously discussed, the attitude of patients and families towards epilepsy surgery may be highly dependent on the knowledge and attitude of healthcare providers. However, a significant deficit in knowledge may exist among these providers about the definition of DRE (48.6%), awareness about existing practice guidelines (45%), indications and timing for epilepsy surgery referral (14.9–30%), and knowledge about particular epilepsies that are amenable to epilepsy surgery (53.2%) [33–40].
In general, neurologists may have misaligned opinions (60–75%) about referral practices with experts in the field, leading to poor quality epilepsy care [38,40]. Familiarity with epilepsy surgery is more likely to occur through an existing practice of referring patients for surgery (potentially related to epilepsy surgery exposure during training and clinical practice) rather than number of years in clinical practice [41]. Providers may also have a lack of understanding and knowledge (43.8–50% of family medicine and neurology providers) about surgical risks and benefits [34,39]. Although clinical guidelines may improve knowledge base among healthcare professionals, inadequate adaptation of guidelines to the local context may prevent translation of knowledge to clinically meaningful practice in real-world settings [42].
Additional barriers exist for disseminating practice in developing countries and among neurosurgeons. Almost all existing guidelines for epilepsy surgery are written in English. This can be a barrier for appropriate uptake and dissemination among non-English speaking physicians [37]. For neurosurgeons, emerging evidence reveals a significant lack of adequate training and education about epilepsy surgery among neurosurgery trainees with limited instruction and hands-on training during residency [43]. Additionally, interested neurosurgeons, even in developed countries, face significant difficulties finding a dedicated epilepsy surgery fellowship program for additional practical clinical training along with understanding in basic neurophysiology and advanced neuroimaging techniques.
2.2. Lack of exposure/experience with epilepsy surgery and evidence-based guideline
Senior neurologists (especially without epilepsy specialization), may be less knowledgeable about the latest evidence-based research and guidelines and are less likely to refer patients for surgical evaluation. In a study among Canadian neurologists, Roberts et al. reported that neurologists who had graduated from medical school before the year 2000 had higher neurologist-related barriers to surgery. The year 2000 was selected as neurologists graduating before that time might not have access to first epilepsy surgery RCT and related practice guideline during their residency training [37]. Regardless of years of experience, the physician’s lack of exposure/experience with epilepsy surgery during clinical training and practice may be a significant barrier to epilepsy surgery [41].
2.3. Biological factors as barriers to epilepsy surgery
Specific epilepsy characteristics can be an additional barrier for surgery. Due to challenges associated with surgical decision making and other biases, certain group of patients (extremes of ages, MRI-negative DRE, epilepsy associated with apparently generalized or multifocal interictal abnormalities, associated comorbidities) may be insufficiently referred on the referring providers’ perception about poor surgical outcome or utility of epilepsy surgery [38,44].
2.3.1. Infants and young children
Age can be a significant barrier for epilepsy surgery. Fewer surgeries are performed in the extremes of age (≤1 and ≥60 years). Although, the absolute number of pediatric epilepsy surgeries in the United States increased from 375 in 1997 to 706 in 2009, the number of surgeries in infants remained stable [45]. Even when surgery is performed in young children, an unacceptable delay is common despite the risk for enduring negative consequences to development [46]. For example, there was an average delay of one year for determination of surgical candidacy in 87 Australian children with drug-resistant early-onset epilepsy (onset less than 3 years of age) [47]. Median interval from seizure onset to epilepsy surgery was 2.5 years, with longer timeframes associated with functional neuroimaging, worse rates of seizure-freedom, and treatment with multiple AEDs. A history of infantile spasms and daily seizures were associated with a lesser delay to surgery. These delays may be secondary to the belief intractable seizures may spontaneously resolve.
The preoperative evaluation and surgical management of infants and toddlers with DRE holds numerous challenges [48]. For example, initial MRI may not reveal an evident cortical dysplasia in early infancy. Some children will need MRI every six months until 24–30 months of age before subtle cortical dysplasia may become overt with the maturation of myelination [49]. Fear exists about surgical complications in young infants such as high mortality and severe morbidity in children less than three years of age due to massive blood loss and coagulopathies during surgery [50]. This is particularly true for large craniotomies and surgeries of considerable duration such as hemispherectomy and multilobar resections that are more common in this age group. In addition, invasive monitoring with intracranial electrodes and functional mapping in young children is challenging due to perceived poor tolerance of chronic intracranial monitoring particularly with grids. While stereoelectroencephalography (stereo-EEG) provides some advantages, it is difficult in children ≤2 years due to skull thickness [51].
2.3.2. Older adults
On the other end of the age spectrum, surgical therapy is rarely offered to older adults with DRE. Older adults with epilepsy continue to worry about stigmatization and suffer adverse psychosocial outcomes, particularly if unable to drive (64% of the participants in one study) due to continued seizures [52,53]. While there was agreement in 1992 that no upper age limit for surgery should be set, few centers perform epilepsy surgery in older adults [54]. A recent systematic literature review found only 58 older adults (≥60 years old) with seizure-outcome data in the existing literature [55]. Although epilepsy after age 65 is 5 times more common than other adult age ranges, the average age of surgical patients was 31 years in the US over the past two decades [18]. Despite excellent postoperative seizure free outcomes, epilepsy surgery is less commonly offered to older adults (≥60 years old) due to associated higher burden of comorbidities, cognitive outcome, and longer duration of epilepsy [55] and poor understanding regarding biological and chronological age during evaluation for epilepsy surgery [56].
2.3.3. Overlapping epileptogenic foci and eloquent cortex
Patients and providers share concerns about neurological deficits associated with epilepsy surgery, but particularly if the epileptogenic zone overlaps with eloquent cortex or critical functional networks. A complex bioethical dilemma exists between accepting the risk of postoperative deficit against the possibility of seizure-freedom and improved quality of life for the patient [57,58]. As stereo-EEG is emerging as the preferred modality for intracranial monitoring over subdural electrodes, there are further challenges for localization of eloquent cortical areas, because of sparse sampling on cortical surface with stereo-EEG, and perceived inability to define the extent of functional areas [59]. Although there is emerging evidence for diagnostic validity and safety of high-gamma modulation (HGM) for functional brain mapping with intracranial EEG, this modality remains primarily experimental and is not accessible to most epilepsy surgery programs [60]. Besides pre-surgical mapping, a global survey performed by the Pediatric Epilepsy Surgery Task Force of the International League Against Epilepsy (ILAE) showed less than optimum use of protective strategies during surgery such as awake surgery for language mapping (33% respondents not using it) or subcortical mapping with tractography (45% denied using this) [61].
