

Abstract
Introduction:
An interprofessional consultation (eConsult) is an asynchronous form of telehealth whereby a primary care provider requests electronic consultation with a specialist in place of an in-person consultation. While eConsults have been successfully implemented in many medical specialties, their use in the practice of urology is relatively unknown.
Methods:
We included data from four academic institutions: University of Michigan, University of California —San Francisco, University of Washington, and Montefiore Medical Center. We included every urological eConsult performed at each institution from the launch of their respective programs through August 2019. We considered an eConsult “converted” when the participating urologist recommended a full in-person evaluation. We report eConsult conversion rate, response time, completion time, and diagnosis categories.
Results:
A total of 462 urological eConsults were requested. Of these, 36% were converted to a traditional in-person visit. Among resolved eConsults, with data on provider response time available (n=119),53.8% of eConsults were addressed in less than 1 day; 28.6% in 1 day; 8.4% in 2 days; 3.4% in 3 days; 3.4% in 4 days; 1.7% in 5 days; and 0.8% in ≥6 days. Among resolved eConsults, with data on provider completion time available (n=283), 50.2% were completed in 1-10 minutes; 46.7% in 11-20 minutes; 2.8% in 21-30 minutes; and less than 1% in ≥31 minutes.
Discussion:
Our study suggests that eConsults are an effective avenue for urologists to provide recommendations for many common non-surgical urological conditions and thus avoid a traditional in-person for low-complexity situations. Further investigation into the impact of eConsults on healthcare costs and access to urological care are necessary.
INTRODUCTION
As the patient population continues to age, there will be a growing need for urological services.1,2However, due to a shortage of urologists, the current medical workforce will have difficulty meeting this need:3By 2035, there will be 46% fewer urologists in the United States than the estimated need.3One possible solution to meet the growing demand for urological care is the implementation of interprofessional consultations (eConsults). The Centers for Medicare & Medicaid Services define an eConsult as an “interprofessional telephone/internet/electronic health record assessment and management service provided by a consultative physician including a written report to the patient’s treating/requesting physician or other qualified healthcare professional”.4Over the last several years, a number of institutions have successfully introduced eConsult programs, and have found them effective at reducing the number of traditional in-person consultations with subspecialists, such as cardiology and dermatology.5,6In 2019, Medicare began reimbursing physicians for eConsults, and many commercial payers have since followed.
Urology interprofessional consults have previously been studied at safety-net hospitals both as a screening tool prior to in-person evaluation and as true eConsults where patients were only evaluated in-person if needed.7,8eConsults were also implemented by some providers during the COVID-19 Pandemic.9However, there is limited knowledge of eConsult use outside of safety net hospitals and during non-pandemic periods. It is critical to understand the landscape of urological eConsult programs as health systems consider whether to implement them to mitigate the impending provider shortage. eConsults may offer an avenue for urologists to screen requests from primary care providers, provide treatment recommendations for simple cases, and prioritize in-person consultation for high-complexity surgical patients. eConsults may also be efficient alternatives for patients. However, given the diversity of existing urological conditions and depth of physical examination needed to appropriately address these conditions, eConsults alone may be insufficient to provide recommendations for some patients.
Limited research in this area has found that a urological eConsult program can indeed improve access to urological care in many clinical scenarios and with high physician-rated satisfaction.10Our work will build on this data by evaluating urological eConsult programs at four large healthcare systems. We hypothesize that, in a majority of cases in which a urological eConsult is requested, the urologist will be able to provide recommendations without the need for escalation to a traditional in-person visit.
METHODS
We collected our data from the eConsult programs at four institutions: University of Michigan in Ann Arbor, University of California - San Francisco, University of Washington in Seattle, and Montefiore Medical Center in The Bronx, New York. These programs launched in February 2019, December 2016, July 2018, and April 2019, respectively. The majority of the support for the eConsult program is provided by the health system at each institution, with primary care and specialty departments serving as participants in the service. In order to request an eConsult, a provider must be a primary care provider who is affiliated with the institution from which the eConsult is being requested. There were no other provider or patient restrictions in place. In this study, we included all eConsults initiated from a referring provider to a urologist from the start of each program through August 2019.
