

Abstract
Objectives
To identify studies evaluating the epidemiology of recurrent respiratory papillomatosis (RRP), including patient demographics, human papillomavirus (HPV) immunology, clinical course, surgical and medical treatments, and psychosocial factors.
Methods
A systematic literature search through PubMed was performed to identify studies evaluating the epidemiological factors associated with RRP. All studies were screened through a priori selection criteria using the titles and abstracts.
Results
A total of 208 studies were identified, of which 54 met eligibility criteria and were included in the review.
Conclusions
RRP is a rare disease most commonly caused by HPV 6 and 11. It is characterized by recurring benign papillomatous lesions in the respiratory tract, particularly the larynx. Existing evidence about disease risk factors is limited but includes both maternal HPV infection and patient smoking and sexual behaviors. Disease management involves a combination of routine surgical and medical treatment. Surgical techniques include CO2‐laser, sharp dissection, coblation, microdebridement, and photoangiolytic laser. Medical treatments which have been found to facilitate disease control off‐label include interferon‐alpha (IFN‐α), indole‐3‐carbinol, acyclovir, bevacizumab, retinoids, and the Gardasil and mumps vaccines. Many patients suffer from additional psychosocial challenges related to their diagnosis. Current disease knowledge remains limited, and more robust controlled trials about risk factors, medical therapies, and surgical options are needed.
Level of Evidence
5.
Keywords: epidemiology, recurrent respiratory papillomatosis

Recurrent respiratory papillomatosis (RRP) is a rare disease caused by human papillomavirus (HPV) characterized by recurring benign papillomatous lesions in the respiratory tract and are often refractory to treatment. The aim of this review is to identify studies evaluating the epidemiology of recurrent respiratory papillomatosis, including patient demographics, human papillomavirus immunology, clinical course, surgical and medical treatments, and psychosocial factors.
1. INTRODUCTION
Recurrent respiratory papillomatosis (RRP) is a rare disease caused by human papillomavirus (HPV). HPV is a double‐stranded DNA virus and member of the papillomaviridae family. It is characterized by recurring benign papillomatous lesions in the respiratory tract and is often refractory to treatment. While the lesions most commonly present in the larynx, they have the potential to spread throughout the respiratory tract and undergo malignant transformation with rates ranging from 2% to 4%. 1 The majority of cases are caused by HPV 6 and 11 but can also be associated with strains 16, 18, 31, and 33. 2
Patients with RRP present clinically with voice changes, difficulty breathing, and/or stridor. 2 Typical management includes a combination of surgical excisions and systemic and intralesional therapies. Due to the non‐remitting nature of RRP, patients undergo an average of 4.4 surgeries annually to maintain control of papillomas. 3
While the clinical presentation and severity of RRP has been well characterized, epidemiological factors and efficacy of treatment options have not. The aim of this review is to critically evaluate the risk factors associated with RRP including patient demographics, HPV immunological characteristics, clinical course, and psychosocial factors. Additionally, we provide a summary and appraisal of the current treatments to serve as a framework to optimize patient outcomes.
2. METHODS
2.1. Literature acquisition and synthesis
A systematic literature search through PubMed was performed on May 1, 2020 to identify studies evaluating the epidemiological factors associated with RRP. Using free‐text we searched the terms recurrent respiratory papillomatosis epidemiology, recurrent respiratory papillomatosis treatment, and recurrent respiratory papillomatosis risk factors. All studies were screened through a priori selection criteria using the titles and abstracts. Inclusion criteria included the following: report of disease severity outcomes or quality of life outcomes, discussion of surgical and medical treatment options, patient demographic information, HPV details, disease‐related psychosocial factors, published works after the year 1987. Exclusion criteria included the following: studies that re‐reported treatment outcomes and patient demographics from the same cohort. For those studies that were excluded, due to re‐reporting the updated reports were included in this review. The literature search yielded 208 studies of which 54 met eligibility criteria and were included in this review. Data was extracted independently from the included reports. The quality of each study was evaluated by two of the authors independently. Notably, data regarding many of the novel surgical and medical treatments are limited by lack of large controlled trials; thus this review aims to summarize and reflect the existing literature while noting the need for future clinical studies pertaining to RRP treatments. This study used existing literature and was therefore exempt from institutional review board review. No review protocol exists for this study.
3. EPIDEMIOLOGICAL FACTORS
3.1. Patient demographics
RRP affects both adults and children and at times involves a life‐long disease burden. RRP is estimated to affect 1.8 per 100 000 adults and 4.3 per 100 000 children in the United States with a balanced sex ratio. 2 , 4 The average age at diagnosis for juvenile onset RRP (JORRP) is 5 years old while adult onset RRP (AORRP) is 37. 4 , 5 RRP is typically considered juvenile onset when it is acquired at birth from mother‐to‐child transmission, while adult onset RRP typically involves sexual transmission of HPV. 6
The definitive risk factors for RRP remain unclear; however, both maternal and patient‐specific factors may play a role in disease contraction. Several known risk factors include maternal HPV infection at time of birth, vaginal delivery, teenage mother, and first born child. 7 , 8 , 9 In addition to mother‐to‐child transmission during birth, RRP may be acquired through sexual contact. Compared with disease‐free controls, patients with RRP have a significantly higher median number of lifetime sexual partners. 7 However, additional studies investigating sexual behavior as a risk factor have mixed findings. 8 Sexual contact may contribute to viral transmission from person to person, yet conclusive evidence is lacking.
Smoking may also contribute to RRP incidence and severity. A study of 113 patients found that smoking habits were correlated with disease severity, location, age of onset, number of treatments, and clinical outcomes. 10 Surprisingly, among patients with RRP, smoking status is independent of risk of malignant transformation. 11 , 12 Further research is warranted to understand transmutability and associated risk factors, such as sexual behavior and smoking. With a more thorough understanding of the disease process, clinicians can better educate their patients regarding modifiable and nonmodifiable risk factors.