2.3.4. Non-lateralized or localized seizure semiology, non-lesional or multifocal epilepsy
Seizure semiology has high lateralizing (74%) and localizing (77%) value but may be discordant with regards to epilepsy type [62]. Some patients with generalized semiology may not even undergo neuroimaging or video-EEG studies, contributing to misclassification of the epilepsy syndrome present in a third of intractable patients [63]. Furthermore, non-lateralized or localized seizure semiology may present unique challenges for the surgical treatment of epilepsy [64]. Several epilepsy types, such as infantile spasms, non-lateralized tonic seizures, focal seizures with rapid propagation to bilateral tonic-clonic seizures, and frontal lobe seizures, can be misclassified as generalized epilepsy.
Moreover, EEG and neuroimaging studies may not provide straightforward guidance in a large proportion of cases. Electroencephalography (EEGs) (ictal and interictal epileptiform discharges) may be non-indicative of localization or lateralization. Lateralizing value of interictal (50–66%) and ictal EEGs (variable) in extra temporal epilepsies are much lower than that noted in temporal lobe epilepsy (interictal EEG- approximately 75% and ictal EEG- 80–92%) [65]. Additionally, the ictal recording may reveal that seizures are originating from multifocal regions or that an epileptogenic focus cannot be identified with certainty even after extensive presurgical evaluation. Those with apparent multifocal seizures or seizures originating from both hemispheres with multiple independent foci have a lower likelihood for seizure freedom and require additional expertise for accurate seizure mapping or consideration for palliative surgery options. Even when anatomic localization is possible, the surgical outcome for extratemporal epilepsies is considered to be less favorable, particularly in patients with normal neuroimaging [66]. The absence of structural lesions or presence of multifocal lesions can therefore become additional barriers for surgical decision making.
2.3.5. Other patient and epilepsy characteristics to be perceived as poor surgical candidates
Other patient and epilepsy characteristics perceived to be indicators of poor surgical candidacy are those with psychiatric comorbidities, autism and other severe behavioral abnormalities, low seizure frequency or severity, associated progressive neurological disorders, developmental and intellectual disabilities, and concurrent severe medical conditions [67,68].
3. Healthcare system
3.1. Lack of communication and coordination of care
3.1.1. Barriers related to ineffective communication
The journey from the first seizure to surgery is usually long, complicated and exceptionally agonizing in the absence of a coordinated treatment approach and excellent communication [69,70]. In the early stages of epilepsy diagnosis and medication management, primary care physicians (pediatricians or family practitioners), general neurologists or even epileptologists may use discouraging words, phrases or sentences when describing the option of epilepsy surgery. These statements can permanently make individuals reluctant to consider surgery. Time-constraints in the busy clinical practice may also lead to ineffective communication between healthcare professionals and patients. Some physicians are inadequately trained on how to present evidence-based information related to epilepsy surgery in a fashion to help patients make an informed decision. In addition, providers are not given adequate opportunities to learn about effective communication strategies. We lack workshops to train physicians on how to effectively listen to patients and families to understand their viewpoint and to provide individualized information about the efficacy and risk of epilepsy surgery.
3.2. Barriers related to physician-only care model
Many healthcare systems are still predominantly relying on clinical expertise and counselling services provided by physicians only without the use of valuable ancillary staff such as nurse specialists, educators, nurse navigators, and clinic managers. Physicians face an increasing challenge to foster a trusting doctor–patient relationship in busy clinical settings when clinical encounters are getting progressively shorter in duration. Even well-educated families often cannot handle the vast amount of information given during clinic encounters and then navigate the complex process of presurgical evaluation, let alone the decision to pursue surgery. Outside the direct clinical care and brief interaction with the provider, many families are without direction and lack adequate social support to help with the decision making process. In addition, providers may lose track of surgery candidates in the midst of busy practice stranding patients during the diagnostic odyssey of presurgical evaluation. Unfortunately, copious information about epilepsy surgery available through social media is not always evidence-based and rather than helping patients and families to understand the benefits and risks of epilepsy surgery, this information may unintentionally deter them from the surgical evaluation. Dedicated nurses may improve communication and patient satisfaction during epilepsy care through spending additional time answering or framing questions, sifting through social media disinformation and providing a more accessible point of contact [70]. However, improved outcome (prevention of surgical delays, cost-benefit, increase in the surgical volume) from the employment of nurse navigators is inadequately investigated in the epilepsy care [71].
3.3. Inadequate health-care access
3.3.1. Communication barrier between community neurologists and epilepsy centers
Providers identify inadequate health-care access (such as long wait times to see specialists, limited resources, referral delays, long distance travel required for the patients, etc., in some studies >75% of the participants) as the single largest barrier to epilepsy surgery [37]. Many community practices do not have streamlined services for patients with DRE or a shared practice model (examples: Patient-Centered Specialty Practice Model or the Veterans Health Administration Epilepsy Centers of Excellence system) with good collaboration between a comprehensive epilepsy center and community neurologists [72]. Although there is a significant deficiency in the continuum of care in the management of DRE with no clear delineation of role and responsibilities among major stakeholders (primary care providers, neurologists, epileptologists, and neurosurgeon), disjointed care becomes especially baffling during any transition process (between community neurologist to epileptologist, between two epilepsy centers, between pediatric and adult epilepsy center). Poor communication and relationships between community neurologists and the surgical epilepsy center can be a significant barrier. Many neurologists do not receive adequate feedback (50–56% of cases in various studies) from the epilepsy centers after referral [34,35]. This can in turn lead to decreased future referrals. Many community neurologists are hesitant to refer patients to experienced centers due to fear of losing decision-making capacity after referral and ultimately losing those patients (16% in one study) to the epilepsy centers [35]. Another barrier can be specialists’ attitude towards primary care providers. In many instances primary providers are often not involved in the ongoing care. However, due to long-term relationships with the family, primary providers may have a better understanding of the family’s attitude regarding surgery and are able to discuss epilepsy surgery more effectively with the family.
3.3.2. Referral, diagnostic, and treatment delays
Most high volume and experienced comprehensive epilepsy centers are concentrated in urban areas. Regional access to epilepsy surgery centers is impeded in many areas due to weak referral systems or lack of centralized subspecialty care [16,73,74]. Access to a comprehensive epilepsy program is particularly sparse in developing countries [75]. However, similarities across dissimilar health systems exist. For instance, despite significant differences between Canada and Mexico’s health delivery system and financial resources, delay in presurgical referral and epilepsy surgery was universal in both countries, with an average waiting period of 20 years prior to surgery [76]. A survey from Central and East European countries (publicly-funded health systems) showed that only 7 out of 10 countries had epilepsy surgery centers with the wait time of epilepsy surgery range from 2 weeks to 3 years [77]. Data from 2 adult tertiary epilepsy centers in New South Wales, Australia, demonstrated less delay compared to the Canada–Mexico study, with a mean duration from the 1st visit to the 1st post-operative visit of 1 year [78]. Data regarding the source of the delays are lacking, although scheduling diagnostic evaluation is one identified source [79].
