

ABSTRACT
Background: Posttraumatic stress disorder (PTSD) is associated with premature onset of chronic health conditions such as cardiovascular disease. Diet and exercise are behavioural contributors to physical health, and research suggests they are influenced by psychiatric symptoms, including PTSD.
Objectives: The aim of this study was to examine longitudinal associations between PTSD and exercise and diet quality and to test if emotion regulation strategies contribute to the link between PTSD and these health behaviours.
Method: A representative sample of US military veterans (n = 860 at Time 1, n = 503 at Time 2, mean age = 63 years, 91.5% male) were assessed twice over the course of approximately three years.
Results: Mediation models revealed that the association between baseline PTSD symptom severity and subsequent diet quality was mediated by emotion suppression (measured at Time 2; indirect B = −.03; 95% CI: −.059 to −.002). Trauma exposure also directly predicted diet quality (B = −.31; p = .003). There were no significant direct or indirect associations between PTSD severity or trauma exposure and exercise engagement.
Conclusions: These results suggest that PTSD symptoms are associated with worse diet quality and that the consumption of unhealthy food may be driven by efforts to suppress emotion. This carries implications for understanding and treating medical comorbidities among those with traumatic stress.
KEYWORDS: PTSD, diet, nutrition, exercise, emotion regulation
HIGHLIGHTS
• Associations between PTSD & exercise and nutrition were evaluated.
• The sample included 860 veterans at Time 1 and 503 at follow-up.
• Emotional suppression mediated the PTSD to decreased nutrition quality association.
• Addressing emotion suppression in treatment may reduce health burden of PTSD.
Antecedentes: El trastorno de estrés postraumático (TEPT) está asociado con el inicio prematuro de condiciones crónicas de salud, como la enfermedad cardiovascular. La dieta y el ejercicio son contribuyentes conductuales para la salud física y las investigaciones sugieren que están influenciados por los síntomas psiquiátricos, incluyendo al TEPT.
Objetivos: El objetivo de este estudio fue el de evaluar las asociaciones longitudinales entre el TEPT y el ejercicio y la calidad de la dieta; asimismo, evaluar si las estrategias de regulación emocional contribuyen al vínculo entre el TEPT y estas conductas de salud.
Métodos: Se evaluó a una muestra representativa de veteranos de guerra estadounidenses (n = 860 en el Tiempo 1, n = 503 en el Tiempo 2, edad promedio = 63 años, 91,5% varones) en dos oportunidades en un periodo de tres años.
Resultados: Los modelos de mediación mostraron que la asociación entre la severidad de los síntomas del TEPT de base y la calidad subsecuente de la dieta estaba mediada por la supresión de emociones (medidos en el Tiempo 2; B indirecta = −.03; 95% CI: − .059 to − .002). La exposición al trauma también predijo la calidad de la dieta de manera directa (B = = −.31; p = .003). No se encontraron asociaciones, directas o indirectas, entre la severidad del TEPT o la exposición al trauma con el compromiso con el ejercicio.
Conclusiones: Estos resultados sugieren que los síntomas del TEPT están asociados a una peor calidad de la dieta y que el consumo de alimentos no saludables puede estar impulsado por esfuerzos para suprimir las emociones. Esto conlleva a implicaciones para comprender y tratar las comorbilidades médicas entre aquellos con estrés traumático.
Palabras clave: TEPT, Dieta, Nutrición, Ejercicio, Regulación Emocional
背景:创伤后应激障碍 (PTSD) 与慢性健康疾病 (如心血管疾病) 的提前发作有关。饮食和运动是影响身体健康的行为因素, 研究表明, 饮食和运动会受到包括PTSD在内的精神病症状的影响。
目的:本研究旨在考查PTSD与运动和饮食质量之间的纵向联系, 并检验情绪调节策略是否有助于PTSD与这些健康行为之间的联系。
方法:一个美国退伍军人的代表性样本 (在时间点1时n = 860, 在时间点2时n = 503, 平均年龄= 63岁, 男性为91.5%) 在大约三年的过程中进行了两次评估。
结果:中介模型揭示出基线PTSD症状严重程度与随后的饮食质量之间的关联受情绪抑制 (在时间点2测量; 间接B = −.03; 95%CI:-.059至-.002) 中介。创伤暴露也直接预测饮食质量 (B = −.31; p = .003) 。PTSD严重程度或创伤暴露与运动参与之间没有显著的直接或间接关联。
结论:这些结果表明, PTSD症状与饮食质量较差有关, 不健康食品的消费可能是努力抑制情绪所致。这对于理解和治疗创伤性应激患者的共病有所启示。
关键词: PTSD, 饮食, 营养运动, 情绪调节
Posttraumatic stress disorder (PTSD) is associated with premature onset of chronic health conditions such as cardiovascular and cardiometabolic diseases (Brudey et al., 2015; Kibler, Tursich, Ma, Malcolm, & Greenbarg, 2014; Levine, Levine, & Levine, 2014; Pacella, Hruska, & Delahanty, 2013; Wolf et al., 2016). This may be a manifestation of an underlying acceleration in the pace of biological ageing (i.e. accelerated cellular ageing; Wolf et al., 2018). Negative physical health behaviours, such as poor exercise engagement and consuming non-nutritious foods that are high in sugar, saturated fats, and sodium may also contribute to this association between PTSD and accelerated ageing.
Various aspects of diet quality have been linked to PTSD in past research. In a meta-analysis of 29 cross-sectional and longitudinal studies, individuals with PTSD evidenced poorer dietary quality, lower exercise engagement, greater obesity, and more cigarette use relative to those without PTSD (van den Berk-clark et al., 2018). In particular, PTSD has been shown to be related to consuming fewer fruits in a cross-sectional mixed community/veteran sample (n = 80; Godfrey, Lindamer, Mostoufi, & Afari, 2013) and to more fast food and soda consumption among 3,181 young women who were studied cross-sectionally (Hirth, Rahman, & Berenson, 2011). These results were further supported by research demonstrating an association between PTSD and binge eating (Braun et al., 2019; Cronce, Bedard‐Gilligan, Zimmerman, Hodge, & Kaysen, 2017).
Research also suggests associations between exercise, physical activity, and PTSD. The constructs of physical activity and exercise differ from each other. Physical activity is a broader construct than exercise as it includes any activity that exerts energy, like getting out of bed, or walking to the refrigerator. Exercise, on the other hand, is more narrowly defined as a ‘planned, structured, repetitive bodily movement’ aimed at maintaining physical fitness (Caspersen, Powell, & Christenson, 1985, p. 128). In a study of 2,832 military veterans, those with probable PTSD were two times more likely to fail to engage in exercise during a given week compared to those without probable PTSD (Adams et al., 2020). Furthermore, exercise intensity (e.g. mild versus vigorous exercise) was inversely related to hyperarousal symptoms in 108 community adults with posttraumatic stress symptoms who were sampled cross-sectionally (Harte, Vujanovic, & Potter, 2015). In a study of 50,327 female nurses, decreased physical activity over the course of 20 years was associated with greater PTSD symptom severity (Winning et al., 2017). Engagement in preventative physical health behaviours, such as having a nutritious diet and adequate exercise, has also been shown to yield beneficial downstream effects for physical health and functioning in those with PTSD (Hall, Hoerster, & Yancy, 2015; Hall et al., 2019; Shivakumar, Anderson, Surís, & North, 2017).
Most studies examining associations between PTSD, diet quality, physical activity and exercise have been cross-sectional in nature, precluding temporal interpretations regarding the direction of association. Commonly, it is thought that PTSD symptoms, such as avoidance, emotional numbing, social disconnect, and sleep dysregulation, could potentiate negative physical health behaviours. Alternatively, these problematic physical health behaviours could increase PTSD symptom severity through behavioural (e.g. increased isolation and avoidance) and biological (e.g. increased inflammation and metabolic pathology) pathways, or the association could be bidirectional in nature.
