

Abstract
Background
Previous Cochrane Reviews have shown that cognitive behavioural therapy (CBT) is effective in treating childhood anxiety disorders. However, questions remain regarding the following: up‐to‐date evidence of the relative efficacy and acceptability of CBT compared to waiting lists/no treatment, treatment as usual, attention controls, and alternative treatments; benefits across a range of outcomes; longer‐term effects; outcomes for different delivery formats; and amongst children with autism spectrum disorders (ASD) and children with intellectual impairments.
Objectives
To examine the effect of CBT for childhood anxiety disorders, in comparison with waitlist/no treatment, treatment as usual (TAU), attention control, alternative treatment, and medication.
Search methods
We searched the Cochrane Common Mental Disorders Controlled Trials Register (all years to 2016), the Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE, Embase, and PsycINFO (each to October 2019), international trial registries, and conducted grey literature searches.
Selection criteria
We included randomised controlled trials of CBT that involved direct contact with the child, parent, or both, and included non‐CBT comparators (waitlist/no treatment, treatment as usual, attention control, alternative treatment, medication). Participants were younger than age 19, and met diagnostic criteria for an anxiety disorder diagnosis. Primary outcomes were remission of primary anxiety diagnosis post‐treatment, and acceptability (number of participants lost to post‐treatment assessment), and secondary outcomes included remission of all anxiety diagnoses, reduction in anxiety symptoms, reduction in depressive symptoms, improvement in global functioning, adverse effects, and longer‐term effects.
Data collection and analysis
We used standard methodological procedures as recommended by Cochrane. We used GRADE to assess the quality of the evidence.
Main results
We included 87 studies and 5964 participants in quantitative analyses.
Compared with waitlist/no treatment, CBT probably increases post‐treatment remission of primary anxiety diagnoses (CBT: 49.4%, waitlist/no treatment: 17.8%; OR 5.45, 95% confidence interval (CI) 3.90 to 7.60; n = 2697, 39 studies, moderate quality); NNTB 3 (95% CI 2.25 to 3.57) and all anxiety diagnoses (OR 4.43, 95% CI 2.89 to 6.78; n = 2075, 28 studies, moderate quality).
Low‐quality evidence did not show a difference between CBT and TAU in post‐treatment primary anxiety disorder remission (OR 3.19, 95% CI 0.90 to 11.29; n = 487, 8 studies), but did suggest CBT may increase remission from all anxiety disorders compared to TAU (OR 2.74, 95% CI 1.16 to 6.46; n = 203, 5 studies).
Compared with attention control, CBT may increase post‐treatment remission of primary anxiety disorders (OR 2.28, 95% CI 1.33 to 3.89; n = 822, 10 studies, low quality) and all anxiety disorders (OR 2.75, 95% CI 1.22 to 6.17; n = 378, 5 studies, low quality).
There was insufficient available data to compare CBT to alternative treatments on post‐treatment remission of primary anxiety disorders, and low‐quality evidence showed there may be little to no difference between these groups on post‐treatment remission of all anxiety disorders (OR 0.89, 95% CI 0.35 to 2.23; n = 401, 4 studies)
Low‐quality evidence did not show a difference for acceptability between CBT and waitlist/no treatment (OR 1.09, 95% CI 0.85 to 1.41; n=3158, 45 studies), treatment as usual (OR 1.37, 95% CI 0.73 to 2.56; n = 441, 8 studies), attention control (OR 1.00, 95% CI 0.68 to 1.49; n = 797, 12 studies) and alternative treatment (OR 1.58, 95% CI 0.61 to 4.13; n=515, 7 studies).
No adverse effects were reported across all studies; however, in the small number of studies where any reference was made to adverse effects, it was not clear that these were systematically monitored.
Results from the anxiety symptom outcomes, broader outcomes, longer‐term outcomes and subgroup analyses are provided in the text.
We did not find evidence of consistent differences in outcomes according to delivery formats (e.g. individual versus group; amount of therapist contact time) or amongst samples with and without ASD, and no studies included samples of children with intellectual impairments.
Authors' conclusions
CBT is probably more effective in the short‐term than waiting lists/no treatment, and may be more effective than attention control. We found little to no evidence across outcomes that CBT is superior to usual care or alternative treatments, but our confidence in these findings are limited due to concerns about the amount and quality of available evidence, and we still know little about how best to efficiently improve outcomes.
Keywords: Adolescent; Child; Child, Preschool; Humans; Anxiety Disorders; Anxiety Disorders/therapy; Bias; Cognitive Behavioral Therapy; Confidence Intervals; Depression; Depression/therapy; Lost to Follow-Up; Parents; Randomized Controlled Trials as Topic; Remission Induction; Time Factors; Waiting Lists
Plain language summary
Cognitive behavioural therapy for anxiety in children and young people
Why is this review important?
Many children and young people experience problems with anxiety. Children and young people with anxiety disorders are more likely than their peers to have difficulty with friendships, family life, and school, and to develop mental health problems later in life. Therapies such as cognitive behavioural therapy (CBT) can help children and young people to overcome difficulties with anxiety by using new ways of thinking and facing their fears.
Who will be interested in this review?
Parents, children, and young people; people working in education and mental health services for children and young people; and general practitioners.
What questions does this review aim to answer?
This review updates and replaces previous Cochrane Reviews from 2005 and 2015, which showed that CBT is an effective treatment for children and young people with anxiety disorders.
This review aimed to answer the following questions:
• Is CBT more effective than a waiting list or no treatment?
• Is CBT more effective than other treatments and medication?
• Does CBT help to reduce anxiety for children and young people in the longer term?
• Are some types of CBT more effective than others? (e.g. individual versus group therapy)
• Is CBT effective for specific groups? (e.g. children with autism)
Which studies were included in the review?
We searched the databases to find all studies of CBT for anxiety disorders in children and young people published up to October 2019. In order to be included in the review, studies had to be randomised controlled trials (a type of study in which participants are assigned to one of two or more treatment groups using a random method) and had to include young people under 19 years of age with an anxiety disorder diagnosis. We included 87 studies with a total of 5964 participants in the analysis.
What does the evidence from the review tell us?
We rated the overall quality of the evidence as 'moderate’ or 'low'. There is evidence that CBT is more effective than a waiting list or no treatment in reducing anxiety in children and young people, although the findings did vary across studies. There is no clear evidence that CBT is more effective than other treatments. A small number of studies looked at outcomes six months after CBT was given and showed that reductions in anxiety continued. We found no clear evidence that one way of providing CBT is more effective than another (e.g. in a group, longer treatments, with parents) or that CBT is more or less effective for any specific group of children (e.g. children with autism spectrum disorders).
What should happen next?
Future research should compare CBT to alternative treatments and medication; identify who does and does not benefit from CBT and what those who do not benefit need; establish how to make CBT more accessible; and give far more consideration to neglected populations, including children and young people from low‐ and middle‐income countries.
Summary of findings
Summary of findings 1. CBT compared with waitlist for children and adolescents with anxiety disorders.
| CBT compared with waitlist for children and adolescents with anxiety disorders | ||||||
|
Patient or population: children and adolescents with anxiety disorders Settings: outpatient clinics/schools Intervention: CBT Comparison: waitlist/no treatment | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | No. of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Waitlist1 | CBT | |||||
| Remission of primary anxiety diagnosis post‐treatment (ITT) | 178 per 1000 | 541 per 1000 (458 to 622) | OR 5.45 (3.90 to 7.60) | 2697 (39 studies) | ⊕⊕⊕⊝ moderate2 | Subgroup analyses:
|
| Acceptability (number of participants lost to post‐treatment assessment) | 104 per 1000 | 112 per 1000 (90 to 141) | OR 1.09 (0.85 to 1.41) | 3158 (45 studies) | ⊕⊕⊝⊝ low3 | |
| Remission of all anxiety diagnoses post‐treatment (ITT) | 191 per 1000 | 512 per 1000 (406 to 616) | OR 4.43 (2.89 to 6.78) | 2075 (28 studies) |
⊕⊕⊕⊝ moderate2 | Subgroup analyses:
|
| Reduction in anxiety symptoms (child report) post‐treatment | The mean anxiety symptoms (child report) in the CBT groups was 0.67standard deviations lower (0.88 to 0.47 lower). | Moderate effect size | 2831 (45 studies) | ⊕⊕⊝⊝ low4 | Subgroup analyses:
|
|
| Reduction in anxiety symptoms (parent report) post‐treatment | The mean anxiety symptoms (parent report) in the CBT groups was 0.70standard deviations lower (0.90 to 0.51 lower). | Moderate effect size | 2137 (35 studies) | ⊕⊕⊝⊝ low4 | Subgroup analyses:
|
|
| Reduction in depressive symptoms post‐treatment | The mean depressive symptoms in the CBT groups was 0.34 standard deviations lower (0.51 to 0.17 lower). | Small effect size | 1157 (17 studies) |
⊕⊕⊕⊝ moderate2 | ||
| Improvement in global functioning post‐treatment | The mean global functioning in the CBT groups was 1.03 standard deviations higher (0.68 to 1.38 higher). | Large effect size | 557 (11 studies) |
⊕⊕⊝⊝ low5 | ||
| Adverse events (randomisation to post‐treatment) | See comment | See comment | Not estimable | ‐ | See comment | No study reported adverse events in both CBT and waitlist/no treatment groups |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CBT: cognitive behavioural therapy; CI: confidence interval; ITT: intention‐to‐treat; OR: odds ratio | ||||||
| GRADE Working Group grades of evidence High quality: Further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: We are very uncertain about the estimate. | ||||||
1Control group risk estimates come from pooled estimates of waitlist groups. 2Downgraded one level due to moderate heterogeneity (inconsistency). 3Downgraded two levels due large variation in treatment effects across studies (inconsistency) and wide confidence intervals (imprecision). 4Downgraded two levels due to substantial heterogeneity (inconsistency). 5Downgraded two levels due to substantial heterogeneity (inconsistency) and assessed and reported in small number of eligible studies (study limitations).
Summary of findings 2. CBT compared with treatment as usual for anxiety disorders in children and adolescents.
| CBT compared with treatment as usual for anxiety disorders in children and adolescents | ||||||
|
Patient or population: children and adolescents with anxiety disorders Settings: outpatient clinics/schools Intervention: CBT Comparison: treatment as usual |
||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | No. of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk1 | Corresponding risk | |||||
| Treatment as usual | CBT | |||||
| Remission of primary anxiety diagnosis post‐treatment (ITT) | 408 per 1000 | 687 per 1000 (383 to 886) | OR 3.19 (0.90 to 11.29) | 487 (8 studies) |
⊕⊕⊝⊝ low2 | Subgroup analyses:
|
| Acceptability (number of participants lost to post‐treatment assessment) | 93 per 1000 | 124 per 1000 (70 to 209) | OR 1.37 (0.73 to 2.56) | 441 (8 studies) |
⊕⊕⊝⊝ low3 | |
| Remission of all anxiety diagnoses post‐treatment (ITT) | 414 per 1000 | 660 per 1000 (451 to 820) | OR 2.74 (1.16 to 6.46) | 203 (5 studies) |
⊕⊕⊝⊝ low3 | |
| Reduction in anxiety symptoms (child report) post‐treatment | The mean anxiety symptoms (child report) in the CBT groups was 0.15standard deviations lower (0.78 lower to 0.48 higher). | Cross 0 | 214 (6 studies) |
⊕⊕⊝⊝ low2 | ||
| Reduction in anxiety symptoms (parent report) post‐treatment | The mean anxiety symptoms (parent report) in the CBT groups was 0.32standard deviations lower (0.70 lower to 0.06 higher). | Cross 0 | 228 (7 studies) |
⊕⊕⊝⊝ low2 | ||
| Reduction in depressive symptoms post‐treatment | See comment | Not estimable | ‐ | See comment | Insufficient evidence to estimate effect | |
| Improvement in global functioning post‐treatment | See comment | Not estimable | ‐ | See comment | Insufficient evidence to estimate effect | |
| Adverse events (randomisation to post‐treatment) | See comment | See comment | Not estimable | ‐ | See comment | No study reported adverse events in both CBT and Treatment as Usual groups |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CBT: cognitive behavioural therapy; CI: confidence interval; ITT: intention‐to‐treat; OR: odds ratio | ||||||
| GRADE Working Group grades of evidence High quality: Further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: We are very uncertain about the estimate. | ||||||
1Control group risk estimates come from pooled estimates of treatment as usual groups. 2Downgraded two levels due to at least moderate heterogeneity (inconsistency) and wide confidence intervals and small number of events or participants (imprecision). 3Downgraded two levels due to large variation in treatment effects across studies (inconsistency) and wide confidence intervals and small number of events (imprecision).
Summary of findings 3. CBT compared with attention control for anxiety disorders in children and adolescents.
| CBT compared with attention control for anxiety disorders in children and adolescents | ||||||
|
Patient or population: children and adolescents with anxiety disorders Settings: outpatient clinics/schools Intervention: CBT Comparison: attention control |
||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | No. of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Attention control1 | CBT | |||||
| Remission of primary anxiety diagnosis post‐treatment (ITT) | 293 per 1000 | 486 per 1000 (355 to 617) | OR 2.28 (1.33 to 3.89) | 822 (10 studies) | ⊕⊕⊝⊝ low2, | Subgroup analyses:
|
| Acceptability (number of participants lost to post‐treatment assessment) | 201 per 1000 | 201 per 1000 (146 to 272) | OR 1.00 (0.68 to 1.49) | 797 (12 studies) | ⊕⊕⊝⊝ low3 | |
| Remission of all anxiety diagnoses post‐treatment (ITT) | 185 per 1000 | 385 per 1000 (217 to 584) | OR 2.75 (1.22 to 6.17) | 378 (5 studies) | ⊕⊕⊝⊝ low2 | |
| Reduction in anxiety symptoms (child report) post‐treatment | The mean anxiety symptoms (child report) in the CBT groups was 0.31standard deviations lower (0.51 to 0.11 lower). | Small effect size | 978 (15 studies) | ⊕⊕⊕⊝ moderate4 | ||
| Reduction in anxiety symptoms (parent report) post‐treatment | The mean anxiety symptoms (parent report) in the CBT groups was 0.25standard deviations lower (0.61 lower to 0.11 higher). | Cross 0 | 638 (8 studies) | ⊕⊕⊝⊝ low5 | ||
| Reduction in depressive symptoms post‐treatment | The mean depressive symptoms in the CBT groups was 0.18standard deviations lower (0.45 lower to 0.09 higher). | Cross 0 | 613 (10 studies) | ⊕⊕⊝⊝ low5 | ||
| Improvement in global functioning post‐treatment | See comment | Not estimable | ‐ | See comment | Insufficient evidence to estimate effect | |
| Adverse events (randomisation to post‐treatment) | See comment | See comment | Not estimable | ‐ | See comment | No study reported adverse events in both CBT and attention control groups |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CBT: cognitive behavioural therapy; CI: confidence interval; ITT: intention‐to‐treat; OR: odds ratio | ||||||
| GRADE Working Group grades of evidence High quality: Further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: We are very uncertain about the estimate. | ||||||
1Control group risk estimates come from pooled estimates of attention control groups. 2Downgraded two levels due to at least moderate heterogeneity and large variation in treatment effects (inconsistency) and small number of events (imprecision). 3Downgraded two levels due to large variation in treatment effects across studies (inconsistency) and wide confidence intervals and small number of events (imprecision). 4Downgraded one level due to moderate heterogeneity (inconsistency). 5Downgraded two levels due to at least moderate heterogeneity (inconsistency) and wide confidence intervals (imprecision).
Summary of findings 4. CBT compared with alternative treatment for anxiety disorders in children and adolescents.
| CBT compared with alternative treatment for anxiety disorders in children and adolescents | ||||||
|
Patient or population: children and adolescents with anxiety disorders Settings: outpatient clinics/schools Intervention: CBT Comparison: alternative treatment |
||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | No. of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Alternative treatment1 | CBT | |||||
| Remission of primary anxiety diagnosis post‐treatment (ITT) | See comment | See comment | Not estimable | ‐ | See comment | Insufficient evidence to estimate effect or conduct subgroup analyses |
| Acceptability (number of participants lost to post‐treatment assessment) | 115 per 1000 | 171 per 1000 (74 to 350) | OR 1.58 (0.61 to 4.13) | 515 (7 studies) | ⊕⊕⊝⊝ low2 |
|
| Remission of all anxiety diagnoses post‐treatment (ITT) | 607 per 1000 | 579 per 1000 (351 to 775) | OR 0.89 (0.35 to 2.23) | 401 (4 studies) | ⊕⊕⊝⊝ low2 |
|
| Reduction in anxiety symptoms (child report) post‐treatment | The mean anxiety symptoms (child report) in the CBT groups was 0.09standard deviations lower (0.40 lower to 0.21 higher). | Cross 0 | 399 (6 studies) | ⊕⊕⊝⊝ low3 | ||
| Reduction in anxiety symptoms (parent report) post‐treatment | The mean anxiety symptoms (child report) in the CBT groups was 0.13standard deviations lower (0.33 lower to 0.06 higher). | Cross 0 | 423 (6 studies) | ⊕⊕⊝⊝ low4 | ||
| Reduction in depressive symptoms post‐treatment | Not estimable | Not estimable | ‐ | See comment | Insufficient evidence to estimate effect | |
| Improvement in global functioning post‐treatment | Not estimable | Not estimable | ‐ | See comment | No evidence available to estimate effect | |
| Adverse events (randomisation to post‐treatment) | See comment | See comment | Not estimable | ‐ | See comment | No study reported adverse events in both CBT and Treatment as Usual groups |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CBT: cognitive behavioural therapy; CI: confidence interval; ITT: intention‐to‐treat; OR: odds ratio | ||||||
| GRADE Working Group grades of evidence High quality: Further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: We are very uncertain about the estimate. | ||||||
1Control group risk estimates come from pooled estimates of alternative treatment groups. 2Downgraded two levels due to at least moderate heterogeneity (inconsistency) and wide confidence intervals and small number of events (imprecision). 3Downgraded two levels due to moderate heterogeneity (inconsistency) and wide confidence intervals (imprecision). 4Downgraded two levels due to large variation in treatment effects across studies (inconsistency) and wide confidence intervals (imprecision).
Background
Description of the condition
Anxiety disorders are amongst the most common psychiatric disorders, occurring in 6.5% of all children and adolescents (Polanczyk 2015). One of the diagnostic challenges in children and adolescents involves distinguishing normal, developmentally appropriate worries, fears, and shyness from anxiety disorders. For example, primary school‐age children commonly have worries about injury and natural events, whereas older children and adolescents typically have worries and fears related to school performance, social competence, and health issues (Beesdo 2009). Distinguishing features of pathological anxiety include severity, persistence, and associated impairment.
The International Classification of Diseases (ICD), WHO 1992, and Diagnostic and Statistical Manual of Mental Disorders (DSM‐5), APA 2013, diagnostic systems distinguish various types of anxiety disorders, including generalised anxiety disorder, panic disorder, social anxiety disorder, separation anxiety disorder, agoraphobia, specific phobias, and selective mutism. These anxiety disorders are often associated with significant impairment in personal, social, and academic functioning (Pine 2009). Comorbidities are common, in particular with other anxiety disorders in children and adolescents (Leyfer 2013), and depression in adolescents (Essau 2003).
The presentation of anxiety disorders varies with age. Separation anxiety disorders are more common in younger children than in adolescents, and difficulties with social anxiety are typically associated with greater disturbance in adolescence (Waite 2014). Anxiety disorders with an onset in childhood often persist into adolescence and early adulthood (Copeland 2014), and are also associated with adverse academic, health, and social functioning in adulthood (Copeland 2014; Essau 2014). Yet these often remain untreated, with an average delay of 9 to 23 years before anxiety disorders are first treated (Wang 2005). It is clear that anxiety disorders in this age group present serious ongoing health issues, therefore effective and readily accessible treatments are needed.
Description of the intervention
Current treatments for anxiety disorders in this age group include behavioural therapy, cognitive behavioural therapy (CBT), or medication, or a combination of some or all these. National Institute for Health and Care Excellence (NICE) guidelines are available for the treatment of social anxiety disorder, which recommend CBT that is specifically focused on social anxiety (NICE 2013). Given the prevalence of these disorders, the age of onset, and public views on the acceptability of pharmacological treatments, psychological treatments are often preferred as first‐line therapy (Brown 2007; Young 2006). CBT is a collaborative psychological treatment that can be delivered in various formats, individually or in groups, and with varying levels of parent or family involvement.
One of the first manualised CBT programmes was Coping Cat (Kendall 1994), which consists of psycho‐education, modification of negative cognitions, exposure, social competence training, coping behaviour, and self‐reinforcement sessions. Others have followed, including the Cool Kids programme (Hudson 2009; Rapee 2006), the Coping Koala programme (Barrett 1996), Skills for Academic and Social Success (SASS) (Masia‐Warner 2005), ACTION (Waters 2009), Intervention With Adolescents With Social Phobia (IAFS) (Sanchez‐Garcia 2009), the TAPS (Warner 2011), and Building Confidence programme (Galla 2012). Alternative programmes involve providing direct support to parents alone, guiding them to implement CBT strategies with their child (Guided Parent‐Delivered CBT (GPD‐CBT) (Lyneham 2006; Thirlwall 2013; Waters 2009). CBT programmes have typically adopted a generic approach and target a range of anxiety disorders (e.g. Coping Cat), but some are disorder‐specific, targeting, for example, social anxiety disorder (e.g. SASS). CBT programmes have been modified in various ways to make them appropriate for children with autism spectrum disorders (ASD), such as by including social stories, social coaching, visual aids, and structured worksheets (Ung 2015). Such programmes include the Multimodal Anxiety and Social Skills Intervention (MASSI) programme (White 2013), TAFF (Schneider 2011), Behavioural Interventions for Anxiety in Children with Autism (BIACA) (Wood 2009), and Facing Your Fears (FYF) (Reaven 2012).
How the intervention might work
CBT for anxiety disorders in children and adolescents typically involves helping the child to recognise anxious feelings and bodily or somatic reactions to anxiety, identify thoughts or cognitions in anxiety‐provoking situations (e.g. unrealistic or negative attributions and expectations), and modifying these anxiety‐provoking cognitions (e.g. testing out predictions based on anxious thoughts, modifying anxious self‐talk into coping self‐talk). A key CBT procedure is exposure (Creswell 2020b), which typically involves testing out and ‘facing’ fears, often in a gradually increasing hierarchy. Behavioural training strategies such as modelling and role playing are often applied as opportunities for developing coping skills (e.g. problem‐solving skills, social skills, relaxation training).
CBT for anxiety disorders in children and adolescents has traditionally begun with six to nine face‐to‐face sessions of anxiety management strategies (emotion identification, relaxation training, cognitive strategies), followed by exposure work (Barrett 1996; Kendall 2006). In one meta‐analysis (Reynolds 2012), this traditional format of anxiety management sessions followed by exposure was observed in 93% of studies. However, Ale 2015 found that treatment outcomes in CBT treatment trials for child and adolescent anxiety disorders were not related to the use of relaxation strategies or the timing of exposure work, and therefore suggested that relaxation training may not be an essential ingredient of CBT, and that it may not be necessary to delay exposure until after anxiety management sessions. Moreover, there is also some preliminary evidence that introducing exposure early in treatment, without any prior anxiety management sessions, could improve outcomes whilst requiring fewer appointments (Whiteside 2015).
Indeed, questions remain about the mechanism of change within CBT. Cognitive restructuring and exposure tasks have each been found to make substantial contributions to improvement in child and adolescent anxiety in line with CBT theory (Peris 2015). More time devoted to exposure has been linked to better outcomes, and greater time spent on more difficult exposure tasks has been shown to predict better outcomes (Peris 2017). Change in coping efficacy, but not anxious self‐talk, has been found to mediate change in anxiety symptoms associated with CBT, medication (sertraline), and their combination, compared to placebo control (Kendall 2016). Furthermore, therapists’ ratings of child compliance and mastery also predict better outcomes (Peris 2017). Cognitive development also plays an important role, and whilst targeting behavioural avoidance appears to be crucial for both children and adolescents, treatment that directly addresses interpretation biases may be particularly beneficial for adolescents, but less so for younger children (Waite 2015).
CBT has been adapted to include family and parents in treatment sessions; however, parents/family members have been included in a wide variety of ways, including, for example, providing education and information on the child‐focused CBT, and/or modifying parents’ beliefs and behaviours, and/or addressing parental anxiety. These different approaches are based on different conceptualisations of the mechanisms of change in child anxiety through parental involvement. It is important to note, however, that changes in parent and child responses are likely to be bidirectional. For example, one study found that child‐focused anxiety treatments resulted in improvements in non‐targeted parent symptoms and family functioning, particularly when children responded successfully to treatment (Keeton 2013).
It is generally assumed that CBT can be applied only after the child has reached a certain level of cognitive development. Kendall 1993 argued that the ability to measure a thought or belief against the notion of a rational standard and the ability to understand that a thought or belief can cause a person to behave and feel in a certain way were central to its proper use. The question arises: at what age does a child have the cognitive capacities to undertake these cognitive operations? One study reported positive effects of CBT in children younger than six years of age (Hirshfeld‐Becker 2010); however, it is not clear whether children this age are able to use the cognitive strategies that are included in traditional CBT protocols. In line with this, research suggests that young children may be more responsive to the behavioural than the cognitive elements of this approach (Essau 2004). With younger children, parental involvement appears particularly important. Indeed, the treatment of anxiety disorders in young children can be effective by applying CBT principles through working directly with parents alone (Cartwright‐Hatton 2011), although there are inconsistent findings in relation to whether child‐parent delivery format is superior to parent‐only or not (Monga 2015; Waters 2009).
Why it is important to do this review
Anxiety disorders in children and adolescents represent a considerable source of morbidity and are associated with later adult psychopathology and greater cost than any other mental health disorder (Fineberg 2013). However, despite high prevalence and substantial morbidity, anxiety disorders in childhood and adolescence can be difficult to diagnose, and may be under‐recognised (NICE 2013), and therefore undertreated (Pine 2009). It is widely reported that only a minority of children and adolescents with mental health problems receive treatment (Green 2004; Merikangas 2011); a recent UK survey reported that fewer than 40% of children with anxiety disorders receive any professional support, and less than 3% receive CBT (Reardon 2020). Limited service provision represents a key barrier to treatment access (Reardon 2017), highlighting the importance of maximising the efficiency of treatment delivery to help ensure that effective treatment is more readily available to children and young people when they need it.
The evidence base for the treatment of anxiety disorders in children and adolescents is growing. Initial trials of CBT were positive (Barrett 1996; Kendall 1994; Kendall 1997), and further randomised controlled trials and reviews followed. Several reviews suggest that CBT for anxiety disorders in this age group is effective (Ale 2015; Crowe 2017; James 2015; Reynolds 2012; Silverman 2008), including an overview of systematic reviews and a network meta‐analysis (Bennett 2016; Zhou 2019). Overall there was a moderate response rate (e.g. 59%; James 2015), and a recent review indicated that benefits extend to broader outcomes, including depressive symptoms and general functioning (Kreuze 2018). However, CBT has not been shown to be superior to active controls or treatment as usual (James 2015; Southam‐Gerow 2010). In some previous studies, the effect sizes associated with CBT for childhood anxiety disorders did not differentiate it from attention placebo, although CBT has been found to be more effective than waiting list control (Ale 2015). It remains unclear whether CBT is superior to alternative treatment approaches.
This review updates and replaces previous Cochrane Reviews of CBT for anxiety disorders in children and adolescents (James 2005; James 2015). The current review aims to provide comprehensive and up‐to‐date evidence on the efficacy and acceptability of CBT in the treatment of anxiety disorders in children and adolescents, with varying amounts of therapist contact time and differing delivery formats, including individual, group, with/without family/parent involvement, and parent‐led. Furthermore, we planned to examine the efficacy of CBT relative to treatment as usual, attention control, and alternative treatments. The question of the comparative efficacy of medication versus CBT and the combination of CBT and medication was also to be addressed.