3.3.3. Systemic inequities in access
Racial, ethnic, socioeconomic, and cultural disparities may restrict patient-access to epilepsy surgery [80]. A study from Alabama, USA, demonstrated that African Americans were 60% less likely compared to non-Hispanic whites to receive surgical treatment for intractable temporal lobe epilepsy due to mesial temporal sclerosis [81]. A large payer database study of 2010–2012 showed Blacks had disproportionately less number of epilepsy surgery than Whites [82]. Disparities in health resource use in epilepsy have been noted in minority populations (example, aboriginals in Canada) in other countries as well, but international research specifically focused on disparities in access to surgical care is limited [83].
The exact source of racial and ethnic disparities in accessing surgical care in epilepsy is unknown. Social determinants of health, such as disparate access to health services, health insurance coverage, income inequality, employment, health literacy and levels of trust impact care in epilepsy [84,85]. Additionally, African Americans with intractable epilepsy may have a lower negative psychosocial effect such as anxiety or hopelessness compared to other races [86,87]. However, these patient-centered factors might be developed with prior inequitable communication and previous experiences with the health care system. Disparities can be generated from overt or unconscious institutional or physician discrimination and bias in the healthcare system [88]. As the racial and economic status, education and insurance coverage are very closely related, a causal association of one individual factor with the access to epilepsy surgery is difficult to determine. Besides a lower rate of epilepsy surgery in nonwhite patients, patients receiving coverage through federal insurance programs and patients with lower economic status may have a lower rate of epilepsy surgery. Rural residence, poor relation with treating clinicians, and absence of regular employment can also be potential barriers to epilepsy surgery [80]. Despite higher incidence and prevalence of epilepsy among low-income individuals, higher risk of untreated epilepsy is present in this population with lack of transportation to the clinic appointments, lack of insurance for completion of preoperative testing and surgery, and lack of financial incentive for physicians to embark on the arduous and complicated process of presurgical workup.
Unfortunately, both public and private payers, may be reluctant to approve diagnostic testing for presurgical evaluation and surgery despite favorable cost-effectiveness of epilepsy surgery [69]. Disparities exist between payers as well. Adult temporal lobe epilepsy patients with private insurance were 85% more likely to receive surgery compared with public insurance or self-pay [89]. Ultimately, providers, patients and family may become frustrated with these additional diagnostic and treatment delays.
3.4. Issues in scheduling diagnostic workup and ineffective use of patient care conference
Besides the lack of dedicated epilepsy surgery clinics, referral challenges, and communication failure, there are problems with scheduling diagnostic workups even in comprehensive epilepsy centers [79]. Lack of resource stewardship can be an obstacle to the completion of the timely evaluation. Infrequent patient care/epilepsy surgery conferences to thoroughly discuss patients can be another barrier. During epilepsy surgery case-conference, there may be asymmetric decision making by a forceful presentation of one physician, who may have a bias against epilepsy surgery, and that can lead to ‘group thinking.’ Individual expertise (based on the physician’s age, experience, exposure, seniority, etc.) may trump a group decision-making process without widespread use of objective tools. Unfortunately, clinical decision making is still predominantly done in a routine, fast, automatic, and intuitive fashion. Although epilepsy surgical conferences can enforce an effortful, slow, conscious, and analytical approach of decision making, the decision-making process can still be erroneous with cognitive biases related to overconfidence, confirmation, diagnostic momentum, availability, and anchoring.
4. Scientific challenges
4.1. Lack of research in epilepsy surgery
The paucity of research to address the underlying causes of disparities in epilepsy surgery evaluation is unfortunate and prevents establishment of policies and programs to reduce disparities in accessing epilepsy surgery [90,91]. There is a shortage of comparative studies to explore the knowledge and attitude of families undergoing epilepsy surgery versus refusing it. Disproportionate deficiency of qualitative research to understand the patient’s viewpoint is extraordinarily glaring. The efficacy of educational and behavioral intervention studies targeting misconceptions of patients and families is unknown. There is also a lack of studies to understand attitudes and education within society regarding epilepsy surgery. Additionally, controlled, high-quality research studies are significantly lacking. For example, there has not been any randomized controlled trial to evaluate the effectiveness of focal neocortical epilepsy surgeries. However, there is no denying there would be significant challenges recruiting patients in epilepsy surgery trials [4]. Besides the lack of randomized control trials for specific subsets of epilepsy surgery, shortage of rigorous prospective studies is also prevalent with a paucity of outcome data regarding efficacy, safety, neuropsychological outcome, and change in the quality of life after epilepsy surgery. Aside from seizure-freedom, there is a deficiency of patient-reported outcome studies to measure improved cognitive function, decreases or cessation of medication to eliminate side effects, ability to drive, return to normal activities, etc. after epilepsy surgery.
4.2. Inequity in research funding
Additionally, there has been a disproportionate allocation of resources to other neurological problems with higher public profiles and less social stigma than epilepsy, for example, amyotrophic lateral sclerosis (ALS) research received more than 60 times of NIH funding-adjusted for disease prevalence-compared to the funding in epilepsy research in 2010 [92,93]. Even within epilepsy, there is increased allocation of resources to palliative procedures such as VNS rather than potentially curative epilepsy surgeries [94]. In particular, epilepsy surgery research may be solely dependent on government funding, without any sponsorship from the pharmaceutical and medical device industry.
5. Barriers at the comprehensive epilepsy surgery centers
Besides barriers related to access to epilepsy surgery evaluation, there are many barriers to ultimate completion of epilepsy surgery. The list of barriers is substantial: complex, nonstandardized presurgical workups, lack of class I and II studies evaluating strengths, caveats, and pitfalls of ancillary tests, lack of availability of ancillary tests due to high cost in acquisition and maintenance of such tools and the need of experienced and highly qualified personnel to run these tests, paucity of collaboration among epilepsy centers, deficiency in the systematically updated publicly available transparent database of epilepsy surgery in the epilepsy centers to allow comparison of surgical volumes and outcome, and rising rates of complex cases that may lead to complex evaluation without ultimate surgery.
5.1. Complex and time-consuming presurgical workup
5.1.1. Lack of high quality MRI with expert interpretation
Most patients with DRE need several diagnostic tests before the provision of definitive surgery. With the possible exception of EEG, a high-quality brain MRI is the most important among all the diagnostic tests. However, there are significant barriers to getting high-quality neuroimaging studies such as availability of MRI in developing countries, the performance of all necessary sequences necessary for epilepsy specific evaluation (sensitivity of detection of epileptogenic lesion decreases to 50% from 91%), availability of 3T MRI versus 1.5T MRI (5–65% new lesional diagnosis with 3T MRI), accessibility of expert radiologists (neuroradiologists vs. general radiologists) to review the brain MRI (sensitivity increased to 91% from 31%), and post-processing capability for subtle structural defects [95–97]. A lack of post-hoc review of the brain MRI (after completion of other studies, such as PET, SPECT, or MEG) can also miss subtle neuroimaging findings and negatively affect surgical decision making. Besides unfavorable surgical outcomes of nonlesional cases, the absence of visible lesion in the MRI may make patients decline to proceed with the surgery due to a lack of visualization of ‘any abnormality.’