The ability to regulate aversive mood states has also been shown to be related to both PTSD (Kaczkurkin et al., 2017; McLean et al., 2019; Seligowski et al., 2015) and engagement in preventative physical health behaviours (Bernstein & McNally, 2018; Holt, Lee, Morton, & Tonstad, 2014, 2015; Mezuk et al., 2017). Baseline emotion regulation difficulties have been linked to increased PTSD severity longitudinally (Pencea et al., 2020). In cross-sectional studies, thought suppression (e.g. avoiding negatively valanced cognitions), in particular, has been associated with worse PTSD symptoms (Seligowski et al., 2015). Several studies have also found associations between emotion regulation deficits, difficulties with emotional awareness and clarity, and poor diet quality (Holt et al., 2014, 2015). Similarly, rumination, which can be conceptualized as a cognitive mechanism for attempting to regulate negative cognitions and affect, has been associated with less exercise engagement (Bernstein & McNally, 2018). Thus, emotion regulation is important to both PTSD and physical health behaviours such as exercise and diet choices, and we suspect it may mediate the relationship between PTSD, diet quality and exercise engagement. Indeed, Michopoulos et al. (2015) showed that emotion dysregulation mediated the association between trauma exposure and disorganized, emotional eating behaviours in a cross-sectional study of 1,110 men and women. However, that study focused on symptoms of eating disorders, which is at the extreme end of problematic diet, and PTSD was not included in the model. Thus, it is still unclear whether emotion regulation might mediate the relationship between PTSD and diet and exercise-related physical health behaviours.
Although many different types of conscious and subconscious emotion regulation approaches are relevant to traumatized populations, this study focused on two overarching emotion regulation strategies: emotion reappraisal and emotion suppression. These explicit, declarative forms of emotion regulation are frequently the target of empirically supported treatments for PTSD. Cognitive reappraisal is a central component of Cognitive Processing Therapy for PTSD (Resick, 2001) and engagement with trauma-related emotions (as opposed to emotional suppression) is a critical piece of Prolonged Exposure therapy for PTSD (Foa & Kozak, 1986). Thus, although other forms of emotion regulation (e.g. including both conscious and, subconscious processes, potentially including dissociation) are important to this population, our aim was to examine approaches that may be the explicit focus of treatment, such that evidenced-based interventions designed to address them may, in turn, alter the physical health outcomes of traumatized individuals.
The primary aim of this study was to test whether emotion dysregulation mediated the association between PTSD and the physical health behaviours of dietary intake and exercise engagement using a longitudinal design. In particular, we focused on the emotion regulation strategies of cognitive reappraisal, defined as a form of cognitive engagement with a situation in order to construct an emotional response that alleviates its impact (Lazarus & Alfert, 1964), and expressive suppression, the act of purposefully preventing emotion expression (Gross, 1998). A second aim was to examine whether this association was replicated for trauma exposure, or if this association was specific to PTSD symptoms. We hypothesized that PTSD symptoms, rather than trauma exposure, would be linked to subsequent poor physical health behaviours via emotion dysregulation. This hypothesis was based on evidence that PTSD is stress-generative (Maniates, Stoop, Miller, Halberstadt, & Wolf, 2018; Miller & Sadeh, 2014) and that symptoms such as avoidance, hyperarousal, emotional numbing, and social disconnect might confer risk for adverse physical health behaviours (Crowell, Puzia, & Yaptangco, 2015).
1. Methods
1.1. Procedure
Data were collected via an online survey administered by the research firm GfK Knowledge Networks, Inc, which uses email to recruit participants into studies hosted on their platform. GfK uses points to incentivize study completion, and participants redeem these points for prizes, cash rewards, and raffles. Further details regarding the baseline recruitment effort and response rate is available in Wolf et al. (2017). Briefly, 1,126 trauma-exposed GfK participants from a previous study on veterans (Pietrzak & Cook, 2013) were selected to receive an invitation for participation in the survey at Time 1 (T1). A total of n = 860 participants completed surveys at T1. Those who completed the study at T1 received 50,000 points (the equivalent of 50 USD) for their participation. Because the surveys were administered online and participants were able to complete these at a convenient pace, the amount of time to complete the survey at T1 varied, with an average of 468 minutes (SD = 1477), and a median of 34.5 minutes. Because of this range, time to survey completion was included as a covariate in the analyses.
Approximately three years later, participants who completed the initial survey, and who were still active in the GfK panel, were invited to participate in a Time 2 (T2) assessment. A total of 621 invitations were sent out, and 503 participants (81% response rate) completed the study. Participants again received points equivalent to 50 USD for their participation in the survey, which took on average 628 minutes (SD = 1572), with a median of 38 minutes to complete. The sequence of the measures used in the analyses was randomized for each participant, with the exception that the PTSD measure always followed the trauma-exposure measure.
1.2. Participants
Out of those who completed the survey at T1, the majority were male (91.5%) and White, non-Hispanic (83.8%; 5.3% Hispanic; 5.2% Black, non-Hispanic). The average age reported in the sample at T1 was 63 years (SD = 12.3), with a range of 22 to 96 years. Of the participants returning for T2, 92.6% identified as male, and 85.9% identified as White, non-Hispanic. Participants who completed T2 did not differ as a function of minority status, age, gender, or PTSD severity (all p > .06) compared to T1 participants who did not complete the T2 assessment. The final sample size differed slightly across analyses due to missing data, (n = 487 for diet-related models and n = 474 for exercise-related models).
1.3. Measures
1.3.1. National Stressful Events Survey (NSES; Kilpatrick, Resnick, Baber, Guille, & Gros, 2011)
Data regarding trauma exposure and PTSD symptoms were collected at T1 using the NSES which assesses exposure to traumatic events and the severity of both past month and lifetime PTSD symptoms. This information is assessed in a two-part process: first, individuals are asked if they have experienced a certain symptom at all, and if endorsed, they are asked if they experienced the symptom within the past month. If so, they are prompted to rate the extent to which that symptom was bothersome on a scale from 1 (‘not at all’) to 5 (‘extremely’). These analyses were based on total lifetime symptom severity (a count of the number of dichotomous lifetime PTSD symptoms endorsed). To receive a probable lifetime PTSD diagnosis, participants had to: (1) endorse symptoms per the DSM-5 criteria; and (2), report significant distress on at least one functional impairment item. The NSES DSM-5 PTSD severity scores correlate strongly with an established measure of DSM-IV-TR PTSD symptom severity (r = .82; Miller et al., 2013). The factor structure of the measure also aligns well with the implied structure in the DSM-5, with a coefficient alpha for the current severity ratings of α = .95 in both a community and veteran sample (Miller et al., 2013). Cronbach’s alpha in these data was α = .92 for the lifetime PTSD severity scale at T1.
1.3.2. Rapid Eating Assessment for Patients (REAP; Gans et al., 2003)
The REAP, which was administered at T2 only, is a 31-item self-report measure aimed at quickly assessing dietary intake and quality during a typical week. It divides diet into eleven separate food groups and assesses frequency of consumption for each type of food in a given week. The categories included grains, fruits and vegetables, dairy, meats, fried foods, snacks, fats and oils, sweets, soft drinks, sodium, and alcohol. We also amended the measure to include an item that assessed fast food consumption, which we included in our total scores. In addition to assessing consumption of these food types, this measure also includes questions about the frequency of meals, and level of exercise engagement (this latter scale was not used in this study as it was not comprehensive enough – instead we employed a stand-alone exercise measure, as described below). Lower scores on this measure indicate poorer diet quality (The phrasing of items assessing fruit and vegetable consumption was reverse worded). In the validation study of 94 participants, the measure evidenced good reliability, with a three-week test-retest coefficient of r = 0.86 (Gans et al., 2006). The coefficient alpha in our sample was α = .72. The REAP has previously demonstrated good content and convergent validity, as evidenced by its alignment with dietary guidelines set forth by the U.S. Department of Agriculture, Center for Nutrition, Policy and Promotion (1996) and US Department of Agriculture, US Department of Health and Human Services (2000) and its moderate correlation with the Healthy Eating Index (r = 0.49; Gans et al., 2006).
