

Abstract
Background
Sports injuries are very common, and the management demands high degrees of skills and best techniques for an early return to play. The use of Platelet Rich Plasma (PRP) injections in the treatment of tendon, muscle and ligament injuries has become popular. This study observes the outcomes of PRP injections in sports injuries.
Methods
Forty-eight athletes (mean age 29.93 ± 8.48, Male: 37, Female: 11) presenting to a sports medicine centre with different sports injuries with symptom duration (2.81 ± 1.94) months were given PRP injections (single or multiple) four weeks apart with maximum number of injections up to three depending upon the clinical condition, Pre and Post VAS scores. Specific rehabilitation program was administered and compliance was graded by Sports Injury Rehabilitation Adherence Scale (SIRAS). A 1 year follow-up of cases was done for assessing player satisfaction and return to play.
Results
Pre-procedure (7.25 ± 0.70) and post-procedure (2.42 ± 0.74) VAS score for all athletes showed significant difference with a p value at 0.0001. The average number of injections was 1.35 ± 1.41 with 72.91% requiring only one injection while 18.75% and 8.33% required two and three injections, respectively.
Conclusion
Athletes who required a single injection for acute injuries of lower grade returned to sports activity earlier than those who required multiple injections for chronic injuries. PRP injection has optimal effects on sports injuries not responding to conservative management
Keywords: Platelet-rich plasma, Sports injury, Return to sports, Ultrasound guided, Rehabilitation, Patient satisfaction
Introduction
Sports for recreation or as a profession has a positive impact on one’s health. Injuries related to sports are inevitable but can be prevented. The incidence of injury in sports has increased many folds due to a rise in participation, poor injury prevention strategies and faulty or inadequate training. These factors can inadvertently affect the athlete, shorten their career, and have significant implications in their quality of life. Musculoskeletal injuries in sports unless traumatic, are mostly a consequence of chronic misuse or overuse. Most of these problems can be treated conservatively with rest, non-steroidal anti-inflammatory drugs (NSAIDs), physiotherapy and rehabilitation. Those conditions that are subacute or chronic and that which does not respond well to rehabilitation needs necessary intervention. These pathologies most often are due to irreversible microstructural changes in the connective tissue that has failed to recover and adapt to rehabilitation. Conditions like these most often affect the tendons and the enthesis where biomechanical stress is higher at any given point in a practising athlete, they may also affect the muscle, cartilage, and bone under chronic stress. These problems do not have an effective treatment modality and this is the grey area where orthopaedic surgeons and sports physicians are trying to employ biological therapy to hasten the repair and thereby bring about recovery.
Basis of Biological Therapy
The role of our immune response in perpetuating chronic inflammation cannot be undermined in such conditions. It is imperative for the treating physician to understand tissue microenvironment in normal as well as diseased connective tissue at various stages of pathology. The appreciation and acceptance of pathologies at a molecular level have opened up possibilities in adapting to biological therapy and this is the reason for the sudden surge of application and research in this domain. The presence of non-myeloid stromal cells and their interaction with inflammatory cells in the maintenance of chronic inflammation is a piece of vital information noted by various researchers. Pro-resolving proteins Formyl peptide receptor 2 (FPR2/ALX) and Chemerin 2(ChemR23) is found in an increased quantity in the early-stage disease of tendons when compared to normal tendons. Their expression in resident stromal cells gives us scientific clues of importance. So, an earlier intervention in form of PRP at the acute stage delivering essential bioactive factors [1] to influence inflammatory and resident stromal cells alike to initiate or bring about a highly activated and co-ordinated process of inflammation resolution and restoration of tissue homeostasis might be helpful to regain tissue homeostasis.
PRP as an interventional treatment modality for sports injuries has proved to be beneficial in certain conditions. PRP is prepared from autologous platelets extracted from a patient's whole blood via centrifugation techniques. PRP has been the most sought research cell therapy in recent times due to its theoretical advantages in bone and soft tissue healing properties [2]. Tendons heal at a slower rate compared to other connective tissue due to its poor vascularity [3, 4]. Apart from its role in haemostasis and clot formation, the various growth factors released by alpha granule which comprise Fibroblast growth factor (FGF), Platelet derived growth factor (PDGF), Vascular endothelial growth factor (VEGF), Transforming growth factor (TGF), epidermal growth factor (EGF) and Insulin like growth factor-1 (IGF-1) are involved in healing process. The normal Platelet count is between 150,000 and 300,000 per μL. However, to obtain the advantage of PRP, the level of concentrated platelets should be supraphysiological in the range of 500,000–1,700,000 per µL. The efficacy however depends on its preparation, centrifugation techniques, presence of leukocytes, addition of activating factor and concentration of different growth factors. There is still no consensus on ideal preparation method. Effects on PRP have been studied on tendon related disorders such as rotator cuff tendinitis, medial and lateral epicondylitis [5], achilles tendinopathy and patellar tendinopathy. Recent studies have emerged that PRP has positive outcomes on certain muscle strains, degenerative conditions such as osteoarthritis [6–8] and in augmenting the outcomes in surgical repair of achilles tendon rupture [9] and rotator cuff tears [10]. Studies on effects of PRP injection among Indian athletes are lacking. This study aims to estimate the efficacy of Platelet-rich plasma injections in Sports injuries among Indian athletes. We hypothesize that PRP injections in sports injuries will aid in early recovery and return to sports.