A recent development is the issue of the reporting of remission of all anxiety diagnoses, as well as the primary anxiety diagnosis (Warwick 2016). Given the high level of comorbid anxiety disorders, this is an important issue, but surprisingly has been previously overlooked. Indeed, focusing solely on recovery from the primary anxiety diagnosis means that children with comorbid anxiety disorders that are present following treatment are often still classed as ‘recovered’. As such, this review distinguishes between and examines outcomes based on both the absence of the ‘primary anxiety disorder’ and the absence of all anxiety disorders. As well as providing evidence on anxiety outcomes (diagnoses and symptoms), we also planned to examine benefits in relation to broader outcomes, including depressive symptoms and global functioning.
We also aimed to assess whether treatment effects of CBT are maintained beyond post‐treatment and at longer‐term follow‐up. Whilst it would not be possible to determine the youngest age at which a child can benefit from CBT without individual patient data, we would identify the age of the youngest participants in trials of CBT for child and adolescent anxiety disorders. It is recognised that children and adolescents with ASDs have high rates of anxiety disorders (van Steensel 2013); however, studies of CBT for anxiety disorders in ASD have had mixed outcomes (Murphy 2017; Ung 2015). Furthermore, it is unclear how anxiety disorders are recognised or, indeed, treated in those with intellectual impairments, indicating a pressing need for work in this area. We planned to examine the efficacy of CBT in children and adolescents with ASD and those with intellectual impairments.
Previous Cochrane Reviews used a cutoff of nine sessions of CBT, based on the practice and thinking at the time (James 2005; James 2015). However, since the last Cochrane Review (James 2015), there have been several developments in the delivery of CBT for anxiety disorders. These include briefer or shorter interventions, in terms of not only the number of sessions, but also the total duration of treatment. As such, we would not set a threshold for the minimum number of sessions, and would explore how treatment effects differ with treatment duration. It is important to note that one potentially efficient means to deliver CBT is online or via digital devices (e.g. computerised CBT). But as online and digital CBT interventions for child anxiety disorders have been reviewed elsewhere (e.g. Pennant 2015), this review focused on face‐to‐face delivery models that include direct contact with either the child or parent alone, or the child and parent together.
Objectives
To carry out a meta‐analysis of identified studies to determine whether CBT leads to remission of 1) the primary child/adolescent anxiety disorder and 2) all anxiety diagnoses, and/or 3) a clinically significant reduction in anxiety symptoms in comparison with waiting list/no treatment, treatment as usual, attention control, alternative treatment, or medication.
To determine the comparative efficacy of CBT alone, and the combination of CBT and medication, versus drug placebo.
To determine if CBT is an acceptable treatment, relative to waiting list/no treatment, treatment as usual, attention control, alternative treatment, and medication.
To determine whether CBT for anxiety leads to a clinically significant reduction in depressive symptoms and/or improvements in global functioning.
To identify any adverse effects associated with CBT, relative to waiting list/no treatment, treatment as usual, attention control, alternative treatment, and medication.
To determine whether post‐treatment gains of CBT are maintained at longer‐term follow‐up.
To describe the age range of participants included in CBT trials in order to determine the age of the youngest participants.
To carry out subgroup analyses of different types of CBT according to 1) amount of therapist contact time; and 2) delivery format (individual and group; child‐focused, child and parent/family, and parent‐only).
To carry out a subgroup analysis of CBT for children and adolescents with ASD and for children and adolescents with intellectual impairments.
Methods
Criteria for considering studies for this review
Types of studies
We included randomised controlled trials (RCTs), cross‐over trials, and cluster‐randomised trials.
Types of participants
Participant characteristics
Children and adolescents younger than 19 years.
Diagnosis
We included participants meeting diagnostic criteria of the DSM (DSM III, III‐R, IV, IV‐TR, 5), APA 1980; APA 1987; APA 1994; APA 2000; APA 2013, or the ICD‐9 and ICD‐10, WHO 1978; WHO 1992, for an anxiety disorder.
Diagnoses had to be made by reliable and valid structured interviews for DSM or ICD child and adolescent anxiety disorders. Disorders classified as anxiety disorders vary across different versions of the DSM, and we included participants meeting diagnostic criteria for one or more of the following disorders: generalised anxiety disorder or overanxious disorder, separation anxiety disorder, social phobia or social anxiety disorder, panic disorder, agoraphobia, simple or specific phobias, or selective mutism.
Comorbidity
We included all comorbidities allowable for anxiety disorders under the rules of DSM or ICD, such as ASD, intellectual impairment, depressive disorders, and physical disorders.
Settings
We included all settings, such as research settings (i.e. university outpatient clinics, inpatient services, community clinics, and schools).
Exclusion criteria
We excluded studies that only included participants with post‐traumatic stress disorder or obsessive compulsive disorder, or both, as they are covered by separate Cochrane Reviews (Gillies 2016; O'Kearney 2006), and are no longer classified as ‘anxiety disorders’ in the DSM‐5 (APA 2013).
Types of interventions
Experimental intervention
The intervention had to be manualised CBT, or modular CBT, alone or in combination with medication, following a documented, written protocol and provided by trained therapists. Since the last review (James 2015), where the number of sessions was arbitrarily fixed at nine, there are now several studies indicating that shorter treatment, in terms of number of sessions or duration of sessions, or both, may be effective. We therefore did not include a minimum number of sessions or duration of sessions as a requirement.
CBT had to be administered according to standard principles as a psychological model of treatment involving helping the child to recognise anxious feelings and somatic reactions to anxiety; identify cognitions in anxiety‐provoking situations; modify these anxiety‐provoking cognitions; and respond to behavioural training strategies with exposure in vivo or by imagination.
CBT could be delivered to children (child‐focused), to children and parents/family members (child and parent), or to parents alone (parent‐only). In child‐focused CBT, the child had direct face‐to‐face contact with a therapist, and the intervention was delivered to children only, with minimal or no parental involvement. CBT with direct parent/family involvement (child and parent) included face‐to‐face child sessions and conjoint or separate sessions with parents/family that included providing psycho‐education for parents or teaching parents to be co‐therapists. Parent‐delivered CBT (parent‐only) only involved direct face‐to‐face contact with parents, and provided support for parents to help them to implement CBT strategies in their child’s day‐to‐day life. Child‐focused, child and parent, and parent‐only CBT could be delivered individually or in a group format. We did not include CBT interventions delivered online or via digital devices (e.g. computerised CBT).
Where studies included medication for the treatment of anxiety (in combination with CBT or alone), no concurrent medication for the treatment of anxiety was to be administered naturalistically. Where studies did not include medication for the treatment of anxiety, any medications administered naturalistically needed to be stable before and during the study.
Comparator interventions
Where CBT was delivered alone
Waitlist and no treatment for anxiety during that period
Treatment as usual (usual treatment or care; where usual care includes therapy, it does not include elements of CBT)
Attention control (attention only, e.g. support or education, but with no elements of CBT)
Alternative treatment (one specific non‐pharmacological intervention for the treatment of anxiety that followed a documented protocol and did not include CBT elements)
Medication for the treatment of anxiety
Drug placebo
Where CBT was delivered in combination with medication for the treatment of anxiety
Drug placebo
Types of outcome measures
We included studies that met the above inclusion criteria and reported or provided data on at least one of the following outcomes.
Primary outcomes
-
Remission: the absence of the primary diagnosis of an anxiety disorder post‐treatment, made by reliable and valid structured interviews for DSM or ICD child and adolescent anxiety disorders, such as:
Anxiety Disorder Interview Schedule for Children – Child and Parent (ADIS‐C/P) (Silverman 1987);
Anxiety Disorder Interview Schedule for Children – Child (ADIS‐C) (Silverman 1987);
Anxiety Disorder Interview Schedule for Children – Parent (ADIS‐P) (Silverman 1987);
Diagnostic Interview Schedule for Children, Adolescents and Parents (DISCAP) (Holland 1995).
Acceptability: loss of participants to post‐treatment assessment
Secondary outcomes
Remission: defined as the absence of all diagnoses of an anxiety disorder post‐treatment, made by reliable and valid structured interviews for DSM or ICD child and adolescent anxiety disorders.
-
Reduction in anxiety symptoms post‐treatment: measured using psychometrically robust measures of anxiety symptoms that yield symptom scores on continuous scales (Myers 2002), such as:
Screen for Child Anxiety Related Emotional Disorders (SCARED) (Birmaher 1999);
Spence Children’s Anxiety Scale (SCAS) (Spence 1997);
Revised Children’s Anxiety and Depression Scale (RCADS) – Anxiety Scale (Chorpita 2000);
Revised Children’s Manifest Anxiety Scale (RCMAS) (Reynolds 1985);
Multidimensional Anxiety Scale for Children (MASC) (March 1997);
State‐Trait Anxiety Inventory for Children (STAI‐C) (Spielberger 1973);
Social Phobia and Anxiety Inventory for Children (SPAI‐C) (Beidel 1995);
Social Anxiety Scale for Adolescents (SAS‐A) (La Greca 1998).
These scales could be self‐report or completed by a parent or an independent rater. Multiple reporters are often used, but the reliability of each reporter is likely to vary with the child’s age (Evans 2017). We therefore determined reduction in anxiety symptoms separately for 1) self‐reported and 2) parent‐reported or independent rater, or both. Multiple measures are also often reported, and we included the most validated, best recognised, or most frequently used measures in the analysis.
A crucial issue is how well these measures discriminate between clinical and non‐clinical levels of anxiety. We prioritised symptom measures that were closely aligned with diagnostic categories, with strong discriminant validity (e.g. RCADS, SCAS, SCARED). We also prioritised broad measures of anxiety symptoms (e.g. SCAS, SCARED, MASC), rather than disorder‐specific symptom measures (e.g. SPAI‐C, SAS‐A). (See Appendix 1)
-
Reduction in depressive symptoms post‐treatment: measured using psychometrically robust measures of depressive symptoms that yielded symptom scores on continuous scales, such as:
Children’s Depression Inventory (Kovacs 1989);
Beck Depression Inventory (Beck 1996);
Revised Children’s Anxiety and Depression Scale (RCADS) – Depression Scale (Chorpita 2000);
Mood and Feelings Questionnaire (Angold 1995).
If multiple depressive symptom measures/reporters were used, we included the most validated, best recognised, or most frequently used measures in the analysis.
-
Improvement in global functioning post‐treatment: measured using psychometrically robust measures of global functioning that yield symptom scores on continuous scales, such as:
Children’s Global Assessment Scale (CGAS) (Shaffer 1983).
If multiple global functioning measures/reporters were used, we included the most validated, best recognised, or most frequently used measures in the analysis.
Adverse events: we determined adverse events outcomes by the number and type of reported adverse events during the trial from randomisation to post‐treatment assessment (e.g. deterioration in anxiety symptoms, deterioration in global functioning, rates of self‐harm, suicide attempts).
Remission defined by the absence of the primary anxiety disorder diagnosis at a series of follow‐up time points (≤ 6 months post‐treatment, > 6 months post‐treatment but ≤ 12 months post‐treatment, and > 12 months post‐treatment).
Remission defined as the absence of all diagnoses of an anxiety disorder at a series of follow‐up time points (≤ 6 months post‐treatment, > 6 months post‐treatment but ≤ 12 months post‐treatment, and >12 months post‐treatment).
Reduction in anxiety symptoms at a series of follow‐up time points (≤ 6 months post‐treatment, > 6 months post‐treatment but ≤ 12 months post‐treatment, and > 12 months post‐treatment).
Search methods for identification of studies
We identified eligible studies (RCTs) of CBT for anxiety disorders in children and adolescents from the Cochrane Common Mental Disorders Controlled Trials Register (CCMDCTR; all years to 2016) (Appendix 2).
Electronic searches
We also ran searches on the following databases using relevant keywords, subject headings (controlled vocabularies), and search syntax, appropriate to each resource (Appendix 3). Searches were initially conducted on 21 November 2018 and updated 10 October 2019.
Cochrane Central Register of Controlled Trials (CENTRAL; Issue 10 of 12, 2019) in the Cochrane Library
Ovid MEDLINE (2016 to 10 October 2019)
Ovid Embase (2016 to 2019 Week 40)
Ovid PsycINFO (all years to October Week 40 2019)
We applied no restriction on language or publication status to the searches.
We also searched the international trial registries (10 October 2019) (including US National Institutes of Health Ongoing Trials Register ClinicalTrials.gov (clinicaltrials.gov) and the World Health Organization International Clinical Trials Registry Platform (apps.who.int/trialsearch/)) to identify additional ongoing and unpublished studies.
Searching other resources
Grey literature
We searched the grey literature for dissertations and theses (all years to 14 October 2019) (Appendix 4), as follows.
Electronic Theses Online Service (EThOS) ‐ British Library (ethos.bl.uk/Home.do)
DART ‐ Europe e‐theses Portal (www.dart-europe.eu/basic-search.php)
Networked Digital Library of Theses and Dissertations (NDLTD) (search.ndltd.org/)
PQDT Open ‐ open access dissertations and theses (pqdtopen.proquest.com/search.html)
Proquest Dissertations & Theses Global (search.proquest.com/pqdtglobal/dissertations/)
Reference lists
We checked the reference lists of all included studies and relevant systematic reviews to identify additional studies missed from the original electronic searches (e.g. unpublished or in‐press citations).
Correspondence
We contacted study authors and subject experts for information on unpublished or ongoing studies, or to request additional data. Where studies included some eligible participants (i.e. some participants were younger than 19 years, or some participants met the diagnostic criteria for an anxiety disorder), we contacted the authors to request data on eligible participants.
Data collection and analysis
Selection of studies
Two review authors (AJ, TR) independently screened the titles and abstracts of all studies identified as a result of the search, coding them as ‘retrieve' (eligible or potentially eligible/unclear) or ‘do not retrieve'. We retrieved the full‐text study reports/publications, and two review authors (AJ, TR) independently screened the full texts to identify studies for inclusion, and identified and recorded reasons for exclusion of the ineligible studies. Any disagreements were resolved through discussion or by consulting a third review author (GJ, AS, CC) if required. We identified and excluded duplicate records and collated multiple reports that related to the same study so that each study, rather than each report, was the unit of interest in the review. We recorded the selection process in sufficient detail to complete a PRISMA flow diagram and ‘Characteristics of excluded studies' table (Moher 2015). We used Covidence software for the screening process (Covidence).
Data extraction and management
We used a data collection form created in Covidence to extract study characteristics and outcome data that we had piloted on two studies in the review. Two review authors (AJ, TR) extracted study characteristics and outcome data from the included studies. We extracted the following study characteristics.
Methods: study design, total duration of study, details of any ‘run‐in' period, number of study centres and location, study setting, withdrawals, and date of study
Participants: number, mean age, age range, gender, severity of condition, diagnostic criteria, comorbid conditions, inclusion criteria, and exclusion criteria
Interventions: intervention, comparison, concomitant medications, excluded medications, delivery format, therapist contact time, who delivers intervention
Outcomes: primary and secondary outcomes specified and collected, and time points reported
Notes: funding for study, and notable conflicts of interest of study authors
We noted in the ‘Characteristics of included studies' table if outcome data were not reported in a useable way. Any disagreements were resolved by consensus or by involving a third review author (GJ, AS, CC). One review author (TR) transferred data into the Review Manager 5 file (Review Manager 2014). We double‐checked that data were entered correctly by comparing the data presented in the systematic review with the study reports. A second review author (AJ) spot‐checked study characteristics for accuracy against the study report.
Main comparisons
CBT compared with waiting list and no treatment controls
CBT compared with treatment as usual
CBT compared with attention control
CBT compared with alternative treatments
CBT compared with medication or drug placebo
CBT and medication combination compared with drug placebo
Assessment of risk of bias in included studies
Two review authors (AJ, TR) independently assessed risk of bias for each study using the criteria outlined in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2017). Any disagreements were resolved by discussion or by involving another review author (GJ, CC). We assessed risk of bias according to the following domains.
Random sequence generation
Allocation concealment
Blinding of participants and personnel
Blinding of outcome assessment
Incomplete outcome data
Selective outcome reporting
Other bias, including therapy integrity
We judged each potential source of bias as low, high, or unclear and provided a supporting quotation from the study report together with a justification for our judgement in the ‘Risk of bias' table. We summarised the 'Risk of bias' judgements across different studies for each of the domains listed.
Selection bias: we assessed the adequacy of the randomisation process in terms of the description of adequacy of sequence generation and the concealment of treatment group allocation.
Performance bias: given the nature of psychological interventions, blinding of either participants or personnel delivering the treatments could only be possible in studies involving CBT versus treatment as usual, attention control, or alternative treatment, therefore we were only able to assess attempts at blinding in those studies.
Detection bias: we evaluated whether study personnel carrying out outcome assessments were blinded to the treatment status of participants.
Attrition bias: we determined whether studies provided a description of withdrawals and dropouts.
Other bias: we also assessed therapy integrity, including therapist competence and adherence to treatment protocol, for all included studies.
We did not exclude studies from meta‐analysis on the basis of the ‘Risk of bias’ assessment. We conducted sensitivity analyses for the primary outcome, excluding trials with high or unclear risk of bias ratings for allocation concealment, and excluding trials with high or unclear risk of bias for blinding of outcome assessment if appropriate. We reported the remainder of the ‘Risk of bias' assessments for these trials, and included discussion of this assessment in the Results and Discussion sections.
Measures of treatment effect
In order to assess post‐treatment outcomes, we used dichotomous data on remission of primary anxiety diagnosis and all anxiety diagnoses, and continuous data on anxiety symptoms, depressive symptoms, and global functioning, with the use of standardised measures. We used data from the assessment administered immediately after treatment (or the assessment closest to the end of treatment) to assess post‐treatment outcomes. We also used these measures to evaluate the maintenance of treatment effects at a series of follow‐up time points (≤ 6 months post‐treatment, > 6 months post‐treatment but ≤ 12 months post‐treatment, and > 12 months post‐treatment). Where studies reported follow‐up data at multiple time points within one category (e.g. one‐month and three‐month follow‐up), we used data from the longer follow‐up period. To assess acceptability, we used frequency data on the numbers of participants who were lost to post‐treatment assessment. Adverse events were determined by the number and type of adverse events during the trial, from randomisation to the post‐treatment assessment.
Dichotomous data
We analysed dichotomous data as odds ratios (OR) and 95% confidence intervals (CI).
Continuous data
We analysed continuous data as mean difference (MD) or standardised mean difference (SMD). We entered data presented as a scale with a consistent direction of effect.
We narratively described skewed data reported as medians and interquartile ranges.
Unit of analysis issues
Cluster‐randomised trials
We included cluster‐randomised controlled trials based in schools. Cluster‐randomised trials can, in principle, be combined with individually randomised trials in the same meta‐analysis (Deeks 2017). We did not anticipate that there would be many cluster‐randomised trials, therefore we included identified cluster‐randomised trials in the meta‐analyses and sensitivity analyses that we planned to undertake to investigate the robustness of any conclusions drawn. To correct the influence of any cluster trials, we used an average intraclass correlation coefficient of 0.02 (Health Services Research Unit 2004).
The effective sample size of a single intervention group in a cluster‐randomised trial is its original sample size divided by the ‘design effect’. The design effect is 1 + (M − 1) ICC, where M is the average cluster size and ICC is the intracluster correlation coefficient (Rao 1992). For dichotomous data, we divided both the number of participants and the number experiencing the event by the same design effect. For continuous data, only the sample size was reduced; we did not alter means and standard deviations (SDs).
Cross‐over trials
We did not anticipate that there would be many cross‐over trials, and the data required to include a paired analysis in a meta‐analysis is often not reported (Higgins 2011). We therefore planned to include any identified cross‐over trials in the meta‐analysis, but only data from the first trial period (i.e. prior to the ‘cross‐over').
Studies with multiple treatment groups
Where multiple trial arms were reported in a single trial, we included only the relevant arms. Studies with more than two intervention arms can pose analytical problems in pair‐wise meta‐analysis. Where studies had two or more relevant active treatment arms to be compared against controls, we managed data as follows.
Continuous data
We divided the control group equally into two or more groups to compare the means and SDs of these groups against the means and SDs of the two treatment arms.
Dichotomous data
For trials with two or more active treatment arms and a control group, we split participants in the control arm group equally between the active treatment arms.
Dealing with missing data
We contacted investigators or study sponsors in order to verify key study characteristics and to obtain missing numerical outcome data where possible (e.g. when we identified a study as abstract only, when a study included a post‐treatment diagnostic assessment but did not report the required remission outcomes, or when a study did not report standard errors or SDs). We documented all correspondence with study authors and reported which study authors responded to our queries.
Missing statistics
In the first instance, we attempted to contact the original researchers for any missing data. If the study only reported standard errors, we calculated SDs.
Missing participants
We undertook intention‐to‐treat (ITT) analyses. When analysing dichotomous data, we assumed that all non‐completers in the CBT group were treatment failures, and non‐completers in the control group were treatment successes, thereby yielding the most conservative treatment estimate.
For dichotomous outcomes, we also undertook completer analysis, using only data from participants who completed post‐treatment assessments.
We did not use any statistical or other methods to impute missing data for continuous outcomes, as we did not have access to raw data.
Assessment of heterogeneity
We assessed clinical heterogeneity by comparing differences in the distribution of important participant factors between studies (e.g. age, gender, specific diagnosis, duration and severity of disorder, associated comorbidities). We assessed methodological heterogeneity by comparing trial factors (randomisation, concealment, blinding of outcome assessment, losses to follow‐up). We used the Chi² test, Deeks 2017, and the I² statistic, Higgins 2003, to assess heterogeneity. We set significance at P < 0.1. The Cochrane Handbook for Systematic Reviews of Interventions recommends using a range for the I² statistic and a guide to interpretation (Deeks 2017). If we found either moderate heterogeneity (I² in the range of 30% to 60%) or substantial heterogeneity (I² in the range of 60% to 90%), we performed subgroup and sensitivity analyses where possible.
Assessment of reporting biases
Where a minimum of 10 studies were included, we investigated publication bias using funnel plots, Sterne 2017, and subjected any asymmetry found to statistical investigation using Egger’s test (Stata 2012).
Data synthesis
We undertook meta‐analyses only where this was meaningful, that is if the treatments, participants, and the underlying clinical question were similar enough for pooling to make sense. We undertook ITT and completer analyses.
We planned to carry out separate analyses to identify whether CBT was more effective post‐treatment than waiting list/no treatment; treatment as usual, attention controls, alternative treatments, medication; and drug placebo; and also to identify whether CBT in combination with medication was more effective than drug placebo.
We used follow‐up data for each comparison to assess maintenance of treatment gains. If it was meaningful to do so, we pooled data separately for each follow‐up time point (≤ 6 months post‐treatment, > 6 months post‐treatment but ≤ 12 months post‐treatment, and > 12 months post‐treatment). Where studies reported follow‐up data at multiple time points within one category (e.g. 9‐month and 12‐month follow‐up), we included data from the longer follow‐up period.
Dichotomous data
We used ORs and 95% CIs based on the random‐effects model, with pooling of data via the inverse variance method of weighting. We set significance at P < 0.05. Where available, we used combined data from an interview with the child or adolescent and the parent; otherwise we used data from one interview (child/adolescent or parent interview). We calculated the number needed to treat for an additional beneficial outcome (NNTB) with 95% CIs (Stata 2012). We calculated a summary statistic of all those responding to treatment as a percentage of the total number of participants for each comparison.
Continuous data
We conducted analysis of continuous data based on the random‐effects model, with pooling of data via the inverse variance method of weighting. We used the SMD to pool continuous data measured in different ways across studies but conceptually the same (i.e. measuring anxiety or depressive symptoms or global functioning). For continuous data measuring anxiety symptoms, we pooled child/adolescent report and parental/clinician reports separately. Where both endpoint and change data were available for the same outcome, we presented the endpoint. We set significance at P < 0.05.
Tables and figures
We transferred data into Review Manager 5 (Review Manager 2014), and presented them graphically, so that the area to the left of the line of no effect (or right for remission outcomes) indicated a favourable outcome for CBT. We used tables to display characteristics of the included studies. We presented a brief list of excluded studies in a table with their reasons for exclusion. We summarised risk of bias in the included studies in a figure, and included a PRISMA flow chart (Moher 2015).
Subgroup analysis and investigation of heterogeneity
The critical need to improve access to treatment for child anxiety disorders means that it is particularly important to explore the efficacy of approaches that may help maximise treatment efficiency, including alternative delivery formats and briefer interventions that involve less therapist contact time than traditional approaches. As outlined above, there are also unanswered questions in relation to the benefits of CBT for children and adolescents with ASD and intellectual impairments. We therefore set out to explore the efficacy of different delivery formats and of briefer and shorter interventions, and to examine treatment effects amongst children and adolescents with ASD and those with intellectual impairment, using subgroup analyses. Specifically, where it was possible and meaningful to do so, we undertook subgroup analyses to examine differences between:
delivery formats (child‐focused, child and parent, and parent‐only; individual and group);
interventions with a varying amount of therapist contact time (< 10 hours, ≥ 10 hours and < 20 hours, ≥ 20 hours);
children and adolescents with and without ASDs;
children and adolescents with and without intellectual impairments.
To examine differences between age groups, we also undertook post hoc subgroup analyses evaluating the differences between studies where all participants were age 12 or younger (≤ 12 years); all participants were age 12 or older (≥ 12 years); and studies that included participants under and over age 12 (< 12 years and ≥ 12 years).
We undertook subgroup analyses for the primary outcome (remission of primary anxiety disorder) across comparisons. For the main comparison with the largest number of studies (CBT versus waitlist/no treatment), we also undertook subgroup analyses for the most frequently reported secondary outcomes (remission of all anxiety diagnoses post‐treatment and reduction in child‐ and parent‐reported anxiety symptoms post‐treatment). To ensure subgroup analyses were meaningful, we only undertook these analyses where there were data from at least three studies for each subgroup.
We assessed statistical heterogeneity for all analyses and between groups with the Chi2 test and the I2 statistic, and set significance at P < 0.1.
Sensitivity analysis