5.1.2. Access issues in advanced imaging and source localization studies and lack of consensus in use of these tools
Apart from brain MRI and video EEG, there are several other advanced imaging and source localization studies available for complex cases; however, these tests have not been evaluated in age or etiology specific epilepsies and have been investigated in a heterogeneous population. Across centers, significant variability of these tests exist, both in availability and practices [98]. Due to lack of a standard algorithm and the cultural bias of the institute, individual opinion and personal preferences of the physicians often guides the selection of various diagnostic tests. Patients may become confused with multiple options that may be vastly different depending on the institutional availability of technologies. In addition, although lack of availability of specific tests can be responsible for missing critical information necessary to proceed to surgery, accessibility of too many ancillary tests can also construct a puzzling situation if these produce discordant results. Notably, several of these diagnostic tests have limited availability due to the cost of the equipment and or need for the experienced personnel to perform the tests, e.g., SPECT, PET, MEG, fMRI, and intracranial monitoring. There is also a lack of understanding of the cost-effectiveness of these various advanced technologies utilized during presurgical workup [99]. Interpretation of the utility of individual technology is challenging to assess in terms of diagnostic accuracy, impact on the treatment decision, and impact on the final clinical outcome after epilepsy surgery. The added value of a particular diagnostic technology in many cases is under-researched and unknown. The available new technologies may gradually increase the evaluation rate and safety of epilepsy surgery; however, it will prolong the evaluation timeframe and may not dramatically increase the surgical success rate, which may be more directly related to the underlying pathology. In the end, it is unknown if sparing use of only high-yield tests is comparable to the generous use of all available tests to provide convergence of data and raising the confidence level of the treating team.
5.2. Complexity associated with invasive diagnostic monitoring
Other than noninvasive evaluation, there is an increasing need for intracranial monitoring with the emergence of more nonlesional cases to characterize the epileptogenic zone better. However, a multicenter study demonstrated that consensus regarding the need of intracranial monitoring among various centers was only fair (intraclass correlation coefficients of 0.5397) [100]. The intra cranial monitoring method can be conventional subdural grids and EEG strips, or stereo-EEG or both. Stereo EEG technology was developed in France in the 1950s but has only become widely utilized outside Europe in recent years, thus creating a significant barrier to access deep areas of the brain such as periventricular regions, insula, and interhemispheric cortex [101]. Unfortunately the expertise to perform stereo EEG is highly variable at different epilepsy centers across the country and the world despite its significantly favorable adverse effect profile compared to traditional subdural electrode implantation [102].
5.3. Low volume epilepsy surgery centers
5.3.1. Increasing number of low volume centers in the setting of increasing complexity of surgical cases
Notably, there has been an explosion of low volume epilepsy surgery centers in the US recently (between 2003 and 2012 the number of centers increased from 37 to 189) [103]. However, individual center can fulfill criteria to become a level 3 or 4 center without performing a large number of epilepsy surgery cases if meet other criteria pertinent to resource requirements and center capabilities. Level 3 centers can potentially deal with temporal lobectomies and lesionectomies (particularly tumor surgery), though complex cases such as nonlesional, multifocal seizures or extratemporal epilepsies may still need to be evaluated in high volume specialized centers [103]. Notably, the increasing complexity of the patients in the surgical pool has been established in several studies. Barba et al. retrospectively evaluated volume and type of epilepsy surgery among nine epilepsy surgery centers in Italy over a period of 7 years (2008–2014) and noted increasing complexity of pediatric epilepsy surgery [104]. In another retrospective study comprising of data from 10 European countries also showed that the total number of pediatric epilepsy surgeries increased from 383 in 2008–2009 to 551 in 2014–2015 with particular increase in extratemporal lobe surgeries (specifically significant for ≥7 years old) [105]. Due to lack of a large volume, it may become progressively difficult for an individual center to develop adequate expertise to offer surgical therapy for complex cases and may lead to higher perioperative mortality and lower rate to surgery after diagnostic evaluation [106,107].
5.3.2. Lack of referral arrangements among epilepsy centers
Referral arrangements between low- and high- volume epilepsy centers may mitigate this quality gap. However, strategic partnerships among low and high volume epilepsy centers are lacking [108]. The impact of a fragmented and disjointed referral network on cost, outcomes, patient satisfaction and epilepsy surgery rate remains unclear.
6. Conclusion
Underutilization of epilepsy surgery negatively impacts patient care across ages and geographies. Yet, access to safe surgical treatment for DRE to cure or mitigate the personal and societal burden. The etiologies for this quality gap remains complex and understudied. The biologic, behavioral and healthcare systems factors limiting patient access require urgent and magnified attention across research and practice environments.
Acknowledgement
The authors wish to acknowledge the member institutions of the PERC Epilepsy Surgery group for their continued support to increase the utilization and understanding of pediatric epilepsy surgery.
Disclosures
RA receives research support from NIH NINDS R01 NS115929 and Procter Foundation (Procter Scholar Award 2018-2021). The other authors declare no potential conflicts of interest with respect to the research, authorship, and publication of this article.