Our primary objective was to perform a descriptive analysis of all urological eConsults requested by referring providers across the four institutions. Thus, we measured the total number of urological eConsults that were “resolved” (i.e., the urologist made a treatment recommendation with no further urologic evaluation) and those “converted” (i.e., the urologist did not offer definitive diagnostic or treatment advice but instead recommended that the patient seek a traditional in-person visit). We also calculated the conversion rate at each institution. In addition, we sought to illustrate the types of urological diagnoses for which eConsults were used, as well as to identify which were most common. To complete this aim, we categorized and tallied all urological eConsults in the study period by diagnosis codes.
We also aimed to assess the efficiency and clinical value of urological eConsults. Therefore, our secondary outcomes included measures such as provider “response time” and “completion time.” Each institution in our study collected slightly different measures from their eConsult programs; when available, we examined “response time,” defined as the amount of time elapsed (in days) from the initial eConsult request to the urologist response. We also examined “completion time” defined as the amount of time spent by a urologist to complete an eConsult request, which specifically included the time to read a patient’s chart and respond to the referring primary care provider with a single submission of written communication. Physicians self-reported this measure, with possible responses including “5–10 minutes,” “11–20 minutes,” “21–30 minutes,” and “31+ minutes.” Lastly, we chose representative questions, asked by primary care physicians, directly from select cases to illustrate the types asked by primary care physicians during urological eConsults. This study was deemed not regulated by the institutional review boards of the four participating institutions.
RESULTS
We identified 462 urological eConsults requested across the four institutions during the study period. Following the initial launch of the eVisit program, the number of eConsults requested per month remained relatively stable at most institutions, ranging from 4–17 eConsults per month depending on the institution. Among all requested eConsults, the top three diagnoses requested were: Andrology/infertility (18.9%), Hematuria (15.6%), and BPH/LUTS (14.5%). Figure 1 illustrates the full distribution of diagnoses.
Figure 1:
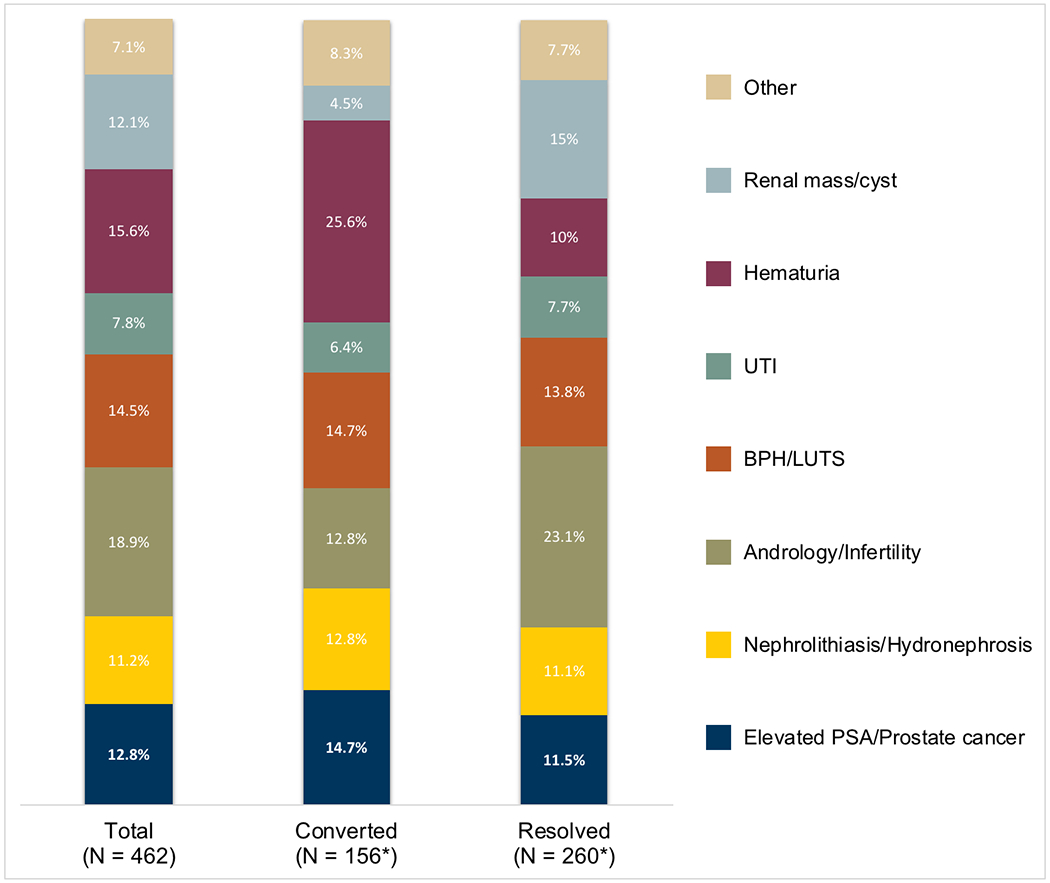
Distribution of eConsult diagnosis. Data shown for all econsults, then stratified by those that were resolved or converted to in-person consultation. *eConsults from one institution (N = 46) did not have conversion/resolution rate data and were excluded.