Materials and Methods
Athletes with clinical signs and symptoms of acute or chronic injuries who presented to our Sports Injury centre between March 2016 and March 2018 were considered as a part of this period study. Inclusion criteria: (1) Sports injuries that occurred in the athletes between the age group 18–50 years, (2) Pain score of more than six on Visual analogue scale, (3) Painful activities that aggravated physical activity for more than a week. (4) Ultrasonographic or Magnetic resonance imaging confirmation of the clinically diagnosed condition. Exclusion criteria: (1) Local wound infection, (2) Pregnancy, (3) Recent surgical history, (4) History of thrombocytopenia, (5) Anticoagulant therapy, (6) Any recent febrile illness or active infectious disease/tumour, (7) Previous needle interventions, (8) Indications for definitive surgical management.
Baseline Data Collection
All patients who fulfilled inclusion criteria were then subjected to a demographic questionnaire which consisted of age, sex, occupation, primary sports, level of participation, mode of injury, training status, previous injuries and treatment obtained. The patients were examined by the trained specialists (Orthopaedic surgeons and sports physicians) who performed a standard clinical and physical examination to ascertain the diagnosis. MRI (Magnetic resonance Imaging) and Ultrasound as per requisites were done by a trained musculoskeletal radiologist to confirm the pathology.
Management
Patients with chronic sports injuries were advised to follow a condition-specific rehab program (The rehabilitation program varied between all athletes depending on the diagnosis, age, sports and functional outcome) and were subjected to PRP injection after a failed rehabilitation. Few subjects with acute conditions like ATFL (Anterior Talo Fibular Ligament) tear and MCL (Medial Collateral Ligament) injury of knee were subjected to the injection procedure without any prior rehabilitation. Those who accepted to participate in the study received oral and written information about the study and signed a written consent form.
Platelet-Rich Plasma Injection
Intralesional injection of autologous PRP was performed in the procedure room of our Sports Injury Centre. Pre VAS score was documented just prior to the first PRP injection for all patients. All injections were performed by the same Orthopaedic surgeon and interventional radiologist under Ultrasound guidance, followed up by an individualised rehabilitation protocol. Post PRP data was collected using an objective proforma and analysed at subsequent visits at four-weekly intervals until 12 weeks.
Preparation
Patient was first placed in an appropriate and comfortable setting that allowed for sterility and access to the site of injection. 30 mL of autologous blood was withdrawn into a Citrate phosphate–dextrose anticoagulant containing tubes from every athlete under aseptic conditions. Activating factors were not added to the concentrate. The samples were centrifuged with ROCHE device, LC Carousel Centrifuge (version 2.0, 2005, Switzerland) using a double spin method. In the first cycle, it is centrifuged at 5600 rpm for 10 min to separate RBCs, platelet-poor plasma (PPP) and PRP. The PPP is then extracted and discarded. Subsequently, the speed of the centrifuge is reduced to 2400 rpm to get a final separation of PRP from the RBCs. The mean baseline and PRP concentrate’s platelet count was between 220,000–340,000 per µL and 801,000–1,102,000 per µL respectively, which was nearly four times the basal value required for the beneficial effects of PRP [11]. Then the PRP is withdrawn and depending on the amount of blood sample collected there will be 4–6 mL of PRP available for injection.
Injection Procedure
The area of injury was marked prior to the injection. WHO’s pre-procedure Time out strategy was followed to ensure the correct side, site and duration of injection. With aseptic precautions, PRP was injected into the lesion under Ultrasonographic guidance (LOGIQ E, GE Medical Systems, Chicago, Illinois, USA) with a musculoskeletal transducer probe of 8–12 Hz. The volume of PRP injection varied from 2–3 mL in small joints (wrist, foot and ankle), 5-6 mL for large joints (Shoulder and knee) and 4-6 mL for muscle injuries. The patient was asked to lie supine for 15–20 min with intermittent ice application (18–20°). Upon discharge, they were given an analgesic (Acetaminophen) for a period of 5–7 days. They were instructed that mild pain will persist for a few days. All patients were advised to limit aggravating activities and apply intermittent ice therapy. Abstinence from sports training and participation was advocated. They were started on an individualised post-PRP rehabilitation program from day one which consisted of stretching followed by a graded strengthening program of the involved segment and was asked to report for adverse reactions. Various phases of tissue healing following PRP injection and the corresponding rehabilitative phases are detailed in Table 1. There are three phases of tendon healing post PRP and so are the rehabilitative phases [12].