Funding
Debopam Samanta is supported by the Translational Research Institute (TRI), grant UL1 TR003107 through the National Center for Advancing Translational Sciences of the National Institutes of Health (NIH). The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
References
- [1].Kwan P, Arzimanoglou A, Berg AT, Brodie MJ, Allen Hauser W, Mathern G, et al. Definition of drug resistant epilepsy: Consensus proposal by the ad hoc task force of the ILAE commission on therapeutic strategies. Epilepsia 2009;51(6):1069–77. 10.1111/j.1528-1167.2009.02397.x. [DOI] [PubMed] [Google Scholar]
- [2].Vaughan KA, Lopez Ramos C, Buch VP, Mekary RA, Amundson JR, Shah M, et al. An estimation of global volume of surgically treatable epilepsy based on a systematic review and meta-analysis of epilepsy. J Neurosurg 2019;130 (4):1127–41. 10.3171/2018.3.jns171722. [DOI] [PubMed] [Google Scholar]
- [3].Wiebe S, Blume WT, Girvin JP, Eliasziw M. A randomized, controlled trial of surgery for temporal-lobe epilepsy. N Engl J Med 2001;345(5):311–8. [DOI] [PubMed] [Google Scholar]
- [4].Engel J, McDermott MP, Wiebe S, Langfitt JT, Stern JM, Dewar S, et al. Early surgical therapy for drug-resistant temporal lobe epilepsy: A randomized trial. JAMA 2012;307(9):922–30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [5].Dwivedi R, Ramanujam B, Chandra PS, Sapra S, Gulati S, Kalaivani M, et al. Surgery for drug-resistant epilepsy in children. N Engl J Med 2017;377 (17):1639–47. [DOI] [PubMed] [Google Scholar]
- [6].Helmstaedter C, Kurthen M, Lux S, Reuber M, Elger CE. Chronic epilepsy and cognition: A longitudinal study in temporal lobe epilepsy. Ann Neurol 2003;54(4):425–32. [DOI] [PubMed] [Google Scholar]
- [7].Sperling MR, Harris A, Nei M, Liporace JD, O’Connor MJ. Mortality after epilepsy surgery. Epilepsia 2005;46:49–53. [DOI] [PubMed] [Google Scholar]
- [8].Picot M, Jaussent A, Neveu D, Kahane P, Crespel A, Gelisse P, et al. Cost-effectiveness analysis of epilepsy surgery in a controlled cohort of adult patients with intractable partial epilepsy: A 5-year follow-up study. Epilepsia 2016;57(10):1669–79. [DOI] [PubMed] [Google Scholar]
- [9].Engel J, Wiebe S, French J, Sperling M, Williamson P, Spencer D, et al. Practice parameter: Temporal lobe and localized neocortical resections for epilepsy. Neurology 2003;60(4):538–47. 10.1212/01.wnl.0000055086.35806.2d. [DOI] [PubMed] [Google Scholar]
- [10].Cross JH, Jayakar P, Nordli D, Delalande O, Duchowny M, Wieser HG, et al. Proposed criteria for referral and evaluation of children for epilepsy surgery: Recommendations of the subcommission for pediatric epilepsy surgery. Epilepsia 2006;47(6):952–9. 10.1111/j.1528-1167.2006.00569.x. [DOI] [PubMed] [Google Scholar]
- [11].Ostendorf AP, In GS. Effect of epilepsy on families, communities, and society. Semin Pediatr Neurol; Elsevier 2017:340–7. [DOI] [PubMed] [Google Scholar]
- [12].Sridharan R Epidemiology of epilepsy. Curr Sci 2002:664–70. [Google Scholar]
- [13].Schiltz NK, Vaca GF. Epidemiologist’s view: Addressing the epilepsy surgery treatment gap with minimally-invasive techniques. Epilepsy Res 2018;142:179–81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [14].England MJ, Liverman CT, Schultz AM, Strawbridge LM. Epilepsy across the spectrum: Promoting health and understanding: A summary of the institute of medicine report. Epilepsy Behav 2012;25(2):266–76. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [15].Berg AT, Langfitt J, Shinnar S, Vickrey BG, Sperling MR, Walczak T, et al. How long does it take for partial epilepsy to become intractable? Neurology 2003;60(2):186–90. [DOI] [PubMed] [Google Scholar]
- [16].Haneef Z, Stern J, Dewar S, Engel J. Referral pattern for epilepsy surgery after evidence-based recommendations: A retrospective study. Neurology 2010;75 (8):699–704. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [17].Jehi L, Friedman D, Carlson C, Cascino G, Dewar S, Elger C, et al. The evolution of epilepsy surgery between 1991 and 2011 in nine major epilepsy centers across the United States, Germany, and Australia. Epilepsia 2015;56 (10):1526–33. Available from: https://pubmed.ncbi.nlm.nih.gov/26250432https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5082694/. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [18].Englot DJ, Ouyang D, Garcia PA, Barbaro NM, Chang EF. Epilepsy surgery trends in the united states, 1990–2008. Neurology 2012;78(16):1200–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [19].Burneo JG, Shariff SZ, Liu K, Leonard S, Saposnik G, Garg AX. Disparities in surgery among patients with intractable epilepsy in a universal health system. Neurology 2016;86(1):72–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [20].Lhatoo SD, Solomon JK, McEvoy AW, Kitchen ND, Shorvon SD, Sander JW. A prospective study of the requirement for and the provision of epilepsy surgery in the united kingdom. Epilepsia 2003;44(5):673–6. [DOI] [PubMed] [Google Scholar]
- [21].Bien CG, Raabe AL, Schramm J, Becker A, Urbach H, Elger CE. Trends in presurgical evaluation and surgical treatment of epilepsy at one centre from 1988–2009. J Neurol Neurosurg Psychiatry. 2012;84(1):54–61. 10.1136/jnnp-2011-301763. [DOI] [PubMed] [Google Scholar]
- [22].Cloppenborg T, May TW, Blümcke I, Grewe P, Hopf LJ, Kalbhenn T, et al. Trends in epilepsy surgery: Stable surgical numbers despite increasing presurgical volumes. J Neurol Neurosurg Psychiatry 2016;87 (12):1322–9. [DOI] [PubMed] [Google Scholar]
- [23].Vakharia VN, Duncan JS, Witt J, Elger CE, Staba R, Engel J Jr. Getting the best outcomes from epilepsy surgery. Ann Neurol 2018;83(4):676–90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [24].Hrazdil C, Roberts JI, Wiebe S, Sauro K, Vautour M, Hanson A, et al. Patient perceptions and barriers to epilepsy surgery: Evaluation in a large health region. Epilepsy Behav 2013;28(1):52–65. [DOI] [PubMed] [Google Scholar]
- [25].Ladino LD, Benjumea-Cuartas V, Diaz-Marin DM, Lopez-Gonzalez R, Orozco-Hernandez JP, Bedoya-Rodriguez P, et al. Patients’ perceptions of and attitudes towards epilepsy surgery: Mistaken concepts in colombia. Rev Neurol 2018;67(1):6–14. [PubMed] [Google Scholar]
- [26].Swarztrauber K, Dewar S, Engel J. Patient attitudes about treatments for intractable epilepsy. Epilepsy Behav 2003;4(1):19–25. 10.1016/s1525-5050(02)00687-x. [DOI] [PubMed] [Google Scholar]