Sensitivity analysis is the study of how the uncertainty in the output of an analysis can be apportioned to different sources of uncertainty in its inputs. Sensitivity analyses can therefore be carried out to test the robustness of decisions made in the review process. We carried out sensitivity analyses where there was evidence of the following:
significant heterogeneity: we inspected forest plots and examined each study in turn to determine the source of any significant heterogeneity;
selection bias: we excluded those studies judged to be at high risk of selection bias from the main analysis;
allocation concealment: we excluded those studies judged to be at high risk of bias for allocation concealment from the main analysis.
Where appropriate, we undertook all of the above sensitivity analyses for the ITT and completer analyses.
Where meta‐analyses examining anxiety symptoms included broad measures of anxiety symptoms and disorder‐specific symptom measures, we also undertook sensitivity analyses excluding studies that only reported disorder‐specific symptom measures.
GRADE and ‘Summary of findings' table
We created a ‘Summary of findings' table including the following primary outcomes:
remission of primary anxiety diagnosis post‐treatment;
acceptability in terms of dropouts from randomisation to the post‐treatment assessment;
and the following secondary outcomes:
remission of all anxiety diagnoses post‐treatment;
reduction in anxiety symptoms (self‐reported and parent‐reported) post‐treatment;
reduction in depressive symptoms post‐treatment;
improvement in global functioning post‐treatment;
adverse events from randomisation to the post‐treatment assessment.
We used the five GRADE considerations (study limitations, consistency of effect, imprecision, indirectness, and publication bias) to assess the quality of a body of evidence as it relates to the studies that contribute data to the meta‐analyses for the prespecified primary and secondary outcomes. Two review authors (AJ, TR) independently assessed risk of bias, and in case of disagreement sought consensus between four review authors (AJ, TR, GJ, CC). We used the methods and recommendations described in Section 8.5, Higgins 2017, and Chapter 12, Schünemann 2017, of the Cochrane Handbook for Systematic Reviews of Interventions, employing GRADEpro GDT software (GRADEpro GDT). We justified all decisions to downgrade or upgrade the quality of studies using footnotes, and made comments to aid the reader's understanding of the review where necessary. We considered whether there was any additional outcome information that could not be incorporated into the meta‐analyses, noting this in the comments and stating if it supported or contradicted the information from the meta‐analyses.
Results
Description of studies
See Characteristics of included studies and Table 5.
1. Summary of characteristics of included studies.
| Study | Comparison 1 | Comparison 2 | Comparison 3 | Broad vs specific anxiety measure | Delivery mode | Delivery mode | ASD vs not ASD | Therapist contact time (hours) | Age | Setting | Disorder‐specific | Other comorbid conditions (required) |
| Afshari 2014 | CBT vs Wait list / no treatment | CBT vs Wait list / no treatment | Broad | Child focused | Group | Not ASD | 10 to 20 | mix | clinic | |||
| Arendt 2016 | CBT vs Wait list / no treatment | Broad | Child+parent | Group | Not ASD | 20+ | mix | clinic (university) | ||||
| Barrett 1996 | CBT vs Wait list / no treatment | CBT vs Wait list / no treatment | Broad | Child focused and child+parent | Individual | Not ASD | 10 to 20 | mix | clinic (university) | |||
| Barrett 1998 | CBT vs Wait list / no treatment | CBT vs Wait list / no treatment | Child focused and child+parent | Group | Not ASD | 20+ | mix | clinic (university) | ||||
| Barrington 2005 | CBT vs TAU | Broad | Child+parent | Individual | Not ASD | 10 to 20 | mix | clinic (CAMHS) | ||||
| Berge 2017 | CBT vs Wait list / no treatment | Specific | Child focused | Individual | Not ASD | less than 10 | mix | clinic ‐dental | Specific Phobia | |||
| Cartwright Hatton 2011 | CBT vs Wait list / no treatment | Parent only | Group | Not ASD | 20+ | ≤ 12 | clinic‐university hospital | |||||
| Chalfant 2007 | CBT vs Wait list / no treatment | Broad | Child+parent | Group | ASD | 20+ | mix | clinic | ||||
| Cheung 2016 | CBT vs Wait list / no treatment | CBT vs Alternative treatment | Broad | Child focused | Individual | Not ASD | 10 to 20 | ≤ 12 | clinic‐CAMHS | |||
| Chiu 2013 | CBT vs Wait list / no treatment | Broad | Child focused | Individual | Not ASD | 10 to 20 | ≤ 12 | school | ||||
| Cobham 2017 | CBT vs Wait list / no treatment | Broad | Parent only | Group | Not ASD | less than 10 | mix | clinic (university) | ||||
| Cornacchio 2019 | CBT vs Wait list / no treatment | Child+parent | Group | Not ASD | 20+ | ≤ 12 | clinic | Selective mutism | ||||
| Creswell 2017 | CBT vs Alertnative treatment | Broad | Parent only | Individual | Not ASD | less than 10 | ≤ 12 | clinic (CAMHS) | ||||
| Dadds 1997 | CBT vs Wait list / no treatment | Broad | Child focused | Group | Not ASD | 10 to 20 | mix | school | ||||
| Flannery Schroeder 2000 | CBT vs Wait list / no treatment | CBT vs Wait list / no treatment | Broad | Child focused | Individual and group | Not ASD | 10 to 20 and 20+ | mix | clinic (university) | |||
| Fujii 2013 | CBT vs TAU | Child+ parent | Individual | ASD | 20+ | ≤ 12 | clinic | |||||
| Gallagher 2004 | CBT vs Wait list / no treatment | Broad | Child focused | Group | Not ASD | less than 10 | ≤ 12 | clinic | Social anxiety disorder | |||
| Ginsburg 2002 | CBT vs Attention control | Broad | Child focused | Group | Not ASD | less than 10 | ≥ 12 | school | ||||
| Ginsburg 2012 | CBT vs TAU | Broad | Child focused | Individual | Not ASD | less than 10 | mix | school | ||||
| Ginsburg 2019 | CBT vs TAU | Child focused | Individual | Not ASD | less than 10 | mix | school | |||||
| Hancock 2018 | CBT vs Wait list / no treatment | CBT vs Wait list / no treatment | Broad | Child +parent | Group | Not ASD | 10 to 20 | mix | clinic (university) | |||
| Herbert 2009 | CBT vs Attention control | CBT vs Attention control | Specific | Child focused | Group and Individual | Not ASD | 20+ and 10 to 20 | ≥ 12 | clinic (university) | Social anxiety disorder | ||
| Hirshfeld Becker 2010 | CBT vs Wait list / no treatment | Child + parent | Individual | Not ASD | 20+ | ≤ 12 | clinic (university) | |||||
| Holmes 2014 | CBT vs Wait list / no treatment | Broad | Child + parent | Group | Not ASD | 10 to 20 | ≤ 12 | clinic (university) | GAD | |||
| Hudson 2009 | CBT vs Attention control | Broad | Child +parent | Group | Not ASD | 20+ | mix | clinic (university) | ||||
| Ingul 2003 | CBT vs Attention control | CBT vs Attention control | Broad | Child focused | Individual and Group | Not ASD | 10 to 20 | ≥ 12 | schools | Social anxiety disorder | ||
| Ishikawa 2019 | CBT vs Wait list / no treatment | Broad | Child +parent | Individual | Not ASD | less than 10 | mix | clinic | ||||
| Kendall 1994 | CBT vs Wait list / no treatment | Broad | Child focused | Individual | Not ASD | 10 to 20 | mix | clinic (university) | ||||
| Kendall 1997 | CBT vs Wait list / no treatment | Broad | Child focused | Individual | Not ASD | 10 to 20 | mix | clinic (university) | ||||
| Kendall 2008 | CBT vs Attention control | CBT vs Attention control | Broad | Child focused and child+parent | Individual | Not ASD | 10 to 20 | mix | clinic (university) | |||
| Kennedy 2009 | CBT vs Wait list / no treatment | Broad | Parent only | Group | Not ASD | 10 to 20 | ≤ 12 | clinic (university) | ||||
| Khanna 2010 | CBT vs Attention control | Broad | Child focused | Individual | Not ASD | 10 to 20 | mix | clinic (university) | ||||
| Kidd 2018 | CBT vs Wait list / no treatment | Broad | Child + parent | Group | ASD | 20+ | ≥ 12 | clinic (university) | ||||
| Last 1998 | CBT vs Attention control | Broad | Child and parent | Individual | Not ASD | 10 to 20 | mix | clinic (university) | School refusal | |||
| Lau 2010 | CBT vs Wait list / no treatment | Broad | Child focused | Group | Not ASD | 10 to 20 | ≤ 12 | clinic | ||||
| Lau 2017 | CBT vs Wait list / no treatment | Broad | Child +parent | Group | Not ASD | 10 to 20 | ≤ 12 | child centres and preschools | ||||
| Lebowitz 2019 | CBT vs Alternative treatment | Broad | Child focused | Individual | Not ASD | 10 to 20 | ≤ 12 | clinic | ||||
| Leutgeb 2012 | CBT vs Wait list / no treatment | Broad | Child focused | Individual | Not ASD | less than 10 | mix | university | Specific Phobia | |||
| Masia Warner 2005 | CBT vs Wait list / no treatment | Specific | Child focused | Group focused | Not ASD | 10 to 20 | ≥ 12 | School | Social anxiety disorder | |||
| Masia Warner 2007 | CBT vs Attention control | Specific | Child focused | Group focused | Not ASD | 10 to 20 | ≥ 12 | School | Social anxiety disorder | |||
| Masia Warner 2011 | CBT vs Wait list / no treatment | Child focused | Individual | Not ASD | 10 to 20 | mix | primary care/special clinic | functional physical complaints | ||||
| Masia Warner 2016 | CBT vs Attention control | CBT vs Attention control | Specific | Child focused | Group focused | Not ASD | 10 to 20 | ≥ 12 | School | Social anxiety disorder | ||
| McConachie 2014 | CBT vs Wait list / no treatment | Broad | Child + parent | Group | ASD | 20+ | mix | clinic (university) | ||||
| McNally Keehn 2013 | CBT vs Wait list / no treatment | Broad | Child focused | Individual | ASD | 20+ | mix | clinic (university) | ||||
| Melfsen 2011 | CBT vs Wait list / no treatment | Specific | Child and parent | Individual | Not ASD | 20+ | mix | clinic | Social anxiety disorder | |||
| Muris 2002 | CBT vs Attention control | Broad | Child focused | Group | Not ASD | less than 10 | ≤ 12 | school | ||||
| Murphy 2017 | CBT vs Alternative treatment | Broad | Child focused | Individual focused | ASD | 10 to 20 | ≥ 12 | CAMHS | ||||
| O'Brien 2007 | CBT vs TAU | Child and parent | Group | Not ASD | 10 to 20 | mix | clinic | |||||
| Olivares 2005 | CBT vs Wait list / no treatment | Specific | Child focused | Group | Not ASD | 10 to 20 | ≥ 12 | school | Social anxiety disorder | |||
| Olivares 2014 | CBT vs Wait list / no treatment | CBT vs Wait list / no treatment | Specific | Child focused | Group | Not ASD | 10 to 20 | ≥ 12 | school | Social anxiety disorder | ||
| Olivares 2019 | CBT vs Wait list / no treatment | CBT vs Wait list / no treatment | Child focused | Group | Not ASD | 10 to 20 | ≥ 12 | school | Social anxiety disorder | |||
| Ollendick 2009 | CBT vs Wait list / no treatment | CBT vs Attention control | Broad | Child focused | Individual | Not ASD | less than 10 | mix | clinic | Specific Phobia | ||
| Ost 2001 | CBT vs Wait list / no treatment | CBT vs Wait list / no treatment | Broad | Child focused and child+parent | Individual | Not ASD | less than 10 | mix | referrals from clinic and schools | Specific Phobia | ||
| Perrin 2019 | CBT vs Wait list / no treatment | Broad | Child focused | Individual | Not ASD | 10 to 20 | mix | CAMHS | GAD | |||
| Pincus 2010 | CBT vs Attention control | Broad | Child focused | Individual | Not ASD | less than 10 | ≥ 12 | clinic (university) | Panic Disorder | |||
| Rapee 2005 | CBt vs Wait list / no treatment | Broad | Parent only | Group | Not ASD | less than 10 | ≤ 12 | preschools | ||||
| Rapee 2006 | CBT vs Wait list / no treatment | Broad | Child+parent | Group | Not ASD | 10 to 20 | ≤ 12 | clinic (university) | ||||
| Reaven 2012 | CBT vs TAU | Child+parent | Group | ASD | 10 to 20 | mix | clinic (university) | |||||
| Reigada 2015 | CBT vs Alternative treatment | Specific | Child focused | Individual | Not ASD | 10 to 20 | mix | clinic (university) | IBD | |||
| Rosa‐Alcazar 2009 | Cbt vs Attention control | CBT vs Attention control | CBT vs Wait list / no treatment | Specific | Child focused | Group | Not ASD | 10 to 20 | ≥ 12 | School | Social anxiety disorder | |
| Salari 2018 | CBT vs Wait list / no treatment | Broad | Parent only | Group | Not ASD | 10 to 20 | ≤ 12 | clinic (university) | ||||
| Salum 2018 | CBT vs Attention control | CBT vs Alternative treatment | Broad | Child+parent | Group | Not ASD | 10 to 20 | ≤ 12 | clinic | |||
| Sanchez Garcia 2009 | CBT vs Wait list / no treatment | Specific | Child focused | Group | Not ASD | 10 to 20 | mix | School | Social anxiety disorder | |||
| Santucci 2013 | CBT vs Wait list / no treatment | Broad | Child +parent | Group | Not ASD | 20+ | ≤ 12 | clinic (university) | Separation anxiety disorder | |||
| Schneider 2011 | CBT vs Wait list / no treatment | Broad | Child +parent | Individual | Not ASD | 10 to 20 | ≤ 12 | clinic (university) | Separation anxiety disorder | |||
| Sciberras 2018 | CBT vs TAU | Broad | Child+parent | Individual | Not ASD | 10 to 20 | ≤ 12 | clinic ADHD | ADHD | |||
| Shahnavaz 2016 | CBT vs TAU | Specific | Child+parent | Individual | Not ASD | 10 to 20 | mix | dental clinics | Specific Phobia | |||
| Sharma 2017 | CBT vs TAU | Broad | Child focused | Group | Not ASD | 20+ | mix | clinic (university) | Headaches | |||
| Shortt 2001 | CBT vs Wait list / no treatment | Broad | Child+parent | Group | Not ASD | 10 to 20 | ≤ 12 | clinic (university) | ||||
| Silk 2018 | CBT vs Alternative treatment | Broad | Child focused | Individual | Not ASD | 10 to 20 | mix | |||||
| Silverman 1999a | CBT vs Attention control | Broad | Child+parent | Individual | Not ASD | 10 to 20 | mix | clinic (university) | ||||
| Silverman 1999b | CBT vs Wait list / no treatment | Broad | Child + parent | Group | Not ASD | 10 to 20 | mix | clinic (university) | ||||
| Simon 2011 | CBt vsWait list / no treatment | CBT vs Wait list / no treatment | Broad | Child focused and parent only | Group | Not ASD | less than 10 and 10 to 20 | mix | School | |||
| Smith 2014 | CBT vs Wait list / no treatment | Broad | Parent only | Individual | Not ASD | 10 to 20 | mix | clinic (university) | ||||
| Southam Gerow 2010 | CBT vs TAU | Broad | Child focused | Individual | Not ASD | 10 to 20 | mix | clinics | ||||
| Spence 2000 | CBT vs Wait list / no treatment | CBT vs Wait list / no treatment | Broad | Child focused and child+parent | Group | Not ASD | 20+ and 10 to 20 | mix | clinic (university) | Social anxiety disorder | ||
| Spence 2006 | CBT vs Wait list / no treatment | Broad | Child+parent | Group | Not ASD | 10 to 20 | mix | clinic (university) | ||||
| Spence 2011 | CBT vs Wait list / no treatment | Broad | Child+parent | Individual | Not ASD | 10 to 20 | ≥ 12 | clinic (university) | ||||
| Storch 2013 | CBT vs TAU | Broad | Child+parent | Individual | ASD | 20+ | ≤ 12 | clinic (university) | ||||
| Storch 2015 | CBT vs TAU | Broad | Child+parent | Individual | ASD | 20+ | ≥ 12 | clinic (university) | ||||
| Thirlwall 2013 | CBT vs Wait list / no treatment | CBT vs Wait list / no treatment | Broad | Parent only | Individual | Not ASD | less than 10 | ≤ 12 | clinic | |||
| Villabo 2018 | CBT vs Wait list / no treatment | CBT vs Wait list / no treatment | Broad | Child focused | Individual and Group | Not ASD | 10 to 20 | mix | clinic | |||
| Waters 2009 | CBT vs Wait list / no treatment | CBT vs Wait list / no treatment | Child+Parent and parent only | Group | Not ASD | 10 to 20 and 20 + | ≤ 12 | clinic (university) | ||||
| Wergelenad 2014 | CBT vs Wait list / no treatment | CBT vs Wait list / no treatment | Broad | Child+parent | Individual and group | Not ASD | 10 to 20 | mix | clinics‐CAMHS | |||
| White 2013 | CBT vs Wait list / no treatment | Broad | Child+parent | Individual | ASD | 20+ | ≥ 12 | clinic (university) | ||||
| Wood 2009 | CBT vs Wait list / no treatment | Broad | Child+parent | Individual | ASD | 20+ | mix | clinic (university) | ||||
| Wood 2015 | CBT vs Wait list / no treatment | Broad | Child+parent | Individual | ASD | 20+ | mix | clinic (university) |
ASD: autism spectrum disorders CBT: cognitive behavioural therapy GAD: generalised anxiety disorder TAU: treatment as usual
Results of the search
The initial database search (21 November 2018) identified 6354 records, and an updated database search (10 October 2019) identified a further 2081 records. A search of the grey literature identified a further 473 records, and an additional 38 records were identified from searching reference lists and correspondence with study authors and experts in the field.
After removing duplicates, we screened a total of 5488 titles/abstracts, and excluded 4746 records. We then assessed 742 full‐texts for eligibility for inclusion in the review, and identified 88 eligible studies (130 articles) (Figure 1).
1.
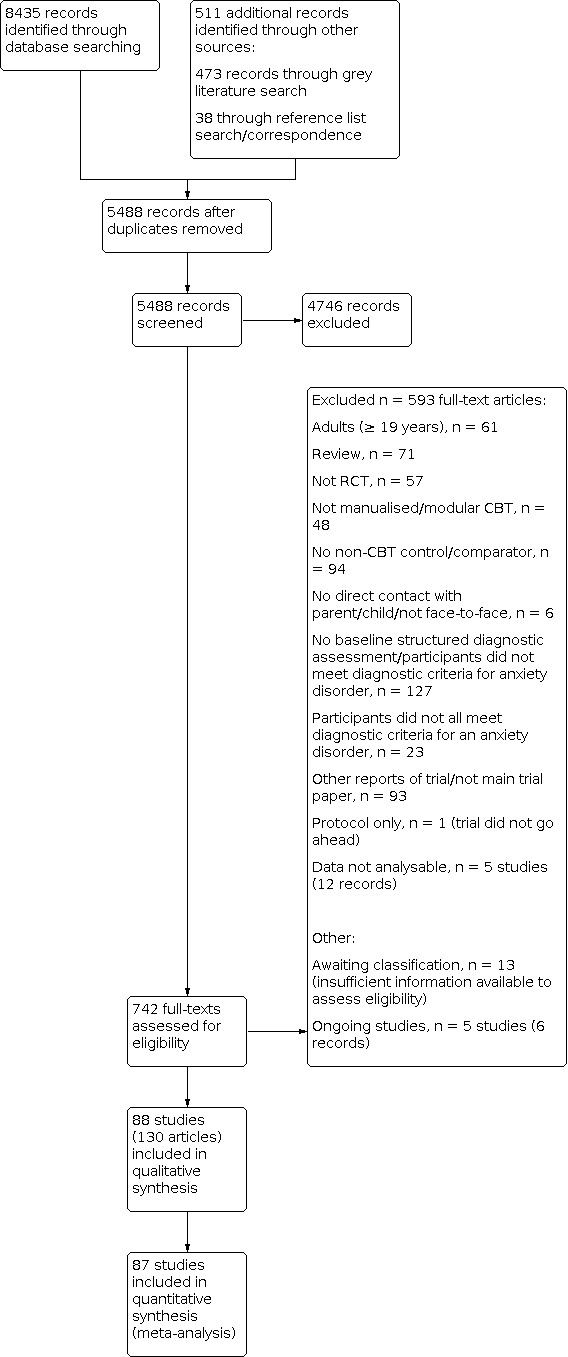
Study flow diagram.
We contacted 58 study authors for clarification or additional data, or both, and 16 study authors provided relevant outcome data for 20 of the included studies.
Included studies
Eighty‐eight studies met the criteria for inclusion in the review, and 87 studies were included in meta‐analyses.
Design
All included studies were RCTs. Two studies used a cluster‐randomised design, where schools, Dadds 1997, and school‐based clinicians, Ginsburg 2019a, were randomised, rather than individual participants. No included studies used a cross‐over design.
Amongst the studies included in meta‐analyses, 20 studies had two CBT arms (Afshari 2014; Barrett 1996; Barrett 1998; Cheung 2016; Flannery Schroeder 2000; Hancock 2018; Herbert 2009; Ingul 2013; Kendall 2008; Masia Warner 2016; Olivares 2014; Olivares 2019; Ost 2001; Salum 2018; Simon 2011; Spence 2000; Thirlwall 2013; Villabo 2018; Waters 2009; Wergeland 2014), including one factorial design (Salum 2018), and another three studies included multiple comparison arms (Cheung 2016; Ollendick 2009; Rosa Alcazar 2009).
Fifty‐seven studies were included in CBT versus waitlist/no treatment comparisons (Afshari 2014; Arendt 2016; Barrett 1996; Barrett 1998; Berge 2017; Cartwright Hatton 2011; Chalfant 2007; Cheung 2016; Chiu 2013; Cobham 2017; Cornacchio 2019; Dadds 1997; Flannery Schroeder 2000; Gallagher 2004; Hancock 2018; Hirshfeld Becker 2010; Holmes 2014; Ishikawa 2019; Kendall 1994; Kendall 1997; Kennedy 2009; Kidd 2018; Lau 2010; Lau 2017; Leutgeb 2012; Masia Warner 2005; Masia Warner 2011; McConachie 2014; McNally Keehn 2013; Melfsen 2011; Olivares 2005; Olivares 2014; Olivares 2019; Ollendick 2009; Ost 2001; Perrin 2019; Rapee 2005; Rapee 2006; Rosa Alcazar 2009; Salari 2018; Sanchez Garcia 2009; Santucci 2013; Schneider 2011; Shortt 2001; Silverman 1999b; Simon 2011; Smith 2014; Spence 2000; Spence 2006; Spence 2011; Thirlwall 2013; Villabo 2018; Waters 2009; Wergeland 2014; White 2013; Wood 2009; Wood 2015). With the exception of three studies (Dadds 1997; Rapee 2005; Simon 2011), participants assigned to the control arm were offered CBT after a waitlist period. Seven studies included eligible follow‐ups that included CBT and waitlist/no treatment participants. Follow‐up assessments were conducted between 3 and 24 months post‐treatment.
Twelve studies compared CBT to treatment as usual (TAU) (Barrington 2005; Fujii 2013; Ginsburg 2012; Ginsburg 2019a; O'Brien 2007; Reaven 2012; Sciberras 2018; Shahnavaz 2016; Sharma 2017; Southam Gerow 2010; Storch 2013; Storch 2015). TAU varied considerably across studies, ranging from eclectic non‐CBT therapeutic approaches or strategies that were offered as part of routine care (Barrington 2005; Ginsburg 2012; Ginsburg 2019a; Southam Gerow 2010), to allowing participants to continue and seek any psychosocial or pharmacological interventions (Fujii 2013; Reaven 2012; Storch 2013; Storch 2015). Four CBT versus TAU studies included 6‐month, 12‐month, or both 6‐ and 12‐month follow‐ups.
Fifteen studies compared CBT to an attention control (Ginsburg 2002; Herbert 2009; Hudson 2009; Ingul 2013; Kendall 2008; Khanna 2010; Last 1998; Masia Warner 2007; Masia Warner 2016; Muris 2002; Ollendick 2009; Pincus 2010; Rosa Alcazar 2009; Salum 2018; Silverman 1999a), which was designed to act as an attention condition, and often included a psychoeducation component. Six CBT versus attention control studies included follow‐ups up to 12 months.
Seven studies included a CBT versus an alternative treatment comparison (Cheung 2016; Creswell 2017; Lebowitz 2019; Reigada 2015; Salum 2018; Silk 2018). Alternative treatments designed to target children's anxiety difficulties included: solution‐focused therapy (Creswell 2017), the parent intervention SPACE (Supportive Parenting for Anxious Childhood Emotions) (Lebowitz 2019), child‐centred therapy (Silk 2018), counselling (Murphy 2017), non‐directive supportive therapy (Reigada 2015), and ABMT (Attention Bias Modification Treatment) (Cheung 2016; Salum 2018). Four CBT versus alternative treatment studies included follow‐ups up to 12 months post‐treatment.
Only one study compared CBT to medication, and CBT in combination with medication to drug placebo (Walkup 2008), therefore it was not possible to conduct meta‐analyses for these comparisons.
Sample size
The 87 studies included in meta‐analyses involved a total of 3492 CBT participants and 2472 controls (waitlist/no treatment controls, N = 1537; TAU, N = 260; attention control, N = 441; alternative treatment, N = 234).
Study sample sizes ranged from 12 participants, Ginsburg 2002; Sciberras 2018, to 206 participants (corrected sample size; Ginsburg 2019a).
Setting
Two‐thirds of the included studies were conducted in either the USA or Australia. The remaining studies were conducted in the UK, Spain, Norway, the Netherlands, Germany, Sweden, Iran, Brazil, Hong Kong, India, Japan, Denmark, and Ireland.
Most studies were conducted in clinical settings, either university research clinics (specified in 41 studies), community mental health clinics (specified in 12 studies), or dental clinics (Berge 2017; Shahnavaz 2016). Sixteen studies recruited participants through schools (Chiu 2013; Dadds 1997; Ginsburg 2002; Ginsburg 2012; Ginsburg 2019a; Ingul 2013; Masia Warner 2005; Masia Warner 2007; Masia Warner 2016; Muris 2002; Olivares 2005; Olivares 2014; Olivares 2019; Rosa Alcazar 2009; Sanchez Garcia 2009; Simon 2011), and two through preschools (Lau 2017; Rapee 2005). No studies were conducted in inpatient settings.
Participants
The included studies involved participants of varied ages. Sixteen studies focused on adolescents and only included participants aged 12 years or over (Ginsburg 2002; Herbert 2009; Ingul 2013; Kidd 2018; Masia Warner 2005; Masia Warner 2007; Masia Warner 2016; Murphy 2017; Olivares 2005; Olivares 2014; Olivares 2019; Pincus 2010; Rosa Alcazar 2009; Spence 2011; White 2013; Wood 2015). Twenty‐five studies included participants up to age 12 years (Cartwright Hatton 2011; Cheung 2016; Chiu 2013; Cornacchio 2019; Creswell 2017; Fujii 2013; Gallagher 2004; Hirshfeld Becker 2010; Holmes 2014; Kennedy 2009; Lau 2010; Lau 2017; Lebowitz 2019; Muris 2002; Rapee 2005; Rapee 2006; Salari 2018; Salum 2018; Santucci 2013; Schneider 2011; Sciberras 2018; Shortt 2001; Storch 2013; Thirlwall 2013; Waters 2009), including 5 studies where participants were all under 8 years of age (Hirshfeld Becker 2010; Kennedy 2009; Lau 2017; Rapee 2005; Schneider 2011). The youngest participants in the included studies were two to three years of age (Cartwright Hatton 2011; Kennedy 2009; Lau 2017; Rapee 2005). The remaining studies included participants both under and over 12 years.
All participants met the diagnostic criteria for at least one anxiety disorder. In most studies, any anxiety disorder, or a subset of anxiety disorders (e.g. generalised anxiety disorder (GAD), social anxiety disorder, or separation anxiety disorder) was required for inclusion. In five studies (Cartwright Hatton 2011; Creswell 2017; Dadds 1997; Rapee 2005; Simon 2011), not all study participants met the diagnostic criteria for an anxiety disorder, but only those who did were included in this review.
Twenty‐four studies focused on a specific anxiety disorder where participants all met the diagnostic criteria for the target anxiety disorder. Disorder‐specific studies included participants with social anxiety disorder (Gallagher 2004; Herbert 2009; Ingul 2013; Masia Warner 2005; Masia Warner 2007; Masia Warner 2016; Melfsen 2011; Olivares 2005; Olivares 2014; Olivares 2019; Rosa Alcazar 2009; Sanchez Garcia 2009; Spence 2000), specific phobia (Berge 2017; Leutgeb 2012; Ollendick 2009; Ost 2001; Shahnavaz 2016), separation anxiety disorder (Santucci 2013; Schneider 2011), GAD (Holmes 2014; Perrin 2019), panic disorder with/without agoraphobia (Pincus 2010), and selective mutism (Cornacchio 2019).
In some studies comorbid conditions were required for inclusion. Twelve studies included participants with an ASD (Chalfant 2007; Fujii 2013; Kidd 2018; McConachie 2014; McNally Keehn 2013; Murphy 2017; Reaven 2012; Storch 2013; Storch 2015; White 2013; Wood 2009; Wood 2015). Other comorbidities required for inclusion in individual studies included attention‐deficit/hyperactivity disorder (ADHD) (Sciberras 2018), school refusal (Last 1998), headaches (Sharma 2017), functional physical complaints (Masia Warner 2011), and inflammatory bowel disease (IBD) (Reigada 2015). No studies included samples of children with intellectual impairments.
Intervention
The most commonly used or adapted treatment manuals were Coping Cat (Kendall 1994), and Cool Kids (Hudson 2009; Rapee 2006). Studies targeting specific anxiety disorders used disorder‐specific interventions (e.g. OST (One‐Session Treatment) for specific phobias, IAFS (Intervention in Adolescents with Social Phobia) for social anxiety disorder), and studies targeting children with ASD (or another comorbidity) used adapted interventions developed specifically for the target population (e.g. BIACA (Behavioral Interventions for Anxiety in Children with Autism), TAPS (Treatment of Anxiety and Physical Symptoms)).
Delivery formats varied across the included studies, including child‐focused interventions (45 studies), interventions delivered to both children and parents (40 studies), and interventions delivered only to parents (10 studies). Approximately half of the CBT interventions involved a group format, including child‐focused interventions (e.g. Gallagher 2004; Ginsburg 2002; Olivares 2005), interventions delivered to children and parents (e.g. Hudson 2009; McConachie 2014; Waters 2009), and parent‐only interventions (e.g. Cartwright Hatton 2011; Cobham 2017; Rapee 2005).
The amount of therapist contact time also varied considerably in the included studies, ranging from under 10 hours (interventions in 16 studies, e.g. Creswell 2017; Ishikawa 2019; Ollendick 2009) to more than 20 hours (interventions in 23 studies, e.g. Herbert 2009; Sharma 2017; Storch 2015). The remaining interventions involved between 10 and 20 hours of therapist contact time.
Measures
The majority of included studies (70 out of 87) included in meta‐analyses used a post‐treatment diagnostic assessment, and reported (or provided) data on remission from primary and/or all anxiety disorders. In most cases, the Anxiety Disorder Interview Schedule for Children (ADIS‐C) was used, although there was variation in how it was administered, including either separate child and parent interviews (e.g. Spence 2011; Thirlwall 2013; Wergeland 2014), joint child and parent interviews (Barrington 2005; Ishikawa 2019; Khanna 2010), only child interviews (e.g. Ginsburg 2002; Olivares 2005; Sanchez Garcia 2009), or only parent interviews (e.g. Lau 2017; McNally Keehn 2013; Waters 2009). Alternative post‐treatment diagnostic assessments included: the Kinder‐DIPS (Melfsen 2011; Schneider 2011), Kiddie Schedule for Affective Disorders and Schizophrenia (K‐SADS) (Hirshfeld Becker 2010; Last 1998; Lau 2010; Silk 2018), Diagnostic Interview Schedule for Children, Adolescents and Parents (DISCAP) (Shortt 2001), Diagnostic Interview Schedule for Children (Southam Gerow 2010), an adapted version of the Development and Well‐Being Assessment (DAWBA) (Shahnavaz 2016), and the Mini‐KID (Sharma 2017).
Anxiety symptoms were assessed using a range of child‐ and parent‐reported questionnaire measures of child anxiety symptoms, including the Spence Children's Anxiety Scale (SCAS‐C/P) (or the parent‐reported Preschool Anxiety Scale for younger children), Multidimensional Anxiety Scale for Children (MASC‐C/P), the Screen for Children Anxiety Related Emotional Disorders (SCARED‐C/P), State Trait Anxiety Inventory‐Trait Scale (STAIC‐T), the child‐reported Revised Children’s Manifest Anxiety Scale (RCMAS), the child‐reported Revised Child Anxiety and Depression Scale‐Anxiety Scale (RCADS‐A), the parent‐reported Child Behavior Checklist‐Anxiety Scale (CBCL‐A), and the parent‐reported Child and Adolescent Symptom Inventory‐4 ASD Anxiety Scale. Where broad measures of anxiety symptoms were not reported, the following disorder‐specific symptom questionnaire measures were used in the main analyses: Social Anxiety Scale for Adolescents (SAS‐A) (Herbert 2009; Masia Warner 2005; Masia Warner 2007; Olivares 2014; Rosa Alcazar 2009), Social Phobia and Anxiety Inventory for Children (SPAI) (Herbert 2009; Masia Warner 2005; Masia Warner 2007; Masia Warner 2016; Melfsen 2011; Olivares 2005; Rosa Alcazar 2009; Sanchez Garcia 2009), IBD‐Specific Anxiety Scale (IBD‐SAS) (Reigada 2015), Intra Oral Injection Fear Scale (IOIF‐s) (Berge 2017), and Child Survey Fear Schedule: Dental Subscale (Shahnavaz 2016).
Depressive symptoms were most frequently assessed using self‐reported questionnaires, and where parent‐report was used, it was always used alongside self‐report, so only self‐report depressive symptom measures were used in the analyses. The most frequently used measure of depressive symptoms was the Children's Depression Inventory; other measures included the Short Mood and Feelings Questionnaire (Arendt 2016; Kidd 2018; Thirlwall 2013; Wergeland 2014), Mood and Feelings Questionnaire (Perrin 2019), Revised Child Anxiety and Depression Scale‐Depression scale (RCADS‐D) (Muris 2002), and Beck Depression Inventory‐II (BDII) (Masia Warner 2007).
The included studies that assessed post‐treatment global functioning all used the clinician‐rated Children’s Global Assessment Scale (CGAS) or adapted, White 2013, or translated versions of the CGAS (Melfsen 2011).
Excluded studies
We excluded 593 full‐text articles; the reasons for exclusion are detailed in Characteristics of excluded studies.
We excluded studies if participants were not fully randomised to conditions (Bodden 2008a; Cobham 2012; Hayward 2000; Kujawa 2019; Mendlowitz 1999; Nauta 2003), or if the study did not use a standardised structured interview to determine the presence of baseline anxiety disorders (e.g. Gil Bernal 2009; Jansen 2012; Kerns 2016; Sevi Tok 2016; Sung 2011). We excluded studies where only some participants were under 19 years of age (e.g. Salzer 2018), or only some participants met the diagnostic criteria for anxiety disorder (e.g. Bernstein 2005; Ginsburg 2019b; Pereira 2014; Weisz 2012), if the study authors did not provide data on eligible participants. We also excluded studies if the intervention did not include both cognitive and behavioural elements (e.g. Beidel 2000; Beidel 2007; Bergman 2013; Cotton 2019; Ebrahiminejad 2016; Oerbeck 2014; Ollendick 2018; Ost 2015; Ozyurt 2018; Rudy 2017; Storch 2019); there were no face‐to‐face CBT sessions (e.g. Lyneham 2006); or where the control intervention included elements of CBT (e.g. Clementi 2019).
We excluded five studies because useable data were not provided for any relevant outcomes (Asbrand; Asbrand 2019; Baer 2005; Flatt 2010; NCT00576719).
Ongoing studies
We identified five ongoing studies that meet our inclusion criteria (see Characteristics of ongoing studies).
Studies awaiting classification
We identified trial registrations for 13 studies where insufficient information was available to determine eligibility, and either the trial was ongoing/not started or the trial data were not available (see Characteristics of studies awaiting classification).
Risk of bias in included studies
A summary of the risk of bias in the included studies is provided in Figure 2 and Figure 3.
2.

Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
3.

Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
Allocation
Over half of the included studies (47 out of 88) clearly described an adequate process of sequence generation, and just under half (39 out of 88) clearly described an adequate process of allocation concealment. In remaining studies, insufficient or no information about the sequence generation process was provided.
We performed a sensitivity analysis for the primary outcome (remission of primary anxiety disorder post‐treatment) amongst CBT versus waitlist controls, using only those studies that clearly described sequence generation, and found similar findings to the main analysis (odds ratio (OR) 4.84, 95% confidence interval (CI) 3.03 to 7.73, Z = 6.61, P < 0.001) (Analysis 1.32).
1.32. Analysis.

Comparison 1: CBT versus waitlist/no treatment, Outcome 32: Sensitivity analysis: remission of primary anxiety diagnosis post‐treatment (ITT) (only studies where sequence generation is clear)
Blinding
The vast majority of studies (72 out of 88) either clearly detailed using blind assessors to administer post‐treatment diagnostic interviews, or only used a parent/child report questionnaire, therefore we judged the risk of bias from not blinding to be low.
We performed a sensitivity analysis examining remission of primary anxiety disorder diagnosis amongst CBT versus waitlist controls, where studies that did not specify using blind assessors were removed. The findings were similar to the main analysis (OR 5.54, 95% CI 3.76 to 8.18, Z = 8.63, P < 0.001) (Analysis 1.33).
1.33. Analysis.

Comparison 1: CBT versus waitlist/no treatment, Outcome 33: Sensitivity analysis: remission of primary anxiety diagnosis post‐treatment (ITT) (only studies where blind assessors used)
Blinding of participants and personnel was only possible in some CBT versus TAU, active control, or alternative treatment studies. These studies described measures to ensure comparability of interventions (e.g. amount of contact time); however, few studies specifically detailed attempts to conceal 'test' versus 'control' intervention from participants.
Incomplete outcome data
Most studies described information on dropouts and missing outcome data. The amount of missing data was small, with a description of appropriate methods to manage missing data provided. Sixteen studies provided insufficient information on missing data, and in three studies missing data were not balanced across groups, with more missing data in the CBT group than in the control group (Afshari 2014; Last 1998; Salum 2018).
Selective reporting
With the exception of two studies where post‐treatment anxiety symptoms outcomes were not reported for CBT and controls (O'Brien 2007; Waters 2009), the study reports included expected outcomes relevant to this review.
Notably, however, six studies included a post‐treatment diagnostic assessment and reported outcomes from this assessment (e.g. remission of a subset of anxiety disorders, reduction in the number of anxiety disorders), but did not report or provide data on remission of primary anxiety disorder or remission of all anxiety disorders (Ginsburg 2012; Hancock 2018; Murphy 2017; Pincus 2010; Walkup 2008; Wood 2009), so these studies were not included in our analyses of diagnostic outcomes.
Other potential sources of bias
Therapy integrity, including therapist competence and adherence, was assessed across all studies. In the majority of studies (61 out of 88), trained and supervised therapists were used, and adherence was measured and reported. In the remaining studies insufficient information was provided on competence or adherence, or both.
The most frequently identified other potential source of bias related to the timing of the post‐treatment assessment. In seven studies (Flannery Schroeder 2000; Fujii 2013; Ishikawa 2019; Kendall 1994; Kendall 1997; Masia Warner 2011; Pincus 2010), the timing of the post‐treatment assessment varied across groups, with a shorter waitlist or control period than treatment period.
Effects of interventions
See: Table 1; Table 2; Table 3; Table 4
Comparison 1: CBT versus waitlist/no treatment
See Table 1.
Primary outcomes
1.1 Remission of primary anxiety diagnosis post‐treatment
We included 39 studies in the analyses examining remission of primary anxiety disorder diagnosis post‐treatment (Arendt 2016; Cartwright Hatton 2011; Cobham 2017; Cornacchio 2019; Dadds 1997; Flannery Schroeder 2000; Gallagher 2004; Hirshfeld Becker 2010; Holmes 2014; Ishikawa 2019; Kendall 1994; Kendall 1997; Kidd 2018; Lau 2010; Masia Warner 2005; Masia Warner 2011; McConachie 2014; McNally Keehn 2013; Melfsen 2011; Olivares 2005; Olivares 2014; Olivares 2019; Ollendick 2009; Ost 2001; Perrin 2019; Rapee 2006; Rosa Alcazar 2009; Sanchez Garcia 2009; Santucci 2013; Schneider 2011; Silverman 1999b; Spence 2000; Spence 2006; Spence 2011; Thirlwall 2013; Villabo 2018; Waters 2009; Wergeland 2014; Wood 2015).
Moderate‐quality evidence from ITT analysis revealed a response rate for remission of primary anxiety diagnosis of 49.4% (802 out of 1623) for CBT versus 17.8% (191 out of 1074) for controls (OR 5.45, 95% CI 3.90 to 7.60, Z = 9.96, P < 0.001) (Analysis 1.1). Over half of the studies (59%; 23 out of 39) and comparisons (52%; 25 out of 48) showed a clear benefit for CBT (95% CI does not cross 1) (Figure 4), with evidence of moderate heterogeneity (Chi² = 97.73, df = 47, P < 0.001; I² = 52%).
1.1. Analysis.

Comparison 1: CBT versus waitlist/no treatment, Outcome 1: Remission of primary anxiety diagnosis post‐treatment (ITT)
4.

Forest plot of comparison: 1 CBT vs waitlist/no treatment, outcome: 1.1 Remission of primary anxiety diagnosis post‐treatment (ITT).
Subgroup analyses
We found a difference in outcomes for the different delivery formats (child‐focused, child and parent, parent only) (Chi² = 8.57, df = 2, P = 0.01), with substantial subgroup heterogeneity (I² = 76.7%) (Analysis 1.1). Inspection of the forest plot and the summary statistics suggest that studies evaluating child‐focused CBT produced greater remission of primary anxiety diagnosis in the CBT arms (OR 10.42, 95% CI 5.84 to 18.58) compared to waitlist/no treatment controls than studies evaluating CBT delivered to both children and parents (OR 4.08, 95% CI 2.72 to 6.11) or parents only (OR 2.83, 95% CI 1.12 to 7.16). Notably, however, there was also evidence of moderate heterogeneity amongst studies evaluating child‐focused CBT (Chi² = 43.41, df = 22, P = 0.004; I² = 49%).
We found no differences in remission of primary anxiety diagnosis outcomes for individual‐ versus group‐delivered CBT (Chi² = 0.90, df = 1, P = 0.34; I² = 0%); interventions with different amounts of therapist contact time (< 10 hours, ≥ 10 and < 20 hours, ≥ 20 hours) (Chi² = 0.52, df = 2, P = 0.77; I² = 0%); or studies with participants in different age groups (≤ 12 years, ≥ 12 years, < 12 years and ≥12 years) (Chi² = 1.59, df = 2, P = 0.45; I² = 0%) (Analysis 1.2; Analysis 1.3; Analysis 1.4).
1.2. Analysis.

Comparison 1: CBT versus waitlist/no treatment, Outcome 2: Subgroup analysis: remission of primary anxiety diagnosis post‐treatment (ITT) (individual vs group)
1.3. Analysis.

Comparison 1: CBT versus waitlist/no treatment, Outcome 3: Subgroup analysis: remission of primary anxiety diagnosis post‐treatment (ITT) (amount of therapist contact time)
1.4. Analysis.

Comparison 1: CBT versus waitlist/no treatment, Outcome 4: Subgroup analysis: remission of primary anxiety diagnosis post‐treatment (ITT) (age)
Subgroup analyses revealed no significant difference in outcomes between studies including participants with and without ASD (Chi² = 2.25, df = 1, P = 0.13; I² = 55.5%) (Analysis 1.5); however, only four studies included children/adolescents with ASD, compared to 35 studies with participants without ASD. The four studies of children/adolescents with ASD revealed no significant difference between CBT and waitlist/no treatment controls in rates of remission of primary anxiety disorder diagnosis (OR 1.79, 95% CI 0.39 to 8.16, Z = 0.76, P = 0.45, n = 136, I² = 59%).
1.5. Analysis.

Comparison 1: CBT versus waitlist/no treatment, Outcome 5: Subgroup analysis: remission of primary anxiety diagnosis post‐treatment (ITT) (ASD vs non‐ASD)
Completer analysis
The completer analysis included 1422 CBT participants and 984 controls, with a response rate for remission of primary anxiety diagnosis of 56.4% for CBT versus 11.7% for controls (OR 11.55, 95% CI 8.41 to 15.86, Z = 15.11, P < 0.001) (Analysis 1.6). Most of the studies (89%, 34 out of 38) and comparisons (81%; 38 out of 47) showed a clear benefit for CBT (95% CI does not cross 1). There was no heterogeneity across studies (Chi² = 61.53, df = 46, P = 0.06; I² = 25%).
1.6. Analysis.

Comparison 1: CBT versus waitlist/no treatment, Outcome 6: Remission of primary anxiety diagnosis post‐treatment (completers)
1.2 Acceptability: loss of participants to post‐treatment assessment
Low‐quality evidence showed no difference between CBT and waitlist/no treatment controls in the rate of those lost to post‐treatment assessment (Analysis 1.7), indicating a similar degree of acceptability. The rate of loss to post‐treatment assessment was 13.5% (260 out of 1919) in the CBT group versus 10.4% (129 out of 1239) in the control group (OR 1.09, 95% CI 0.85 to 1.41, Z = 0.69, P = 0.49, n = 3158, k = 45, I² = 4%).
1.7. Analysis.

Comparison 1: CBT versus waitlist/no treatment, Outcome 7: Acceptability (number of participants lost to post‐treatment assessment)
Secondary outcomes
1.3 Remission for all anxiety disorders post‐treatment
We included 28 studies in the analyses examining post‐treatment remission of all anxiety disorder diagnoses (Arendt 2016; Barrett 1996; Barrett 1998; Cartwright Hatton 2011; Chalfant 2007; Chiu 2013; Cobham 2017; Dadds 1997; Hirshfeld Becker 2010; Ishikawa 2019; Kennedy 2009; Lau 2017; McConachie 2014; Melfsen 2011; Olivares 2005; Perrin 2019; Rapee 2005; Rapee 2006; Rosa Alcazar 2009; Sanchez Garcia 2009; Shortt 2001; Simon 2011; Spence 2000; Spence 2006; Spence 2011; Thirlwall 2013; Villabo 2018; Waters 2009).
The ITT analysis included 1213 CBT participants and 862 controls, with a response rate for remission of all anxiety disorder diagnoses of 46.8% for CBT versus 19.1% for waitlist/no treatment controls (OR 4.43, 95% CI 2.89 to 6.78, Z = 6.85, P < 0.001) (Analysis 1.8). Sixty per cent of included studies (17 out of 28) and 51% of comparisons (18 out of 35) reported findings showing a clear benefit for CBT (95% CI does not cross 1). There was evidence of moderate heterogeneity (Chi² = 84.49, df = 34, P < 0.001; I² = 60%), and thus moderate‐quality evidence overall for the benefit of CBT compared to waitlist/no treatment controls for remission of all anxiety disorders.
1.8. Analysis.

Comparison 1: CBT versus waitlist/no treatment, Outcome 8: Remission of all anxiety diagnoses post‐treatment (ITT)
Subgroup analyses
We found a difference in outcomes for different delivery formats (child‐focused, child and parent, parent‐only) (Chi² = 8.14, df = 2, P = 0.02), with substantial subgroup heterogeneity (I² = 75.4%). There was evidence of substantial heterogeneity amongst studies evaluating child‐focused CBT (I² = 70%), but we found that overall these studies produced greater remission of all anxiety disorder diagnoses following CBT compared to waitlist/no treatment controls (OR 8.52, 95% CI 2.97 to 24.39), than studies evaluating child‐and‐parent delivered CBT (OR 5.19, 95% CI 3.26 to 8.27), or studies evaluating parent‐delivered CBT (OR 1.89, 95% CI crosses 1).
We found no differences in remission of all anxiety disorder diagnoses outcomes for individual‐ versus group‐delivered CBT (Chi² = 0.35, df = 1, P = 0.56; I² = 0%) (Analysis 1.9); however, there was variation in these outcomes amongst interventions with differing amounts of therapist contact time (Chi² = 10.75, df = 2, P = 0.005; I² = 81.4%) (Analysis 1.10). Only five studies evaluated interventions involving < 10 hours therapist contact time (Cobham 2017; Ishikawa 2019; Rapee 2005; Simon 2011; Thirlwall 2013), and did not indicate a benefit for CBT compared to waitlist/no treatment control groups for remission of all anxiety disorders (OR 1.42, 95% CI 0.68 to 2.96, Z = 0.93, P = 0.35), whilst interventions with 10 to 20 hours or ≥ 20 hours contact time both showed a clear benefit for CBT (OR 6.59, 95% CI 3.62 to 12.01 and OR 5.03, 95% CI 2.55 to 9.93, respectively).
1.9. Analysis.

Comparison 1: CBT versus waitlist/no treatment, Outcome 9: Subgroup analysis: remission of all anxiety diagnoses post‐treatment (ITT) (individual vs group)
1.10. Analysis.

Comparison 1: CBT versus waitlist/no treatment, Outcome 10: Subgroup analysis: remission of all anxiety diagnoses post‐treatment (ITT) (amount of therapist contact time)
Subgroup analyses did not show differences in remission of all anxiety disorder diagnoses outcomes amongst studies with participants in different age groups (Chi² = 0.80, df = 2, P = 0.67; I² = 0%) (Analysis 1.11), and as only two studies included participants with ASD, meaningful subgroup analyses comparing studies with and without participants with ASD was not possible.
1.11. Analysis.

Comparison 1: CBT versus waitlist/no treatment, Outcome 11: Subgroup analysis: remission of all anxiety diagnoses post‐treatment (ITT) (age)
Completer analysis
The completer analysis included 1074 CBT participants and 797 controls, with a response rate for remission of any anxiety disorder diagnosis of 52.9% for CBT versus 14.2% for controls (OR 9.13, 95% CI 5.78 to 14.41, Z = 9.49, P < 0.001) (Analysis 1.12). More than three‐quarters of included studies (21 out of 27) and 65% of comparisons (22 out of 34) reported findings showing a clear benefit for CBT (95% CI does not cross 1). There was evidence of moderate heterogeneity (Chi² = 68.75, df = 33, P < 0.001; I² = 52%).
1.12. Analysis.