Table 1.
Phases of tendon healing and corresponding phases of rehabilitation
| Tendon healing phases | Cellular mechanisms | Rehabilitation phases | Considerations | Components |
|---|---|---|---|---|
|
Phase I Inflammatory Phase (48–72 h) |
Debris removed from damaged tissue Cytokines and growth factors recruited |
Phase I Tissue protection (0–3 days) |
Reduction of load to the involved joint Avoid NSAIDs |
Adequate rest Initiate assisted range of motion Other activities as tolerated |
|
Phase II Proliferative phase (48 h to 6 weeks) |
Proteolytic degradation Chemotaxis Fibroblastic activity |
Phase II Early tissue healing (4 days to 6 weeks) |
Progressive loading of the involved joint Avoid cryotherapy Avoid NSAIDs Avoid eccentric training |
Gentle prolonged stretches to dynamic stretches Isometric exercises Strengthening of the adjacent kinetic chain |
|
Phase III Maturation phase (> 6 weeks) |
Accumulation of Type I collagen Remodelling |
Phase III Collagen strengthening (6 weeks to 3 months) |
Closed kinetic chain exercises Plyometric and proprioceptive training Eccentric strengthening Sports specific drills RTS after 3 months if pain scale < 3/10 |
The number of injections was decided according to the VAS score upon further reviews at 4th and 8th week. While few conditions required only one injection, these individuals had better outcome scores at 4th week and returned to pre-injury level earlier than expected. There were certain athletes who required two or three injections and all subsequent injections were given at 4th and 8th week respectively according to their VAS score, outcome measures and clinical signs and symptoms. Those patients who were unresponsive after three PRP injections or 12 weeks of treatment were advised to undergo alternative therapy.
Outcome Variables
Our Outcome Measures were Based on the Following
VAS score
Compliance to rehabilitation post PRP injection
Patient satisfaction
Recurrence of symptoms
Adverse effects
Return to pre injury level activity
VAS {Visual Analog Scale Analog Pain Score (VAS) (range 0 [no pain] to 10 [agonizing pain])} score was documented for all athletes at every visit. The validity and reliability of self-rating scales like the VAS have previously been well described [13]. Despite single or multiple injections, the Post VAS score following four weeks after the last injection was considered for final analysis. Compliance to rehabilitation post-PRP injection: compliance to rehabilitation post PRP injection was graded according to Sports Injury Rehabilitation Adherence Scale (SIRAS) which is a three-item scale completed by the physiotherapist during each visit [14, 15]. A score of 3–5 indicates poor adherence, 6–9 moderate adherence and 10–15 high adherence to rehabilitation by athletes. Patient satisfaction: all patients were assessed for treatment satisfaction using the Likert scale (I-Strongly disagree to V-Strongly agree). The satisfactory outcome was documented at 3 months, 6 months and 1 year. Questions included were pertaining to the pain, analgesic intake, response to rehabilitation and training (Fig. 1). The mean Likert score of all the above questions were considered for final analysis. Recurrence: recurrence of pain which aggravated on physical activity and on rehabilitation was assessed at subsequent reviews at the 4th and 8th week. Those patients who had persistent pain at the end of 4th and 8th week were given a second and third PRP injection respectively. Patients with recurrence of symptoms beyond 12 weeks, were advised alternative therapy pertaining to the condition. Adverse effects: giddiness was documented in two patients who received shoulder injections in a sitting position which was managed with continuous vital monitoring for a period of one hour. A sudden increase in pain in one shoulder and one knee injection for a period of three days were noted, treated with cryotherapy and analgesics which subsided gradually. No anaphylaxis or infections occurred in our study. Return to pre-injury activity: all the athletes who complete the course of PRP injection either single or multiple were assessed at 3 months, 6 months and at the end of 1 year to evaluate their status on return to pre-injury activity with the same level of intensity.
Fig. 1.

Components of Likert’s scale
Statistical Analysis
Descriptive statistics of the demographic data was performed and expressed as mean (± 1SD). Paired t-test was done to compare the VAS score pre and post PRP injection using the IBM SPSS Statistics software, version 26, with significance set at p value < 0.05 and a confidence interval of 95%.