- [27].Baca CB, Cheng EM, Spencer SS, Vassar S, Vickrey BG. Racial differences in patient expectations prior to resective epilepsy surgery. Epilepsy Behav 2009;15(4):452–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [28].Prus N, Grant AC. Patient beliefs about epilepsy and brain surgery in a multicultural urban population. Epilepsy Behav 2010;17(1):46–9. Available from: https://pubmed.ncbi.nlm.nih.gov/19910261https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2818497/. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [29].Anderson CT, Noble E, Mani R, Lawler K, Pollard JR. Epilepsy surgery: Factors that affect patient decision-making in choosing or deferring a procedure. Epilepsy Res Treat 2013;2013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [30].Choi H, Pargeon K, Bausell R, Wong JB, Mendiratta A, Bakken S. Temporal lobe epilepsy surgery: What do patients want to know? Epilepsy Behav 2011;22 (3):479–82. [DOI] [PubMed] [Google Scholar]
- [31].Rapport F, Shih P, Faris M, Nikpour A, Herkes G, Bleasel A, et al. Determinants of health and wellbeing in refractory epilepsy and surgery: The patient reported, ImpleMentation sciEnce (PRIME) model. Epilepsy Behav 2019;92:79–89. [DOI] [PubMed] [Google Scholar]
- [32].Prus N, Grant AC. Patient beliefs about epilepsy and brain surgery in a multicultural urban population. Epilepsy Behav 2010;17(1):46–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [33].Erba G, Messina P, Pupillo E, Beghi E, Group TOP. Acceptance of epilepsy surgery in the pediatric age—what the parents think and what the doctors can do. Epilepsy Behav 2013;29(1):112–20. [DOI] [PubMed] [Google Scholar]
- [34].Hakimi AS, Spanaki MV, Schuh LA, Smith BJ, Schultz L. A survey of neurologists’ views on epilepsy surgery and medically refractory epilepsy. Epilepsy Behav 2008;13(1):96–101. 10.1016/j.yebeh.2008.02.003. [DOI] [PubMed] [Google Scholar]
- [35].Hall-Patch L, Gayatri N, Ferrie C, Morrall, Matthew CHJ. Clinical reasoning and investigations for resective surgery for medically refractory epilepsies in children. Epilepsy Behav 2012;23(4):442–6. 10.1016/j.yebeh.2012.01.025. [DOI] [PubMed] [Google Scholar]
- [36].Kumlien E, Mattsson P. Attitudes towards epilepsy surgery: A nationwide survey among Swedish neurologists. Seizure 2010;19(4):253–5. 10.1016/j.seizure.2010.02.001. [DOI] [PubMed] [Google Scholar]
- [37].Roberts JI, Hrazdil C, Wiebe S, Sauro K, Vautour M, Wiebe N, et al. Neurologists’ knowledge of and attitudes toward epilepsy surgery: A national survey. Neurology 2015;84(2):159–66. Available from: https://pubmed.ncbi.nlm.nih.gov/25503624https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4336084/. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [38].Uijl SG, Leijten FSS, Moons KGM, Veltman Ellen PHM, Ferrier CH, van Donselaar CA. Epilepsy surgery can help many more adult patients with intractable seizures. Epilepsy Res 2012;101(3):210–6. 10.1016/j.eplepsyres.2012.04.002. [DOI] [PubMed] [Google Scholar]
- [39].Cothros N, Burneo JG, Steven DA. Knowledge and attitudes about epilepsy surgery among family doctors in Ontario. Can J Neurol Sci 2016;43 (5):672–1627. 10.1017/cjn.2016.277. [DOI] [PubMed] [Google Scholar]
- [40].Erba G, Moja L, Beghi E, Messina P, Pupillo E. Barriers toward epilepsy surgery. A survey among practicing neurologists. Epilepsia 2011;53(1):35–43. 10.1111/j.1528-1167.2011.03282.x. [DOI] [PubMed] [Google Scholar]
- [41].Erba G, Moja L, Beghi E, Messina P, Pupillo E. Barriers toward epilepsy surgery. A survey among practicing neurologists. Epilepsia 2012;53(1):35–43. [DOI] [PubMed] [Google Scholar]
- [42].Harrison MB, Légaré F, Graham ID, Fervers B. Adapting clinical practice guidelines to local context and assessing barriers to their use. CMAJ 2010;182 (2):E78–84. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [43].Sheehan J, Starke RM, Pouratian N, Litvack Z. Identification of knowledge gaps in neurosurgery using a validated self-assessment examination: differences between general and spinal neurosurgeons. World Neurosurg 2013;80(5): e27–31. [DOI] [PubMed] [Google Scholar]
- [44].Kumlien E, Mattsson P. Attitudes towards epilepsy surgery: A nationwide survey among Swedish neurologists. Seizure 2010;19(4):253–5. [DOI] [PubMed] [Google Scholar]
- [45].Pestana Knight EM, Schiltz NK, Bakaki PM, Koroukian SM, Lhatoo SD, Kaiboriboon K. Increasing utilization of pediatric epilepsy surgery in the united states between 1997 and 2009. Epilepsia 2015;56(3):375–81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [46].Freitag H, Tuxhorn I. Cognitive function in preschool children after epilepsy surgery: Rationale for early intervention. Epilepsia 2005;46(4):561–7. [DOI] [PubMed] [Google Scholar]
- [47].Prideaux L, Barton S, Maixner W, Harvey AS. Potential delays in referral and assessment for epilepsy surgery in children with drug-resistant, early-onset epilepsy. Epilepsy Res 2018;143:20–6. 10.1016/j.eplepsyres.2018.04.001. [DOI] [PubMed] [Google Scholar]
- [48].Pindrik J, Hoang N, Smith L, Halverson M, Wojnaroski M, McNally K, et al. Preoperative evaluation and surgical management of infants and toddlers with drug-resistant epilepsy. Neurosurg Focus 2018;45(3):E3. [DOI] [PubMed] [Google Scholar]
- [49].Daghistani R, Widjaja E. Role of MRI in patient selection for surgical treatment of intractable epilepsy in infancy. Brain Dev 2013;35(8):697–705. [DOI] [PubMed] [Google Scholar]
- [50].Wyllie E, Comair YG, Kotagal P, Raja S, Ruggieri P. Epilepsy surgery in infants. Epilepsia 1996;37(7):625–37. [DOI] [PubMed] [Google Scholar]
- [51].Taussig D, Dorfmüller G, Fohlen M, Jalin C, Bulteau C, Ferrand-Sorbets S, et al. Invasive explorations in children younger than 3 years. Seizure 2012;21 (8):631–8. [DOI] [PubMed] [Google Scholar]
- [52].May TW, Pfäfflin M, Brandt C, Füratsch N, Schmitz B, Wandschneider B, et al. Epilepsy in the elderly: Restrictions, fears, and quality of life. Acta Neurol Scand 2015;131(3):176–86. [DOI] [PubMed] [Google Scholar]
- [53].Martin R, Vogtle L, Gilliam F, Faught E. What are the concerns of older adults living with epilepsy? Epilepsy Behav 2005;7(2):297–300. [DOI] [PubMed] [Google Scholar]
- [54].Engel J Jr Update on surgical treatment of the epilepsies. Clin Exp Neurol 1992;29:32. [PubMed] [Google Scholar]
- [55].Punia V, Abdelkader A, Busch RM, Gonzalez-Martinez J, Bingaman W, Najm I, et al. Time to push the age limit: Epilepsy surgery in patients 60 years or older. Epilepsia Open 2018;3(1):73–80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [56].Sen A, Jette N, Husain M, Sander JW. Epilepsy in older people. Lancet 2020;395(10225):735–48. [DOI] [PubMed] [Google Scholar]