Comparison 1: CBT versus waitlist/no treatment, Outcome 12: Remission of all anxiety diagnoses post‐treatment (completers)
1.4 Reduction in anxiety symptoms (child report) post‐treatment
We included 45 studies in the analyses examining post‐treatment child‐reported anxiety symptoms (Afshari 2014; Arendt 2016; Barrett 1996; Berge 2017; Chalfant 2007; Cheung 2016; Chiu 2013; Cobham 2017; Dadds 1997; Flannery Schroeder 2000; Gallagher 2004; Hancock 2018; Holmes 2014; Ishikawa 2019; Kendall 1994; Kendall 1997; Kidd 2018; Lau 2010; Leutgeb 2012; Masia Warner 2005; McConachie 2014; McNally Keehn 2013; Melfsen 2011; Olivares 2005; Olivares 2014; Ollendick 2009; Ost 2001; Perrin 2019; Rapee 2006; Rosa Alcazar 2009; Salari 2018; Sanchez Garcia 2009; Santucci 2013; Schneider 2011; Shortt 2001; Silverman 1999b; Simon 2011; Smith 2014; Spence 2000; Spence 2006; Spence 2011; Thirlwall 2013; Villabo 2018; Wergeland 2014; Wood 2009). The standardised mean difference (SMD) between CBT groups and waitlist/no treatment controls was −0.67 (95% CI −0.88 to −0.47, Z = 6.36, P < 0.001, n = 2831) (Analysis 1.13; Figure 5). Substantial heterogeneity (Chi² = 352.54, df = 56, P < 0.001; I² = 84%) reduced our confidence in this result, and we rated this evidence as low‐quality.
1.13. Analysis.

Comparison 1: CBT versus waitlist/no treatment, Outcome 13: Reduction in anxiety symptoms (child report) post‐treatment
5.

Forest plot of comparison: 1 CBT vs waitlist/no treatment, outcome: 1.13 Reduction in anxiety symptoms (child report) post‐treatment.
Indeed, including only studies that used a broad measure of child‐reported anxiety symptoms (38 studies, 2459 participants), the SMD between CBT groups and waitlist controls was reduced to −0.41 (95% CI −0.57 to −0.25, Z = 5.13, P < 0.001, I² = 68%) (Analysis 1.14).
1.14. Analysis.

Comparison 1: CBT versus waitlist/no treatment, Outcome 14: Sensitivity analysis: reduction in anxiety symptoms (child report) post‐treatment (broad anxiety measures)
Subgroup analyses
We found a significant difference between child‐focused, child‐and‐parent, and parent‐only CBT (Chi² = 14.67, df = 2, P < 0.001) on child‐reported anxiety symptom outcomes, with considerable subgroup heterogeneity (I² = 86.4%). There was no significant difference between CBT and waitlist/no treatment control groups in post‐treatment child‐reported anxiety symptoms for parent‐delivered CBT (SMD 0.04, 95% CI −0.38 to 0.46, Z = 0.19, P = 0.85, 5 studies). The forest plot and summary statistics indicated that child‐focused CBT produced a greater reduction on child‐reported anxiety symptoms amongst CBT groups compared to waitlist/no treatment controls (SMD −1.04, 95% CI −1.41 to −0.67, Z = 5.48, P < 0.001, 24 studies) than child‐and‐parent delivered CBT (SMD −0.45, 95% CI −0.67 to −0.23, Z = 3.99, P < 0.001, 20 studies), but with substantial heterogeneity within each of these subgroups (child‐focused: I² = 88%; child‐and‐parent: I² = 69%).
Subgroup analyses also revealed a significance difference between individual‐ and group‐focused CBT (Chi² = 6.47, df = 1, P = 0.01; I² = 84.5%) (Analysis 1.15). The SMD in post‐treatment child‐reported anxiety symptoms between CBT and waitlist/no treatment control groups was −0.91 (95% CI −1.22 to −0.60) in studies evaluating group‐focused CBT compared to −0.39 (95% CI −0.64 to −0.15) in studies evaluating individual‐focused CBT.
1.15. Analysis.

Comparison 1: CBT versus waitlist/no treatment, Outcome 15: Subgroup analysis: reduction in anxiety symptoms (child report) post‐treatment (individual vs group)
We found no differences between interventions with different amounts of therapist contact time (< 10 hours, ≥ 10 and < 20 hours, ≥ 20 hours) (Chi² = 3.33, df = 2, P = 0.19; I² = 39.9%) (Analysis 1.16), but child‐reported anxiety symptoms outcomes did vary amongst different age groups (Chi² = 8.27, df = 2, P = 0.02), with substantial subgroup heterogeneity (I² = 75.8%) (Analysis 1.17). Amongst studies of children aged ≥ 12 years, the SMD between CBT and waitlist/no treatment controls was −1.78 (95% CI −3.01 to −0.56) compared to −0.62 (95% CI −0.83 to −0.41) where studies included participants over and under 12 years of age, and −0.23 (95% CI cross 0) amongst studies of children ≤ 12 years, but with variation within each of these age groups (I² = 71% to 95%).
1.16. Analysis.

Comparison 1: CBT versus waitlist/no treatment, Outcome 16: Subgroup analysis: reduction in anxiety symptoms (child report) post‐treatment (amount of therapist contact time)
1.17. Analysis.

Comparison 1: CBT versus waitlist/no treatment, Outcome 17: Subgroup analysis: reduction in anxiety symptoms (child report) post‐treatment (age)
We did not find differences between studies including participants with and without ASD on post‐treatment child‐reported anxiety symptoms outcomes (Chi² = 0.02, df = 1, P = 0.88; I² = 0%) (Analysis 1.18).
1.18. Analysis.

Comparison 1: CBT versus waitlist/no treatment, Outcome 18: Subgroup analysis: reduction in anxiety symptoms (child report) post‐treatment (ASD vs non‐ASD)
1.5 Reduction in anxiety symptoms (parent report) post‐treatment
We included 35 studies in analyses examining post‐treatment parent‐reported anxiety symptoms (Afshari 2014; Arendt 2016; Chalfant 2007; Cheung 2016; Chiu 2013; Cobham 2017; Flannery Schroeder 2000; Holmes 2014; Ishikawa 2019; Kendall 1994; Kendall 1997; Kennedy 2009; Kidd 2018; Lau 2010; Lau 2017; Masia Warner 2005; McConachie 2014; McNally Keehn 2013; Olivares 2014; Perrin 2019; Rapee 2005; Rapee 2006; Rosa Alcazar 2009; Santucci 2013; Schneider 2011; Silverman 1999b; Smith 2014; Spence 2006; Spence 2011; Thirlwall 2013; Villabo 2018; Wergeland 2014; White 2013; Wood 2009; Wood 2015). The SMD between CBT and waitlist/no treatment control groups was −0.70 (95% CI −0.90 to −0.51, Z = 7.01, P < 0.001, n = 2137, low‐quality evidence), with substantial heterogeneity (Chi² = 171.97, df = 40, P < 0.001; I² = 77%) (Analysis 1.19; Figure 6.
1.19. Analysis.

Comparison 1: CBT versus waitlist/no treatment, Outcome 19: Reduction in anxiety symptoms (parent report) post‐treatment
6.

Forest plot of comparison: 1 CBT vs waitlist/no treatment, outcome: 1.19 Reduction in anxiety symptoms (parent report) post‐treatment.
Including only studies that used a broad measure of parent‐reported anxiety symptoms (32 studies, 1952 participants), the SMD between CBT and waitlist groups was reduced to −0.59 (95% CI −0.77 to −0.41, Z = 6.33, P < 0.001, I² = 71%) (Analysis 1.20).
1.20. Analysis.

Comparison 1: CBT versus waitlist/no treatment, Outcome 20: Sensitivity analysis: reduction in anxiety symptoms (parent report) post‐treatment (broad anxiety measures only)
Subgroup analyses
Subgroup analyses revealed no significant differences between child‐focused, child and parent, and parent‐only on parent‐reported anxiety symptom outcomes (Chi² = 3.43, df = 2, P = 0.18) (Analysis 1.19). However, there was evidence of a difference amongst individual compared to group interventions (Chi² = 6.79, df = 1, P = 0.009), with substantial subgroup heterogeneity (I² = 85.3%) (Analysis 1.21). The SMD between CBT and waitlist/no treatment post‐treatment parent‐reported anxiety symptoms was −0.92 (95% CI −1.21 to −0.62) amongst group interventions, compared to −0.43 (95% CI −0.65 to −0.21) for individual interventions.
1.21. Analysis.

Comparison 1: CBT versus waitlist/no treatment, Outcome 21: Subgroup analysis: reduction in anxiety symptoms (parent report) post‐treatment (individual vs group)
We did not find differences in parent‐reported anxiety symptom outcomes across interventions involving varying amount of therapist contact time (Chi² = 3.77, df = 2, P = 0.15; Analysis 1.22). On the other hand, there was evidence of a difference in these outcomes amongst different age groups (Chi² = 5.87, df = 2, P = 0.05), with substantial subgroup heterogeneity (I² = 65.9%) (Analysis 1.23). Amongst studies that included participants aged ≥ 12 years, the SMD between CBT and waitlist/no treatment groups was −1.07 (95% CI −1.78 to −0.37), compared to −0.76 (95% CI −1.04 to −0.49) in studies that included participants under and over 12 years of age, and −0.40 (95% CI −0.63 to −0.17) where participants were ≤ 12 years.
1.22. Analysis.

Comparison 1: CBT versus waitlist/no treatment, Outcome 22: Subgroup analysis: reduction in anxiety symptoms (parent report) post‐treatment (amount of therapist contact time)
1.23. Analysis.

Comparison 1: CBT versus waitlist/no treatment, Outcome 23: Subgroup analysis: reduction in anxiety symptoms (parent report) post‐treatment (age)
We found no significant differences in parent‐reported anxiety symptom outcomes amongst samples with and without ASD (Chi² = 1.42, df = 1, P = 0.23; Analysis 1.24).
1.24. Analysis.

Comparison 1: CBT versus waitlist/no treatment, Outcome 24: Subgroup analysis: reduction in anxiety symptoms (parent report) post‐treatment (ASD vs non‐ASD)
1.6 Reduction in depressive symptoms post‐treatment
Seventeen studies reported post‐treatment depressive symptoms (Arendt 2016; Barrett 1996; Flannery Schroeder 2000; Gallagher 2004; Ishikawa 2019; Kendall 1994; Kendall 1997; Kidd 2018; Masia Warner 2005; Melfsen 2011; Ollendick 2009; Ost 2001; Perrin 2019; Salari 2018; Silverman 1999b; Thirlwall 2013; Wergeland 2014). The SMD between CBT and waitlist/no treatment control groups was −0.34 (95% CI −0.51 to −0.17, Z = 3.96, P < 0.001, n = 1157, moderate‐quality evidence), with moderate heterogeneity (Chi² = 39.62, df = 22, P = 0.01; I² = 44%) (Analysis 1.25).
1.25. Analysis.

Comparison 1: CBT versus waitlist/no treatment, Outcome 25: Reduction in depressive symptoms post‐treatment
1.7 Improvement in global functioning post‐treatment
Data pooled from 11 studies that reported post‐treatment global functioning produced an SMD between CBT and waitlist/no treatment control groups of 1.03 (95% CI 0.68 to 1.38, Z = 5.83, P < 0.001, n = 557, low‐quality evidence), with substantial heterogeneity (Chi² = 37.41, df = 11, P < 0.001; I² = 71%) (Analysis 1.26) (Cornacchio 2019; Holmes 2014; Masia Warner 2005; Masia Warner 2011; Melfsen 2011; Perrin 2019; Salari 2018; Santucci 2013; Spence 2011; Villabo 2018; White 2013).
1.26. Analysis.

Comparison 1: CBT versus waitlist/no treatment, Outcome 26: Improvement in global functioning post‐treatment
1.8 Adverse events
No included study reported adverse events in both CBT and waitlist/no treatment groups, so meta‐analysis was not possible.
Remission of primary anxiety disorder diagnosis at follow‐up
Four studies reported remission of primary anxiety disorder at follow‐up assessments ≤ 6 months post‐treatment (Dadds 1997; Gallagher 2004; Olivares 2005; Rosa Alcazar 2009), with ITT analysis showing a rate for remission of primary anxiety diagnosis of 66.7% (48 out of 72) for CBT groups versus 34.6% (28 out of 81) for waitlist/no treatment controls (OR 10.94, 95% CI 2.33 to 51.41, Z = 3.03, P = 0.002, I² = 40%) (Analysis 1.27). Only 3 studies (166 participants) reported remission of primary anxiety disorder 12 months post‐treatment (Cartwright Hatton 2011; Dadds 1997; Rosa Alcazar 2009); pooled data did not suggest a benefit for CBT compared to waitlist/no treatment control groups (OR 2.80, 95% 0.24 to 33.19, Z = 0.82, P = 0.41, I² = 83%).
1.27. Analysis.

Comparison 1: CBT versus waitlist/no treatment, Outcome 27: Remission of primary anxiety diagnosis at follow‐up (ITT)
Only one study reported remission of primary anxiety disorder > 12 months post‐treatment, so meta‐analysis was not possible.
Completer analyses produced similar findings, with evidence of an intervention effect at follow‐up assessments ≤ 6 months post‐treatment but not at 12‐month follow‐up (Analysis 1.28)
1.28. Analysis.

Comparison 1: CBT versus waitlist/no treatment, Outcome 28: Remission of primary anxiety diagnosis at follow‐up (completers)
Remission of all anxiety disorder diagnoses at follow‐up
Five studies reported data on remission of all anxiety disorders at follow‐up assessments (Cartwright Hatton 2011; Dadds 1997; Olivares 2005; Rosa Alcazar 2009; Simon 2011), including ≤ 6 months post‐treatment (Dadds 1997; Olivares 2005; Rosa Alcazar 2009), 12 months post‐treatment (Cartwright Hatton 2011; Dadds 1997; Rosa Alcazar 2009), and 24 months post‐treatment (Dadds 1997; Simon 2011). Neither ITT analyses (Analysis 1.29) nor completer analyses (Analysis 1.30) showed a significant difference between CBT and waitlist/no treatment at any of these follow‐up time points.
1.29. Analysis.

Comparison 1: CBT versus waitlist/no treatment, Outcome 29: Remission of all anxiety diagnoses at follow‐up (ITT)
1.30. Analysis.

Comparison 1: CBT versus waitlist/no treatment, Outcome 30: Remission of all anxiety diagnoses at follow‐up (completers)
Reduction in anxiety symptoms at follow‐up
Six studies reported data on child‐reported anxiety symptoms at follow‐up assessments (Analysis 1.31) (Afshari 2014; Dadds 1997; Gallagher 2004; Olivares 2005; Rosa Alcazar 2009; Simon 2011). Child‐reported anxiety symptoms at ≤ 6 months post‐treatment produced an SMD of −1.92 (95% CI −2.95 to −0.89, Z = 3.65, P < 0.001, n = 179) between CBT and waitlist/no treatment groups (Afshari 2014; Dadds 1997; Gallagher 2004; Olivares 2005; Rosa Alcazar 2009), with substantial heterogeneity across studies (Chi² = 35.35, df = 5, P < 0.001; I² = 86%). Only two studies reported corresponding outcomes at 12‐month follow‐up (Dadds 1997; Rosa Alcazar 2009), and only one study at 24‐month follow‐up (Simon 2011), so meta‐analyses were not possible for these time points.
1.31. Analysis.

Comparison 1: CBT versus waitlist/no treatment, Outcome 31: Reduction in anxiety symptoms (child report) at follow‐up
As only two studies reported data on parent‐reported anxiety symptoms at 6 months post‐treatment (Afshari 2014; Rosa Alcazar 2009), and one with corresponding data at 12 months post‐treatment (Rosa Alcazar 2009), meta‐analyses were not performed using these data.
Comparison 2: CBT versus treatment as usual
See Table 2.
Primary outcomes
2.1 Remission of primary anxiety diagnosis post‐treatment
Eight studies provided uncertain evidence on post‐treatment remission of primary anxiety disorder diagnosis for CBT versus TAU (Fujii 2013; Ginsburg 2019a; Reaven 2012; Shahnavaz 2016; Sharma 2017; Southam Gerow 2010; Storch 2013; Storch 2015).
The ITT analysis included 281 CBT participants and 206 TAU participants, with no evidence of a significant difference in the rate of remission of primary anxiety diagnosis post‐treatment (44.1% and 40.8% respectively; OR 3.19, 95% CI 0.90 to 11.29, Z = 1.80, P = 0.07, low‐quality evidence) (Analysis 2.1). There was evidence of substantial heterogeneity (Chi² = 28.93, df = 7, P < 0.001; I² = 76%).
2.1. Analysis.

Comparison 2: CBT versus treatment as usual, Outcome 1: Remission of primary anxiety diagnosis post‐treatment (ITT)
Subgroup analyses
There was a significant difference in remission of primary anxiety disorder outcomes amongst studies evaluating child‐focused CBT compared to child‐and‐parent delivered CBT (Chi² = 10.90, df = 1, P < 0.001; I² = 90.8%). Data pooled from five studies (172 participants) that evaluated a child‐and‐parent delivered intervention showed a clear benefit for CBT compared to TAU (OR 8.56, 95% CI 3.10 to 23.66, Z = 4.14, P < 0.001), whereas data from three studies (315 participants) evaluating child‐focused interventions did not (OR 0.61, 95% CI cross 1). None of the studies that compared CBT to TAU evaluated a parent‐only intervention.
Planned subgroup analyses comparing individual versus group interventions, interventions with varying amount of therapist contact time, and different age groups were not possible due to an insufficient number of studies. Only two studies evaluated group CBT; only one study used an intervention with < 10 hours therapist contact time; and five (out of eight) studies included pre‐adolescent and adolescent participants.
Subgroup analyses also indicated a difference in remission outcomes in studies with participants with ASD compared to studies with participants without ASD (Chi² = 5.71, df = 1, P = 0.02; I² = 82.5%) (Analysis 2.2). Pooled data from four ASD samples showed a higher rate of remission of primary anxiety disorder amongst CBT groups compared to TAU groups (OR 11.25, 95% CI 3.11 to 40.79, Z = 3.68, P < 0.001, n = 142, I² = 0%), but corresponding data from four samples without ASD showed no significant difference between CBT and TAU groups (OR 1.14, 95% CI 0.29 to 4.47, Z = 0.18, P = 0.85, n = 345, I² = 75%).
2.2. Analysis.

Comparison 2: CBT versus treatment as usual, Outcome 2: Subgroup analysis: remission of primary anxiety diagnosis post‐treatment (ITT) (ASD vs non‐ASD)
Completer analysis
The completer analysis included 248 CBT participants and 192 TAU participants, with a response rate for remission of primary anxiety diagnosis of 50.4% for CBT versus 36.5% for controls (OR 4.87, 95% CI 1.51 to 15.72, Z = 2.65, P = 0.008) (Analysis 2.3). Similar to the ITT analysis, there was substantial heterogeneity across the eight studies (Chi² = 21.30, df = 7, P = 0.003; I² = 67%).
2.3. Analysis.

Comparison 2: CBT versus treatment as usual, Outcome 3: Remission of primary anxiety diagnosis post‐treatment (completers)
2.2 Acceptability: loss of participants to post‐treatment assessment
We found no evidence of a difference between CBT and TAU in rate of those lost to post‐treatment assessment, illustrating a comparable degree of acceptability (OR 1.37, 95% CI 0.73 to 2.56, Z = 0.98, P = 0.33, I² = 0%, k = 8, n = 441, low‐quality evidence) (Analysis 2.4).
2.4. Analysis.

Comparison 2: CBT versus treatment as usual, Outcome 4: Acceptability (number of participants lost to post‐treatment assessment)
Secondary outcomes
2.3 Remission of all anxiety disorders post‐treatment
Five studies provided uncertain evidence on remission of all anxiety disorder diagnoses post‐treatment for CBT versus TAU (Barrington 2005; Sciberras 2018; Sharma 2017; Storch 2013; Storch 2015).
The ITT analyses showed a rate of remission of all anxiety diagnoses of 55.8% for CBT versus 41.4% for TAU (OR 2.74, 95% CI 1.16 to 6.46, Z = 2.30, P = 0.02, k = 5, n = 203, low‐quality evidence) (Analysis 2.5). There was no evidence of significant heterogeneity (Chi² = 3.92, df = 4, P = 0.42; I² = 0%).
2.5. Analysis.

Comparison 2: CBT versus treatment as usual, Outcome 5: Remission of all anxiety diagnoses post‐treatment (ITT)
Completer analyses showed a similar benefit for CBT versus TAU (OR 2.78, 95% CI 1.18 to 6.55, Z = 2.33, P = 0.02, k = 5, n = 201, I² = 0%) (Analysis 2.6).
2.6. Analysis.

Comparison 2: CBT versus treatment as usual, Outcome 6: Remission of all anxiety diagnoses post‐treatment (completers)
2.4 Reduction in anxiety symptoms (child‐report) post‐treatment
We included six studies in the analyses examining post‐treatment child‐reported anxiety symptoms (Barrington 2005; Ginsburg 2012; Sciberras 2018; Shahnavaz 2016; Sharma 2017; Southam Gerow 2010). We found no difference between CBT and TAU in child‐reported anxiety symptoms post‐treatment (SMD −0.15, 95% CI −0.78 to 0.48, Z = 0.46, P = 0.64, n = 214, low‐quality evidence), although there was substantial heterogeneity (Chi² = 23.55, df = 5, P < 0.001; I² = 79%) (Analysis 2.7). This finding was replicated after removal of the one study that used a disorder‐specific symptoms measure (SMD 0.07, 95% CI −0.54 to 0.68, Z = 0.22, P = 0.83, n = 187, I² = 74%) (Analysis 2.8).
2.7. Analysis.

Comparison 2: CBT versus treatment as usual, Outcome 7: Reduction in anxiety symptoms (child report) post‐treatment
2.8. Analysis.

Comparison 2: CBT versus treatment as usual, Outcome 8: Sensitivity analysis: reduction in anxiety symptoms (child report) post‐treatment (broad anxiety measures only)
2.5 Reduction in anxiety symptoms (parent‐report) post‐treatment
Pooled data from seven studies showed no difference between CBT and TAU in post‐treatment parent‐reported anxiety symptoms (SMD −0.32, 95% CI −0.70 to 0.06, Z = 1.64, P = 0.10, n = 228, low‐quality evidence) (Barrington 2005; Ginsburg 2002; Sciberras 2018; Shahnavaz 2016; Southam Gerow 2010; Storch 2013; Storch 2015), with moderate heterogeneity across studies (Chi² = 11.66, df = 6, P = 0.07; I² = 49%) (Analysis 2.9). Removal of one study that used a disorder‐specific measure did not change this finding (SMD −0.16, 95% CI −0.44 to 0.11, Z = 1.16, P = 0.25, n = 202, I² = 0%) (Analysis 2.10).
2.9. Analysis.

Comparison 2: CBT versus treatment as usual, Outcome 9: Reduction in anxiety symptoms (parent report) post‐treatment
2.10. Analysis.

Comparison 2: CBT versus treatment as usual, Outcome 10: Sensitivity analysis: reduction in anxiety symptoms (parent report) post‐treatment (broad anxiety measures only)
2.6 Reduction in depressive symptoms post‐treatment
Only one study reported depressive symptoms post‐treatment for CBT versus TAU (O'Brien 2007), so meta‐analysis was not possible.
2.7 Improvement in global functioning post‐treatment
Only one study reported post‐treatment global functioning for CBT versus TAU (Sharma 2017), so meta‐analysis was not possible.
2.8 Adverse events
No included study reported adverse events in both CBT and TAU groups, so meta‐analysis was not possible.
2.9 Follow‐up outcomes
There was an insufficient number of studies to conduct meta‐analyses examining longer‐term diagnostic or symptom outcomes. Only two studies reported remission from primary anxiety disorders at 12 months post‐treatment (Ginsburg 2019a; Shahnavaz 2016), and one study reported remission from all anxiety disorders at 6 and 12 months (Barrington 2005). Similarly, only three studies reported child‐reported and parent‐reported anxiety symptoms at 6‐month and/or 12‐month follow‐up (Barrington 2005; Ginsburg 2012; Shahnavaz 2016).
Comparison 3: CBT versus attention control
See Table 3.
Primary outcomes
3.1 Remission of primary anxiety diagnosis post‐treatment
Ten studies evaluating CBT versus attention control provided data on post‐treatment remission of primary anxiety disorder diagnosis (Ginsburg 2002; Hudson 2009; Kendall 2008; Khanna 2010; Last 1998; Masia Warner 2007; Masia Warner 2016; Ollendick 2009; Rosa Alcazar 2009; Silverman 1999a).
The ITT analysis (484 CBT participants; 338 control participants) provided uncertain evidence for a greater rate of remission of primary anxiety diagnosis post‐treatment for CBT compared to attention controls (48.3% versus 29.3%; OR 2.28, 95% CI 1.33 to 3.89, Z = 3.00, P = 0.003, low‐quality evidence), with moderate heterogeneity across studies (Chi² = 28.77, df = 12, P = 0.004; I² = 58%) (Analysis 3.1).
3.1. Analysis.

Comparison 3: CBT versus attention control, Outcome 1: Remission of primary anxiety diagnosis post‐treatment (ITT)
Subgroup analyses
None of the studies that evaluated CBT versus attention controls used a parent‐only intervention, but there was a difference in the pattern of results for remission of primary anxiety disorder outcomes amongst studies evaluating child‐focused CBT and child‐and‐parent delivered CBT when each was compared to attention controls (Chi² = 7.65, df = 1, P = 0.006; I² = 86.9%) (Analysis 3.1). Summary statistics indicated a benefit for CBT compared to attention controls amongst child‐focused interventions (OR 3.58, 95% CI 1.92 to 6.65, k = 7, n = 509), but not amongst child‐and‐parent delivered interventions (OR 1.12, 95% CI cross 1, k = 4, n = 313).
Subgroup analyses revealed no significant difference in remission of primary anxiety disorder outcomes in studies evaluating individual CBT versus group CBT (Chi² = 1.22, df = 1, P = 0.27; I² = 17.7%) (Chi² = 0.48, df = 1, P = 0.49; I² = 0%) (Analysis 3.2).
3.2. Analysis.

Comparison 3: CBT versus attention control, Outcome 2: Subgroup analysis: remission of primary anxiety diagnosis post‐treatment (ITT) (individual vs group)
Further subgroup analyses were not possible because there were fewer than three studies in at least one group for each planned subgroup analysis.
Completer analysis
In the completer analysis, 53.1% of CBT participants compared to 23.2% of attention control participants were free of their primary anxiety disorder diagnosis post‐treatment, with a significant intervention effect (OR 3.88, 95% CI 2.52 to 5.97, Z = 6.17, P < 0.001, k = 10, n = 752, I² = 21%) (Analysis 3.3).
3.3. Analysis.

Comparison 3: CBT versus attention control, Outcome 3: Remission of primary anxiety diagnosis post‐treatment (completers)
3.2 Acceptability: loss of participants to post‐treatment assessment
Low‐quality evidence indicated no difference between CBT and attention controls in rate of those lost to post‐treatment assessment, suggesting a similar degree of acceptability (OR 1.00, 95% CI cross 1, Z = 0.01, P = 0.99, n = 797, k = 12, I² = 0%) (Analysis 3.4).
3.4. Analysis.