Results
Demographic data of the study population are drafted in Table 2. The mean age was 29.93 ± 8.48 years consisting of 37 males and 11 females from a variety of sports backgrounds. Football players constituted 18.8% of the sample followed by 16.7% badminton and 8.3% volleyball players. Remaining 56.2% had players from the domains of wrestling, hockey, tennis, basketball, weight lifting and others (Fig. 2). The most common site of PRP injection was the shoulder (50%) followed by the knee (22.91%) and ankle (14.58%). Distribution of the anatomical region of injection is given in (Fig. 3). The outcome variables are quantified in Table 3. A graphical representation of Likert's scale distribution over 3 months, 6 months and 1 year is shown in Fig. 4. Percentile distribution of compliance to post PRP rehabilitation graded by means of SIRAS score is represented in Fig. 5. Those who showed moderate (25%) and high compliance (66.7%) to the rehab program had a lower mean Post VAS score of 2.5 ± 0.35 and 2.21 ± 0.7, respectively. Whereas those with a poor compliance (8.3%) had a comparatively higher mean VAS of 3.75 ± 1.25.
Table 2.
Demographic data
| Parameter | Data obtained |
|---|---|
| Sample size (n) | 48 |
| Age (years) | 29.93 ± 8.48 |
| Male: female | 37:11 |
| Level of participation | 68.75%—Professionals |
| 31.25%—Amateurs | |
| Mean duration of symptoms (months) | 2.81 ± 1.94 |
| Mean duration of conservative management (months) | 1.57 ± 2.12 |
Fig. 2.
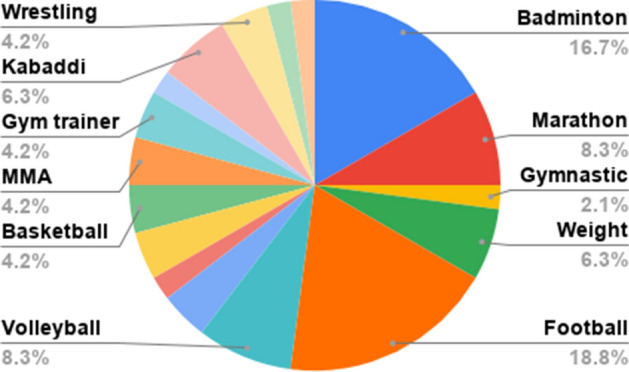
Count of sports
Fig. 3.
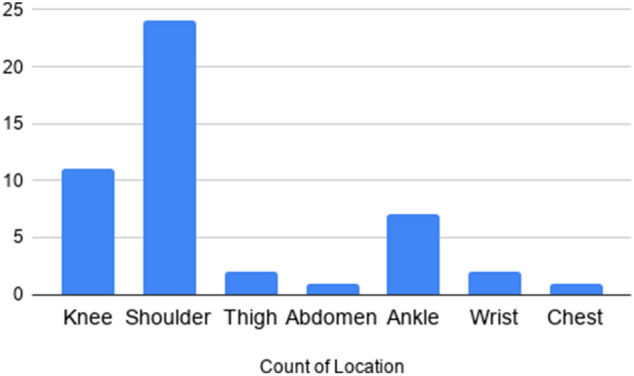
Pathological sites involved
Table 3.
Outcome measures and observed values
| Outcome variable | Value | ||
|---|---|---|---|
| Mean pre VAS score | 7.25 ± 0.70 | ||
| Mean post VAS score | 2.42 ± 0.74 | ||
| p value | 0.0001 (statistically significant) | ||
| Average number of injections | 1.35 ± 1.41 | ||
| Return to pre-injury activity level | 93.75% | ||
| SIRAS score | High adherence—66.66% | ||
| Moderate adherence—25% | |||
| Poor adherence—8.33% | |||
| Likert’s patient satisfaction scale | 3 months | 6 months | 1 year |
| I- 18.75% | I- 10.41% | I- 12.5% | |
| II- 31.25% | II- 8.33% | II- 6.25% | |
| III- 43.75% | III- 45.83% | III- 16.66% | |
| IV- 8.33% | IV- 33.33% | IV- 54.1% | |
| V- 0% | V- 0% | V- 10.41% | |
Fig. 4.
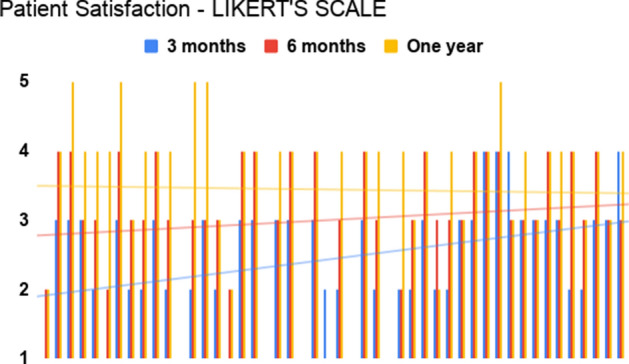
Patient satisfaction over subsequent follow-up
Fig. 5.