1.3.3. Godin Leisure-time Exercise Questionnaire (GLTEQ; Godin & Shephard, 1997)
The GLTEQ, administered at T2 only, evaluates exercise engagement during the past 7 days. The GLTEQ is comprised of three parts that assess an individual’s engagement in 15 minutes or more of strenuous (e.g. jogging), moderate (e.g. fast walking), or mild (e.g. yoga) intensity exercise in a given week. Participants report the number of times per week that they engaged in each type of exercise. Each category is then scored, with weights assigned according to the amount of effort exerted during each activity. Each type of exercise is weighted by its own coefficient: strenuous activity by 9, moderate by 5, and mild by 3. Weighted scores for each type of activity are then summed to create a total score. A total score of 24 or greater suggests an active lifestyle, while a score under 14 indicates a sedentary lifestyle (Godin, 2011). This measure was validated by comparing scores against the percentage of body fat and maximum oxygen intake of participants, which was used to define overall fitness (Godin & Shephard, 1985). The GLTEQ displayed weak but significant associations with oxygen intake (r = 0.24; p < .05) and body fat (r = 0.21; p < .05), suggesting construct validity with physiological measures known to relate to exercise engagement. The average test-retest reliability over a two-week interval was good in a sample of 306 healthy adults (r = 0.63) across the strenuous, moderate and mild scales (Godin & Shephard, 1985). The coefficient alpha in this study was α = .47, which is below standard cut-offs but likely due to the fact that that individuals who participate in one type of exercise are not necessarily expected to participate in other types of exercise as well.
1.3.4. Emotion Regulation Questionnaire (ERQ; Gross & John, 2003)
The ERQ (T2 data were used for these analyses) measures a participant’s propensity to regulate their emotions through either cognitive reappraisal or emotion suppression, which are the two subscales in the measure (i.e. Reappraisal and Suppression, respectively). The ERQ consists of ten statements that assess the individual’s method of coping with negative and positive emotions, with each item rated on a scale from 1 (‘strongly disagree’) to 7 (‘strongly agree’). The initial validation of the measure was conducted in a sample of 1,483 undergraduates. The test-retest reliability over three months in that sample was good, with r = .69 for both scales. Across four different samples, the mean cognitive reappraisal scale alpha was .79, while the mean emotional suppression alpha was .73 (Gross & John, 2003). In this study, the coefficient alphas were α = .90 for the Reappraisal subscale, and α = .78 for the Suppression subscale. The questionnaire has previously demonstrated adequate convergent and discriminant validity with other measures of emotion regulation (Gross & John, 2003).
1.4. Data analyses
First, we examined the descriptive statistics on all key variables and the bivariate correlations among them. We then used the SPSS Process Macro (version 3.4; Hayes, 2017) to test the indirect effects of trauma and PTSD on eating and exercise habits via emotion regulation. This mediation model (‘model 4’ per Hayes, 2017) examined the indirect effect of trauma exposure or PTSD severity through two different mediators (emotion reappraisal and emotion suppression) on our dependent variables (eating habits/exercise engagement). The model was estimated four times with 5000 bootstrapped samples in each model (one model for each dependent variable and one model for PTSD controlling for trauma and one for trauma controlling for PTSD as the Process macro does not allow estimation of simultaneous indirect effects for multiple predictor variables). Demographic, health, and methodological variables (i.e. age, gender, race, BMI and survey time to completion at T2) were included as covariates of each dependent variable (i.e. mediators and eating habits/exercise engagement). The final sample size differed slightly between the REAP (n = 487) and GLTEQ (n = 474) analyses due to missing data and the exclusion of two GLTEQ outliers that were leverage points.
2. Results
2.1. Descriptive statistics and bivariate correlations
Descriptive statistics and bivariate correlations pertaining to all variables of interest are reported in Table 1. The prevalence of lifetime PTSD diagnosis at T1 was 16.5% (n = 142). In terms of demographic differences in key variables, self-reported racial minority status was associated with a greater number of lifetime traumatic events (r = .088, p < .01) and more severe PTSD symptoms at T1 (r = .199, p < .01). Being White was associated with more engagement in emotion reappraisal (r = -.094, p < .05). Sex was also correlated with PTSD severity, with women endorsing more symptoms (r = .209, p < .01) and less emotion suppression (r = −.108, p < .05). These demographic variables were included as covariates in all regression models.
Table 1.
Descriptive statistics and bivariate correlations among variables included in mediation models
| Descriptive Statistics |
Bivariate Correlations (Pearson’s r) |
|||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Variable | % | Mean (SD) | Median | Range | 1 | 2 | 3 | 4 | 5 | 6 |
| Age, years | 62.88 (11.78) | 64 | 23–89 | −.316** | −.192** | .003 | −.087 | −.083 | .038 | |
| Sex (male) | 92.6 | .209** | −.005 | .024 | .053 | .098* | −.108* | |||
| Race (White) | 85.8 | .199** | .088** | −.082 | −.022 | −.094* | .045 | |||
| BMI | 29.66 (5.74) | 28.58 | 13.65–57.39 | .106* | .097* | −.073 | −.182** | .089* | .013 | |
| 1. T1 Lifetime PTSD Severity | 4.79 (5.36) | 3 | 0–22 | |||||||
| 2. T1 Number of lifetime traumas | 2.43 (3.51) | 1 | 0–30 | .391** | ||||||
| 3. T2 REAP total score | 49.64 (7.44) | 50 | 25–68 | −.099* | −.159** | |||||
| 4. T2 GLTEQ total score | 23.31 (21.38) | 19 | 0–119 | −.012 | .042 | .200** | ||||
| 5. T2 Emotion Reappraisal | 26.95 (6.46) | 27 | 6–42 | .053 | .094* | .016 | .041 | |||
| 6. T2 Emotion Suppression | 14.89 (4.43) | 15 | 4–28 | .094* | .026 | −.123** | −.075 | .279** | ||
N = 501. SD = Standard Deviation; BMI = Body Mass Index; PTSD = Posttraumatic Stress Disorder; REAP = Rapid Eating Assessment for Patients; GLTEQ = Godin Leisure-Time Exercise Questionnaire; T1 = Time 1; T2 = Time 2.
*p < .05; **p < .01.
2.2. Mediation models
2.2.1. Diet quality
The first mediation model examined the indirect effects of T1 lifetime PTSD symptom severity on T2 Diet Quality via T2 emotion suppression and cognitive reappraisal, controlling for T1 lifetime trauma exposure, age, sex, minority status, time to complete the T2 survey, and T2 BMI. Results of this model are shown in Figure 1(a) and Table 2. T1 PTSD did not evidence direct effects on diet quality (B = −.04, p = .62), but it was associated with increased emotion suppression (B = .11, p = .01), which in turn was associated with poorer diet quality (B = −.23, p = .005). The indirect effect of T1 PTSD symptoms on T2 eating behaviour via T2 emotion suppression was significant, B = −.03; 95% CI [−.059, −.002]. In contrast, PTSD was not associated with cognitive reappraisal (B = .01, p = .88), and cognitive reappraisal was not associated with diet quality. Thus, PTSD symptom severity was associated with poorer diet quality through the emotion regulation strategy of emotion suppression. This model explained 5.8% of the variance in diet quality, 2.6% of the variance in emotion suppression, and 4.1% of the variance in emotion reappraisal. A significant covariate effect of trauma exposure on poorer diet quality also emerged (Table 2).
Figure 1.