Overall, 296 eConsults (64%) were successfully resolved and 166 (36%) converted to in-person consultations. We also examined variation in rates of conversion to in-person consultations across institutions. Conversion rates ranged from 20% (Institution A) to 48% (Institution D), with Institutions B and C in between (32.6% and 41.1%, respectively). Among resolved eConsults with available diagnosis data (n=260), the top three diagnoses were: Andrology/Infertility (23.1%), Renal mass/cyst (15%), and BPH/LUTS (13.8%). Among converted eConsults with available diagnosis data (n=156), the top three diagnoses were Hematuria (25.6%), Elevated PSA/Prostate cancer (14.7%), and BPH/LUTS (14.7%) (Figure 1).
Among resolved eConsults with data on response time (n=119),53.8% of eConsults were addressed in less than 1 day; 28.6% in 1 day; 8.4% in 2 days; 3.4% in 3 days; 3.4% in 4 days; 1.7% in 5 days; and 0.8% in ≥6 days. Among resolved eConsults with data on completion time (n=283), 50.2% were completed in 1–10 minutes (68.9% at Institution A, 31.1% at Institution B, and 25.7% at Institution C); 46.7% in 11–20 minutes (8.9%, 34.2%, and 31.2%, respectively); 2.8% in 21–30 minutes (2.2%, 1.6%, and 2.0%, respectively); and less than 1% in ≥31 minutes (Figure 2).
Figure 2:
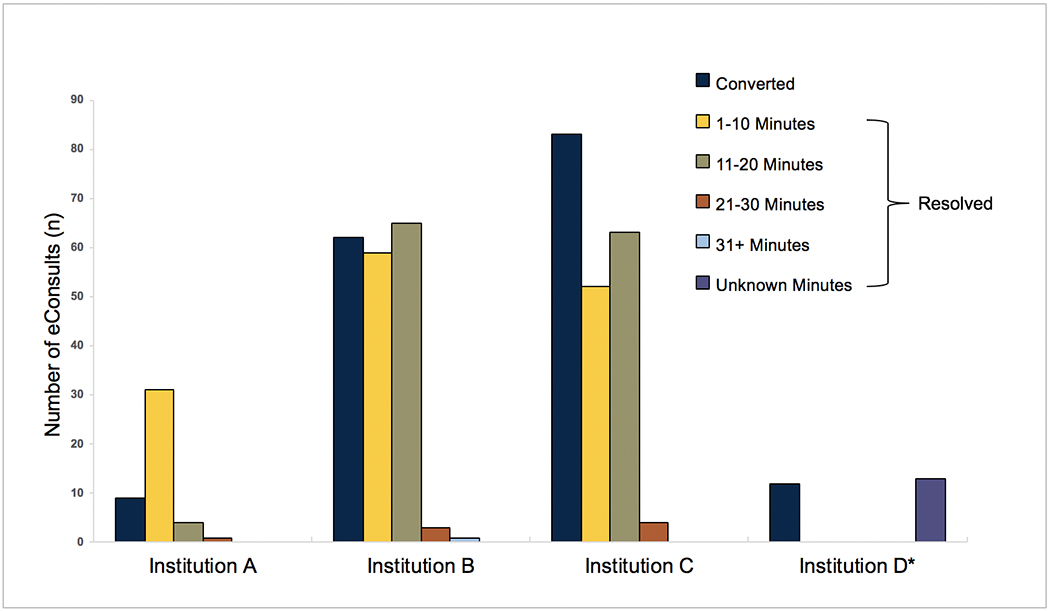
Frequency of converted and resolved eConsults by institution. Resolved visit counts further divided by provider completion time. *Provider completion time data was not available for resolved visits (n=13) from Institution D.