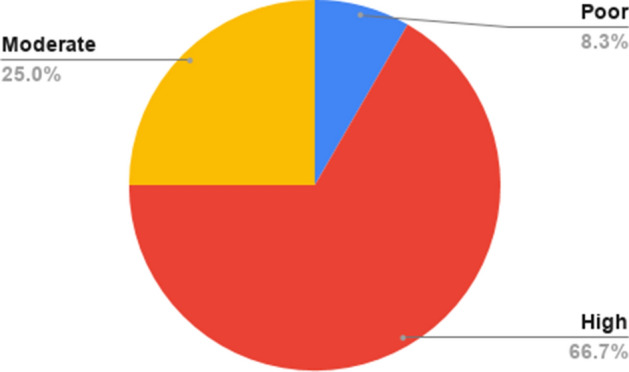
Compliance to rehabilitation (SIRAS score)
Discussion
This study was done to estimate the efficacy of PRP injections among different sports injuries in athletes (Professional and Amateurs). In certain acute conditions, after a failed conservative management, Corticosteroid (CS) injections, known for their anti-inflammatory effect were offered for pain relief. But recently, the use of PRP has been advocated due to its biological healing properties and lesser side effects compared with CS injections. The popularity of PRP usage in Orthopaedics has increased owing to the presence of several growth factors released from the alpha granules of platelets. Growth factors present in PRP is outlined in Table 4. All the injections were given under Ultrasound guidance as it is evident that it enhances the accuracy of injections, more so in musculoskeletal pathologies. Ultrasound further improves visualisation and our understanding of the pathology by means of distinctive tissue characterisation (can differentiate normal, tendinosis, tear).
Table 4.
Growth factors in PRP
| Platelet-derived growth factor (PDGF) | Enhances collagen synthesis, proliferation of bone cells, fibroblast chemotaxis and proliferative activity, macrophage activation |
| Transforming growth factor ß (TGF-ß) | Enhances synthesis of type I collagen, promotes angiogenesis, stimulates chemotaxis of immune cells, inhibits osteoclast formation and bone resorption |
| Vascular endothelial growth factor (VEGF) | Stimulates angiogenesis, migration and mitosis of endothelial cells, increases permeability of the vessels, stimulates chemotaxis of macrophages and neutrophils |
| Epidermal growth factor (EGF) | Stimulates cellular proliferation, differentiation of epithelial cells, promotes cytokine secretion by mesenchymal and epithelial cells |
| Insulin-like growth factor (IGF) | Promotes cell growth, differentiation, recruitment in bone, blood vessel, skin and other tissues, stimulates collagen synthesis together with PDGF |
| Fibroblast growth factor (FGF) | Promotes proliferation of mesenchymal cells, chondrocytes and osteoblasts, stimulates the growth and differentiation of chondrocytes and osteoblasts |
According to the results of our study, the primary outcome variable which was considered as the pre (7.25 ± 0.70) and post (2.42 ± 0.74) VAS score for all athletes showed significant difference with a p value at 0.0001. The average number of injections was 1.35 ± 1.41 with 72.91% requiring only one injection while 18.75% and 8.33% required two and three injections respectively. The number of injections can vary depending on the severity and type of injury [16]. The number of injections was based on the clinical signs and symptoms and response to rehabilitation. If the symptoms worsened or did not show any substantial improvement at subsequent visits during 4th and 8th week, they were given additional PRP injections. At the end of 12 weeks, patients who had received either single or multiple injections were reassessed with a clinical and physical examination and underwent surgical management. Of all the athletes (n = 48), only six (12.5%) required further treatment and among those, five athletes underwent surgery for respective conditions and one athlete was lost to follow up. Return to preinjury activity was evaluated through Post VAS score irrespective of the secondary treatment. A total of 45 athletes (93.75%) were able to return to their pre-injury activity (range 2–12 months) and were able to perform the sport-specific exercises at high intensity with minimum to no pain. The exercises post PRP injection were taught by a physiotherapist to all athletes in a supervised manner and the SIRAS score was used to calculate the adherence to the rehabilitation program every week.