3.2. Clinical presentation and diagnosis
RRP has a wide range of clinical presentations. It most commonly presents with hoarseness, mild respiratory distress, loss of voice, mouth breathing, foreign body sensation, stridor, and snoring. 7 , 13 , 14 , 15 Interestingly, dysphonia is more commonly seen in adults than children. 14 The most common site for lesions are the true vocal cords followed by infrahyoid supraglottis, anterior commissure, subglottis, suprahyoid supraglottis, trachea, piriform sinus, and oropharynx. 10 Poor innate immunity plus immunologic tolerance to HPV within the larynx contribute to its typical respiratory tract distribution. 16 A study found that new lesions occur adjacent to preexisting lesions between 66% and 83% of the time, irrespective of initial lesion site. Additionally, HPV can be detected on biopsy of non‐papillomatous areas of the larynx of patients with a history of RRP suggesting latent infection and thus explains the propensity for lesions to recur. 17
In addition to clinical symptoms, otolaryngologists rely on key endoscopic findings to establish the diagnosis of RRP. Typical findings include multiple, fragile grape‐like clusters (Figure 1). Once identified and biopsied, histologic examination of the papillomas reveals projections of neoplastic and squamous epithelium overlying a fibrovascular stromal core. Despite these classic findings, variability and intermittency of symptoms may unfortunately postpone the diagnosis and delay treatment. 18
FIGURE 1.
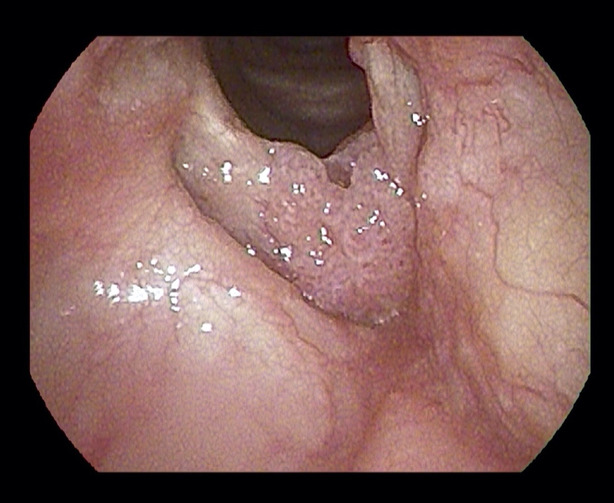
Endoscopic view of the larynx showing confluence of lesions on both vocal folds and demonstrates grape like clustering of lesion
Though no uniform classification tool exists, several methods are currently used to classify vocal symptoms associated with RRP. One such method is the Voice Handicap Index (VHI), a validated tool to assess functional, physical, and emotional degree of vocal impairment. 19 A higher VHI score corresponds to a worse voice‐related quality of life. 20 The Derkay score is an additional clinical tool, which classifies the disease by extent of anatomic involvement of the lesions. 15 , 21 Derkay score tends to vary by age of disease onset with patients with JORRP having a higher mean score than those with AORRP. 15 Furthermore, higher Derkay score is associated with increased voice handicap rated by VHI score in adult patients with RRP. 21 No relationship between Derkay score and VHI has been reported in existing literature in the JORRP population.
Younger age at diagnosis and increased laryngeal involvement at the time of first endoscopy are additional poor prognostic factors. 15 , 22 A 2019 cohort study found that patients with a more aggressive disease were diagnosed a median of 7.4 years earlier than patients with less severe disease. 13 Additional complications of early age at diagnosis include increased risk of disease spread within the distal respiratory tract and increased recurrence rates. 23 The aforementioned clinical, endoscopic, histologic, and demographic information help guide the diagnosis and treatment of RRP.
3.3. HPV characteristics
The benign neoplasms of RRP are caused by infection of the respiratory tract epithelium by HPV. RRP is most commonly caused by HPV type 6 and 11 but also caused by rarer types 16, 18, 31, and 33. 2 Expression of HPV‐encoded oncogenes E6 and E7 potentiate viral proliferation and plays an important role in RRP pathogenesis.
Classically, HPV 11 has been associated with more aggressive disease compared with HPV 6; however, additional data supporting this are discordant and limited. 24 One study found that HPV 11 was associated with a shorter interval between surgeries than HPV 6 only in the setting of JORRP but not AORRP. 13 The aforementioned evidence points to the fact that AORRP and JORRP are not synonymous, and further research is required to better understand the differences in disease pathogenesis and management. It has been proposed that the variability of disease severity by HPV type and patient age may be explained by the host's immunologic ability to fight different HPV oncogenes. A study found that patients infected with HPV 11 had higher levels of E6 and E7 than patients with HPV 6. 22 Additionally, patients diagnosed before the age of 24 months had higher levels of E7 expression independent of HPV type. 22 This suggests that HPV genotyping and oncogenic assays of all patients with RRP can serve as both diagnostic and prognostic tools.
It is estimated that 1% of the general population has commensal HPV 6 and 11 DNA in their larynx, yet only a small fraction of those exposed develop RRP due to variations in immune susceptibility. 25 Impaired natural killer (NK) cell function accounts for this difference in part. 16 , 25 Additionally, patients with RRP have an increased number of CD4+ T cells that express Th2‐like cytokines. Increased levels of Th2‐like cytokines suppress production of interferon‐gamma (IFN‐γ), which in turn decreases HPV clearance. 16 Infected laryngeal cells overexpress epidermal growth factor receptor (EGFR), which causes a prolific inflammatory response and papilloma formation. It is evident that both the immune response of the laryngeal tissue and immune susceptibility of the host may contribute laryngeal papilloma formation.