Comparison 3: CBT versus attention control, Outcome 4: Acceptability (number of participants lost to post‐treatment assessment)
Secondary outcomes
3.3 Remission of all anxiety disorders post‐treatment
We included five studies in analyses comparing CBT versus attention controls for remission of all anxiety disorder diagnoses post‐treatment (Ginsburg 2002; Hudson 2009; Kendall 2008; Masia Warner 2007; Rosa Alcazar 2009).
Both ITT analyses and completer analyses indicated a benefit for CBT compared to attention control conditions (ITT: OR 2.75, 95% CI 1.22 to 6.17, Z = 2.45, P = 0.01, n = 378, I² = 49%, low‐quality evidence; completers: OR 3.88, 95% CI 1.58 to 9.51, Z = 2.96, P = 0.003, n = 359, I² = 48%) (Analysis 3.5; Analysis 3.6).
3.5. Analysis.

Comparison 3: CBT versus attention control, Outcome 5: Remission of all anxiety diagnoses post‐treatment (ITT)
3.6. Analysis.

Comparison 3: CBT versus attention control, Outcome 6: Remission of all anxiety diagnoses post‐treatment (completers)
3.4 Reduction in anxiety symptoms (child‐report) post‐treatment
Fifteen studies provided moderate‐quality evidence for post‐treatment child‐reported anxiety symptoms for CBT and attention control groups (Ginsburg 2002; Herbert 2009; Hudson 2009; Ingul 2013; Kendall 2008; Khanna 2010; Last 1998; Masia Warner 2007; Masia Warner 2016; Muris 2002; Ollendick 2009; Pincus 2010; Rosa Alcazar 2009; Salum 2018; Silverman 1999a). The SMD between CBT and attention controls for child‐reported anxiety symptoms was −0.31 (95% CI −0.51 to −0.11, Z = 3.09, P = 0.002, n = 978) (Analysis 3.7). There was evidence of moderate heterogeneity across studies (Chi² = 40.95, df = 20, P = 0.004; I² = 51%).
3.7. Analysis.

Comparison 3: CBT versus attention control, Outcome 7: Reduction in anxiety symptoms (child report) post‐treatment
After removal of studies that used a disorder‐specific symptom measure, the SMD between CBT and attention controls was reduced to −0.18 (95% CI −0.34 to −0.02, Z = 2.26, P = 0.02, n = 685, k = 11, I² = 0%) (Analysis 3.8).
3.8. Analysis.

Comparison 3: CBT versus attention control, Outcome 8: Sensitivity analysis: reduction in anxiety symptoms (child report) post‐treatment (broad anxiety measures only)
3.5 Reduction in anxiety symptoms (parent‐report) post‐treatment
Eight studies provided data on post‐treatment parent‐reported anxiety symptoms for CBT and attention control groups (Herbert 2009; Hudson 2009; Kendall 2008; Masia Warner 2007; Masia Warner 2016; Rosa Alcazar 2009; Salum 2018; Silverman 1999a). The analyses indicated no significant differences between CBT and attention controls (SMD −0.25, 95% CI −0.61 to 0.11, Z = 1.37, P = 0.17, n = 638, low‐quality evidence), but with substantial heterogeneity across studies (Chi² = 47.61, df = 11, P < 0.001; I² = 77%) (Analysis 3.9). Removal of studies that used disorder‐specific measures did not change this finding (SMD −0.04, 95% CI −0.26 to 0.18, Z = 0.36, P = 0.72, n = 345, k = 4, I² = 0%) (Analysis 3.10).
3.9. Analysis.

Comparison 3: CBT versus attention control, Outcome 9: Reduction in anxiety symptoms (parent report) post‐treatment
3.10. Analysis.

Comparison 3: CBT versus attention control, Outcome 10: Sensitivity analysis: reduction in anxiety symptoms (parent report) post‐treatment (broad anxiety measures only)
3.6 Reduction in depressive symptoms post‐treatment
Ten studies reported post‐treatment depressive symptoms for CBT versus attention controls (Ingul 2013; Kendall 2008; Khanna 2010; Last 1998; Masia Warner 2007; Muris 2002; Ollendick 2009; Pincus 2010; Salum 2018; Silverman 1999a), finding no between‐group difference (SMD −0.18, 95% CI −0.45 to 0.09, Z = 1.32, P = 0.19, n = 613, low‐quality evidence) (Analysis 3.11). There was evidence of moderate heterogeneity across studies (Chi² = 29.19, df = 12, P = 0.004; I² = 59%).
3.11. Analysis.

Comparison 3: CBT versus attention control, Outcome 11: Reduction in depressive symptoms post‐treatment
3.7 Improvement in global functioning post‐treatment
Only two studies reported post‐treatment global functioning for CBT versus attention controls (Khanna 2010; Masia Warner 2007), so meta‐analysis was not possible.
3.8 Adverse events
No study reported adverse events in both CBT and attention control groups, so meta‐analysis was not possible.
Remission of primary anxiety disorder diagnoses at follow‐up
Four studies provided data on remission of primary anxiety disorder at ≤ 6 months follow‐up (Hudson 2009; Masia Warner 2007; Masia Warner 2016; Rosa Alcazar 2009). ITT analyses showed a greater rate of remission for CBT groups compared to attention controls (OR 3.06, 95% CI 1.22 to 7.65, Z = 2.39, P = 0.02, n = 341), but with substantial heterogeneity across studies (Chi² = 12.62, df = 5, P = 0.02; I² = 60%) (Analysis 3.12).
3.12. Analysis.

Comparison 3: CBT versus attention control, Outcome 12: Remission of primary anxiety diagnosis at follow‐up (ITT)
The intervention effect increased in the completer analysis (OR 6.52, 95% CI 2.58 to 16.43, Z = 3.97, P < 0.001, k = 4, n = 302, I² = 44%) (Analysis 3.13).
3.13. Analysis.

Comparison 3: CBT versus attention control, Outcome 13: Remission of primary anxiety diagnosis at follow‐up (completers)
Only one study reported remission of primary anxiety disorder at 12‐month follow‐up, so meta‐analysis was not possible for this time point.
Remission of all anxiety disorder diagnoses at follow‐up
Three studies reported remission from all anxiety disorder diagnoses at ≤ 6 months post‐treatment (Hudson 2009; Masia Warner 2007; Rosa Alcazar 2009). ITT analyses and completer analyses indicated a greater rate of remission of all anxiety disorders for CBT groups compared to attention controls (ITT: OR 5.44, 95% CI 1.00 to 29.60, Z = 1.96, P = 0.05, n = 205; completer analysis: OR 11.19, 95% CI 1.94 to 64.51, Z = 2.70, P = 0.007, n = 182), but with substantial heterogeneity across studies (ITT: I² = 72%, completer analysis: I² = 62%) (Analysis 3.14; Analysis 3.15).
3.14. Analysis.

Comparison 3: CBT versus attention control, Outcome 14: Remission of all anxiety diagnoses at follow‐up (ITT)
3.15. Analysis.

Comparison 3: CBT versus attention control, Outcome 15: Remission of all anxiety diagnoses at follow‐up (completers)
Only one study reported remission of all anxiety disorder diagnoses at 12 months (Rosa Alcazar 2009), so meta‐analysis was not possible for this time point.
Reduction in anxiety symptoms at follow‐up
Six studies reported child‐reported anxiety symptoms at ≤ 6 months post‐treatment (Herbert 2009; Hudson 2009; Masia Warner 2007; Masia Warner 2016; Rosa Alcazar 2009; Silverman 1999a). Pooled data from these studies indicated a benefit for CBT compared to attention controls (SMD −0.44, 95% CI −0.79 to −0.08, Z = 2.40, P = 0.02, n = 434), but there was substantial heterogeneity across studies (Chi² = 23.08, df = 8, P = 0.003; I² = 65%) (Analysis 3.16).
3.16. Analysis.

Comparison 3: CBT versus attention control, Outcome 16: Reduction in anxiety symptoms (child report) at follow‐up
The same six studies provided parent‐reported anxiety symptoms at ≤ 6 months post‐treatment; analyses showed no significant difference between CBT and attention controls (SMD −0.63, 95% CI cross 0, n = 434, I² = 90%) (Analysis 3.17).
3.17. Analysis.

Comparison 3: CBT versus attention control, Outcome 17: Reduction in anxiety symptoms (parent report) at follow‐up
Only two studies reported child‐reported anxiety symptoms and parent‐reported anxiety symptoms at 12 months follow‐up (Rosa Alcazar 2009; Silverman 1999a), so meta‐analyses for these outcomes were not possible for this time point.
Comparison 4: CBT versus alternative treatment
See Table 4.
Primary outcomes
4.1 Remission of primary anxiety diagnosis post‐treatment
Only two studies that compared CBT to an alternative treatment reported post‐treatment remission of primary anxiety disorder (Creswell 2017; Reigada 2015), therefore data were insufficient to conduct meaningful meta‐analysis or planned subgroup analyses for this outcome.
4.2 Acceptability: loss of participants to post‐treatment assessment
Low‐quality evidence showed no difference between CBT and alternative treatments in rate of those lost to post‐treatment assessment (OR 1.58, 95% CI crosses 1, Z = 0.94, P = 0.35, k = 7, n = 515, I² = 53%), suggesting no difference in degree of acceptability (Analysis 4.1).
4.1. Analysis.

Comparison 4: CBT versus alternative treatment, Outcome 1: Acceptability (number of participants lost to post‐treatment assessment)
Secondary outcomes
4.3 Remission of all anxiety disorders post‐treatment
Pooled data from four studies that reported remission of all anxiety disorder diagnoses post‐treatment showed no difference between CBT and alternative treatment groups in either ITT analyses (OR 0.89, 95% CI crosses 1, Z = 0.25, P = 0.80, n = 401, I² = 73%, low‐quality evidence) or completer analyses (OR 1.52, 95% CI crosses 1, Z = 1.06, P = 0.29, n = 348, I² = 57%) (Analysis 4.2; Analysis 4.3) (Creswell 2017; Lebowitz 2019; Reigada 2015; Silk 2018).
4.2. Analysis.

Comparison 4: CBT versus alternative treatment, Outcome 2: Remission of all anxiety diagnoses post‐treatment (ITT)
4.3. Analysis.

Comparison 4: CBT versus alternative treatment, Outcome 3: Remission of all anxiety diagnoses post‐treatment (completers)
4.4 Reduction in anxiety symptoms (child‐report) post‐treatment
Low‐quality evidence showed no differences between CBT and alternative treatment groups in post‐treatment child‐reported anxiety symptoms (SMD −0.09, 95% CI crosses 0, Z = 0.58, P = 0.56, k = 6, n = 399, I² = 51%) (Analysis 4.4). Removal of one study that used a disorder‐specific symptom measure did not change this finding (Analysis 4.5).
4.4. Analysis.

Comparison 4: CBT versus alternative treatment, Outcome 4: Reduction in anxiety symptoms (child report) post‐treatment
4.5. Analysis.

Comparison 4: CBT versus alternative treatment, Outcome 5: Sensitivity analysis: reduction in anxiety symptoms (child report) post‐treatment (broad anxiety measures only)
4.5 Reduction in anxiety symptoms (parent‐report) post‐treatment
We also found no significant differences between CBT and alternative treatment groups in post‐treatment parent‐reported anxiety symptoms (SMD −0.13, 95% CI −0.33 to 0.06, Z = 1.31, P = 0.19, k = 6, n = 423, 6 studies, I² = 0%, low‐quality evidence) (Analysis 4.6). The studies all used a broad‐based anxiety measure, so planned sensitivity analysis was not required.
4.6. Analysis.

Comparison 4: CBT versus alternative treatment, Outcome 6: Reduction in anxiety symptoms (parent report) post‐treatment
4.6 Reduction in depressive symptoms post‐treatment
Only only study reported post‐treatment depressive symptoms (Salum 2018), so meta analysis was not possible.
4.7 Improvement in global functioning post‐treatment
No studies reported post‐treatment global functioning for CBT versus alternative treatments.
4.8 Adverse events
No included study reported adverse events in both CBT and alternative treatment groups, so meta‐analysis was not possible.
4.9 Follow‐up outcomes
For each of the longer‐term outcomes, data were only available from a maximum of two studies, so meta‐analyses were not possible.
Publication bias
We investigated publication bias in relation to remission of the primary anxiety disorder post‐treatment for CBT versus waitlist controls, and CBT versus attention controls.
CBT versus waitlist/no treatment
There was clear evidence of publication bias from inspection of the funnel plot (Figure 7), which was asymmetric, and the Egger’s test, which was highly significant (t = 5.52, P < 0.000). Furthermore, a contour funnel plot (not included here) indicated that the missing studies were in the areas of low significance, more compatible with publication bias than other explanations of funnel plot asymmetry such as variable study design (Peters 2008).
7.

Funnel plot of comparison: 1 CBT vs waitlist/no treatment, outcome: 1.1 Remission of primary anxiety diagnosis post‐treatment (ITT).
CBT versus attention control
There was no evidence of publication bias with a symmetrical funnel plot (Figure 8) and non‐significant Egger’s test (t = 1.99, P = 0.072).
8.