Among the two patients diagnosed with Early Osteoarthritis of the knee, both received three injections each and had favourable outcomes and returned to pre-injury activity. Likewise athletes with Chondromalacia patella (10.41%) also returned to pre-injury activity with one injection each. This finding supports the evidence that PRP injection can be useful in treating athletes with chondromalacia patella as a part of Patellofemoral pain syndrome [17]. Athletes with Glenohumeral joint pathology (50%) constituted the major part of the sample. Among the shoulder pathologies, most athletes had rotator cuff tendinopathy (20.83%). The number of injections received by them was 1.52 ± 0.71. Of all the athletes, those who did not return to pre-injury activity (6.25%), they had pathology around the Glenohumeral joint (GHJ). Likewise, athletes requiring secondary treatment in the form of surgery or interventional therapy were also with GHJ issues (10.41%) while one patient with Scapulothoracic bursitis was lost to follow up at the end of 1 year. Literature regarding the use of PRP injection in chronic rotator cuff tendinopathy is still inconclusive as it depends on multiple factors [18–20]. Whereas there is no evidence to support the use of PRP in conditions such as Superior Labrum Anterior–Posterior (SLAP) tear of grade I and II, Biceps tendinitis, Partial Articular Supraspinatus Tendon Avulsion (PASTA) lesion etc. Athletes with SLAP tear (8.33%) and biceps tendinitis (6.25%) returned to their pre-injury activity, whereas athletes with PASTA lesion (4.1%) required surgical management despite multiple injections. Among muscle injuries of Grade I and II (Rectus femoris, Rectus abdominis and Pectoralis major) there were four athletes (8.33%) who all returned to pre-injury activity with a single injection of PRP at an early stage. This supports the evidence that muscle strains of grade I and II when treated with PRP injection and a supervised strengthening program guided to an early return to pre-injury activity. On the contrary, low to moderate quality randomized controlled trials show that PRP injections provide no superior, clinically relevant, effect on return to sport, recurrences, function, and pain for athletes with acute muscle injuries [21]. Muscle lesions account for one third of sport-related injuries and 92% of them affect the four major muscle groups of the lower limb: first and foremost hamstrings, followed by adductors, quadriceps, and calf muscles with reinjury rates as high as 39% in season [22].
Other tendon related injuries such as Achilles tendinopathy (6.25%) and patellar tendinopathy (4.1%) had excellent outcomes with mean injection of one and two respectively and returned to pre-injury activity. This stands in line with available literature where there is moderate to strong evidence for PRP injection in treatment of chronic achilles tendinopathy [23–26] and patellar tendinopathy [27, 28]. Three athletes (6.25%) with achilles tendinopathy received only one injection and all returned to pre-injury activity with minimal pain as quoted in previous studies [29, 30]. Patient satisfaction scoring was done with Likert scale showed that patients with acute injury had favourable outcomes earlier with single injection whereas those with chronic injuries and degenerative conditions were less satisfied and required multiple injections. Similarly, high levels of compliance (SIRAS score) with the post PRP rehabilitation program was directly proportional to patient satisfaction and VAS pain score.
Limitations
As it was a period study the power analysis was not done to obtain an adequate sample size. A homogenous study would have been better for comparing outcomes. Subgroup analysis between different conditions and sports was not done due to varied sample representation. Functional outcome scores pertaining to a particular joint was not possible because of multiple sites involved in the study. Future scope: USG guided tissue characterisation to determine tears, follow up Ultrasonography for tissue repair, Consensus on number of injections, volume and ideal platelet concentration method to be determined by performing large size randomised controlled trials.
Conclusion
Athletes who required a single injection for acute injuries of lower grade returned to sports activity earlier than those who required multiple injections for chronic injuries. We advocate the use of PRP as an adjunct therapy for augmentation of tissue healing for better recovery. PRP injection has optimal effects on sports injuries not responding to conservative management.
Compliance with Ethical Standards
Conflict of interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Ethical standard statement
This article does not contain any studies with human or animal subjects performed by the any of the authors.
Informed consent
For this type of study informed consent is not required.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Sivaraman Arumugam, Email: drarumugam@csstrucoach.in.
Ayyadurai Prakash, Email: prakashortho@outlook.com.
Gopalakrishnan Janani, Email: shubajanani@gmail.com.
Moorthy Vignesh, Email: v.moorthykz@gmail.com.
Masilamani Mukilvannan Anjanavannan, Email: dr.vannan95@gmail.com.
Suresh Perumal, Email: apsureshortho@gmail.com.
Thiagarajan Alwar, Email: drkatn@csstrucoach.in.