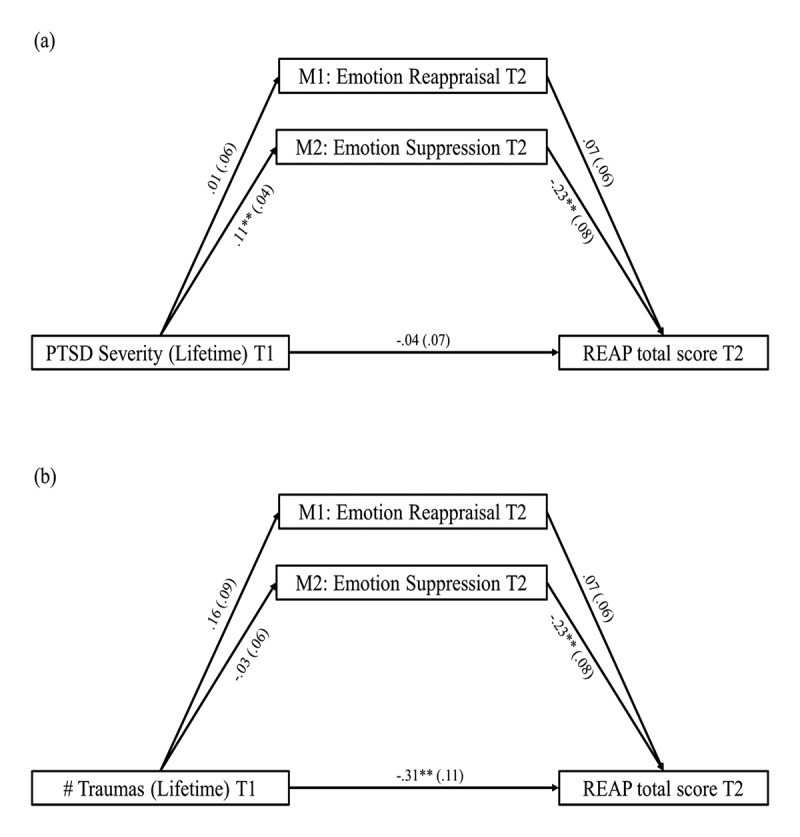
Panel A (top) shows the mediation model which examined the role of emotion regulation in the relation between PTSD severity at T1 and diet quality at T2. Panel B (bottom) shows the role of emotion regulation in mediating the relation between number of lifetime traumatic events (measured at T1) and T2 diet quality. Coefficients reported are unstandardized betas, with standard error reported in parentheses. Indirect effects in Panel A: via emotion reappraisal: B = .001 (.01), 95% CIs [−.012, .013]; via emotion suppression: B = −.03 (.02), 95% CIs [−.059, −.002]. Indirect effects in Panel B: via emotion reappraisal: B = .012 (.01), 95% CIs [−.006, .040]; via emotion suppression: B = .007 (.02), 95% CIs [−.029, .047]. Age, sex, race, BMI, and T2 duration were included as covariates of REAP total score and both mediators. These parameter estimates are listed in Table 2. M1 = Mediator 1; M2 = Mediator 2; T1 = Time 1; T2 = Time 2; REAP = Rapid Eating Assessment for Patients. *p < .05; **p < .01
Table 2.
Parameter estimates for models predicting T2 diet quality via emotion regulation
| Emotion Reappraisal |
Emotion Suppression |
Diet Quality |
||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Predictor Variable | Ba | SE | 95% CI | P | Ba | SE | 95% CI | p | Ba | SE | 95% CI | p |
| T1 PTSD Lifetime Severity | 0.01 | 0.06 | [−0.11, 0.13] | .879 | 0.11 | 0.04 | [0.03, 0.20] | .010 | −0.04 | 0.07 | [−0.18, 0.11] | .619 |
| T1 # of Lifetime Traumas | 0.16 | 0.09 | [−0.02, 0.34] | .078 | −0.03 | 0.06 | [−0.15, 0.09] | .627 | −0.31 | 0.11 | [−0.52, −0.11] | .003 |
| Age | −0.03 | 0.03 | [−0.09, 0.02] | .277 | 0.02 | 0.02 | [−0.02, 0.05] | .436 | −0.03 | 0.03 | [−0.09, 0.04] | .406 |
| Sex | 2.24 | 1.17 | [−0.05, 4.53] | .055 | −1.70 | 0.80 | [−3.28, −0.13] | .034 | 0.29 | 1.35 | [−2.37, 2.95] | .832 |
| Race | −2.29 | 0.86 | [−3.97, −0.60] | .008 | 0.49 | 0.59 | [−0.67, 1.64] | .410 | −1.19 | 0.99 | [−3.14, 0.77] | .234 |
| BMI | 0.08 | 0.05 | [−0.03, 0.18] | .143 | 0.01 | 0.04 | [−0.06, 0.08] | .783 | −0.09 | 0.06 | [−0.21, 0.03] | .130 |
| Time to complete survey | 0.0001 | 0.0002 | [−0.0003, 0.0005] | .633 | <0.0001 | 0.0001 | [−0.0003, .0002] | .972 | 0.0003 | 0.0002 | [−0.0001, 0.0007] | .158 |
| Emotion Reappraisal | 0.07 | 0.06 | [−0.04, 0.18] | .193 | ||||||||
| Emotion Suppression | −0.23 | 0.08 | [−0.38, −0.07] | .005 | ||||||||
N = 487; REAP = Rapid Eating Assessment for Patients; CI = Confidence Interval; SE = Standard Error; BMI = Body Mass Index; PTSD = Posttraumatic Stress Disorder. aAll beta values are unstandardized. There were two different models investigated, one PTSD-focused and the other trauma exposure-focused. The columns in this table represent the three different dependent variables (two mediators and one final endogenous variable) in these models. Each model was examined with the same covariates (age, gender, race, BMI, and survey completion time), using two different mediators: Emotion suppression and emotion reappraisal.
The second model with diet quality as the outcome examined the indirect effects of trauma exposure via emotion regulation strategies, controlling for T1 PTSD symptom severity scores and the covariates listed above. Results are shown in Figure 1(b) and Table 2. This model revealed direct effects of trauma exposure on diet quality (B = −.31, p = .003), but no significant effects of trauma exposure on either emotion regulation variable, meaning there can be no significant indirect effects. Therefore, experiencing a higher number of traumatic events (over a lifetime) was directly associated with poorer diet quality.
2.2.2. Exercise
Next, we examined indirect effects of PTSD on exercise engagement. Results for this model are shown in Table 3. As displayed in Figure 2(a), T1 PTSD symptom severity did not have a significant direct effect on T2 exercise habits, after controlling for number of lifetime traumas and the other covariates. Although PTSD was associated with emotion suppression, neither emotion regulation strategy was associated with exercise habits. Thus, there were no significant indirect effects.
Table 3.
Parameter estimates for models predicting T2 exercise engagement via emotion regulation
| Emotion Reappraisal |
Emotion Suppression |
Exercise Engagement |
||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Predictor Variable | Ba | SE | 95% CI | P | Ba | SE | 95% CI | p | Ba | SE | 95% CI | p |
| T1 PTSD Lifetime Severity | −0.008 | 0.06 | [−0.13, 0.11] | .896 | 0.10 | 0.04 | [0.02, 0.19] | .019 | −0.16 | 0.21 | [−0.57, 0.24] | .425 |
| T1 # of Lifetime Traumas | 0.10 | 0.10 | [−0.09, 0.29] | .305 | −0.08 | 0.07 | [−0.21, 0.05] | .224 | 0.28 | 0.32 | [−0.35, 0.91] | .382 |
| Age | −0.03 | 0.03 | [−0.08, 0.03] | .332 | 0.01 | 0.02 | [−0.02, 0.05] | .463 | −0.24 | 0.09 | [−0.42, −0.06] | .010 |
| Sex | 2.28 | 1.15 | [0.01, 4.55] | .049 | −1.66 | 0.80 | [−3.22, −0.09] | .038 | 1.48 | 3.83 | [−6.04, 8.99] | .700 |
| Race | −2.18 | 0.86 | [−3.87, −0.50] | .011 | 0.60 | 0.59 | [−0.57, 1.76] | .313 | −2.17 | 2.84 | [−7.74, 3.40] | .445 |
| BMI | 0.07 | 0.05 | [−0.03, 0.18] | .150 | 0.01 | 0.04 | [−0.06, 0.08] | .767 | −0.79 | 0.17 | [−1.12, −0.45] | .0000 |
| Time to complete survey | 0.0001 | 0.0002 | [−0.0003, 0.0005] | .525 | 0.0000 | 0.0001 | [−0.0002, 0.0003] | .919 | −0.0003 | 0.0006 | [−0.002, 0.001] | .587 |
| Emotion Reappraisal | 0.21 | 0.16 | [−0.10, 0.52] | .179 | ||||||||
| Emotion Suppression | −0.38 | 0.23 | [−0.83, 0.07] | .100 | ||||||||
N = 474; GLTEQ = Golden Leisure-Time and Exercise Questionnaire; CI = Confidence Interval; SE = Standard Error; BMI = Body Mass Index. aAll beta values are unstandardized. There were two different models investigated, one PTSD-focused and the other trauma exposure-focused. The columns in this table represent the three different dependent variables (two mediators and one final endogenous variable) in these models. Each model was examined with the same covariates (age, gender, race, BMI, and survey completion time), using two different mediators: Emotion suppression and emotion reappraisal.
