
Figure 1. P. falciparum interactions with the vasculature along its life cycle.
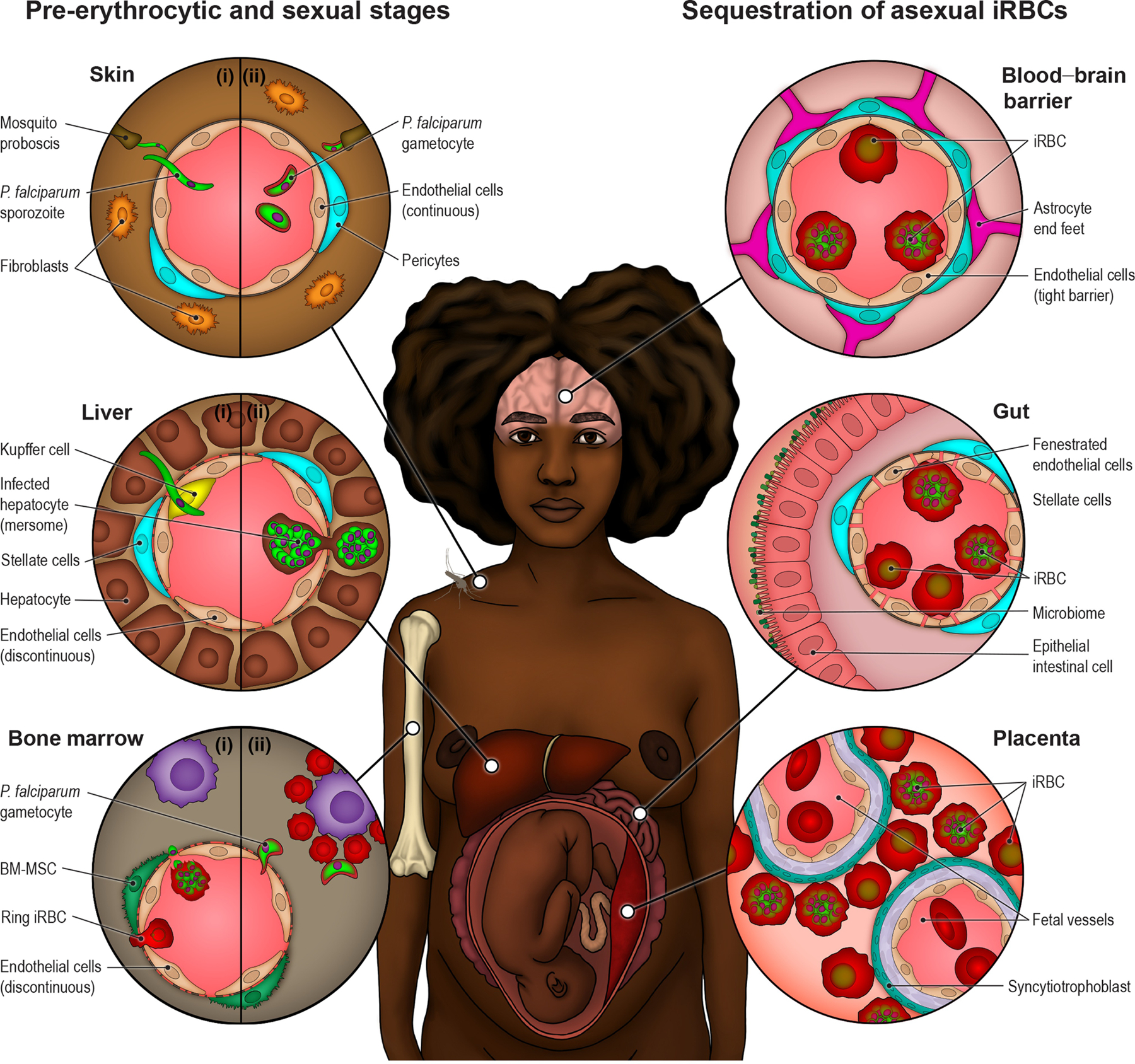
Top left circle (Skin): P. falciparum parasites interact with skin blood vessels when initiating infection (I) and during transmission back to mosquitoes (II). The molecular mechanism of sporozoite crossing across blood vessels or whether mature gametocytes accumulate in skin capillaries remains unknown. Middle left circle (Liver): sporozoites arrest on endothelial cells in the liver and cross the liver sinuosoidal barrier probably through Kupffer cells to infect hepatocytes (I). There, they will asexually multiply into thousands of merozoites that will be released back to bloodstream through budding of membranous structures known as merosomes, containing merozoite parasite forms (II). Left bottom circle (Bone Marrow): P. falciparum sexual development occurs in the bone marrow. Immature ring stage iRBC or merozoites, asexual or sexually committed, have been proposed as candidates to cross the discontinuous bone marrow vasculature (I). Early stage gametocye-iRBCs mature on erythroblastic islands until they re-enter the blood circulation as less-rigid stage V gametocyte-iRBCs (II). Asexual P. falciparum-iRBC sequester in the microvasculature to avoid splenic clearance. There is widespread sequestration in fatal cases. Top right circle (Blood-Brain Barrier): P. falciparum accumulation in the brain is highly pathogenic due to inherent properties of the blood-brain barrier to protect neuronal function. Middle right circle (Gut): One of the main parasite sequestration sites is the gut fenestrated microvasculature, which may contribute to high parasite biomass. Right bottom circle (Placenta): During pregnancy, P. falciparum-iRBCs accumulate in the maternal intervillous space and attached to the syncytiotrophoblast lining in the placenta.