Funnel plot of comparison: 3 CBT vs attention control, outcome: 3.1 Remission of primary anxiety diagnosis post‐treatment (ITT).
Discussion
Summary of main results
Since the last Cochrane Review, James 2015, there has been a considerable increase in the number of studies available for review, from 41 to 88, with more than three times the total number of participants. We found moderate‐quality evidence that CBT leads to greater remission of primary and all anxiety disorders than waitlist/no treatment in the short term. Using conservative ITT criteria, we found a remission rate of 49% for the primary anxiety disorder for CBT versus 18% for waitlist/no treatment controls (OR 5.45, 95% CI 3.90 to 7.60). Although this indicates a slight attenuation in effects from the last Cochrane Review, this is not uncommon as studies accumulate over time. Consistent with the last review, the number needed to treat for an additional beneficial outcome (NNTB) using these conservative ITT data was 3 (95% CI 2.25 to 3.57). Notably, the benefit of CBT compared to waitlist/no treatment controls was shown across all post‐treatment outcomes, albeit with uncertain evidence due to variation in reductions in child‐ and parent‐reported anxiety symptoms, and depressive symptoms, and limited data related to global functioning.
Unfortunately, despite the general increase in studies, there remains a relatively small number of studies comparing CBT to 'active' controls, and where this has been done the control arms included a broad range of interventions (from undefined and variable ‘treatment as usual’ to attention controls, and in a small number of cases treatments that might credibly be delivered in practice). Due to insufficient data, there was low‐quality evidence for each of these comparisons across most outcomes. Encouragingly, the available data did indicate that CBT may be associated with a higher rate of remission of the primary anxiety disorder and all anxiety disorders and a greater reduction in child‐reported anxiety symptoms, compared to attention controls. However, the limited data did not reveal an advantage of CBT compared to treatment as usual across most outcomes, or indicate a benefit of CBT compared to specified alternative treatments. Furthermore, we were unable to compare CBT to medication or CBT in combination with medication to drug placebo due to a lack of available studies.
Unsurprisingly given the high frequency of waitlist control designs, there also continues to be only a very small number of studies that have controlled outcomes at longer‐term follow‐up points. Where outcomes beyond post‐treatment were available, the studies had mixed results, but in terms of remission of the primary anxiety disorder, the current findings support an advantage of CBT compared to waitlist/no treatment and attention controls six months after treatment. However, there is as yet no evidence that this advantage of CBT continues at later time points, and there were insufficient data to determine whether any longer‐term benefits hold up against treatment as usual or alternative treatments.
Previous Cochrane Reviews on this topic have only included studies that involved children older than four years of age; however, in the current review we removed this restriction in order to identify the age of the youngest participants in RCTs of CBT for child anxiety disorders, and to explore relative outcomes for different age groups. We identified studies that included children as young as two years of age. Notably, studies with younger children typically took a parent‐led approach in which parents were supported by a clinician to implement CBT principles in their child’s day‐to‐day life (e.g. Cartwright Hatton 2011).
Given the low number of children with anxiety disorders who access evidence‐based treatments for anxiety disorders (e.g. Reardon 2020), we specifically looked at outcomes for subgroups of studies categorised by the amount of therapist contact time. Relatively few studies involved less than 10 hours of therapist contact time, limiting the amount of data available. However, primary anxiety disorder and anxiety symptom outcomes for CBT compared to waitlist/no treatment did not differ from the more lengthy treatments. The currently available data therefore suggests that services could provide CBT programmes that involve relatively low levels of therapist contact time without a negative impact on post‐treatment outcomes.
The wide variation across trials in relation to a range of study and sample characteristics limits our ability to draw clear conclusions about particular treatment formats or age groups. Amongst waitlist/no treatment comparisons, we found stronger effects for child‐focused CBT than child‐and‐parent and parent‐only interventions. However, parent involvement in trials is related to potentially confounding factors (e.g. child's age, study setting), and even within the child‐focused CBT studies there was considerable heterogeneity in outcomes and variation across study characteristics. Indeed, although we also found variation in outcomes amongst different age groups for CBT versus wait list/no treatment comparisons, this differed according to outcome and may indicate age‐related measurement issues, rather than differences in true effects. We found stronger effects amongst samples of adolescents than samples of children or mixed child/adolescent samples on child‐ and parent‐reported anxiety symptoms, but not in terms of remission of primary or all anxiety disorders. We found a similar picture when looking at subgroups of studies on the basis of whether they delivered CBT with individuals or groups. For example, there was no evidence of different results on diagnostic outcomes, but outcomes for group formats were stronger than individual formats when parent‐ and child‐reported symptoms were assessed (in the waitlist/no treatment comparison). Again, various potential confounders are likely to have influenced these outcomes, including, for example, participant age, study setting (e.g. school versus clinic), and target disorders. Consequently, on the basis of findings relating to treatment format, the currently available literature does not give clear and consistent evidence that one format is better or worse than any other.
Finally, we also set out to assess outcomes specifically for children with autism spectrum disorders (ASD) and intellectual disabilities. Twelve studies evaluated CBT for the treatment of anxiety disorders in children with ASD, with mixed findings across comparisons and outcomes. Notably, the four studies that compared CBT to treatment as usual for children with ASD (where 'treatment as usual' typically meant participants could continue to seek alternative interventions only) did find a consistent advantage of CBT in relation to remission of primary anxiety disorder. However, amongst waitlist/no treatment control comparisons, we only found evidence of a benefit for CBT in parent‐reported anxiety symptoms, not child‐reported symptoms or diagnostic outcomes. No RCTs evaluated the effectiveness of CBT for anxiety disorders amongst children with intellectual disabilities.
Overall completeness and applicability of evidence
As in the previous Cochrane Review, almost all included studies involved participants of both sexes. Whilst a number of countries are represented in this review, it is notable that they were almost exclusively high‐income countries (with two‐thirds of the included studies having been conducted either in the USA or Australia).
Although the overall age of participants ranged from 2 to 18 years, less than 30% of studies focused specifically on children up to age 12 (with less than 6% focusing on children under 8 years of age), and less than 20% focused specifically on adolescents, with the majority including children and adolescents across broad age ranges. This made it difficult to draw conclusions on the basis of specific child ages.
We included participants with comorbid disorders such as depression, other anxiety disorders, ADHD, and conduct disorders, permitting generalised conclusions that appear to be applicable to clinical practice. However, the majority of studies were conducted in outpatient settings, with 41 studies conducted in university‐based research settings. We considered other settings, including primary care and schools; notably, however, no studies were conducted with the most severe cases who receive treatment as day‐ or inpatients, which is perhaps a reflection of the challenges associated with running trials in these settings. Despite the continued growth in studies evaluating CBT for anxiety disorders in general, there were few additional studies that targeted children with ASD since the last Cochrane Review, and the lack of evaluation of CBT for anxiety disorders, including parent‐only approaches, amongst children with intellectual disabilities remains a considerable limitation.
It is important to note that we conducted separate analyses for different diagnostic and child/parent report measures; this meant that given the high levels of inconsistency in measures used and how they were reported, only a subset of studies were included in any one analysis. The most consistent diagnostic outcome measure was remission of the primary diagnosis (included in about two‐thirds of the CBT versus waitlist/no treatment comparisons), whereas less than half of the studies reported remission of all anxiety disorder diagnoses. Some studies did not report remission of anxiety disorders in either of these ways, instead, for example, reporting remission from particular groups of diagnoses, or changes in the total number of different diagnoses. As a result, these studies were not included in our analyses of diagnostic outcomes. Similarly, relevant studies were identified that did not provide data on any of the target outcomes and were therefore not included in the review (e.g. Baer 2005; Flatt 2010; NCT00576719).
Encouragingly, the evidence of the acceptability of CBT was consistent across comparisons, with no difference in the number of CBT participants retained to post‐treatment assessments compared to each of the control groups. However, it is important to acknowledge that rates of attrition may in part reflect acceptability of the research process, and alternative measures of acceptability (e.g. participant perceptions of the intervention) were not assessed in this review.
As in previous Cochrane Reviews of CBT for child anxiety disorders, the number of follow‐up studies remains very limited (four studies reported on our primary outcome at follow‐up assessments), making it difficult to draw conclusions about the medium‐ to long‐term benefits of CBT. The available findings from controlled studies suggest that there is evidence that CBT provides an advantage over waitlist/no treatment six months after treatment, but there is currently no evidence to support longer‐term benefits. However, the recent Child/Adolescent Anxiety Multimodal Study (CAMS) highlights the importance of controlled outcome data at longer‐term follow‐up, based on their findings that over two‐thirds of patients that showed initial treatment gains relapsed over the following four years (Ginsburg 2018).
A major weakness found across studies was the absence of systematic reporting of adverse effects. No adverse effects were reported across all studies; however, in the small number of studies where any reference was made to adverse effects, it was not clear that these were systematically monitored. This issue is not limited to trials of CBT for child anxiety disorders; for example, Duggan 2014 reported that none of the 72 trials of psychological interventions considered in their systematic review mentioned the occurrence of adverse events in their final report, despite the recognition that psychological treatments can introduce a range of negative effects (Barlow 2010).
Given the limited data for treatment as usual, attention control, and alternative treatment comparisons, not all analyses were possible across all comparisons, and many of our subgroup analyses were limited to waitlist/no treatment comparisons.
Quality of the evidence
This review included 87 studies in the quantitative synthesis, with a reasonably large number of study participants (n= 5964). As noted above, we distinguished between baseline and outcome measures using tight criteria in order to ensure we were comparing like with like as far as possible. For example, we distinguished between remission in the primary anxiety disorder and remission of all anxiety disorders, and selected symptom measures that were most consistently reported, prioritising measures of broad anxiety symptoms where possible.
We rated evidence as moderate or low quality across comparisons and outcomes. There was consistent evidence for the benefit of CBT compared to waitlist/no treatment controls, but with moderate to substantial heterogeneity across outcomes, reducing certainty in the results. We assessed the evidence for CBT compared to treatment as usual, attention controls, and alternative treatments mostly as low quality, primarily due to the limited amount of available data.
We noted methodological shortcomings in some studies, although this typically reflected inadequate reporting, rather than evidence of high risk of bias, and was more common amongst older studies. Participant blinding is not possible in research on psychological interventions, which is an obvious potential source of bias; however, the evaluations were typically carried out blind. Nonetheless, we found similar outcomes when we removed studies with weaknesses related to allocation and blinding, supporting the robustness of the results.
Given the increase in number of studies available since previous reviews, we took the opportunity for a stricter approach to our inclusion criteria. We only included studies with robust randomisation procedures, and excluded studies included in other reviews where, for example, children who might be considered at risk were automatically enrolled in the intervention arm (e.g. Nauta 2003). However, we did include studies where assessment points differed between treatment arms, and, in some cases, the period between randomisation and assessment was twice as long in the intervention arm compared to the control arm (e.g. Fujii 2013; Kendall 1994; Kendall 1997), which clearly introduces the potential for substantial bias. The timing of the post‐treatment assessment (the assessment closest to the end of the treatment) also varied across trials.
There was evidence of publication bias (asymmetric funnel plot, significant Egger’s test and contour funnel plot), with a marked absence of non‐significant studies for both CBT versus waitlist/no treatment controls. This is an area that has been richly debated, and remains a significant area of concern when interpreting the results of meta‐analyses, as it is likely that, with the lack of published negative trials, any estimate of the effectiveness of an intervention (CBT in this case) is likely to be inflated. We welcome the call for journals to publish negative trials, and for chief investigators of all registered trials to publish findings, especially negative ones, online within a set time of the trial end date.
Potential biases in the review process
We were able to obtain all the referenced papers; we searched grey literature and reference lists; and made contact with leading researchers in the field. We also included studies that were not in the English language. However, meta‐analyses are limited by the robustness of any search method. The electronic search was thorough and large in scale with broad parameters. Of note, we broadened certain parameters since the last Cochrane Review on this topic, for example removing a restriction on the minimum number of sessions, minimum child age, and including CBT delivered via parents. Nonetheless, there are some limitations to the review. For example, whilst we set a fairly broad definition of ‘cognitive behaviour therapy’, some studies were excluded where the description of the intervention did not include all the core stated components of CBT despite the treatments appearing similar in many ways (e.g. social effectiveness therapy; Beidel 2000; Beidel 2007; behaviour therapy; Rudy 2017; Storch 2019), and it is possible that the brief descriptions of treatments provided in papers may not fully reflect how the treatment is being delivered in practice. We also required some in‐person treatment delivery, and therefore did not include CBT interventions delivered online or purely over the telephone, despite these interventions often being very similar in content. Indeed there is evidence supporting the effectiveness of these remotely delivered approaches (e.g. Lyneham 2006; Pennant 2015).
The analysis of studies with three arms ‐ CBT in two formats versus waiting list controls or active controls ‐ is problematic in that double counting of any group is wrong. We chose a conservative approach to managing this by splitting the control samples into two equal halves between the CBT groups; however, this means that in these cases the odds ratios and confidence intervals appear smaller despite recovery rates that are similar to those found in other studies (e.g. Flannery Schroeder 2000; Thirlwall 2013). We also prioritised ITT analyses and adopted a conservative approach in which drop out in the treatment group was treated as if the participant did not recover, but drop out in the control group was treated as recovery. This conservative approach may have underestimated treatment effects; unsurprisingly, treatment effects were larger in the follow‐up completer analyses. Whilst we took a strict approach to measures that were included (only using specific measures of anxiety symptoms and not, for example, combined measures of emotional and behavioural symptoms), and prioritised broad measures of anxiety symptoms to promote consistency, this may have come at a disadvantage for studies that focused on treating specific disorders, where only a subset of the items on a broad measure might apply to the target of treatment.
Agreements and disagreements with other studies or reviews
Two previous Cochrane Reviews have been conducted on this topic. The first review identified 18 studies with 498 participants and 311 controls, and found a response rate for remission of any measure of anxiety diagnosis using an ITT analysis of 56% for CBT versus 28.2% for controls with the NNTB of 3.0 (95% CI 2.5 to 4.5) (James 2005). The second review identified 41 studies with 1806 participants, with a rate of remission of any measure of anxiety disorder of 58.9% for CBT versus 16% for the waitlist (James 2015). In the current review, we identified a further substantial increase in studies, including 81 studies with 5964 participants. We made a number of changes, most notably distinguishing between remission of the primary anxiety disorder and remission of all anxiety disorders; however, the findings were fairly consistent, with 49.4% of participants being free of their primary anxiety disorder following CBT (versus 17.8% for waitlist controls), and 46.8% being free of all anxiety disorders (versus 19.1% for waitlist controls). It is important to note that studies presenting remission based on primary diagnosis and all anxiety diagnoses only partly overlapped, so these outcomes should not be compared directly. Despite the differences in outcome measures, and our broader inclusion criteria for CBT formats, length, and participant ages, the NNTB has been consistent at NNTB = 3 across all three Cochrane Reviews. These effects are consistent with other meta‐analyses of CBT for anxiety disorders in children and young people (e.g. Cartwright‐Hatton 2004; Compton 2004; Reynolds 2012; Seligman 2011; Silverman 2008; Wang 2017; Warwick 2016).
Our findings are also consistent with previous reviews in terms of the limited available data for comparisons with treatment as usual/alternative treatments (e.g. Wang 2017). Indeed, like others, we have concluded that there is no clear evidence of an advantage of CBT over treatment as usual or treatments that might credibly be used within mental health settings. However, we did find more consistent evidence of an advantage of CBT over attention controls, although the available data are still limited.
However, our conclusions differed from those of a recent network meta‐analysis of psychotherapies for anxiety disorders in children and young people, which concluded that group CBT was more effective that other forms of psychotherapy (including other CBT formats included in this review) (Zhou 2019). Notably, this network meta‐analysis considered outcomes based on symptom questionnaires (prioritising child self‐report). Indeed, when we consider our subgroup analyses, amongst waitlist/no treatment comparisons, we also found stronger effects of group CBT than individual CBT on child‐ and parent‐reported anxiety symptoms; however we did not find significant differences between these subgroups based on our primary outcome (remission of primary anxiety diagnosis) or on our other diagnostic outcome (free of all anxiety diagnoses). Furthermore, studies that differed in terms of treatment delivery format also differed on a number of other characteristics that would likely be associated with outcome (including differences in the study setting, population, and nature of outcome measures). For example, most (5 out of 7) studies that only reported disorder‐specific symptom measures were studies that evaluated treatments delivered in groups, so differences between group versus individual formats may reflect a measurement issue rather than a true difference in effect sizes. As such, we do not feel that the evidence provides clear and consistent support for group CBT having an advantage over other delivery formats.
The same conclusion applies to treatment delivery with children, children and parents, or parents alone. Like previous reviews (e.g. Breinholst 2012; Reynolds 2012; Silverman 2008), we did not find clear evidence of an advantage of any of these delivery formats. Although we found the strongest effects for child‐focused CBT among waitlist/no treatment comparisons, there was considerable variation in findings amongst child‐focused CBT studies, and the treatment delivery subgroups also often differed on other key study and sample characteristics (e.g. child age, setting, comorbidities, treatment duration). Notably, there were relatively few studies that delivered treatment through parents only, and these tended to be more recent studies and included children of younger ages than studies that took a child‐only or child‐and‐parent approach.
Where there were sufficient studies, we generally found fairly consistent findings regardless of whether children in the studies had ASD or not, supporting the evidence from previous meta‐analyses suggesting that CBT can be an effective treatment of anxiety for children with ASD (e.g. Perihan 2019; Ung 2015). Notably, recent reviews have suggested that parental involvement may be particularly important for treating childhood anxiety disorders in the context of ASD, and that longer‐term interventions were associated with larger effects (Perihan 2019). These questions are beyond the scope of the current review; however, it is noteworthy that neither of these sets of findings were replicated in our broader sample, highlighting the need to consider the specific conditions that are needed to optimise CBT approaches amongst particular subgroups of children and young people with anxiety disorders.
Authors' conclusions
Implications for practice.
This review reinforces conclusions from previous reviews finding moderate‐quality evidence that cognitive behavioural therapy (CBT) is more effective in improving diagnostic outcomes in the short term than a waiting list or no treatment. The advantage of CBT compared to waitlist/no treatment is evident across a range of other short‐term outcomes, although variation in findings or limited available data, or both, reduces certainty in these results. Clear and consistent evidence of differences between the formats of individual, group, and parent/family CBT continues to be lacking. Available, low‐quality evidence supports a benefit of CBT compared to attention control, but the evidence base remains small, and there continues to be insufficient and inclusive evidence that CBT is superior to either treatment as usual or alternative treatments.
Pharmacological interventions are typically not recommended as a first‐line treatment due to patient preference (e.g. Brown 2007), relative high rates of attrition, and concerns about potential side effects (Wang 2017). However, we know very little about the comparative efficacy of pharmacological interventions and CBT, with evidence still limited to one, albeit large, multicentre study (Walkup 2008). Clearly further work is needed to guide practice about the circumstances in which pharmacological approaches might be most acceptable and effective for the treatment of anxiety disorders in children and young people.
A major challenge for clinical practice is the very limited access that children with anxiety disorders have to evidence‐based psychological interventions, such as CBT. In a recent study, only 2% of children with anxiety disorders identified in the community in England had received CBT (Reardon 2020). These findings are consistent with previous studies indicating low rates of service use in the UK, Australia, and the USA (Green 2004; Lawrence 2015; Merikangas 2011). Of importance to this clinical challenge is our finding that there is currently no evidence of differences in outcome on the basis of therapist contact time, with similar effects being achieved when therapists provided less than 10 hours of clinical contact compared to higher amounts of clinical contact in terms of remission of the primary anxiety disorder and child‐ and parent‐reported anxiety symptoms. Notably, results were less strong in terms of remission of all anxiety disorders; however, there is evidence to suggest that benefits might generalise to other disorders beyond the end of (brief) treatment (e.g. Ollendick 2010). These findings indicate that access could be improved through the provision of stepped‐care models of treatment delivery in which relatively brief interventions are offered as a first‐line approach, and more intensive interventions are saved for those who need them (Bower 2005). A recent systematic evaluation of stepped‐care treatment for child anxiety disorders provided promising evidence for a benefit of a stepped‐care approach in terms of clinical time saved and reduced societal costs (Chatterton 2019).
Implications for research.
There is now sufficient evidence to conclude that CBT is an effective treatment for anxiety disorders in children and young people when compared to waiting lists/no treatment.
A number of reviews have concluded that overall about 50% of children and young people recover from their primary anxiety disorder following a course of CBT, but still very little is known about how these outcomes can be improved and what the other 50% of patients need. A better understanding of what the core mechanisms of effective interventions are and how this varies according to individual characteristics or contexts is needed. For example, currently very little is known about how treatments should best be delivered according to child age and developmental status, the presence of comorbid conditions, or the nature of the anxiety disorders experienced. Almost three‐quarters of the studies in this review included children with a broad range of anxiety disorders, and those that focused on specific disorders were spread across studies of, for example, social anxiety disorder, selective mutism, panic disorder, generalised anxiety disorder, and specific phobia, thereby limiting our ability to draw firm conclusions about any particular approach for any particular disorder, let alone how that might vary according to, for example, child age. Larger studies that are sufficiently powered to examine predictors, mediators, and moderators of treatment outcomes are now needed to identify how to improve treatment outcomes and develop more personalised models of care.
Individual patient data meta‐analyses may be useful to help us better understand the extensive heterogeneity between study outcomes; however, meaningful conclusions will rely on clear and consistent reporting across studies so that data can be linked in sensible ways. In this review we focused on remission of the primary and all anxiety diagnoses, but a number of studies were excluded from these analyses as they reported other kinds of data from diagnostic assessments. This issue was highlighted in a recent position paper which set out a number of recommendations for reporting and terminology to promote greater consistency going forwards (Creswell 2020a). It is important to note a number of other areas where the field would benefit from greater clarity and consistency in reporting by researchers. For example, in treatment as usual studies, it was not always clear what 'treatment as usual' actually consisted of and to what extent it differed from the index treatment or a no treatment control. Indeed, categorising the format of any treatment typically relied on only a brief description, which may have led to faulty conclusions. We encourage researchers to make good use of online supplementary materials to ensure clear descriptions of the content and format of interventions, using consistent terminology (Creswell 2020a).
There continues to be a lack of evidence that CBT is superior to other credible alternative treatments, so it will be essential to identify what the core components of effective treatments are, for example through experimental and treatment dismantling studies (e.g. Whiteside 2015), so that outcomes can be optimised and treatments can be targeted to maximise their efficiency. Head‐to‐head comparisons of different active (and credible) interventions will be required, but these will inevitably require larger sample sizes, as they will need to be set up to detect smaller effects than those found with waitlist/no treatment comparisons; however, these designs will also enable studies to compare longer‐term outcomes between groups. Given the risks for longer‐term adjustment of anxiety disorders in childhood and adolescence, controlled studies with longer‐term outcomes are essential to ensure that children’s life trajectories are being optimally supported through early intervention.
As noted above, increasing access to effective treatments is an urgent challenge for our field, and it will be essential that studies consider accessibility of treatment and cost‐effectiveness going forwards. We did not consider outcomes in terms of cost‐effectiveness in this review; however, it is clear that to date very few studies have taken cost‐effectiveness into account when evaluating CBT for child anxiety disorders. We anticipate that cost‐effectiveness data will have a marked impact on the clinical implications that can be drawn from the available evidence, particularly given our finding that clinician contact time did not seem to be related to treatment outcome. Equally, it is often assumed that group treatments may be cost‐effective; however, this has not been supported when evaluated in other contexts (e.g. Mavranezouli 2015), and some of the group treatments identified in this review involved very high levels of therapist involvement and supported activities. Future studies would benefit from including a cost‐effectiveness analysis, and considering the costs and benefits to both the health service and broader society including costs related to the child themselves and family members, whose work and home lives are often heavily impacted by child anxiety problems (e.g. Bodden 2008b).
Finally, it was disappointing to see that, whilst the number of trials evaluating CBT for childhood anxiety disorders has increased substantially, these have not extended to children in low‐ or middle‐income countries, children with intellectual disabilities or physical health conditions, the most severely affected children in inpatient settings, and there are still very few studies that have focused specifically on either young children or (strikingly given the prevalence of anxiety disorders) adolescents.
What's new
| Date | Event | Description |
|---|---|---|
| 13 November 2020 | New search has been performed | This Cochrane Review supersedes the Cochrane Review 'Cognitive behavioural therapy for anxiety disorders in children and adolescents' published in 2015 (James 2015). |
History
Protocol first published: Issue 10, 2018 Review first published: Issue 11, 2020
Acknowledgements
Oxford Health Foundation NHS Trust, Guy’s and St Thomas’ NHS Foundation Trust, National Institute for Health Research (NIHR), the University of Reading, and the University of Oxford provided support to the review authors to complete this review.
We are extremely grateful to the Cochrane Common Mental Disorders Group (CCMD) for their guidance, and in particular to Sarah Dawson (CCMD Information Specialist) for her input.
The authors and the Cochrane Common Mental Disorders Editorial Team are grateful to the protocol peer reviewers and Copy Edit Support for their time and comments. Peer reviewers included: Georgina Cox, Lina Gega, David Marshall, Ruth Simmonds, and Gill Worthy.
Cochrane review group funding acknowledgement: the NIHR is the largest single funder of Cochrane Common Mental Disorders.
Disclaimer: the views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR, or the Department of Health and Social Care.
Appendices
Appendix 1. Hierarchy of anxiety symptoms measures
| Broad‐based anxiety measures |
| 1. Spence Children’s Anxiety Scale (SCAS) (child‐/parent‐report versions) or derivatives of the SCAS, including Revised Children’s Anxiety and Depression Scale (RCADS) (child‐ and parent‐report versions) Anxiety Scale and the Preschool Anxiety Scale (parent‐report) |
| 2. Multidimensional Anxiety Scale for Children (MASC) (child‐ and parent‐report versions) |
| 3. Screen for Child Anxiety Related Disorders (SCARED) (child‐ and parent‐report versions) |
| 4. Revised Children’s Manifest Anxiety Scale (RCMAS) |
| 5. State‐Trait Anxiety Inventory for Children (STAIC) ‐ Trait Scale |
| 6. Child and Adolescent Symptom Inventory‐4 ASD Anxiety Scale |
| Social anxiety (disorder‐specific) measures |
| 7. Social Phobia and Anxiety Inventory for Children (SPAI‐C) |