Figure 2.
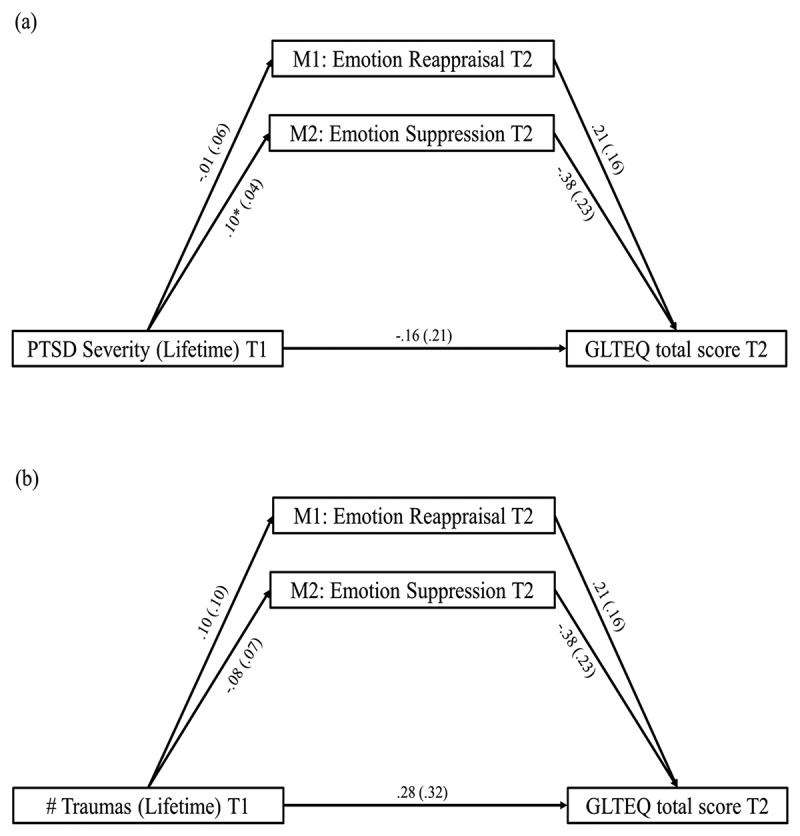
Panel A (top) shows the results of the mediation model which examined the role of emotion regulation in the relation between PTSD severity at T1 and exercise engagement at T2. Panel B (bottom) examined the role of emotion regulation in mediating the relation between number of lifetime traumatic events (measured at T1) and T2 exercise engagement. Coefficients reported are unstandardized betas, with standard error reported in parentheses. Indirect effects in Panel A: via emotion reappraisal: B = −.002 (.02), 95% CIs [−.046, .030]; via emotion suppression: B = −.038 (.03), 95% CIs [−.113, .010]. Indirect effects in Panel B: via emotion reappraisal: B = .021 (.03), 95% CIs [−.027, .100]; via emotion suppression: B = .031 (.04), 95% CIs [−.023, .128]. Age, sex, race, BMI, and T2 duration were included as covariates of GLTEQ total score and both mediators. These parameter estimates are listed in Table 3. M1 = Mediator 1; M2 = Mediator 2; T1 = Time 1; T2 = Time 2; GLTEQ = Godin Leisure-Time Exercise Questionnaire. *p < .05; **p < .01
The final model examined the indirect effect of trauma exposure on exercise habits via T2 emotion reappraisal and emotion suppression, while controlling for T1 PTSD symptom severity and the same covariates mentioned above (see Figure 2(b)). As observed in the correlations in Table 1, trauma exposure did not have a significant direct effect on T2 exercise engagement. In this model, number of lifetime traumatic events was not associated with either emotion regulation strategy, and neither of these was associated with exercise engagement; thus, there were no significant indirect effects evident in this model. Each mediation model was estimated with and without the aforementioned covariates, and the overall pattern of results remained unchanged.
3. Discussion
Results of our analyses revealed that efforts to regulate emotion through suppression mediated the association between T1 PTSD severity and later diet quality, which is consistent with two separate lines of research suggesting associations between PTSD and emotion regulation (Kaczkurkin et al., 2017; McLean et al., 2019) and emotion regulation and eating habits (Holt et al., 2014). These findings suggest that people who experience worse PTSD symptoms may eat poorer quality foods as a way to reduce their emotional burden. This, in turn, could partially explain the relation between PTSD, cardiometabolic health and accelerated ageing (Wolf et al., 2016, 2019). While the association between PTSD and eating behaviour was indirect via emotional suppression, the number of lifetime traumatic experiences was directly associated with poor diet, even after controlling for the effects of PTSD. Therefore, both trauma exposure and PTSD are important and independent contributors to diet quality.
Despite these associations with diet, neither PTSD severity nor trauma exposure directly or indirectly was associated with exercise habits. Although these results for exercise engagement were not consistent with our hypotheses, they are not surprising, as the results of prior studies concerning this association have been equivocal. In a review of 12 studies, half did not yield evidence of a significant relationship between PTSD and exercise or physical activity (van den Berk-clark et al., 2018), while others supported an association between trauma and vigorous exercise, such that trauma-exposed individuals with lower PTSD symptom severity engaged in more vigorous forms of exercise (Harte et al., 2015). It may be that in our sample of older adults, we were unable to observe significant effects of trauma and psychiatric variables on exercise engagement because other factors, such as age and age-related ailments, were more substantial contributors to exercise in this sample.
Collectively, these results suggest that trauma exposure and PTSD severity have an impact on emotion regulation strategies and diet quality. It is possible that addressing emotion regulation difficulties among individuals with PTSD may have downstream preventative effects on adverse physical health outcomes (e.g. cardiometabolic disease) often associated with traumatic stress (Afari et al., 2014; Pacella et al., 2013). In addition to cardiometabolic conditions, diet quality has also been linked to other physical health conditions that are known to be associated with PTSD, such as dementia (Yaffe et al., 2010) and cortical thinning (Wrocklage et al., 2017). Certain foods, including those rich in vitamins E and B12 and fish, have been associated with a decreased risk for dementia (Morris, 2012; Perez, Heim, Sherzai, Jaceldo-Siegl, & Sherzai, 2012) while sugary drinks have been linked to an increased risk (Pase et al., 2017).Vitamin D, omega-3 fatty acids, and cholesterol levels are related to cortical sparing and thinning (Walhovd, Storseve, Westlye, Drevon, & Fjell, 2014). Therefore, diet quality is a common denominator among multiple physical and neurological health outcomes commonly comorbid with PTSD. In light of our results that emotion regulation mediated the relation between PTSD and diet quality, emotion regulation may offer a potential explanation as to how PTSD is associated with these physical health conditions. This raises the question of whether targeting emotion regulation can also impact these heath conditions.