The immunologic response of the larynx plays a critical role in acquisition of HPV infection and papilloma formation. Its location, at the junction between the respiratory and gastrointestinal tracts, makes the larynx an important checkpoint to mediate both immune tolerance and inflammatory activation in response to infiltrating pathogens. The normal laryngeal immune response to HPV involves antigen presenting cells (APCs), Langerhans cells, macrophages, T cells, and immunoglobulins. Dysregulation of this normal immune response is central to the pathogenesis of RRP. Future directions for research surrounding treatment of RRP include immune targeted therapies.
3.4. Surgical treatments
No definitive cure for RRP exists; however typical management includes both surgical and medical therapy to treat papilloma recurrences. On average, patients with RRP undergo about 4 surgeries per year. 3 , 26 Common surgical modalities include CO2‐laser, sharp dissection, and microdebridement. 22 The goals of surgery include removal of papillomas while preserving healthy respiratory tract tissue.
Though there is no gold standard treatment for RRP, one study attempted to characterize the benefits and risks of various surgical techniques including cold instruments, microdebridement, and laser. 27 While microdebridement offers precise resection of papillomas, undesired post‐operative sequelae include vocal cord injury and scarring. An additional study investigated the use of coblation and microdebridement for treatment of RRP. Both microdebridement and coblation result in satisfactory recurrence rates and improved voice quality. Microdebridement causes less thermal damage than coblation, however, coblation typically has less bleeding during a procedure due to its thermal coagulation of small vessels. 14
Carbon dioxide (CO2) laser therapy is another treatment for RRP. Through precise vaporization of diseased tissue, the laser helps minimize disease recurrence. One study found that 17% of patients treated with carbon dioxide laser every 2 months until remission was achieved were disease‐free for 5 years following treatment; however, this could be also simply be due to spontaneous remission and requires further investigation. 1 Disadvantages of laser therapy include the cost and maintenance of the laser, rare risk of fire, and complications such as glottic anterior commissure synechia and subglottic stenosis. 1 , 28 In summary, the CO2‐laser has some drawbacks but has been used successfully for many years to lessen the burden of HPV lesions.
Photodynamic therapy (PDT) is also utilized for management of RRP. Unlike traditional surgical debridement, PDT induces slow necrosis of affected tissue causing release of HPV‐related proteins, such as E6 and E7. This provides an opportunity for antigen presentation and short‐term immunologic viral clearance mediated by IL‐10 and IFN‐γ. 29 Unfortunately, the dye used in PDT is not virus‐specific and thus has potential to cause damage to nearby healthy laryngeal tissue.
Photoangiolytic laser is a unique, office‐based procedure which provides safe and effective treatment for RRP. The most commonly utilized photoangiolytic laser is the KTP (potassium titanyl phosphate) laser which disrupts the microcirculation of the papillomas causing involution of diseased tissue. The laser allows for reasonable surgical precision and versatility and has been used in combination with other drugs such as bevacizumab, a synergistic anti‐angiogenic agent. 30 In addition to its favorable clinical outcomes, the KTP laser offers increased patient convenience since it can be performed in office, without general anesthesia thus saving both money and operating room time.
Though there are advantages and disadvantages to each surgical modality, most patients continue to experience relapsing disease and require trial of many treatment options during their clinical course. While RRP is usually a life‐long disease, most patients achieve remission, or disease‐free intervals, throughout the course of the disease. Surgical intervention helps increase instances of disease remission and decrease unwanted voice and respiratory symptoms. 31
3.5. Systemic and intralesional treatments
In addition to surgical treatment, systemic and intralesional medical therapies are known to reduce papilloma recurrences. Some of these medications include interferon‐alpha (IFN‐α), indole‐3‐carbinol (I3C), acyclovir, retinoids, and cidofovir. 22 Though many of these medical treatments help optimize disease control, it is important to note that none of the aforementioned medications have FDA approval for the treatment of RRP. The most common intralesional medication used is cidofovir.
RRP has a relapsing remitting pattern, so medications that decrease surgery frequency and extend disease‐free intervals are desired. A randomized controlled trial (RCT) of adjuvant IFN‐α found a significantly higher proportion of patients achieving remission and that the rate of papilloma growth decreased in the first 6 months after treatment compared with controls, but that this benefit was not sustained long‐term. 32 Though IFN‐α helps with disease control, there are many undesired side effects including fever, fatigue, headache, elevated serum aspartate aminotransferase, and nausea. 33 Additional limitations of IFN‐α use include a lack of achieving a long remission phase, no standard dosing regimen, and high cost.
I3C is another medication commonly given to patients as an adjunctive therapy. Through alteration of estrogen metabolism, I3C helps decrease unwanted DNA synthesis and reduces hyperproliferation of papillomatous epithelial cells. 34 A clinical study of the long‐term outcomes of I3C treatment found that 33% of patients experienced complete papilloma remission and an additional 30% had marked reduction in papilloma growth. 35 Some patients elect to take 3,3′‐diindolylmethane (DIM), the main precursor of I3C, to achieve the same effects. 36 I3C and DIM are relatively safe drugs with low rates of adverse events and acceptable patient tolerance. 37
Cidofovir, a cytosine nucleotide analog, is an antiviral agent with Food and Drug Administration (FDA) approval to treat cytomegalovirus retinopathy in patients with acquired immunodeficiency syndrome (AIDS). It has gained recognition as a viable off‐label intralesional treatment for patients with RRP; however, RCTs investigating its utility in this setting are limited by small sample size and lack of long‐term follow up. 20 , 38 , 39 There is a lack of consensus regarding optimal initiation of cidofovir; however, one recent study found that most providers begin cidofovir treatment in patients who require six or more surgeries per year or for those who require increasingly frequent surgeries. 40 Current studies have shown that cidofovir can increase the intersurgical interval and decrease the number of required surgeries per year. 41 Importantly, cidofovir has limited utility in pregnant women as it is a pregnancy category C drug due to potential teratogenicity and testicular toxicity. 42 , 43 Early reports concerned the possibility of malignant transformation of papillomas in patients receiving the drug, but these have not been identified in other more controlled studies. 44 Nonetheless, cidofovir remains an accepted treatment for RRP due to a lack of adequate alternative intralesional options and its relative success at controlling disease flares.