- [57].Maragkos GA, Geropoulos G, Kechagias K, Ziogas IA, Mylonas KS. Quality of life after epilepsy surgery in children: A systematic review and meta-analysis. Neurosurgery 2019;85(6):741–9. [DOI] [PubMed] [Google Scholar]
- [58].Delev D, Hakvoort K, Grote A, Neuloh G, Clusmann H, von Lehe M. Quality of life in elderly patients after surgery for drug-resistant epilepsy–The impact of seizure outcome, neurological deficits and anxiety. Epilepsy Behav 2020;112:107410. [DOI] [PubMed] [Google Scholar]
- [59].Grande KM, Ihnen SK, Arya R. Electrical stimulation mapping of brain function: A comparison of subdural electrodes and stereo-EEG. Front Hum Neurosci 2020;14:538. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [60].Cuisenier P, Testud B, Minotti L, Tiali SEB, Martineau L, Job A, et al. Relationship between direct cortical stimulation and induced high-frequency activity for language mapping during SEEG recording. J Neurosurg 2020;1(aop):1–11. [DOI] [PubMed] [Google Scholar]
- [61].Jayakar P, Jayakar A, Libenson M, Arzimanoglou A, Rydenhag B, Cross JH, et al. Epilepsy surgery near or in eloquent cortex in children—Practice patterns and recommendations for minimizing and reporting deficits. Epilepsia 2018;59 (8):1484–91. [DOI] [PubMed] [Google Scholar]
- [62].Scheffer IE, Berkovic S, Capovilla G, Connolly MB, French J, Guilhoto L, et al. ILAE classification of the epilepsies: Position paper of the ILAE commission for classification and terminology. Epilepsia 2017;58(4):512–21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [63].Asadi-Pooya AA, Emami M, Ashjazadeh N, Nikseresht A, Shariat A, Petramfar P, et al. Reasons for uncontrolled seizures in adults; the impact of pseudointractability. Seizure 2013;22(4):271–4. [DOI] [PubMed] [Google Scholar]
- [64].Elwan S, Alexopoulos A, Silveira DC, Kotagal P. Lateralizing and localizing value of seizure semiology: Comparison with scalp EEG, MRI and PET in patients successfully treated with resective epilepsy surgery. Seizure 2018;61:203–8. [DOI] [PubMed] [Google Scholar]
- [65].Asadi-Pooya AA. Lateralizing and localizing findings in focal epilepsies: A concise review. J Neurol Neurophysiol 2012;2:17–9. [Google Scholar]
- [66].Kim DW, Lee SK, Moon H, Jung K, Chu K, Chung C. Surgical treatment of nonlesional neocortical epilepsy: Long-term longitudinal study. JAMA Neurol 2017;74(3):324–31. [DOI] [PubMed] [Google Scholar]
- [67].Kanner AM, Byrne R, Chicharro A, Wuu J, Frey M. A lifetime psychiatric history predicts a worse seizure outcome following temporal lobectomy. Neurology 2009;72(9):793–9. [DOI] [PubMed] [Google Scholar]
- [68].Qualmann KJ, Spaeth CG, Myers MF, Horn PS, Holland K, Mangano FT, et al. Pediatric epilepsy surgery: The prognostic value of central nervous system comorbidities in patients and their families. J Child Neurol 2017;32 (5):467–74. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [69].Baca CB, Pieters HC, Iwaki TJ, Mathern GW, Vickrey BG. A journey around the world: Parent narratives of the journey to pediatric resective epilepsy surgery and beyond. Epilepsia. 2015;56(6):822–32. Available from: https://pubmed.ncbi.nlm.nih.gov/25894906https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4457674/. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [70].Pieters HC, Iwaki T, Vickrey BG, Mathern GW, Baca CB. “It was five years of hell”: Parental experiences of navigating and processing the slow and arduous time to pediatric resective epilepsy surgery. Epilepsy Behav 2016;62:276–84. 10.1016/j.yebeh.2016.07.019. [DOI] [PubMed] [Google Scholar]
- [71].Hoffman HJ, LaVerda NL, Young HA, Levine PH, Alexander LM, Brem R, et al. Patient navigation significantly reduces delays in breast cancer diagnosis in the district of columbia. Cancer Epidemiol Biomarkers Prev 2012;21 (10):1655–63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [72].Altalib HH, Fenton BT, Cheung K, Pugh MJV, Bates J, Valente TW, et al. Care coordination in epilepsy: Measuring neurologists’ connectivity using social network analysis. Epilepsy Behav 2017;73:31–5. [DOI] [PubMed] [Google Scholar]
- [73].De Flon P, Kumlien E, Reuterwall C, Mattsson P. Empirical evidence of underutilization of referrals for epilepsy surgery evaluation. Eur J Neurol 2009;17(4):619–25. 10.1111/j.1468-1331.2009.02891.x. [DOI] [PubMed] [Google Scholar]
- [74].Benbadis SR, Heriaud L, Tatum IV WO, Vale FL. Epilepsy surgery, delays and referral patterns—are all your epilepsy patients controlled? Seizure 2003;12 (3):167–70. [DOI] [PubMed] [Google Scholar]
- [75].Scott RA, Lhatoo SD, Sander JW. The treatment of epilepsy in developing countries: Where do we go from here? Bull World Health Organ 2001;79:344–51. [PMC free article] [PubMed] [Google Scholar]
- [76].Martínez-Juárez IE, Funes B, Moreno-Castellanos JC, Bribiesca-Contreras E, Martínez-Bustos V, Zertuche-Ortuño L, et al. A comparison of waiting times for assessment and epilepsy surgery between a canadian and a mexican referral center. Epilepsia open 2017;2(4):453–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [77].Jędrzejczak J, Marusic P, Haldre S, Majkowska-Zwolińska B, Bojinova-Tchamova V, Mameniskiene R, et al. Current status of epilepsy health care for adult patients from central and eastern european union Countries—A survey of members of the central europe epilepsy experts working group. Seizure 2013;22(6):452–6. [DOI] [PubMed] [Google Scholar]
- [78].Mumford V, Rapport F, Shih P, Mitchell R, Bleasel A, Nikpour A, et al. Promoting faster pathways to surgery: A clinical audit of patients with refractory epilepsy. BMC Neurol. 2019;19(1):29. Available from: https://pubmed.ncbi.nlm.nih.gov/30782132https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6381714/. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [79].Drees C, Sillau S, Brown M, Abosch A. Preoperative evaluation for epilepsy surgery: Process improvement. Neurol Clin Pract. 2017;7(3):205–13. Available from: https://pubmed.ncbi.nlm.nih.gov/30107011https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6081968/. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [80].Burneo JG, Jette N, Theodore W, Begley C, Parko K, Thurman DJ, et al. Disparities in epilepsy: Report of a systematic review by the North American commission of the international league against epilepsy. Epilepsia. 2009;50 (10):2285–95. Available from: https://pubmed.ncbi.nlm.nih.gov/19732134https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3181115/. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [81].Burneo JG, Black L, Knowlton RC, Faught E, Morawetz R, Kuzniecky RI. Racial disparities in the use of surgical treatment for intractable temporal lobe epilepsy. Neurology 2005;64(1):50–4. 10.1212/01.wnl.0000150829.89586.25. [DOI] [PubMed] [Google Scholar]