In addition to showing that emotion regulation mediated the relation between PTSD and diet, our results demonstrated that the mediating effect is dependent on the specific type of emotion regulation employed. Suppressing emotions may lead to unhealthy compensatory coping mechanisms, such as eating unhealthy food, whereas experiencing and expressing emotions lessens the need to engage in such behaviours. In an experimental study comparing emotion suppression with emotion acceptance among individuals with anxiety and depression, those in the emotion suppression condition had more negative affect and increased heart rate after watching an emotionally upsetting film (Campbell-Sills, Barlow, Brown, & Hofmann, 2006). Thus, engaging in emotional suppression may lead to multiple adverse behavioural and biological outcomes that could collectively contribute to disease.
3.1. Treatment implications
Our results also carry clinical implications, as they show that it is important for nutritionists to understand how trauma exposure and trauma-related psychiatric symptoms influence diet and food choices. In particular, it may be necessary to address emotion regulation skills and PTSD in therapy in order to effectively treat poor eating habits. In a study comparing the effectiveness of the Veterans Health Administration’s weight-loss programme MOVE! in patients with and without PTSD, it was found that participants with PTSD lost less weight than those without (Hoerster et al., 2014). Thus, intervening on diet quality alone may not be sufficient if eating habits are impacted by trauma exposure and PTSD, so treatment must also address the upstream components leading to the lack of a nutritious diet.
That emotion suppression mediated the association between PTSD severity and diet could also potentially impact how clinicians move forward in their treatment plans. McLean et al. (2019) showed the important implications of emotion dysregulation on PTSD treatment outcomes. In this study, use of the emotion regulation strategy of catastrophizing was associated with reduced treatment effectiveness in response to Prolonged Exposure (PE) and Present-centred therapy (PCT), two widely-used treatments for PTSD. Thus, addressing emotion processing approaches can help predict treatment efficacy. In addition, our results suggest the importance of considering other types of therapy that could be useful in PTSD treatment. For instance, therapies that directly address emotion regulation, like mindfulness and Dialectical Behaviour Therapy (DBT; Linehan & Wilks, 2018), and Prolonged Exposure (Foa & Kozak, 1986), which requires engagement with trauma-focused emotions, could help ameliorate not only the PTSD symptoms, but problematic physical health behaviours as well.
3.2. Limitations
There are limitations to consider when interpreting the results of this study. This was a self-report, web-based study, which reduces internal control and validity. We did not use nutrition diaries, direct measurements of exercise (e.g. using an actigraph), or structured diagnostic interviews, which are the gold standard measurement approaches for these constructs and superior to self-report measures, which are vulnerable to reporting biases (Adams et al., 2005). Furthermore, a comprehensive physical activity measure was not administered, which means our index of exercise engagement may underestimate total physical activity. We also could not control how long respondents took to complete the questionnaires. However, our results did not suggest that time to study completion was associated with the dependent variables. We could not examine the reverse direction of effect (i.e. physical health behaviours to PTSD) because exercise and diet quality were not assessed at T1. The prevalence of PTSD in our sample was low, so this limited variability and may have curtailed the strength of the associations. In addition, the ERQ only assesses two broad forms of emotion regulation strategies – cognitive reappraisal and expression suppression. Other, more detailed measures, such as the Difficulties in Emotion Regulation Scale (DERS; Gratz & Roemer, 2004), and assessment of other conscious and subconscious emotion regulation strategies, could provide a more comprehensive picture of the ways in which emotion regulation may impact physical health behaviours and outcomes among traumatized populations. Finally, given that our sample was comprised primarily of an ageing sample of male veterans, the generalizability of our results is limited to this population and age-related factors and illnesses may have influenced exercise engagement and diet quality, but were not assessed in this study.
3.3. Future directions and conclusions
Based on our findings, future studies could examine whether reductions in PTSD symptoms due to treatment have downstream positive effects on diet quality. Because we were unable to test the opposite direction of effect in this study, assessment of PTSD and diet quality at each time point would allow for comparison of competing hypotheses concerning the direction of effect. Assessing additional conscious and subconscious emotion regulation techniques would also expand scientific knowledge concerning the pathways to negative physical health behaviours and may potentially point to new treatment approaches to mitigate adverse outcomes. Our results demonstrate the role of emotion regulation strategies in the association between PTSD and compromised diet and carry implications for understanding the relation between PTSD and early onset of adverse physical health outcomes. These results also raise the possibility that addressing emotion dysregulation in treatment may have positive downstream effects on physical health behaviours and physical wellness.
Funding Statement
This work was supported by the National Center for PTSD. The contents of this manuscript do not represent the views of the U.S. Department of Veterans Affairs or the USA Government.
Disclosure statement
All authors report no conflicts of interest.
Data availability statement
Participants did not consent to data sharing (as the data were collected prior to this being common), thus we are unable to share these data. However, summary statistics, analytic scripts, and analytic output are available from the corresponding author.
References
- Adams, S. A., Matthews, C. E., Ebbeling, C. B., Moore, C. G., Cunningham, J. E., Fulton, J., & Hebert, J. R. (2005). The effect of social desirability and social approval on self-reports of physical activity. American Journal of Epidemiology, 161(4), 389–12. doi: 10.1093/aje/kwi054. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Adams, T. G., Forte, J., Fogle, B. M., Southwick, S. M., & Pietrzak, R. H. (2020). Self-reported exercise frequency and PTSD: Results from the national health and resilience in veterans study. Acta Psychiatrica Scandinavica, 142, 486–495. doi: 10.1111/acps.13234. [DOI] [PubMed] [Google Scholar]
- Afari, N., Ahumada, S. M., Wright, L. J., Mostoufi, S., Golnari, G., Reis, V., & Cuneo, J. G. (2014). Psychological trauma and functional somatic syndromes: A systematic review and meta-analysis. Psychosomatic Medicine, 76(1), 2. doi: 10.1097/PSY.0000000000000010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bernstein, E. E., & McNally, R. J. (2018). Exercise as a buffer against difficulties with emotion regulation: A pathway to emotional wellbeing. Behaviour Research and Therapy, 109, 29–36. doi: 10.1016/j.brat.2018.07.010. [DOI] [PubMed] [Google Scholar]
- Braun, J., El-Gabalawy, R., Sommer, J. L., Pietrzak, R. H., Mitchell, K., & Mota, N. (2019). Trauma exposure, DSM-5 posttraumatic stress, and binge eating symptoms: Results from a nationally representative sample. The Journal of Clinical Psychiatry, 80, 6. doi: 10.4088/jcp.19m12813. [DOI] [PubMed] [Google Scholar]