Bevacizumab, a monoclonal antibody which inhibits VEGF, has recently been studied as a potential treatment for RRP. While clinical trials are limited, one case report found that sublesional injections of bevacizumab significantly increase the duration between required surgical debridements. 45 A larger case series reported similar results with systemic bevacizumab and found that all patients had a significant increase in the surgical interval between papilloma excisions and some patients no longer required any debridements after treatment. 46 Its low side effect profile makes bevacizumab a promising drug, yet its expense is a significant downside.
In addition to the aforementioned systemic and intralesional medications, acyclovir holds promise in the treatment of RRP. Though acyclovir, a viral DNA polymerase inhibitor, was designed to treat herpesvirus infections, it is commonly used to treat RRP despite no biochemical rationale for its efficacy against HPV. 47 In a recent study, systemic acyclovir was given post‐operatively to 21 patients with JORRP and was found to significantly increase the time interval between papilloma operations and decrease the number of surgeries required after treatment compared with before treatment. Gastrointestinal side effects and headache are the most common adverse events related to acyclovir use. Evidence from this study suggests that acyclovir has both a safe side effect profile and may be used in combination with surgery as an adjuvant treatment for aggressive RRP. 48 Though robust clinical trials are limited, additional reports endorse these findings and suggest the need for future studies. 49
Retinoids, a drug class modeled from analogues of vitamin A, have long been used to treat dermatologic conditions of epithelial cells. RRP involves hyperproliferation of respiratory tract epithelium, and recent case reports have experimented with retinoid treatments. While two studies identified dramatic clinical improvement, a larger RCT was prematurely terminated due to the drug's toxic effects without sufficient clinical improvement. 50 , 51 , 52 The current evidence is inconclusive yet certainly warrants further investigation.
While no curative therapy for RRP exists, patients may achieve disease control using a combination of multi‐medication therapy, though they are not yet FDA approved for RRP, coupled with surgical debridement. Most patients typically achieve reduction in the number and size of their lesions over time with the requirement for less frequent excisions. Of note, existing evidence for some of the novel and experimental treatment options is limited both by sample size and sub‐optimal study design. Further formal clinical trials are required to develop advantageous surgical techniques and intralesional therapies that minimize complications and maximize the interval between required surgeries.
3.6. HPV vaccine and immunotherapy
As novel treatments continue to develop, the HPV vaccine has recently emerged as both a form of prevention and treatment. The quadrivalent HPV vaccine (Gardasil) was first introduced in 2006 which covered strains 6, 11, 16, and 18. Though originally designed for the prevention of cervical cancer, the Gardasil vaccine has been found to reduce the risk of RRP, decrease annual surgery requirements, and increase the interval between procedures. 53 , 54
The current literature suggests that implementation of the HPV vaccine can reduce the incidence of childhood HPV infection leading to subsequent JORRP and can also be used as secondary prevention to treat active RRP disease. 16 A 2007 prospective study of Australian JORRP population found a significant decrease in the disease incidence rate after implementation of a Gardasil vaccination program aimed to create herd immunity. In this study, the authors also found that male genital warts declined after vaccine implementation, thus suggesting that HPV vaccination can also serve to reduce horizontal viral transmission. 55 In practice, the HPV vaccine should be followed by immediate resection of existing lesions to allow growth of new, non‐diseased epithelial tissue which is protected from HPV. 56 A 2017 systematic review of HPV vaccination similarly found that HPV vaccination resulted in decreased disease recurrence and disease burden and increased intersurgical interval. 57 Additional evidence revealed that the vaccine resulted in increased antibodies against patient‐specific HPV viral strains amongst those with RRP. 58 Though larger clinical trials are warranted, preliminary evidence suggests Gardasil can help prevent viral transmission, reduce disease burden, and prevent papilloma recurrences.
Additionally, the mumps vaccine, originally designed for childhood immunization, may have utility as a potential treatment for RRP. Though the mechanism is unclear, small pilot studies have shown that intralesional vaccine injection may help induce remission of RRP by causing a robust inflammatory response that facilitates papilloma clearance. 59 It is inexpensive, safe, and widely available making it a viable potential treatment.
More recently, immune modulating therapies have been under investigation for the treatment of RRP. It has been well described that HPV‐associated head and neck squamous cell carcinoma (HNSCC) have high expression of programmed death ligand‐1 (PD‐L1). 60 Binding of PD‐L1 and PD‐1, present on leukocytes, causes downregulation of the host's immune system. Immune checkpoint inhibitors are drugs which prevent this downregulation of the immune response. Promising data showing the utility of PD‐1 inhibitors, such as pembrolizumab and avelumab, in the treatment of HPV‐associated HNSCC has prompted the investigation of these immunotherapies in the treatment of RRP. 61 An ongoing Phase II clinical trial (NCT 02632344) is investigating the efficacy of pembrolizumab in the treatment of RRP while another phase II clinical trial (NCT 02859454) is assessing efficacy of avelumab for the treatment of RRP. 16 Results from these large clinical trials will certainly provide guidance for future immunotherapy directions and provide hope for the potential novel treatments.