- [82].Sánchez Fernández I, Stephen C, Loddenkemper T. Disparities in epilepsy surgery in the United States of America. J Neurol 2017;264(8):1735–45. 10.1007/s00415-017-8560-6. [DOI] [PubMed] [Google Scholar]
- [83].Jetté N, Quan H, Faris P, Dean S, Li B, Fong A, et al. Health resource use in epilepsy: Significant disparities by age, gender, and aboriginal status. Epilepsia 2008;49(4):586–93. [DOI] [PubMed] [Google Scholar]
- [84].Szaflarski M Social determinants of health in epilepsy. Epilepsy Behav 2014;41:283–9. [DOI] [PubMed] [Google Scholar]
- [85].Berg AT, Baca CB, Rychlik K, Vickrey BG, Caplan R, Testa FM, et al. Determinants of social outcomes in adults with childhood-onset epilepsy. Pediatrics 2016;137(4):e20153944. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [86].Griggs JJ, Engel J. No title. Epilepsy surgery and the racial divide. 2005. [DOI] [PubMed] [Google Scholar]
- [87].Gehlert S, DiFrancesco A, Chang C. Black-white differences in the psychosocial outcomes of epilepsy. Epilepsy Res 2000;42(1):63–73. [DOI] [PubMed] [Google Scholar]
- [88].Nathan CL, Gutierrez C. FACETS of health disparities in epilepsy surgery and gaps that need to be addressed. Neurol Clin Pract 2018;8(4):340–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [89].McClelland S, Curran CC, Davey CS, Okuyemi KS. Intractable pediatric temporal lobe epilepsy in the United States: Examination of race, age, sex, and insurance status as factors predicting receipt of resective treatment. J Neurosurg Pediatr 2007;107(6):469–73. 10.3171/ped-07/12/469. [DOI] [PubMed] [Google Scholar]
- [90].Privitera M Large clinical trials in epilepsy: Funding by the NIH versus pharmaceutical industry. Epilepsy Res 2006;68(1):52–6. 10.1016/j.eplepsyres.2005.09.020. [DOI] [PubMed] [Google Scholar]
- [91].Solli E, Colwell NA, Say I, Houston R, Johal AS, Pak J, et al. Deciphering the surgical treatment gap for drugâ resistant epilepsy (DRE): A literature review. Epilepsia 2020;61(7):1352–64. [DOI] [PubMed] [Google Scholar]
- [92].Meador KJ, French J, Loring DW, Pennell PB. Disparities in NIH funding for epilepsy research. Neurology 2011;77(13):1305–7. Available from: https://pubmed.ncbi.nlm.nih.gov/21947534https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3265048/. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [93].AES calls for more epilepsy research funding American Epilepsy Society.
- [94].ClinicalTrials.gov [homepage on the Internet]. [cited 12/23/2020]. Available from: https://www.clinicaltrials.gov/ct2/results?cond=VNS&term=&cntry=&state=&city=&dist=.
- [95].Winston GP, Micallef C, Kendell BE, Bartlett PA, Williams EJ, Burdett JL, et al. The value of repeat neuroimaging for epilepsy at a tertiary referral centre: 16 years of experience. Epilepsy Res 2013;105(3):349–55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [96].Knake S, Triantafyllou C, Wald LL, Wiggins G, Kirk GP, Larsson PG, et al. 3T phased array MRI improves the presurgical evaluation in focal epilepsies: A prospective study. Neurology 2005;65(7):1026–31. [DOI] [PubMed] [Google Scholar]
- [97].Von Oertzen J, Urbach H, Jungbluth S, Kurthen M, Reuber M, Fernandez G, et al. Standard magnetic resonance imaging is inadequate for patients with refractory focal epilepsy. J Neurol Neurosurg Psychiatry 2002;73 (6):643–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [98].Jayakar P, Gaillard WD, Tripathi M, Libenson MH, Mathern GW, Cross JH. Diagnostic test utilization in evaluation for resective epilepsy surgery in children. Epilepsia 2014;55(4):507–18. 10.1111/epi.12544. [DOI] [PubMed] [Google Scholar]
- [99].Hinde S, Soares M, Burch J, Marson A, Woolacott N, Palmer S. The added clinical and economic value of diagnostic testing for epilepsy surgery. Epilepsy Res 2014;108(4):775–81. Available from: https://pubmed.ncbi.nlm.nih.gov/24630045https://www.ncbi.nlm.nih.gov/pmc/articles/PMC-4000270/. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [100].Haut SR, Berg AT, Shinnar S, Cohen HW, Bazil CW, Sperling MR, et al. Interrater reliability among epilepsy centers: Multicenter study of epilepsy surgery. Epilepsia 2002;43(11):1396–401. [DOI] [PubMed] [Google Scholar]
- [101].Englot DJ. A modern epilepsy surgery treatment algorithm: Incorporating traditional and emerging technologies. Epilepsy Behav 2018;80:68–74. Available from: https://pubmed.ncbi.nlm.nih.gov/29414561https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5845806/. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [102].Tandon N, Tong BA, Friedman ER, Johnson JA, Von Allmen G, Thomas MS, et al. Analysis of morbidity and outcomes associated with use of subdural grids vs stereoelectroencephalography in patients with intractable epilepsy. JAMA Neurol 2019;76(6):672–81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [103].Kaiboriboon K, Malkhachroum AM, Zrik A, Daif A, Schiltz NM, Labiner DM, et al. Epilepsy surgery in the United States: Analysis of data from the national association of epilepsy centers. Epilepsy Res 2015;116:105–9. [DOI] [PubMed] [Google Scholar]
- [104].Barba C, Specchio N, Guerrini R, Tassi L, De Masi S, Cardinale F, et al. Increasing volume and complexity of pediatric epilepsy surgery with stable seizure outcome between 2008 and 2014: A nationwide multicenter study. Epilepsy Behav 2017;75:151–7. [DOI] [PubMed] [Google Scholar]
- [105].Barba C, Cross JH, Braun K, Cossu M, Klotz KA, De Masi S, et al. Trends in pediatric epilepsy surgery in Europe between 2008 and 2015: Country-, center-, and age-specific variation. Epilepsia 2020;61(2):216–27. [DOI] [PubMed] [Google Scholar]
- [106].Englot DJ, Ouyang D, Wang DD, Rolston JD, Garcia PA, Chang EF. Relationship between hospital surgical volume, lobectomy rates, and adverse perioperative events at US epilepsy centers. J Neurosurg 2013;118(1):169–74. [DOI] [PubMed] [Google Scholar]
- [107].Rolston JD, Englot DJ, Knowlton RC, Chang EF. Rate and complications of adult epilepsy surgery in North America: Analysis of multiple databases. Epilepsy Res 2016;124:55–62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [108].Vadera S, Chan AY, Mnatsankanyan L, Sazgar M, Sen-Gupta I, Lin J, et al. Strategic hospital partnerships: Improved access to care and increased epilepsy surgical volume. Neurosurg Focus 2018;44(5):E9. 10.3171/2018.1.focus17683. [DOI] [PubMed] [Google Scholar]