Table 1 demonstrates representative questions asked by primary care physicians during eConsults.
Table 1.
Sample Consult Questions Asked by Requesting Providers
| Question |
|---|
| What are next steps in work up of microscopic hematuria intermittent for almost 2 years now (once during cystitis but has persisted now treated and asymptomatic)? |
| Enlarging renal cyst found incidentally. How likely is this to be benign? Does it require tx, or need to be monitored routinely, or only if the pt has flank pain? |
| Patient was seen for scrotal swelling and work up revealed elevated PSA. He will have scrotal ultrasound to evaluate for hydrocele but could he also have prostatitis and should I do a prostate ultrasound as well? |
| Patient with recurrent, usually post-coital, culture confirmed UTIs now >2 in the last few months. Please advise if dedicated urologic imaging recommended, as well as preferred antibiotic prophylaxis (Bactrim allergy as well as nitrofurantoin previous resistance on culture). |
| Asymptomatic no signs UTI or epididymitis with painless enlargement of right scrotum. Checking PSA and CBC and urinalysis. Any other workup needed? |
DISCUSSION
We found that providers are using eConsults to gain specialty advice on a wide variety of urological diagnoses. From exploring the specific questions primary care physicians ask when using eConsults to evaluate patients’ conditions, we discovered that eConsults cover an equally wide range of clinical issues, from medication management to imaging and preventive measures. Furthermore, most eConsults are able to be resolved or addressed virtually, with a minority of cases escalated to traditional in-person visits. The eConsult itself requires minimal time from the urologist; more than half of the cases in our study required 10 or less minutes to complete. Collectively, these findings suggest that eConsults can successfully triage and address a variety of urological diagnoses, often without the need for further traditional in-person consultations.
Generally, prior studies of eConsults within other surgical specialties have found that eConsults can often substitute for in-person consultations in certain clinical scenarios. For example, in a study of eConsults within otolaryngology, only 11% of patients required a follow-up in-person exam by an otolaryngologist.11In another study, less than 50% of eConsults between primary care physicians and obstetrician-gynecologists converted to a follow-up specialist visit.12Considering the conversion rate seen in our study, this appears to be the case in urology as well.
Furthermore, our work is consistent with a prior Canadian study on urological eConsults.10In a study by Witherspoon et al., over one-third of a urologist’s office visits were substituted with eConsults.10Interestingly, based on the resolution rate observed in our study, the potential benefit of urological eConsults may in fact be even greater. In terms of other outcomes, our results largely agree with the findings of Witherspoon et al. For example, our study reiterated the time-efficiency associated with eConsults, as providers completed a majority of urological eConsults within 10 minutes in both studies.10Additionally, both studies demonstrated that, while conditions like hematuria and kidney stones are common subjects of urological eConsults, the full range of diagnoses is broadly encompassing.10
Of note, two other studies in the literature have also noted success in the avoidance of in-person consultations with the use of urological eConsults.7,8 In addition, McGeady et al demonstrated the ability for urological eConsults to improve efficiency of care even amongst patients who required follow-up evaluation in clinic.7 Specifically, the study found that eConsults were able to improve the rate of completion of necessary laboratory and imaging testing prior to formal urological evaluation as well as streamline surgical planning for operative patients.7
However, as previously mentioned, these studies were conducted in safety-net hospitals and the unique practice environment which comes with such institutions. For example, safety-net hospitals and non-safety net hospitals may differ in regards to the level of available financial resources, medical services available, and serve a higher proportion of patients with socioeconomic challenges.13,14,15As a result, we believe our findings both offer additional insights and are perhaps more broadly generalizable to nationwide urological practices.