It is important to note that many of the aforementioned medical and surgical treatments are still in the early stages of investigation. Most of the existing RRP literature is limited by small sample sizes, short‐term patient follow up, and anecdotal evidence. Additionally, there is potential for bias since it is difficult to identify the motive of authors in testing certain medications and devices. It is critical to recognize the lack of robust evidence about the various treatments, and future research should be directed at improving the quantity and quality of such data.
3.7. Psychosocial factors
In addition to the physical disease toll, RRP places a burden on patients' quality of life (QOL). Numerous monthly doctor visits, complex medication regimens, and countless invasive operations contribute to some of the negative psychosocial implications. Otolaryngologists often assess disease burden through QOL surveys, such as the Health‐Related Quality of Life score (HR‐QOL) which assesses level of physical, mental, social, and functional health. 20 , 62 A multi‐institution study found that patients with RRP had significantly higher Hospital Anxiety and Depression Scale (HADS) scores for depression and worse voice‐related quality of life than paired controls. 63 Many patients endure social challenges due to problems with voice quality, breathing difficulty, and the need for regular doctor visits. Often patients are referred to voice therapy which helps them unlearn detrimental, compensatory voice behaviors and improves natural healing of the vocal cords. 14
There is additional stigma surrounding RRP due to concerns about spreading the disease to partners and close contacts. This can negatively impact patients' interpersonal relationships and at times warrants referral to psychologists for additional resources. Care for patients with RRP should involve a whole‐person oriented approach addressing disease risk factors, medical and surgical disease management, and psychosocial support to optimize patient outcomes.
4. CONCLUSION
Recurrent respiratory papillomatosis (RRP) is a rare disease of the larynx caused by human papillomavirus (HPV). It is characterized by recurring, benign laryngeal papillomas which are often refractory to treatment. This review describes the epidemiology of RRP, including patient demographics, HPV immunology, clinical course, and psychosocial factors. RRP affects both children and adults and most commonly presents with difficulty breathing, vocal changes, or stridor. Endoscopy reveals characteristic grape‐like clusters of papillomatous lesions. Potential maternal risk factors for RRP include maternal HPV infection, vaginal delivery, and teenage mother. Additionally, patient smoking status, sexual behaviors, and younger age at diagnosis may contribute to disease incidence and severity. Treatment involves a combination of medical therapy (eg, interferon‐alpha (IFN‐α), indole‐3‐carbinol (I3C), acyclovir, retinoids, cidofovir, HPV vaccine, and mumps vaccine) in combination with frequent surgical excisions. Future disease management may involve herd immunity through HPV vaccination and secondary HPV vaccine treatment as well as novel immunotherapies, like pembrolizumab and avelumab. Common surgical modalities include CO2‐laser, sharp dissection, coblation, microdebridement, and photoangiolytic laser. The clinical course of RRP varies widely based on each individual, ranging from spontaneous remission to distal respiratory tract involvement and/or malignant transformation. Optimal patient management involves a customized, multi‐treatment regimen coupled with psychosocial support. Despite the existing literature, RRP remains a poorly understood disease, and future studies evaluating risk factors, medical therapies, and surgical options are needed.
CONFLICT OF INTEREST
None.
ACKNOWLEDGMENTS
We would like to acknowledge the support of this research by the Arthur Lacerte gift fund.
Welschmeyer A, Berke GS. An updated review of the epidemiological factors associated with recurrent respiratory papillomatosis. Laryngoscope Investigative Otolaryngology. 2021;6:226–233. 10.1002/lio2.521
Funding information Arthur Lacerte gift fund, Grant/Award Number: gift grant
BIBLIOGRAPHY
- 1. Dedo HH, Yu KCY. CO2 laser treatment in 244 patients with respiratory papillomas. Laryngoscope. 2001;111:1639‐1644. 10.1097/00005537-200109000-00028. [DOI] [PubMed] [Google Scholar]
- 2. Derkay CS, Wiatrak B. Recurrent respiratory papillomatosis: a review. Laryngoscope. 2008;118:1236‐1247. 10.1097/MLG.0b013e31816a7135. [DOI] [PubMed] [Google Scholar]
- 3. Alkhilaiwi F, Paul S, Zhou D, et al. High‐throughput screening identifies candidate drugs for the treatment of recurrent respiratory papillomatosis. Papillomavirus Res. 2019;8:100181. 10.1016/j.pvr.2019.100181. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Moreddu E, Lambert E, Kacmarynski D, Nicollas R, Triglia JM, Smith RJ. Risk factors for severity of juvenile‐onset recurrent respiratory papillomatosis at first endoscopy. Eur Ann Otorhinolaryngol Head Neck Dis. 2019;136:25‐28. 10.1016/j.anorl.2018.11.007. [DOI] [PubMed] [Google Scholar]