- Brudey, C., Park, J., Wiaderkiewicz, J., Kobayashi, I., Mellman, T. A., & Marvar, P. J. (2015). Autonomic and inflammatory consequences of posttraumatic stress disorder and the link to cardiovascular disease. American Journal of Physiology-Regulatory, Integrative and Comparative Physiology, 309(4), R315–R321. doi: 10.1152/ajpregu.00343.2014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Campbell-Sills, L., Barlow, D., Brown, T., & Hofmann, S. (2006). Effects of suppression and acceptance on emotional responses of individuals with anxiety and mood disorders. Behaviour Research and Therapy, 44, 1251–1263. doi: 10.1016/j.brat.2005.10.001. [DOI] [PubMed] [Google Scholar]
- Caspersen, C. J., Powell, K. E., & Christenson, G. M. (1985). Physical activity, exercise, and physical fitness: Definitions and distinctions for health-related research. Public Health Reports, 100(2), 126–131. [PMC free article] [PubMed] [Google Scholar]
- Cronce, J. M., Bedard‐Gilligan, M. A., Zimmerman, L., Hodge, K. A., & Kaysen, D. (2017). Alcohol and binge eating as mediators between posttraumatic stress disorder symptom severity and body mass index. Obesity, 25(4), 801–806. doi: 10.1002/oby.21809. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Crowell, S. E., Puzia, M. E., & Yaptangco, M. (2015). The ontogeny of chronic distress: Emotion dysregulation across the life span and its implications for psychological and physical health. Current Opinion in Psychology, 3, 91–99. doi: 10.1016/j.copsyc.2015.03.023. [DOI] [Google Scholar]
- Foa, E. B., & Kozak, M. J. (1986). Emotional processing of fear: Exposure to corrective information. Psychological Bulletin, 99(1), 20. doi: 10.1037/0033-2909.99.1.20. [DOI] [PubMed] [Google Scholar]
- Gans, K. M., Risica, P. M., Wylie-Rosett, J., Ross, E. M., Strolla, L. O., McMurray, J., & Eaton, C. B. (2006). Development and evaluation of the nutrition component of the Rapid Eating and Activity Assessment for Patients (REAP): A new tool for primary care providers. Journal of Nutrition Education and Behavior, 38(5), 286–292. doi: 10.1093/jn/133.2.556S. [DOI] [PubMed] [Google Scholar]
- Gans, K. M., Ross, E., Barner, C. W., Wylie-Rosett, J., McMurray, J., & Eaton, C. (2003). REAP and WAVE: New tools to rapidly assess/discuss nutrition with patients. Journal of Nutrition, 133, 556S–562S. doi: 10.1016/j.jneb.2005.12.002. [DOI] [PubMed] [Google Scholar]
- Godfrey, K. M., Lindamer, L. A., Mostoufi, S., & Afari, N. (2013). Posttraumatic stress disorder and health: A preliminary study of group differences in health and health behaviors. Annals of General Psychiatry, 12(1), 30. doi: 10.1186/1744-859X-12-30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Godin, G. (2011). The Godin-Shephard leisure-time physical activity questionnaire. The Health & Fitness Journal of Canada, 4(1), 18–22. doi: 10.14288/hfjc.v4i1.82. [DOI] [Google Scholar]
- Godin, G., & Shephard, R. J. (1985). A simple method to assess exercise behavior in the community. Canadian Journal of Applied Sport Sciences, 10(3), 141–146. [PubMed] [Google Scholar]
- Godin, G., & Shephard, R. J. (1997). Godin leisure-time exercise questionnaire. Medicine and Science in Sports and Exercise, 29(6), S36–S38. [Google Scholar]
- Gratz, K. L., & Roemer, L. (2004). Multidimensional assessment of emotion regulation and dysregulation: Development, factor structure, and initial validation of the difficulties in emotion regulation scale. Journal of Psychopathology and Behavioral Assessment, 26(1), 41–54. doi: 10.1023/b:joba.0000007455.08539.94. [DOI] [Google Scholar]
- Gross, J. J. (1998). Antecedent-and response-focused emotion regulation: Divergent consequences for experience, expression, and physiology. Journal of Personality and Social Psychology, 74(1), 224. doi: 10.1037//0022-3514.74.1.224. [DOI] [PubMed] [Google Scholar]
- Gross, J. J., & John, O. P. (2003). Individual differences in two emotion regulation processes: Implications for affect, relationships, and well-being. Journal of Personality and Social Psychology, 85(2), 348. doi: 10.1037/0022-3514.85.2.348. [DOI] [PubMed] [Google Scholar]
- Hall, K. S., Hoerster, K. D., & Yancy, J. W. (2015). Post-traumatic stress disorder, physical activity, and eating behaviors. Epidemiologic Reviews, 37(1), 103–115. doi: 10.1093/epirev/mxu011. [DOI] [PubMed] [Google Scholar]
- Hall, K. S., Morey, M. C., Bosworth, H. B., Beckham, J. C., Pebole, M. M., Sloane, R., & Pieper, C. F. (2019). Pilot randomized controlled trial of exercise training for older veterans with PTSD. Journal of Behavioral Medicine, 1–12. doi: 10.1007/s10865-019-00073-w [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harte, C. B., Vujanovic, A. A., & Potter, C. M. (2015). Association between exercise and posttraumatic stress symptoms among trauma-exposed adults. Evaluation & the Health Professions, 38(1), 42–52. doi: 10.1177/0163278713494774. [DOI] [PubMed] [Google Scholar]
- Hayes, A. F. (2017). Introduction to mediation, moderation, and conditional process analysis: A regression-based approach. New York: Guilford Publications. [Google Scholar]
- Hirth, J. M., Rahman, M., & Berenson, A. B. (2011). The association of posttraumatic stress disorder with fast food and soda consumption and unhealthy weight loss behaviors among young women. Journal of Women’s Health, 20(8), 1141–1149. doi: 10.1089/jwh.2010.2675. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hoerster, K. D., Lai, A., Goodrich, D., Damschroder, L., Littman, A., Klingaman, E., & Kilbourne, A. M. (2014). Weight loss after participation in a national VA weight management program among veterans with or without PTSD. Psychiatric Services, 65, 1385–1388. doi: 10.1176/appi.ps.201300404. [DOI] [PubMed] [Google Scholar]
- Holt, M. E., Lee, J. W., Morton, K. R., & Tonstad, S. (2014). Mediterranean diet and emotion regulation. Mediterranean Journal of Nutrition and Metabolism, 7(3), 163–172. doi: 10.3233/MNM-140016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Holt, M. E., Lee, J. W., Morton, K. R., & Tonstad, S. (2015). Trans fatty acid intake and emotion regulation. Journal of Health Psychology, 20(6), 785–793. doi: 10.1177/1359105315580215. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kaczkurkin, A. N., Zang, Y., Gay, N. G., Peterson, A. L., Yarvis, J. S., Borah, E. V., … Young‐McCaughan, S. (2017). Cognitive emotion regulation strategies associated with the DSM‐5 posttraumatic stress disorder criteria. Journal of Traumatic Stress, 30(4), 343–350. doi: 10.1002/jts.22202. [DOI] [PubMed] [Google Scholar]
- Kibler, J. L., Tursich, M., Ma, M., Malcolm, L., & Greenbarg, R. (2014). Metabolic, autonomic and immune markers for cardiovascular disease in posttraumatic stress disorder. World Journal of Cardiology, 6(6), 455. doi: 10.4330/wjc.v6.i6.455. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kilpatrick, D. G., Resnick, H. S., Baber, B., Guille, C., & Gros, K. (2011). The National Stressful Events Web Survey (NSES-W) [Measurement instrument]. Charleston: Medical University of South Carolina. [Google Scholar]
- Lazarus, R. S., & Alfert, E. (1964). Short-circuiting of threat by experimentally altering cognitive appraisal. The Journal of Abnormal and Social Psychology, 69(2), 195. doi: 10.1037/h0044635. [DOI] [PubMed] [Google Scholar]
- Levine, A. B., Levine, L. M., & Levine, T. B. (2014). Posttraumatic stress disorder and cardiometabolic disease. Cardiology, 127(1), 1–19. doi: 10.1159/000354910. [DOI] [PubMed] [Google Scholar]
- Linehan, M., & Wilks, C. (2018). The course and evolution of dialectical behavior therapy. Psychotherapy, 69, 97–110. doi: 10.1176/appi.psychotherapy.2015.69.2.97. [DOI] [PubMed] [Google Scholar]