We did find variation in conversion and response rates between the institutions that we studied. There are several factors that may cause this variation such as the diversity of consults, complexity of the questions from the primary care doctors and the comfort level of the provider responding to the consults. For example, Institution C (conversion rate=41.1%) had many eConsults for elevated PSA, which were converted to in-person visits because the providers felt more comfortable seeing these patients in-person. While there was variation among the institutions, the general trend was the same (high rates of resolved consults and almost no consults that took more than 20 minutes).
There are a few limitations to our study. First, our study looked only at the eConsult programs at four academic institutions. Thus, the results may differ relative to other academic institutions and non-academic healthcare settings. However, the four institutions covered in our study are diverse in terms of geographic location and primary care referral base. Second, we did not assess provider satisfaction from referring or consulting providers in our study. Being that eConsults are physician-to-physician interactions, we expect that these metrics will be crucial in assessing both the long-term functionality and potential for expansion of these programs. A third limitation of our study is that our data regarding time spent responding to an eConsult were self-reported by urologists with minimal measures taken to ensure standardization. Lastly, data on provider completion time of resolved eConsults was not available for Institution D.
These limitations notwithstanding, this study has important implications for policymakers, as the Medicare program has begun to reimburse for eConsults and the impacts are percolating through the private insurance markets. Our findings demonstrate that eConsults offer utility in the care of urological diseases, though outcomes may vary once healthcare providers adopt eConsults more widely. Similarly, for health systems, our study shows that even within surgical specialties, eConsults can free up capacity to address high-complexity surgical cases and ease access issues. A few of the institutions from our study have already incorporated clinical pathways agreed-upon by multiple specialty services to supplement eConsults for select diagnoses. Further addition of these pathways has the potential to either improve in-person care through expedited clinical work-up or help avoid in-person care altogether. However, though reimbursement for these services is now available, health systems will have to weigh reimbursement against the allocation of time and resources. Depending on the length of time spent on an eConsult, current reimbursement ranges from 0.35 RVU to 1.40 RVU within the Medicare program.9 At a national scale, the overall financial impact of eConsults on health systems also remains unclear. For patients and physicians, given the high acceptance rate of eConsults, it is clear that eConsults have the potential to be safely used for many types of urological diagnoses, and thus may be a more efficient way to manage low-complexity issues.
Finally, it is important to consider that the entirety of our study was completed in a non-pandemic period. During this time, the total number of requested urological eConsults remained low despite the fact that these programs were no longer nascent. With the onset of the COVID-19 Pandemic, methods of telemedicine such as eConsults are being increasingly relied on for urological care.9 As data becomes available on the success of these programs, it will come with the caveat that these eConsults were performed at a time when physical contact and other elements of an in-person consultation were strongly recommended against, outside of the most necessary situations. Thus, the results of our study portray an accurate assessment of the applicability and utility of eConsults that one may expect in a post-pandemic period.
CONCLUSION
In summary, our findings suggest that eConsults offer a new, feasible avenue for urologic consultation. Moving forward, research in this area should evaluate larger-scale outcomes, such as cost, quality, and access to care, as well as the provider experience with eConsults in urology. As we continue to explore the capabilities of eConsult programs, we may uncover a long-lasting solution to alleviate the effects of the provider shortage not only in urology, but other fields of medicine.
ACKNOWLEDGEMENTS:
FUNDING:
This work was supported by the Telehealth Research Incubator project grant (MPrOVE Research Challenge Grant). Dr. Ellimoottil’s time was supported by K08 HS027632-01 from the Agency for Healthcare Research and Quality. No funding agency had a role in study design, data collection and analysis, decision to publish, or preparation of the manuscript
KEY DEFINITIONS
- eConsult
interprofessional electronic consultation
- BPH
benign prostatic hyperplasia
- LUTS
lower urinary tract symptoms
Footnotes
DECLARATION OF CONFLICTING INTERESTS:
The Authors declare that there is no conflict of interest.