- 5. Omland T, Lie KA, Akre H, et al. Recurrent respiratory papillomatosis: HPV genotypes and risk of high‐grade laryngeal neoplasia. PLoS One. 2014;9:e99114. 10.1371/journal.pone.0099114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Fortes HR, von Ranke FM, Escuissato DL, et al. Recurrent respiratory papillomatosis: a state‐of‐the‐art review. Respir Med. 2017;126:116‐121. 10.1016/j.rmed.2017.03.030. [DOI] [PubMed] [Google Scholar]
- 7. James M, Katundu D, Chussi D, Shija P. Prevalence, clinical presentations, associated risk factors and recurrence of laryngeal papillomatosis among inpatients attended at a Tertiary Hospital in Northern zone Tanzania. Pan Afr Med J. 2018;30. 10.11604/pamj.2018.30.209.11211. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Kashima HK, Shah F, Lyles A, et al. A comparison of risk factors in juvenile‐onset and adult‐onset recurrent respiratory papillomatosis. Laryngoscope. 1992;102:9‐13. 10.1288/00005537-199201000-00002. [DOI] [PubMed] [Google Scholar]
- 9. Ruiz R, Achlatis S, Verma A, et al. Risk factors for adult‐onset recurrent respiratory papillomatosis. Laryngoscope. 2014;124:2338‐2344. 10.1002/lary.24730. [DOI] [PubMed] [Google Scholar]
- 10. Quiney RE, Hall D, Croft CB. Laryngeal papillomatosis: analysis of 113 patients. Clin Otolaryngol Allied Sci. 1989;14:217‐225. 10.1111/j.1365-2273.1989.tb00364.x. [DOI] [PubMed] [Google Scholar]
- 11. Lie ES, Engh V, Boysen M, et al. Squamous cell carcinoma of the respiratory tract following laryngeal papillomatosis. Acta Otolaryngol. 1994;114:209‐212. 10.3109/00016489409126044. [DOI] [PubMed] [Google Scholar]
- 12. Karatayli‐Ozgursoy S, Bishop JA, Hillel A, Akst L, Best SRA. Risk factors for dysplasia in recurrent respiratory papillomatosis in an adult and pediatric population. Ann Otol Rhinol Laryngol. 2016;125:235‐241. 10.1177/0003489415608196. [DOI] [PubMed] [Google Scholar]
- 13. Buchinsky FJ, Valentino WL, Ruszkay N, et al. Age at diagnosis, but not HPV type, is strongly associated with clinical course in recurrent respiratory papillomatosis. PLoS One. 2019;14:e0216697. 10.1371/journal.pone.0216697. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Awad R, Shamil E, Aymat‐Torrente A, Gibbins N, Harris S. Management of laryngeal papillomatosis using coblation: another option of surgical intervention. Eur Arch Oto‐Rhino‐Laryngol. 2019;276:793‐800. 10.1007/s00405-019-05354-3. [DOI] [PubMed] [Google Scholar]
- 15. El Achkar VNR, Duarte A, Carlos R, et al. Histopathological features of juvenile‐onset laryngeal papillomatosis related to severity. Head Neck. 2019;41:1412‐1417. 10.1002/hed.25602. [DOI] [PubMed] [Google Scholar]
- 16. Ivancic R, Iqbal H, de Silva B, Pan Q, Matrka L. Immunological tolerance of low‐risk HPV in recurrent respiratory papillomatosis. Clin Exp Immunol. 2020;199:131‐142. 10.1111/cei.13387. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Hu L, Benedict PA, Garber D, Wang B, Amin MR, Branski RC. Laryngeal distribution of adult‐onset recurrent respiratory papillomatosis: a longitudinal study. Laryngoscope. 2019;129:1993‐1997. 10.1002/lary.27694. [DOI] [PubMed] [Google Scholar]
- 18. Xue Q, Wang H, Wang J. Recurrent respiratory papillomatosis: an overview. Eur J Clin Microbiol Infect Dis. 2010;29:1051‐1054. 10.1007/s10096-010-0963-6. [DOI] [PubMed] [Google Scholar]
- 19. Arffa RE, Krishna P, Gartner‐Schmidt J, Rosen CA. Normative values for the voice handicap index‐10. J Voice. 2012;26:462‐465. 10.1016/j.jvoice.2011.04.006. [DOI] [PubMed] [Google Scholar]
- 20. McMurray JS, Connor N, Ford CN. Cidofovir efficacy in recurrent respiratory papillomatosis: a randomized, double‐blind, placebo‐controlled study. Ann Otol Rhinol Laryngol. 2008;117:477‐483. 10.1177/000348940811700702. [DOI] [PubMed] [Google Scholar]
- 21. Kupfer RA, Çadalli Tatar E, Barry JO, Allen CT, Merati AL. Anatomic Derkay score is associated with voice handicap in laryngeal papillomatosis in adults. Otolaryngology – Head Neck Surg. 2016;154:689‐692. 10.1177/0194599816628871. [DOI] [PubMed] [Google Scholar]
- 22. Shehata BM, Otto KJ, Sobol SE, et al. E6 and E7 oncogene expression by human papilloma virus (HPV) and the aggressive behavior of recurrent laryngeal papillomatosis (RLP). Pediatr Dev Pathol. 2008;11:118‐121. 10.2350/06-09-0160.1. [DOI] [PubMed] [Google Scholar]
- 23. Marchiori E, De Araujo Neto C, Meirelles GSP, et al. Laryngotracheobronchial papillomatosis: findings on computed tomography scans of the chest. J Bras Pneumol. 2008;1084‐1089. 10.1590/S1806-37132008001200016. [DOI] [PubMed] [Google Scholar]
- 24. Tjon Pian Gi REA, San Giorgi MRM, Slagter‐Menkema L, et al. Clinical course of recurrent respiratory papillomatosis: comparison between aggressiveness of human papillomavirus‐6 and human papillomavirus‐11. Head Neck. Vol 37. New Jersey: Wiley Periodicals, LLC; 2015:1625‐1632. 10.1002/hed.23808. [DOI] [PubMed] [Google Scholar]