References
- 1.Anitua E, Andia I, Ardanza B, Nurden P, Nurden AT. Autologous platelets as a source of proteins for healing and tissue regeneration. Thrombosis and Haemostasis. 2004;91(1):4–15. doi: 10.1160/TH03-07-0440. [DOI] [PubMed] [Google Scholar]
- 2.de Mos M, van der Windt AE, Jahr H, van Schie HTM, Weinans H, Verhaar JAN, et al. Can platelet-rich plasma enhance tendon repair?: a cell culture study. American Journal of Sports Medicine. 2008;36(6):1171–1178. doi: 10.1177/0363546508314430. [DOI] [PubMed] [Google Scholar]
- 3.Hayem G. The normal tendon and the abnormal tendon. Joint Bone Spine. 2001;68(1):19–25. doi: 10.1016/S1297-319X(01)00261-5. [DOI] [PubMed] [Google Scholar]
- 4.Fenwick SA, Hazleman BL, Riley GP. The vasculature and its role in the damaged and healing tendon. Arthritis Research & Therapy. 2002;4(4):252. doi: 10.1186/ar416. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Raeissadat, S. A., Sedighipour, L., Rayegani, S. M., Bahrami, M. H., Bayat, M., Rahimi, R. (2014). Effect of Platelet-Rich Plasma (PRP) versus Autologous Whole Blood on Pain and Function Improvement in Tennis Elbow: A Randomized Clinical Trial [Internet]. Vol. 2014, Pain Research and Treatment. Hindawi. p. e191525. Available from: https://www.hindawi.com/journals/prt/2014/191525/ Accessed 26 May 2020. [DOI] [PMC free article] [PubMed]
- 6.Heijink A, Gomoll AH, Madry H, Drobnič M, Filardo G, Espregueira-Mendes J, et al. Biomechanical considerations in the pathogenesis of osteoarthritis of the knee. Knee Surgery, Sports Traumatology, Arthroscopy. 2012;20(3):423–435. doi: 10.1007/s00167-011-1818-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Hart R, Safi A, Komzák M, Jajtner P, Puskeiler M, Hartová P. Platelet-rich plasma in patients with tibiofemoral cartilage degeneration. Archives of Orthopaedic and Trauma Surgery. 2013;133(9):1295–1301. doi: 10.1007/s00402-013-1782-x. [DOI] [PubMed] [Google Scholar]
- 8.Jang S-J, Kim J-D, Cha S-S. Platelet-rich plasma (PRP) injections as an effective treatment for early osteoarthritis. European Journal of Orthopaedic Surgery & Traumatology. 2013;23(5):573–580. doi: 10.1007/s00590-012-1037-5. [DOI] [PubMed] [Google Scholar]
- 9.Sánchez M, Anitua E, Azofra J, Andía I, Padilla S, Mujika I. Comparison of surgically repaired achilles tendon tears using platelet-rich fibrin matrices. American Journal of Sports Medicine. 2007;35(2):245–251. doi: 10.1177/0363546506294078. [DOI] [PubMed] [Google Scholar]
- 10.Weber SC, Kauffman JI, Parise C, Weber SJ, Katz SD. Platelet-rich fibrin matrix in the management of arthroscopic repair of the rotator cuff: a prospective, randomized, double-blinded study. The American Journal of Sports Medicine. 2012 doi: 10.1177/0363546512467621. [DOI] [PubMed] [Google Scholar]
- 11.Eppley BL, Woodell JE, Higgins J. Platelet quantification and growth factor analysis from platelet-rich plasma: implications for wound healing. Plastic and Reconstructive Surgery. 2004;114:1502–1508. doi: 10.1097/01.PRS.0000138251.07040.51. [DOI] [PubMed] [Google Scholar]
- 12.Sampson S, Gerhardt M, Mandelbaum B. Platelet rich plasma injection grafts for musculoskeletal injuries: a review. Current Reviews in Musculoskeletal Medicine. 2008;1(3–4):165–174. doi: 10.1007/s12178-008-9032-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Kelly A-M. The minimum clinically significant difference in visual analogue scale pain score does not differ with severity of pain. Emergency Medicine Journal. 2001;18(3):205–207. doi: 10.1136/emj.18.3.205. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Kolt GS, Brewer BW, Pizzari T, Schoo AMM, Garrett N. The sport injury rehabilitation adherence scale: a reliable scale for use in clinical physiotherapy. Physiotherapy. 2007;93(1):17–22. doi: 10.1016/j.physio.2006.07.002. [DOI] [Google Scholar]
- 15.Brewer BW, Van Raalte JL, Cornelius AE, Petitpas AJ, Sklar JH, Pohlman MH, et al. Psychological factors, rehabilitation adherence, and rehabilitation outcome after anterior cruciate ligament reconstruction. Rehabilitation Psychology. 2000;45(1):20–37. doi: 10.1037/0090-5550.45.1.20. [DOI] [Google Scholar]