REFERENCES
- 1.Medina Lauren, Sabo Shannon, and Vespa Jonathan: Living Longer: Historical and Projected Life Expectancy in the United States, 1960 to 2060. U.S. Census Bureau; 2020. Available at:https://www.census.gov/content/dam/Census/library/publications/2020/demo/p25-1145.pdf. [Google Scholar]
- 2.Pruthi RS, Neuwahl S, Nielsen ME, et al. : Recent trends in the urology workforce in the United States. Urology 2013; 82: 987–993. [DOI] [PubMed] [Google Scholar]
- 3.McKibben MJ, Kirby EW, Langston J, et al. : Projecting the Urology Workforce Over the Next 20 Years. Urology 2016; 98: 21–26. [DOI] [PubMed] [Google Scholar]
- 4.Centers for Medicare & Medicaid Services: Medicare Program; Revisions to Payment Policies Under the Physician Fee Schedule and Other Revisions to Part B for CY 2019; Medicare Shared Savings Program Requirements; Quality Payment Program; Medicaid Promoting Interoperability Program; Quality Payment Program-Extreme and Uncontrollable Circumstance Policy for the 2019 MIPS Payment Year; Provisions From the Medicare Shared Savings Program-Accountable Care Organizations-Pathways to Success; and Expanding the Use of Telehealth Services for the Treatment of Opioid Use Disorder Under the Substance Use-Disorder Prevention That Promotes Opioid Recovery and Treatment (SUPPORT) for Patients and Communities Act. Federal Register 2018; 83: 59452–60303. Available at:https://www.federalregister.gov/d/2018-24170. [Google Scholar]
- 5.Olayiwola JN, Anderson D, Jepeal N, et al. : Electronic Consultations to Improve the Primary Care-Specialty Care Interface for Cardiology in the Medically Underserved: A Cluster-Randomized Controlled Trial. Ann. Fam. Med 2016; 14: 133–140. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Kim GE, Afanasiev OK, O’Dell C, et al. : Implementation and evaluation of Stanford Health Care store-and-forward teledermatology consultation workflow built within an existing electronic health record system. J. Telemed. Telecare 2018: 1357633X18799805. [DOI] [PubMed] [Google Scholar]
- 7.McGeady James B, Blaschko Sarah D, Brajtbord Jonathan S, et al. : Electronic Preconsultation as a Method of Quality Improvement for Urological Referrals. Urology Practice 2014; 1: 172–175. [DOI] [PubMed] [Google Scholar]
- 8.Nathan Chertack, Yair Lotan, Christian Mayorga, et al. : Implementation of a Urology E-Consult Service at a Safety Net County Hospital. Urology Practice 2020; 0: 10.1097/UPJ.0000000000000140. [DOI] [PubMed] [Google Scholar]
- 9.Gadzinski AJ, Andino JJ, Odisho AY, et al. : Telemedicine and eConsults for Hospitalized Patients During COVID-19. Urology 2020. Available at: 10.1016/j.urology.2020.04.061. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Witherspoon L, Liddy C, Afkham A, et al. : Improving access to urologists through an electronic consultation service. Can. Urol. Assoc. J 2017; 11: 270–274. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Hofstetter PJ, Kokesh J, Ferguson AS, et al. : The impact of telehealth on wait time for ENT specialty care. Telemed. J. E. Health 2010; 16: 551–556. [DOI] [PubMed] [Google Scholar]
- 12.Keely E, Liddy C and Afkham A: Utilization, benefits, and impact of an e-consultation service across diverse specialties and primary care providers. Telemed. J. E. Health 2013; 19: 733–738. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Popescu I, Fingar KR, Cutler E, et al. : Comparison of 3 Safety-Net Hospital Definitions and Association With Hospital Characteristics. JAMA Netw Open 2019; 2: e198577. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Mouch CA, Regenbogen SE, Revels SL, et al. : The quality of surgical care in safety net hospitals: a systematic review. Surgery 2014; 155: 826–838. [DOI] [PubMed] [Google Scholar]
- 15.Zwanziger J and Khan N: Safety-net hospitals. Med. Care Res. Rev 2008; 65: 478–495. [DOI] [PubMed] [Google Scholar]