- 25. Bonagura VR, Hatam LJ, Rosenthal DW, et al. Recurrent respiratory papillomatosis: a complex defect in immune responsiveness to human papillomavirus‐6 and ‐11. Apmis. 2010;118(6–7):455‐470. 10.1111/j.1600-0463.2010.02617.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Rasmussen ER, Schnack DT, Jørkov AS, Raja AA, Olsen CH, Homøe P. Long‐term follow‐up and outcome in patients with recurrent respiratory laryngeal papillomatosis. Dan Med J. 2017;64(12):A5424. [PubMed] [Google Scholar]
- 27. Avelino MAG, Zaiden TCDT, Gomes RO. Surgical treatment and adjuvant therapies of recurrent respiratory papillomatosis. Braz J Otorhinolaryngol. 2013;79:636‐642. 10.5935/1808-8694.20130114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Papaspyrou G, Schick B, Papaspyrou S, Eivazi B, Kadah BA. Retrospective analysis of laser vs other therapeutic modalities for laryngeal papillomatosis: European multicenter study. J BUON. 2016;21:1274‐1278. [PubMed] [Google Scholar]
- 29. Shikowitz MJ, Abramson AL, Steinberg BM, et al. Clinical trial of photodynamic therapy with meso‐tetra (hydroxyphenyl) chlorin for respiratory papillomatosis. Arch Otolaryngol – Head Neck Surg. 2005;131:99‐105. 10.1001/archotol.131.2.99. [DOI] [PubMed] [Google Scholar]
- 30. Zeitels SM, Barbu AM, Landau‐Zemer T, et al. Local injection of bevacizumab (Avastin) and angiolytic KTP laser treatment of recurrent respiratory papillomatosis of the vocal folds: a prospective study. Ann Otol Rhinol Laryngol. 2011;120:627‐634. 10.1177/000348941112001001. [DOI] [PubMed] [Google Scholar]
- 31. Yang S, Zhou C, Sun B, et al. Efficacy of microsurgery in combined with topical‐PDT in treating recurrent respiratory papillomatosis: compare JORRP with AORRP. Acta Otolaryngol. 2019;139(12):1133‐1139. 10.1080/00016489.2019.1667530. [DOI] [PubMed] [Google Scholar]
- 32. Healy GB, Gelber RD, Trowbridge AL, Grundfast KM, Ruben RJ, Price KN. Treatment of recurrent respiratory papillomatosis with human leukocyte interferon. N Engl J Med. 1988;319:401‐407. 10.1056/NEJM198808183190704. [DOI] [PubMed] [Google Scholar]
- 33. Leventhal BG, Kashima HK, Weck PW, et al. Randomized surgical adjuvant trial of interferon Alfa‐n1 in recurrent papillomatosis. Arch Otolaryngol Neck Surg. 1988;114:1163‐1169. 10.1001/archotol.1988.01860220097032. [DOI] [PubMed] [Google Scholar]
- 34. Michnovicz JJ, Bradlow HL. Altered estrogen metabolism and excretion in humans following consumption of Indole‐3‐Carbinol. Nutr Cancer. 1991;16:59‐66. 10.1080/01635589109514141. [DOI] [PubMed] [Google Scholar]
- 35. Rosen CA, Bryson PC. Indole‐3‐carbinol for recurrent respiratory papillomatosis: long‐term results. J Voice. 2004;18:248‐253. 10.1016/j.jvoice.2003.05.005. [DOI] [PubMed] [Google Scholar]
- 36. Ampofo E, Schmitt BM, Menger MM, Laschke MW. Targeting the microcirculation by indole‐3‐carbinol and its Main derivate 3,3′‐diindolylmethane: effects on angiogenesis, thrombosis and inflammation. Mini‐Rev Med Chem. 2018;18:962‐968. 10.2174/1389557518666180313100144. [DOI] [PubMed] [Google Scholar]
- 37. Soldatskiǐ IL, Onufrieva EK, Steklov AM, Gasparian SF, Strygina IV. The results of adjuvant therapy of juvenile recurring respiratory papillomatosis with the use of indole‐3‐carbinol. Vestn Otorinolaringol. 2011;5:47‐50. [PubMed] [Google Scholar]
- 38. Lee AS, Rosen CA. Efficacy of cidofovir injection for the treatment of recurrent respiratory papillomatosis. J Voice. 2004;18:551‐556. 10.1016/j.jvoice.2003.07.007. [DOI] [PubMed] [Google Scholar]
- 39. Pransky SM, Brewster DF, Magit AE, Kearus DB. Clinical update on 10 children treated with intralesional cidofovir injections for severe recurrent respiratory papillomatosis. Arch Otolaryngol – Head Neck Surg. 2000;126:1239‐1243. 10.1001/archotol.126.10.1239. [DOI] [PubMed] [Google Scholar]
- 40. Derkay CS, Volsky PG, Rosen CA, et al. Current use of intralesional cidofovir for recurrent respiratory papillomatosis. Laryngoscope. 2013;123:705‐712. 10.1002/lary.23673. [DOI] [PubMed] [Google Scholar]
- 41. Jackowska J, Piersiala K, Klimza H, Wierzbicka M. Outcomes of bevacizumab and cidofovir treatment in HPV‐associated recurrent respiratory papillomatosis – review of the literature. Otolaryngol Pol = Polish Otolaryngol. Vol 72. Netherlands: Elsevier; 2018:1‐4. 10.5604/01.3001.0012.0484. [DOI] [PubMed] [Google Scholar]
- 42. Broekema FI, Dikkers FG. Side‐effects of cidofovir in the treatment of recurrent respiratory papillomatosis. Eur Arch Oto‐Rhino‐Laryngol. 2008;265:871‐879. 10.1007/s00405-008-0658-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Lacy SA, Hitchcock MJM, Lee WA, Tellier P, Cundy KC. Effect of oral probenecid coadministration on the chronic toxicity and pharmacokinetics of intravenous cidofovir in cynomolgus monkeys. Toxicol Sci. 1998;44:97‐106. 10.1006/toxs.1998.2481. [DOI] [PubMed] [Google Scholar]