- Maniates, H., Stoop, T. B., Miller, M. W., Halberstadt, L., & Wolf, E. J. (2018). Stress‐generative effects of posttraumatic stress disorder: Transactional associations between posttraumatic stress disorder and stressful life events in a longitudinal sample. Journal of Traumatic Stress, 31(2), 191–201. doi: 10.1002/jts.22269. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McLean, C. P., Zang, Y., Gallagher, T., Suzuki, N., Yarvis, J. S., Litz, B. T., & Consortium, S. T. R. O. N. G. S. T. A. R. (2019). Trauma-related cognitions and cognitive emotion regulation as mediators of PTSD change among treatment-seeking active-duty military Personnel with PTSD. Behavior Therapy, 50(6), 1053–1062. doi: 10.1016/j.beth.2019.03.006. [DOI] [PubMed] [Google Scholar]
- Mezuk, B., Ratliff, S., Concha, J. B., Abdou, C. M., Rafferty, J., Lee, H., & Jackson, J. S. (2017). Stress, self-regulation, and context: Evidence from the health and retirement survey. SSM – Population Health, 3, 455–463. doi: 10.1016/j.ssmph.2017.05.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Michopoulos, V., Powers, A., Moore, C., Villarreal, S., Ressler, K. J., & Bradley, B. (2015). The mediating role of emotion dysregulation and depression on the relationship between childhood trauma exposure and emotional eating. Appetite, 91, 129–136. doi: 10.1016/j.appet.2015.03.036. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miller, M. W., & Sadeh, N. (2014). Traumatic stress, oxidative stress and post-traumatic stress disorder: Neurodegeneration and the accelerated-aging hypothesis. Molecular Psychiatry, 19(11), 1156–1162. doi: 10.1038/mp.2014.111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miller, M. W., Wolf, E. J., Kilpatrick, D., Resnick, H., Marx, B. P., Holowka, D. W., … Friedman, M. J. (2013). The prevalence and latent structure of proposed DSM-5 posttraumatic stress disorder symptoms in US national and veteran samples. Psychological Trauma: Theory, Research, Practice, and Policy, 5(6), 501. doi: 10.1037/a0029730. [DOI] [Google Scholar]
- Morris, M. C. (2012). Nutritional determinants of cognitive aging and dementia. The Proceeding of the Nutrition Society, 71, 1–13. doi: 10.1017/S0029665111003296. [DOI] [PubMed] [Google Scholar]
- Pacella, M. L., Hruska, B., & Delahanty, D. L. (2013). The physical health consequences of PTSD and PTSD symptoms: A meta-analytic review. Journal of Anxiety Disorders, 27(1), 33–46. doi: 10.1016/j.janxdis.2012.08.004. [DOI] [PubMed] [Google Scholar]
- Pase, M., Himali, J., Beiser, A., Aparicio, H., Satizabal, C., Vasan, R., … Jacques, P. (2017). Sugar- and artificially sweetened beverages and the risks of incident stroke and dementia. Stroke, 48, 1129–1146. doi: 10.1161/STROKEAHA.116.016027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pencea, I., Munoz, A. P., Maples-Keller, J. L., Fiorillo, D., Schultebraucks, K., Galatzer-Levy, I., … Powers, A. (2020). Emotion dysregulation is associated with increased prospective risk for chronic PTSD development. Journal of Psychiatric Research, 121, 222–228. doi: 10.1016/j.jpsychires.2019.12.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Perez, L., Heim, L., Sherzai, A., Jaceldo-Siegl, K., & Sherzai, A. (2012). Nutrition and vascular dementia. The Journal of Nutrition, Health & Aging, 16, 319–324. doi: 10.1007/s12603-012-0042-z. [DOI] [PubMed] [Google Scholar]
- Pietrzak, R. H., & Cook, J. M. (2013). Psychological resilience in older U.S. veterans: Results from the national health and resilience in veterans study. Depression and Anxiety, 30, 432–443. doi: 10.1002/da.22083. [DOI] [PubMed] [Google Scholar]
- Resick, P. A. (2001). Cognitive therapy for posttraumatic stress disorder. Journal of Cognitive Psychotherapy, 15(4), 321–329. [Google Scholar]
- Seligowski, A. V., Lee, D. J., Bardeen, J. R., & Orcutt, H. K. (2015). Emotion regulation and posttraumatic stress symptoms: A meta-analysis. Cognitive Behaviour Therapy, 44(2), 87–102. doi: 10.1080/16506073.2014.980753 [DOI] [PubMed] [Google Scholar]
- Shivakumar, G., Anderson, E. H., Surís, A. M., & North, C. S. (2017). Exercise for PTSD in women veterans: A proof-of-concept study. Military Medicine, 182(11–12), e1809–e1814. doi: 10.7205/MILMED-D-16-00440. [DOI] [PubMed] [Google Scholar]
- U.S. Department of Agriculture, Center for Nutrition, Policy and Promotion . (1996). The food guide pyramid (Home and garden bulletin no. 252). Retrieved from http://www.usda.gov/cnpp/pyramid2.htm
- US Department of Agriculture, US Department of Health and Human Services . (2000). Nutrition and your health: Dietary guidelines for Americans. Retrieved from https://www.hhs.gov/fitness/eat-healthy/dietary-guidelines-for-americans/index.html
- van den Berk-clark, C., Secrest, S., Walls, J., Hallberg, E., Lustman, P. J., Schneider, F. D., & Scherrer, J. F. (2018). Association between posttraumatic stress disorder and lack of exercise, poor diet, obesity, and co-occuring smoking: A systematic review and meta-analysis. Health Psychology, 37(5), 407. doi: 10.1037/hea0000593. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Walhovd, K., Storseve, A., Westlye, L., Drevon, C., & Fjell, A. (2014). Blood markers of fatty acids and vitamin D, cardiovascular measures, body mass index, and physical activity relate to longitudinal cortical thinning in normal aging. Neurobiology of Aging, 35, 1055–1064. doi: 10.1016/j.neurobiolaging.2013.11.011. [DOI] [PubMed] [Google Scholar]
- Winning, A., Gilsanz, P., Koenen, K. C., Roberts, A. L., Chen, Q., Sumner, J. A., … Kubzansky, L. D. (2017). Post-traumatic stress disorder and 20-year physical activity trends among women. American Journal of Preventive Medicine, 52(6), 753–760. doi: 10.1016/j.amepre.2017.01.040. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wolf, E. J., Bovin, M. J., Green, J. D., Mitchell, K. S., Stoop, T. B., Barretto, K. M., … Rosen, R. C. (2016). Longitudinal associations between post-traumatic stress disorder and metabolic syndrome severity. Psychological Medicine, 46, 2215–2226. doi: 10.1017/S0033291716000817. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wolf, E. J., Maniates, H., Nugent, N., Maihofer, A. X., Armstrong, D., Ratanatharathorn, A., & Logue, M. W.; Workgroup, V. M. A. M. . (2018). Traumatic stress and accelerated DNA methylation age: A meta-analysis. Psychoneuroendocrinology, 92, 123–134. doi: 10.1016/j.psyneuen.2017.12.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wolf, E. J., Mitchell, K. S., Sadeh, N., Hein, C., Fuhrman, I., Pietrzak, R. H., & Miller, M. W. (2017). The dissociative subtype of PTSD scale: Initial evaluation in a national sample of trauma-exposed veterans. Assessment, 24(4), 503–516. doi: 10.1177/1073191115615212. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wolf, E. J., Morrison, F. G., Sullivan, D. R., Logue, M. W., Guetta, R. E., Stone, A., & Miller, M. W. (2019). The goddess who spins the thread of life: Klotho, psychiatric stress, and accelerated aging. Brain, Behavior, and Immunity, 80, 193–203. doi: 10.1016/j.bbi.2019.03.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wrocklage, K. M., Averill, L. A., Cobb Scott, J., Averill, C. L., Schweinsburg, B., Trejo, M., … Abdallah, C. G. (2017). Cortical thickness reduction in combat exposed U.S. veterans with and without PTSD. European Neuropsychopharmacology: The Journal of the European College of Neuropsychopharmacology, 27, 515–525. doi: 10.1016/j.euroneuro.2017.02.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yaffe, K., Vittinghoff, E., Lindquist, K., Barnes, D., Covinsky, K., Neyland, T., … Marmar, C. (2010). Posttraumatic stress disorder and risk of dementia among US veterans. Archives of General Psychiatry, 67, 608–613. doi: 10.1001/archgenpsychiatry.2010.61. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Participants did not consent to data sharing (as the data were collected prior to this being common), thus we are unable to share these data. However, summary statistics, analytic scripts, and analytic output are available from the corresponding author.