- 16.Engebretsen L, Steffen K, Alsousou J, Anitua E, Bachl N, Devilee R, et al. IOC consensus paper on the use of platelet-rich plasma in sports medicine. British Journal of Sports Medicine. 2010;44(15):1072–1081. doi: 10.1136/bjsm.2010.079822. [DOI] [PubMed] [Google Scholar]
- 17.Örsçeli̇K A, Yildiz Y. Comparison of single and triple platelet rich plasma injections in the treatment of patellofemoral pain syndrome. TurkiyeKlinikleri Journal of Medical Sciences. 2015;35(2):78–87. [Google Scholar]
- 18.Rha D, Park G-Y, Kim Y-K, Kim MT, Lee SC. Comparison of the therapeutic effects of ultrasound-guided platelet-rich plasma injection and dry needling in rotator cuff disease: a randomized controlled trial. Clinical Rehabilitation. 2012 doi: 10.1177/0269215512448388. [DOI] [PubMed] [Google Scholar]
- 19.Kesikburun S, Tan AK, Yılmaz B, Yaşar E, Yazıcıoğlu K. Platelet-rich plasma injections in the treatment of chronic rotator cuff tendinopathy: a randomized controlled trial with 1-year follow-up. The American Journal of Sports Medicine. 2013 doi: 10.1177/0363546513496542. [DOI] [PubMed] [Google Scholar]
- 20.Shams A, El-Sayed M, Gamal O, Ewes W. Subacromial injection of autologous platelet-rich plasma versus corticosteroid for the treatment of symptomatic partial rotator cuff tears. European Journal of Orthopaedic Surgery & Traumatology. 2016;26(8):837–842. doi: 10.1007/s00590-016-1826-3. [DOI] [PubMed] [Google Scholar]
- 21.Grassi A, Napoli F, Romandini I, Samuelsson K, Zaffagnini S, Candrian C, et al. Is platelet-rich plasma (PRP) effective in the treatment of acute muscle injuries? a systematic review and meta-analysis. Sports Medicine (Auckland, N. Z.) 2018;48(4):971–989. doi: 10.1007/s40279-018-0860-1. [DOI] [PubMed] [Google Scholar]
- 22.Ekstrand J, Hägglund M, Waldén M. Epidemiology of muscle injuries in professional football (soccer) American Journal of Sports Medicine. 2011;39(6):1226–1232. doi: 10.1177/0363546510395879. [DOI] [PubMed] [Google Scholar]
- 23.Gaweda K, Tarczynska M, Krzyzanowski W. Treatment of achillestendinopathy with platelet-rich plasma. International Journal of Sports Medicine. 2010;31(08):577–583. doi: 10.1055/s-0030-1255028. [DOI] [PubMed] [Google Scholar]
- 24.de Vos RJ, Weir A, van Schie HTM, Bierma-Zeinstra SMA, Verhaar JAN, Weinans H, et al. Platelet-Rich plasma injection for chronic achillestendinopathy: a randomized controlled trial. JAMA. 2010;303(2):144. doi: 10.1001/jama.2009.1986. [DOI] [PubMed] [Google Scholar]
- 25.Owens RF, Ginnetti J, Conti SF, Latona C. Clinical and magnetic resonance imaging outcomes following platelet rich plasma injection for chronic midsubstanceachillestendinopathy. Foot and Ankle International. 2011;32(11):1032–1039. doi: 10.3113/FAI.2011.1032. [DOI] [PubMed] [Google Scholar]
- 26.Monto RR. Platelet rich plasma treatment for chronic achillestendinosis. Foot and Ankle International. 2012;33(5):379–385. doi: 10.3113/FAI.2012.0379. [DOI] [PubMed] [Google Scholar]
- 27.Filardo G, Kon E, Di Matteo B, Pelotti P, Di Martino A, Marcacci M. Platelet-rich plasma for the treatment of patellar tendinopathy: clinical and imaging findings at medium-term follow-up. International Orthopaedics (SICOT). 2013;37(8):1583–1589. doi: 10.1007/s00264-013-1972-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Kon E, Filardo G, Delcogliano M, Presti ML, Russo A, Bondi A, et al. Platelet-rich plasma: new clinical application: a pilot study for treatment of jumper’s knee. Injury. 2009;40(6):598–603. doi: 10.1016/j.injury.2008.11.026. [DOI] [PubMed] [Google Scholar]
- 29.Lai MWW, Sit RWS. Healing of complete tear of the anterior talofibular ligament and early ankle stabilization after autologous platelet rich plasma: a case report and literature review. Archives of Bone Joint Surgery. 2018;6(2):146–149. [PMC free article] [PubMed] [Google Scholar]
- 30.Gallesio G, Del Fabbro M, Pol R, Mortellaro C, Mozzati M. Conservative treatment with plasma rich in growth factors-endoret for osteoradionecrosis. J Craniofac Surg. 2015;26(3):731–736. doi: 10.1097/SCS.0000000000001537. [DOI] [PubMed] [Google Scholar]