- 44. Gupta HT, Robinson RA, Murray RC, Karnell LH, Smith RJH, Hoffman HT. Degrees of dysplasia and the use of cidofovir in patients with recurrent respiratory papillomatosis. Laryngoscope. 2010;120:698‐702. 10.1002/lary.20785. [DOI] [PubMed] [Google Scholar]
- 45. Nagel S, Busch C, Blankenburg T, Schütte W. Treatment of respiratory papillomatosis a case report on systemic treatment with bevacizumab. Pneumologie. 2009;63:387‐389. 10.1055/s-0029-1214714. [DOI] [PubMed] [Google Scholar]
- 46. Best SR, Mohr M, Zur KB. Systemic bevacizumab for recurrent respiratory papillomatosis: a national survey. Laryngoscope. 2017;127:2225‐2229. 10.1002/lary.26662. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47. Kimberlin DW. Current status of antiviral therapy for juvenile‐onset recurrent respiratory papillomatosis. Antiviral Res. 2004;63:141‐151. 10.1016/j.antiviral.2004.06.013. [DOI] [PubMed] [Google Scholar]
- 48. Mitra S, Das A, Ghosh D, Sengupta A. Postoperative systemic acyclovir in juvenile‐onset recurrent respiratory papillomatosis: the outcome. Ear Nose Throat J. 2019;98:28‐31. 10.1177/0145561318823311. [DOI] [PubMed] [Google Scholar]
- 49. Chaturvedi J, Sreenivas V, Hemanth V, Nandakumar R. Management of adult recurrent respiratory papillomatosis with oral acyclovir following micro laryngeal surgery: a case series. Indian J Otolaryngol Head Neck Surg. 2014;66:359‐363. 10.1007/s12070-011-0456-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50. Eicher SA, Taylor Cooley LD, Donovan DT. Isotretinoin therapy for recurrent respiratory papillomatosis. Arch Otolaryngol Neck Surg. 1994;120:405‐409. 10.1001/archotol.1994.01880280033005. [DOI] [PubMed] [Google Scholar]
- 51. Osborne C, LeBoeuf H, Jones J. Isotretinoin in respiratory papillomatosis. Ann Intern Med. 2000;132:1007. 10.7326/0003-4819-132-12-200006200-00028. [DOI] [PubMed] [Google Scholar]
- 52. Bell R, Hong WK, Itri LM, McDonald G, Stuart Strong M. The use of cis‐retinoic acid in recurrent respiratory papillomatosis of the larynx: a randomized pilot study. Am J Otolaryngol – Head Neck Med Surg. 1988;9:161‐164. 10.1016/S0196-0709(88)80023-1. [DOI] [PubMed] [Google Scholar]
- 53. Rosenberg T, Philipsen BB, Mehlum CS, et al. Therapeutic use of the human papillomavirus vaccine on recurrent respiratory papillomatosis: a systematic review and meta‐analysis. J Infect Dis. 2019;219:1016‐1025. 10.1093/infdis/jiy616. [DOI] [PubMed] [Google Scholar]
- 54. Yiu Y, Fayson S, Smith H, Matrka L. Implementation of routine HPV vaccination in the management of recurrent respiratory papillomatosis. Ann Otol Rhinol Laryngol. 2019;128:309‐315. 10.1177/0003489418821695. [DOI] [PubMed] [Google Scholar]
- 55. Novakovic D, Cheng ATL, Zurynski Y, et al. A prospective study of the incidence of juvenile‐onset recurrent respiratory papillomatosis after implementation of a national HPV vaccination program. J Infect Dis. 2018;217:208‐212. 10.1093/infdis/jix498. [DOI] [PubMed] [Google Scholar]
- 56. Papaioannou VA, Lux A, Voigt‐Zimmermann S, Arens C. Treatment outcomes of recurrent respiratory papillomatosis: retrospective analysis of juvenile and adult cases. German version. HNO. 2017;65:923‐932. 10.1007/s00106-017-0377-1. [DOI] [PubMed] [Google Scholar]
- 57. Dion GR, Teng S, Boyd LR, et al. Adjuvant human papillomavirus vaccination for secondary prevention: a systematic review. JAMA Otolaryngol – Head Neck Surg. 2017;143:614‐622. 10.1001/jamaoto.2016.4736. [DOI] [PubMed] [Google Scholar]
- 58. Tjon Pian Gi REA, San Giorgi MRM, Pawlita M, et al. Immunological response to quadrivalent HPV vaccine in treatment of recurrent respiratory papillomatosis. Eur Arch Oto‐Rhino‐Laryngol. 2016;273:3231‐3236. 10.1007/s00405-016-4085-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59. Pashley NRT. Can mumps vaccine induce remission in recurrent respiratory papilloma? Arch Otolaryngol – Head Neck Surg. 2002;128:783‐786. 10.1001/archotol.128.7.783. [DOI] [PubMed] [Google Scholar]
- 60. Lyford‐Pike S, Peng S, Young GD, et al. Evidence for a role of the PD‐1:PD‐L1 pathway in immune resistance of HPV‐associated head and neck squamous cell carcinoma. Cancer Res. 2013;73:1733‐1741. 10.1158/0008-5472.CAN-12-2384. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61. Brahmer JR, Drake CG, Wollner I, et al. Phase I study of single‐agent anti‐programmed death‐1 (MDX‐1106) in refractory solid tumors: safety, clinical activity, pharmacodynamics, and immunologic correlates. J Clin Oncol. 2010;28:3167‐3175. 10.1200/JCO.2009.26.7609. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62. Horner‐Johnson W, Krahn G, Andresen E, Hall T, RRTC Expert Panel on Health Status Measurement . Developing summary scores of health‐related quality of life for a population‐based survey. Public Health Rep. 2009;124:103‐110. 10.1177/003335490912400113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63. San Giorgi MRM, Aaltonen LM, Rihkanen H, et al. Quality of life of patients with recurrent respiratory papillomatosis. Laryngoscope. 2017;127:1826‐1831. 10.1002/lary.26413. [DOI] [PubMed] [Google Scholar]