| 8. Social Anxiety Scale for Adolescents (SAS‐A)/Social Anxiety Scale for Children‐Revised (SASC‐R) |
Appendix 2. Cochrane Common Mental Disorders Controlled Trials Register (CCMDCTR)
Cochrane Common Mental Disorders Controlled Trials Register (CCMDCTR)
Cochrane Common Mental Disorders (CCMD) maintains two archived clinical trials registers at its editorial base in York, UK: a references register and a studies‐based register. The CCMDCTR‐References Register contains over 40,000 reports of RCTs in depression, anxiety and neurosis. Approximately 50% of these references have been tagged to individual, coded trials. The coded trials are held in the CCMDCTR‐Studies Register and records are linked between the two registers through the use of unique Study ID tags. Coding of trials is based on the EU‐Psi coding manual, using a controlled vocabulary; (please contact the CCMD Information Specialists for further details). Reports of trials for inclusion in the Group's registers are collated from routine (weekly), generic searches of MEDLINE (1950 to 2016), Embase (1974 to 2016) and PsycINFO (1967 to 2016); quarterly searches of the Cochrane Central Register of Controlled Trials (CENTRAL) and review‐specific searches of additional databases. Reports of trials are also sourced from international trial registers via the World Health Organization's trials portal (the International Clinical Trials Registry Platform (ICTRP)), pharmaceutical companies, the handsearching of key journals, conference proceedings and other (non‐Cochrane) systematic reviews and meta‐analyses.
Details of CCMD's generic search strategies (used to identify RCTs) can be found on the Group's website, (cmd.cochrane.org/specialised-register), with an example of the core MEDLINE search (used to inform the register) listed below. The Group’s Specialised Register has fallen out of date with the Editorial Group’s move from Bristol to York in the summer of 2016.
Core search strategy used to inform the Cochrane Common Mental Disorders Group's Specialised Register: OVID MEDLINE (to June 2016)
A weekly search alert based on condition + RCT filter only 1. [MeSH Headings]: eating disorders/ or anorexia nervosa/ or binge‐eating disorder/ or bulimia nervosa/ or female athlete triad syndrome/ or pica/ or hyperphagia/ or bulimia/ or self‐injurious behavior/ or self mutilation/ or suicide/ or suicidal ideation/ or suicide, attempted/ or mood disorders/ or affective disorders, psychotic/ or bipolar disorder/ or cyclothymic disorder/ or depressive disorder/ or depression, postpartum/ or depressive disorder, major/ or depressive disorder, treatment‐resistant/ or dysthymic disorder/ or seasonal affective disorder/ or neurotic disorders/ or depression/ or adjustment disorders/ or exp antidepressive agents/ or anxiety disorders/ or agoraphobia/ or neurocirculatory asthenia/ or obsessive‐compulsive disorder/ or obsessive hoarding/ or panic disorder/ or phobic disorders/ or stress disorders, traumatic/ or combat disorders/ or stress disorders, post‐traumatic/ or stress disorders, traumatic, acute/ or anxiety/ or anxiety, castration/ or koro/ or anxiety, separation/ or panic/ or exp anti‐anxiety agents/ or somatoform disorders/ or body dysmorphic disorders/ or conversion disorder/ or hypochondriasis/ or neurasthenia/ or hysteria/ or munchausen syndrome by proxy/ or munchausen syndrome/ or fatigue syndrome, chronic/ or obsessive behavior/ or compulsive behavior/ or behavior, addictive/ or impulse control disorders/ or firesetting behavior/ or gambling/ or trichotillomania/ or stress, psychological/ or burnout, professional/ or sexual dysfunctions, psychological/ or vaginismus/ or Anhedonia/ or Affective Symptoms/ or *Mental Disorders/ 2. [Title/ Author Keywords]: (eating disorder* or anorexia nervosa or bulimi* or binge eat* or (self adj (injur* or mutilat*)) or suicide* or suicidal or parasuicid* or mood disorder* or affective disorder* or bipolar i or bipolar ii or (bipolar and (affective or disorder*)) or mania or manic or cyclothymic* or depression or depressive or dysthymi* or neurotic or neurosis or adjustment disorder* or antidepress* or anxiety disorder* or agoraphobia or obsess* or compulsi* or panic or phobi* or ptsd or posttrauma* or post trauma* or combat or somatoform or somati#ation or medical* unexplained or body dysmorphi* or conversion disorder or hypochondria* or neurastheni* or hysteria or munchausen or chronic fatigue* or gambling or trichotillomania or vaginismus or anhedoni* or affective symptoms or mental disorder* or mental health).ti,kf. 3. [RCT filter]: (controlled clinical trial.pt. or randomized controlled trial.pt. or (randomi#ed or randomi#ation).ab,ti. or randomly.ab. or (random* adj3 (administ* or allocat* or assign* or class* or control* or determine* or divide* or distribut* or expose* or fashion or number* or place* or recruit* or subsitut* or treat*)).ab. or placebo*.ab,ti. or drug therapy.fs. or trial.ab,ti. or groups.ab. or (control* adj3 (trial* or study or studies)).ab,ti. or ((singl* or doubl* or tripl* or trebl*) adj3 (blind* or mask* or dummy*)).mp. or clinical trial, phase ii/ or clinical trial, phase iii/ or clinical trial, phase iv/ or randomized controlled trial/ or pragmatic clinical trial/ or (quasi adj (experimental or random*)).ti,ab. or ((waitlist* or wait* list* or treatment as usual or TAU) adj3 (control or group)).ab.) 4. (1 and 2 and 3) Records are screened for reports of RCTs within the scope of the Cochrane Common Mental Disorders Group. Secondary reports of RCTs are tagged to the appropriate study record. Similar weekly search alerts are also conducted on OVID Embase and PsycINFO, using relevant subject headings (controlled vocabularies) and search syntax, appropriate to each resource.
Search strategy for this review
The CCMDCTR was searched for this review using the following terms:
CCMDCTR‐Studies (all years up to June 2016) #1 (anxiety or anxious or phobi* or agoraphobi* or panic or mutism or "school refusal") and STUDY:CRSTYPE and INSEGMENT #2 behavio* or cognitive or counsel* or train* or therap* or psychotherap* and STUDY:CRSTYPE and INSEGMENT #3 (child* or adolescent*) and STUDY:CRSTYPE and INSEGMENT #4 (#1 or #2 or #3) CCMDCTR‐References (all years up to June 2016) [Outcomes] #1 (ADIS‐C* or ADIS‐P* or DISCAP or SCARED or SCAS or RCADS or RCMAS or MASC or CBCL or STAI‐C or SPAI‐C or SAS‐A) AND INSEGMENT [Condition] #2 (“anxiety disorder*” or agoraphobi* or “generalized anxiety” or “generalised anxiety” or GAD or (separation near2 anxiety) or (social near2 anxi*) or (social near2 phobi*) or phobi* or panic or mute* or mutism or (school near2 refus*)) AND INSEGMENT #3 ((infant* or child* or adolesc* or pediatric* or paediatric* or teen* or young* or youth or school* or preschool*) near2 anxi*) AND INSEGMENT #4 (anxiety. and (autism or autistic or “child development disorder*”)) AND INSEGMENT #5 (anxiety or panic or phobi* or agoraphobi*):ti AND INSEGMENT [Intervention] #6 ((ACCEPTANCE and COMMITMENT) or “ANXIETY MANAGEMENT” or “BEHAVIOUR MODIFICATION” or “BEHAVIOR MODIFICATION” or “BEHAVIOURAL MODIFICATION” or “BEHAVIORAL MODIFICATION” or BIBLIOTHERAPY or “COGNITIVE BEHAVIOUR THERAPY“ or “COGNITIVE BEHAVIOR THERAPY“ or “COGNITIVE BEHAVIOURAL THERAPY“ or “COGNITIVE BEHAVIORAL THERAPY“ or “COGNITIVE THERAPY“ or “COGNITIVE TECHNIQUES” or “COGNITIVE RESTRUCTURING” or COUNSELING or (PSYCHOTHERAPY near2 GROUP) or “FAMILY THERAPY” or “GROUP THERAPY” or MINDFULNESS or “PLAY THERAPY” or PSYCHODRAMA or PSYCHOTHERAPY or “RATIONAL EMOTIVE THERAPY” or RELAXATION or “ROLE PLAYING” or “SENSITIVITY TRAINING” or BIBLIOTHERAPY or “SELF CONTROL”):emt,mh,kw,ky AND INSEGMENT #7 (CBT or CBGT* or bCBT or b‐CBT or GPDCBT or GPD‐CBT) AND INSEGMENT #8 ((cogniti* or behavio*) near3 (counsel* or intervention or therap* or psychotherap* or training or treatment or technique* or restructur* or defusion)):ti,ab AND INSEGMENT #9 (“rational emoti*” or (problem* near2 (focus* or sol*)) or psychoeducat* or “role play*” or schema* or “self‐control*” or “self control*”):ti,ab AND INSEGMENT #10 (((psychotherap* or therap*) near3 (commitment or acceptance)) or ((self* or stress*) near3 (control or analysis or direct* or esteem or help or instruct* or manage*))):ti,ab AND INSEGMENT #11 ((attribution* or reattribution*) near3 (therap* or psychotherap*)):ti,ab AND INSEGMENT #12 (mindfulness* or “third wave” or experiential or (behavio* near3 (activation or modification)) or (thought* near3 suppress*) or rumination):ti,ab AND INSEGMENT #13 (“anxiety manag*” or “confidence building” or “coping skills” or “exposure therapy” or “exposure task*” or psychoeducat* or psycho‐educat* or relaxation or “sensitivity training” or “self talk” or (social near2 (coach* or skill* or effectiveness))):ti,ab AND INSEGMENT #14 ((controlling or overcoming) near2 (anxiety or panic or phobi* or agoraphobi* or shyness)):ti,ab AND INSEGMENT #15 (child* near2 (cent* or deliver* or focus*) adj2 (counsel* or intervention* or program* or psychotherap* or therap* or train* or treat*)):ti,ab AND INSEGMENT #16 ((parent* or guardian*) near2 (cent* or deliver* or focus*) adj2 (counsel* or intervention* or program* or psychotherap* or therap* or train* or treat*)):ti,ab AND INSEGMENT #17 ((individually or group or conjoint or family) near2 (counsel* or intervention* or program* or psychotherap* or therap* or train* or treat*)):ti,ab AND INSEGMENT [Age Group] #18 (infant* or child* or adolesc* or paediatr* or pediatr*):emt,mh,kw,ky,so AND INSEGMENT #19 (infant* or child* or boy* or girl* or kids or juvenil* or minors or paediatric* or pediatric* or adolesc* or preadolesc* or pre‐adolesc* or pubert* or pubescen* or prepube* or pre‐pube* or teen* or (young next (survivor* or offender* or minorit*)) or youth* or school* or preschool* or nurser* or kindergarten):ti,emt,mh,kw,ky AND INSEGMENT #20 (#2 OR #3 OR #4 OR #5) [Condition] #21 (#6 OR #7 OR #8 OR #9 OR #10 OR #11 OR #12 OR #13 OR #14 OR #15 OR #16 OR #17) [Intervention] #22 (#18 OR #19) [Age Group] #23 (#20 AND #21 AND #22) #24 ((anxi* or phobi* or agoraphobi* or panic) and (effectiveness or efficacy or evaluat* or intervention or program* or train* or treat* or prevent* or therapy or psychotherapy or trial or study) and (infant* or child* or adolesc* or paediatric* or pediatric* or teen* or young* or youth or school* or preschool*)):ti AND INSEGMENT #25 (#24 AND #21) #26 (#1 OR #23 OR #25) #27 ((OCD or obsessive compulsive or PTSD or posttraumatic stress disorder* or post‐traumatic stress disorder*) not (anxi* or phobi* or agoraphobi* or panic)):ti AND INSEGMENT #28 (#26 not #27) #29 ((pregnan* or "post natal" or postnatal* "post partum" or postpartum) not (adolesc* or teen* or young* or youth*)):ti AND INSEGMENT #30 (#28 not #29) #31 (“Coping Cat” or “Cool Kids” or “Coping Koala” or “Face your Fear” or “Face your Fears” or “Facing your Fear” or “Facing your Fears” or (“Multimodal Anxiety” and “Social Skills”) or (Academic and Skills and ”Social Success”) or (Intervention near adolesc* near “Social Phobia”) or BIACA or IAFS or MASSI or SASS or TAPS) AND INSEGMENT #32 (#30 OR #31)
Appendix 3. Database search strategies
In addition to searching the CCMDCTR we ran searches on CENTRAL, Ovid MEDLINE, Embase, and PsycINFO as listed below.
Dates of searches: 21 November 2018 and 10 October 2019.
Cochrane Central Register of Controlled Trials (CENTRAL; issue 10 of 12, 2019) in the Cochrane Library #1 ((infant or infants or child* or adolesc* or pediatric* or paediatric* or teen* or young* or youth or school* or preschool*) and (anxi* or phobi* or panic)):ti
#2 ((infant or infants or child* or adolesc* or pediatric* or paediatric* or teen* or young* or youth or school* or preschool*) near/2 (anxi* or phobi* or panic)):ab
#3 MeSH descriptor: [Anxiety Disorders] this term only #4 MeSH descriptor: [Anxiety] this term only and with qualifier(s): [diagnosis ‐ DI, prevention & control ‐ PC, psychology ‐ PX, therapy ‐ TH]
#5 MeSH descriptor: [Agoraphobia] this term only
#6 MeSH descriptor: [Panic Disorder] this term only
#7 MeSH descriptor: [Anxiety, Separation] this term only
#8 MeSH descriptor: [Phobic Disorders] explode all trees
#9 MeSH descriptor: [Phobia, Social] this term only
#10 (agoraphobi* or "generalized anxiety" or "generalised anxiety" or GAD or "separation anxiety" or (social* NEAR/2 (anxi* or fear*)) or phobi* or mute or mutes or mutism or "school refusal”):ti,ab,kw
#11 panic:ti,ab,kw
#12 (anxiety near (autism or autistic)):ti,ab,kw #13 MeSH descriptor: [Child Development Disorders, Pervasive] explode all trees
#14 anxiety:ti,ab,kw
#15 (#13 and #14)
#16 (#3 OR #4 OR #5 OR #6 OR #7 OR #8 OR #9 OR #10 OR #11 OR #12 OR #15) #17 MeSH descriptor: [Cognitive Therapy] explode all trees
#18 MeSH descriptor: [Psychotherapy, Group] explode all trees
#19 MeSH descriptor: [Bibliotherapy] this term only
#20 MeSH descriptor: [Early Intervention (Education)] this term only
#21 (CBT or CBGT* or bCBT or b‐CBT or GPDCBT or GPD‐CBT):ab
#22 ((cogniti* or behavio*) NEAR/3 (counsel* or intervention or therap* or psychotherap* or training or treatment or technique* or restructur* or defusion)):Ti,AB
#23 ("rational emotive" or (problem* NEAR/2 (focus* or sol*)) or psychoeducat* or psycho‐educat* or "role play" or "role playing" or schema* or self‐control* or "self control" or "self controlling”):ti,ab
#24 (((psychotherap* or therap*) near/3 (commitment or acceptance)) or ((self* or stress*) near/3 (control or analysis or direct* or esteem or help or instruct* or manage*))):ti,ab
#25 ((attribution* or reattribution*) near/3 (therap* or psychotherap*)):ti,ab 20
#26 (mindfulness* or "third wave" or experiential or (behavio* near/3 (activation or modification)) or (thought* near/3 suppress*) or rumination):ti,ab
#27 ((anxiety near/2 manag*) or "confidence building" or "coping skills" or "exposure therapy" or "exposure task" or "exposure tasks" or psychoeducat* or psycho‐educat* or relaxation or "sensitivity training" or "self talk" or (social near/2 (coach* or skill* or effectiveness))):ti,ab
#28 ((controlling or overcoming) near/2 (anxiety or panic or phobi* or agoraphobi* or shyness)):ti,ab
#29 (child* near/2 (deliver* or focus*) near/2 (counsel* or intervention* or program* or psychotherap* or therap* or train* or treat*)):ti,ab
#30 ((parent* or guardian*) near/2 (deliver* or focus*) near/2 (counsel* or intervention* or program* or psychotherap* or therap* or train* or treat*)):ti,ab
#31 ((individual* or group or conjoint or family) next (counsel* or intervention* or program* or psychotherap* or therap* or train* or treat*)):ti,ab,kw
#32 ("Coping Cat" or "Cool Kids" or "Coping Koala" or "Facing your Fears" or (Skills near Academic near "Social Success") or (Intervention near Adolescents near "Social Phobia") or ("Multimodal Anxiety" near "Social Skills") or BIACA or IAFS or MASSI or SASS or TAPS):ti,ab
#33 MeSH descriptor: [Psychotherapy] this term only and with qualifier(s): [methods ‐ MT, standards ‐ ST, statistics & numerical data ‐ SN]
#34 (#17 or #18 or #19 or #20 or #21 or #22 or #23 or #24 or #25 or #26 or #27 or #28 or #29 or #30 or #31 or #32 or #33)
#35 MeSH descriptor: [Adolescent] this term only 97662
#36 MeSH descriptor: [Child] explode all trees 1394
#37 MeSH descriptor: [Infant] this term only
#38 (infant* or child* or adolesc* or paediatr* or pediatr*):kw,so
#39 (infant* or child* or boy* or girl* or kids or juvenil* or minors or paediatric* or pediatric* or adolesc* or preadolesc* or pre‐adolesc* or pubert* or pubescen* or prepube* or pre‐pube* or teen* or (young next (survivor* or offender* or minorit*)) or youth* or schoo* or preschool* or nurser* or kindergarten):ti,kw
#40 (#36 or #37 or #38 or #39 or #40) #41 (#17 and #35) #41 (#16 and #34 and #40) #42 (#1 or #2) and #34
#43 (#41 or #42)
#44 ((OCD or "obsessive compulsive" or PTSD or "posttraumatic stress" or "post‐traumatic stress") not (anxi* or phobi* or agoraphobi* or panic)):ti
#45 (#43 not #44) #46 (ADIS‐C* or ADIS‐P* or DISCAP or SCARED or SCAS or RCADS or RCMAS or MASC or CBCL or STAI‐C or SPAI‐C or SAS‐A):ab #47 (#46 and #34) #48 (#47 not #43) #49 (#48 not #44)
OvidPsycINFO (all years to October Week 40 2019) 1 clinical trials.sh. 2 (randomi#ed or randomi#ation or randomi#ing).ti,ab,id. 3 (RCT or at random or (random* adj3 (administ* or allocat* or assign* or class* or control* or determine* or divide* or division or distribut* or expose* or fashion or number* or place* or recruit* or split or subsitut* or treat*))).ti,ab,id. 4 (control* and (trial or study or group) and (placebo or waitlist* or wait* list* or ((treatment or care) adj2 usual))).ti,ab,id,hw. 5 ((single or double or triple or treble) adj2 (blind* or mask* or dummy)).ti,ab,id. 6 trial.ti. 7 placebo.ti,ab,id,hw. 8 treatment outcome.md. 9 treatment effectiveness evaluation.sh. 10 mental health program evaluation.sh. 11 or/1‐10 12 *anxiety/ 13 anxiety disorders/ or generalized anxiety disorder/ or panic disorder/ or exp phobias/ or separation anxiety disorder/ 14 social anxiety/ 15 school refusal/ or school phobia/ 16 exp separation anxiety/ 17 panic/ or panic attack/ or panic disorder/ 18 mutism/ or elective mutism/ 19 (agoraphobi* or generali#ed anxiety or GAD or separation anxiety or (social* adj2 (anxi* or fear*)) or phobi* or mute? or mutism or school refusal).ti,ab,id. 20 ((infant? or child* or adolesc* or p?ediatric* or teen* or young* or youth or school? or preschool*) adj2 anxi*).ti,ab,id. 21 over anxious.ti,ab,id. 22 anxiety.ab. /freq=3 23 panic.ti,ab,id,hw. 24 (anxiety adj5 (autism or autistic)).ti,ab,id. 25 anxiety.ti,ab,id,tm. and (autism spectrum disorders/ or autistic thinking/ or exp developmental disabilities/) 26 or/12‐25 27 ((anxi* or phobi* or panic) and (effectiveness or efficacy or evaluat* or intervention or program* or train* or treat* or prevent* or therapy or psychotherapy or trial or study) and (infant? or child* or adolesc* or paediatric* or pediatric* or teen* or young* or youth or school? or preschool*)).ti. 28 anxiety management/ 29 exp cognitive behavior therapy/ 30 cognitive techniques/ or cognitive restructuring/ or cognitive therapy/ 31 behavior modification/ 32 exp relaxation therapy/ 33 exp family therapy/ 34 exp group psychotherapy/ or psychodrama/ or role playing/ or role playing games/ 35 bibliotherapy/ 36 counseling/ or group counseling/ or exp psychotherapeutic counseling/ or school counseling/ 37 psychotherapy/ 38 psychotherapeutic techniques/ or mindfulness/ 39 (CBT or CBGT* or bCBT or b‐CBT or GPDCBT or GPD‐CBT).ab. 40 ((cogniti* or behavio*) adj3 (counsel* or intervention or therap* or psychotherap* or training or treatment or technique* or restructur* or defusion)).ti,ab,id. 41 (rational emoti* or (problem* adj2 (focus* or sol*)) or psychoeducat* or role play* or schema* or self‐control* or self control*).ti,ab,id,hw. 42 (((psychotherap* or therap*) adj3 (commitment or acceptance)) or ((self* or stress*) adj3 (control or analysis or direct* or esteem or help or instruct* or manage*))).ti,ab,id. 43 ((attribution* or reattribution*) adj3 (therap* or psychotherap*)).ti,ab,id. 44 (mindfulness* or third wave or experiential or (behavio* adj3 (activation or modification)) or (thought* adj3 suppress*) or rumination).ti,ab,id. 45 ((anxiety adj1 manag*) or confidence building or coping skills or exposure therapy or exposure task* or psychoeducat* or psycho‐educat* or relaxation or sensitivity training or self talk or (social adj2 (coach* or skill* or effectiveness))).ti,ab,id,hw. 46 ((controlling or overcoming) adj2 (anxiety or panic or phobi* or agoraphobi* or shyness)).ti,ab,id. 47 (child* adj2 (centred or centered or deliver* or focus*) adj2 (counsel* or intervention* or program* or psychotherap* or therap* or train* or treat*)).ti,ab,id. 48 ((parent* or guardian*) adj2 (centred or centered or deliver* or focus*) adj2 (counsel* or intervention* or program* or psychotherap* or therap* or train* or treat*)).ti,ab,id. 49 ((individually or group or conjoint or family) adj2 (counsel* or intervention* or program* or psychotherap* or therap* or train* or treat*)).ti,ab,id. 50 (Coping Cat or Cool Kids or Coping Koala or Fac* your Fear? or (Multimodal Anxiety adj Social Skills) or (Skills adj Academic adj Social Success) or (Intervention adj Adolescents adj Social Phobia) or BIACA or IAFS or MASSI or SASS or TAPS).ti,ab,id. 51 or/28‐50 52 pediatrics/ 53 child psychiatry/ or child psychopathology/ or child psychology/ 54 adolescent psychiatry/ or adolescent psychopathology/ or adolescent psychology/ 55 (infant? or child* or adolesc* or paediatr* or pediatr*).hw,jx. 56 (infant* or child* or boy* or girl* or kids or juvenil* or minors or paediatric* or pediatric* or adolesc* or preadolesc* or pre‐adolesc* or pubert* or pubescen* or prepube* or pre‐pube* or teen* or (young adj (survivor* or offender* or minorit*)) or youth* or school? or preschool* or nurser* or kindergarten).ti,id. 57 or/52‐56 58 (ADIS‐C* or ADIS‐P* or DISCAP or SCARED or SCAS or RCADS or RCMAS or MASC or CBCL or STAI‐C or SPAI‐C or SAS‐A).ab,id,tm. 59 11 and 26 and 51 and 57 60 11 and 27 and 51 61 11 and 51 and 58 62 11 and 50 63 59 or 60 or 61 or 62 64 ((OCD or obsessive compulsive or PTSD or posttraumatic stress disorder* or post‐traumatic stress disorder*) not (anxi* or phobi* or agoraphobi* or panic)).ti. 65 63 not 64 Ovid MEDLINE Databases (2016 to 10 Oct 2019) Ovid MEDLINE(R) and Epub Ahead of Print, In‐Process & Other Non‐Indexed Citations and Daily 1 controlled clinical trial.pt. 2 randomized controlled trial.pt.
3 (randomi#ed or randomi#ation or randomi#ing).ti,ab,kf. 4 (RCT or "at random" or (random* adj3 (administ* or allocat* or assign* or class* or cluster or control* or determine* or divide* or division or distribut* or expose* or fashion or number* or place* or pragmatic or quasi or recruit* or split or subsitut* or treat*))).ti,ab,kf. 5 (placebo or ((attention or active) adj control*)).ti,ab,kf. 6 trial.ab,ti,kf. 7 ((control* or group* or compar*) adj5 (((care or treatment*) adj2 (usual or standard or routine)) or TAU or CAU)).ab. 8 ((control* or group* or compar*) adj5 (waitlist* or wait* list* or waiting or WLC)).ab. 9 or/1‐8 10 ANXIETY DISORDERS/ 11 *ANXIETY/di, pc, px, th 12 AGORAPHOBIA/ or PANIC DISORDER/ or ANXIETY, SEPARATION/ 13 PHOBIC DISORDERS/ or PHOBIA, SOCIAL/ 14 (agoraphobi* or generali#ed anxiety or GAD or separation anxiety or (social* adj2 (anxi* or fear*)) or phobi* or mute? or mutism or school refusal).ti,ab,kf. 15 ((infant? or child* or adolesc* or p?ediatric* or teen* or young* or youth or school? or preschool*) adj2 anxi*).ti,ab,kf. 16 anxiety.ab. /freq=3 17 panic.mp. 18 (anxiety adj5 (autism or autistic)).ti,ab,kf. 19 anxiety.mp. and (child development disorders, pervasive/px or autism spectrum disorder/px or autistic disorder/px) 20 or/10‐19 21 ((anxi* or phobi* or panic) and (effectiveness or efficacy or evaluat* or intervention or program* or train* or treat* or prevent* or therapy or psychotherapy or trial or study) and (infant? or child* or adolesc* or paediatric* or pediatric* or teen* or young* or youth or school? or preschool*)).ti. 22 exp COGNITIVE THERAPY/ 23 PSYCHOTHERAPY, GROUP/ 24 FAMILY THERAPY/ or PSYCHODRAMA/ or ROLE PLAYING/ or SENSITIVITY TRAINING GROUPS/ 25 BIBLIOTHERAPY/ 26 "EARLY INTERVENTION (Education)"/ 27 (CBT or CBGT* or bCBT or b‐CBT or GPDCBT or GPD‐CBT).ab. 28 ((cogniti* or behavio*) adj3 (counsel* or intervention or therap* or psychotherap* or training or treatment or technique* or restructur* or defusion)).ti,ab,kf. 29 (rational emoti* or (problem* adj2 (focus* or sol*)) or psychoeducat* or role play* or schema* or self‐control* or self control*).ti,ab,kf. 30 (((psychotherap* or therap*) adj3 (commitment or acceptance)) or ((self* or stress*) adj3 (control or analysis or direct* or esteem or help or instruct* or manage*))).ti,ab,kf. 31 ((attribution* or reattribution*) adj3 (therap* or psychotherap*)).ti,ab,kf. 32 (mindfulness* or third wave or experiential or (behavio* adj3 (activation or modification)) or (thought* adj3 suppress*) or rumination).ti,ab,kf. 33 ((anxiety adj1 manag*) or confidence building or coping skills or exposure therapy or exposure task* or psychoeducat* or psycho‐educat* or relaxation or sensitivity training or self talk or (social adj2 (coach* or skill* or effectiveness))).ti,ab,kf,hw. 34 ((controlling or overcoming) adj2 (anxiety or panic or phobi* or agoraphobi* or shyness)).ti,ab,kf. 35 (child* adj2 (deliver* or focus*) adj2 (counsel* or intervention* or program* or psychotherap* or therap* or train* or treat*)).ti,ab,kf. 36 ((parent* or guardian*) adj2 (deliver* or focus*) adj2 (counsel* or intervention* or program* or psychotherap* or therap* or train* or treat*)).ti,ab,kf. 37 ((individually or group or conjoint or family) adj2 (counsel* or intervention* or program* or psychotherap* or therap* or train* or treat*)).ti,ab,kf. 38 (Coping Cat or Cool Kids or Coping Koala or Fac* your Fear? or (Multimodal Anxiety adj Social Skills) or (Skills adj Academic adj Social Success) or (Intervention adj Adolescents adj Social Phobia) or BIACA or IAFS or MASSI or SASS or TAPS).ti,ab,kf. 39 *PSYCHOTHERAPY/mt, st, sn, tu 40 or/22‐39 41 ADOLESCENT/ or CHILD/ or CHILD, PRESCHOOL/ 42 (infant? or child* or adolesc* or paediatr* or pediatr*).hw,jn. 43 (infant* or child* or boy* or girl* or kids or juvenil* or minors or paediatric* or pediatric* or adolesc* or preadolesc* or pre‐adolesc* or pubert* or pubescen* or prepube* or pre‐pube* or teen* or (young adj (survivor* or offender* or minorit*)) or youth* or school? or preschool* or nurser* or kindergarten).ti,kf. 44 (infant? or child* or adolesc* or paediatr* or pediatr*).ab. /freq=3 45 or/41‐44 46 9 and 20 and 40 and 45 47 9 and 21 and 40 48 46 or 47 49 (ADIS‐C* or ADIS‐P* or DISCAP or SCARED or SCAS or RCADS or RCMAS or MASC or CBCL or STAI‐C or SPAI‐C or SAS‐A).ab. 50 9 and 40 and 49 51 48 or 50 52 ((OCD or obsessive compulsive or PTSD or posttraumatic stress disorder* or post‐traumatic stress disorder*) not (anxi* or phobi* or agoraphobi* or panic)).ti. 53 (2016* or 2017* or 2018*).yr,dp,dt,ep,ez. 54 51 not 52 55 53 and 54
Ovid Embase (2016 to 2019 Week 40) 1 randomized controlled trial/ 2 randomization.de. 3 controlled clinical trial/ and (Disease Management or Drug Therapy or Prevention or Rehabilitation or Therapy).fs. 4 *clinical trial/ 5 placebo.de. 6 placebo.ti,ab. 7 trial.ti. 8 (randomi#ed or randomi#ation or randomi#ing).ti,ab,kw. 9 (RCT or "at random" or (random* adj3 (administ* or allocat* or assign* or class* or control* or determine* or divide* or division or distribut* or expose* or fashion or number* or place* or recruit* or split or subsitut* or treat*))).ti,ab,kw. 10 ((singl$ or doubl$ or trebl$ or tripl$) adj3 (blind$ or mask$ or dummy)).mp. 11 (control* and (trial or study or group) and (placebo or waitlist* or wait* list* or ((treatment or care) adj2 usual))).ti,ab,kw,hw. 12 or/1‐11 13 ((animal or nonhuman) not (human and (animal or nonhuman))).de. 14 12 not 13 15 anxiety disorder/ or anxiety neurosis/ or generalized anxiety disorder/ or "mixed anxiety and depression"/ or panic/ or exp phobia/ or separation anxiety/ 16 *anxiety/ 17 (agoraphobi* or generali#ed anxiety or GAD or separation anxiety or (social* adj2 (anxi* or fear*)) or phobi* or mute? or mutism or school refusal).ti,ab,kw. 18 ((infant? or child* or adolesc* or p?ediatric* or teen* or young* or youth or school? or preschool*) adj2 anxi*).ti,ab,kw. 19 anxiety.ab. /freq=3 20 panic.mp. 21 (anxiety adj5 (autism or autistic)).ti,ab,kw. 22 anxiety.mp. and (autism/ or asperger syndrome/ or "pervasive developmental disorder not otherwise specified"/) 23 school refusal/ 24 mutism/ or selective mutism/ 25 or/15‐24 26 cognitive behavioral therapy/ or cognitive behavioral stress management/ 27 exp cognitive therapy/ 28 psychotherapy/ or bibliotherapy/ or family therapy/ or group therapy/ or mindfulness/ or play therapy/ or psychodrama/ or relaxation training/ or role playing/ 29 (CBT or CBGT* or bCBT or b‐CBT or GPDCBT or GPD‐CBT).ab. 30 ((cogniti* or behavio*) adj3 (counsel* or intervention or therap* or psychotherap* or training or treatment or technique* or restructur* or defusion)).ti,ab,kw. 31 (rational emoti* or (problem* adj2 (focus* or sol*)) or psychoeducat* or role play* or schema* or self‐control* or self control*).ti,ab,kw. 32 *self control/ 33 (((psychotherap* or therap*) adj3 (commitment or acceptance)) or ((self* or stress*) adj3 (control or analysis or direct* or esteem or help or instruct* or manage*))).ti,ab,kw. 34 ((attribution* or reattribution*) adj3 (therap* or psychotherap*)).ti,ab,kw. 35 (mindfulness* or third wave or experiential or (behavio* adj3 (activation or modification)) or (thought* adj3 suppress*) or rumination).ti,ab,kw. 36 ((anxiety adj1 manag*) or confidence building or coping skills or exposure therapy or exposure task* or psychoeducat* or psycho‐educat* or relaxation or sensitivity training or self talk or (social adj2 (coach* or skill* or effectiveness))).ti,ab,kw,hw. 37 ((controlling or overcoming) adj2 (anxiety or panic or phobi* or agoraphobi* or shyness)).ti,ab,kw. 38 (child* adj2 (centred or centered or deliver* or focus*) adj2 (counsel* or intervention* or program* or psychotherap* or therap* or train* or treat*)).ti,ab,kw. 39 ((parent* or guardian*) adj2 (centred or centered or deliver* or focus*) adj2 (counsel* or intervention* or program* or psychotherap* or therap* or train* or treat*)).ti,ab,kw. 40 ((individually or group or conjoint or family) adj2 (counsel* or intervention* or program* or psychotherap* or therap* or train* or treat*)).ti,ab,kw. 41 (Coping Cat or Cool Kids or Coping Koala or Fac* your Fear? or (Multimodal Anxiety adj Social Skills) or (Skills adj Academic adj Social Success) or (Intervention adj Adolescents adj Social Phobia) or BIACA or IAFS or MASSI or SASS or TAPS).ti,ab,kw. 42 or/26‐41 43 juvenile/ or exp adolescent/ or exp child/ 44 (infant? or child* or adolesc* or paediatr* or pediatr*).hw,jx. 45 (infant* or child* or boy* or girl* or kids or juvenil* or minors or paediatric* or pediatric* or adolesc* or preadolesc* or pre‐adolesc* or pubert* or pubescen* or prepube* or pre‐pube* or teen* or (young adj (survivor* or offender* or minorit*)) or youth* or school? or preschool* or nurser* or kindergarten).ti,kw. 46 or/43‐45 47 14 and 25 and 42 and 46 48 ((anxi* or phobi* or panic) and (effectiveness or efficacy or evaluat* or intervention or program* or train* or treat* or prevent* or therapy or psychotherapy or trial or study) and (infant? or child* or adolesc* or paediatric* or pediatric* or teen* or young* or youth or school? or preschool*)).ti. 49 14 and 42 and 48 50 (ADIS‐C* or ADIS‐P* or DISCAP or SCARED or SCAS or RCADS or RCMAS or MASC or CBCL or STAI‐C or SPAI‐C or SAS‐A).ab. 51 14 and 42 and 50 52 47 or 49 or 51 53 ((OCD or obsessive compulsive or PTSD or posttraumatic stress disorder* or post‐traumatic stress disorder*) not (anxi* or phobi* or agoraphobi* or panic)).ti. 54 52 not 53 55 (2016* or 2017* or 2018*).yr,dp,dc. 56 54 and 55
Appendix 4. Grey literature search strategies
We ran the searches listed below on Proquest Dissertations & Theses Global, PQDT Open, Open Access Theses and Dissertations, DART and NDLTD.
Dates of searches: All years to 14 Oct 2019
Proquest Dissertations & Theses Globalsearch.proquest.com/pqdtglobal/dissertations/
ti(adolescent OR adolescents OR teenager OR teenagers OR teen OR teens OR child OR children OR childhood OR kids OR kiddies OR youth OR youths OR young OR pediatric OR paediatric OR school OR schools) AND ti(anxiety OR anxious OR fear OR panic OR phobia OR phobias OR phobic) AND ti(effect OR effects OR effective OR effectiveness OR evaluation OR evaluations OR evaluating OR evaluated OR findings OR intervention OR interventions OR outcome OR outcomes OR prevent OR preventing OR prevention OR program OR programs OR programme OR programmes OR psychotherapy OR psychotherapies OR psychotherapeutic OR results OR study OR studies OR therapy OR therapies OR therapeutic OR treat OR treated OR treating OR treatment OR treatments OR trial OR trials) AND noft(CBT OR cognitive OR behaviour OR behavioural OR behavior OR behavioral) AND noft(RCT OR randomized OR randomised OR randomly OR assignment OR allocation)
PQDT Open ‐ open access dissertations and thesespqdtopen.proquest.com/search.html
ti(anxiety OR anxious OR fear OR panic OR phobia OR phobias OR phobic) AND (RCT OR randomized OR randomised OR randomly)
Open Access Theses and Dissertationsoatd.org
title:(anxiety OR anxious OR fear OR panic OR phobia OR phobias OR phobic) AND title:(adolescent OR adolescents OR teenager OR teenagers OR teen OR teens OR child OR children OR childhood OR kids OR kiddies OR youth OR youths OR young OR pediatric OR paediatric OR school OR schools) AND (RCT OR randomized OR randomised OR randomly)
DART ‐ Europe e‐theses Portalwww.dart-europe.eu/basic-search.php
(anxiety OR anxious OR fear OR panic OR phobia OR phobias OR phobic) AND (RCT OR randomized OR randomised OR randomly) AND (CBT OR cognitive OR behaviour OR behavioural OR behavior OR behavioral) AND (adolescent OR adolescents OR teenager OR teenagers OR teen OR teens OR child OR children OR childhood OR kids OR kiddies OR youth OR youths OR young OR pediatric OR paediatric OR school OR schools)
Networked Digital Library of Theses and Dissertations (NDLTD)search.ndltd.org/
title:(anxiety OR anxious OR fear OR panic OR phobia OR phobias OR phobic) AND title:(adolescent OR adolescents OR teenager OR teenagers OR teen OR teens OR child OR children OR childhood OR kids OR kiddies OR youth OR youths OR young OR pediatric OR paediatric OR school OR schools) AND (RCT OR randomized OR randomised OR randomly)
Electronic Theses Online Service (EThOS) ‐ British Library ethos.bl.uk/Home.do
Recommend searching EThOS via Proquest Dissertations and Theses Global (as listed above).
Data and analyses
Comparison 1. CBT versus waitlist/no treatment.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1.1 Remission of primary anxiety diagnosis post‐treatment (ITT) | 39 | 2697 | Odds Ratio (IV, Random, 95% CI) | 5.45 [3.90, 7.60] |
| 1.1.1 Child focused | 19 | 1184 | Odds Ratio (IV, Random, 95% CI) | 10.42 [5.84, 18.58] |
| 1.1.2 Child and parent | 19 | 1142 | Odds Ratio (IV, Random, 95% CI) | 4.08 [2.72, 6.11] |
| 1.1.3 Parent only | 4 | 371 | Odds Ratio (IV, Random, 95% CI) | 2.83 [1.12, 7.16] |
| 1.2 Subgroup analysis: remission of primary anxiety diagnosis post‐treatment (ITT) (individual vs group) | 39 | Odds Ratio (IV, Random, 95% CI) | Subtotals only | |
| 1.2.1 Individual focused | 17 | 1165 | Odds Ratio (IV, Random, 95% CI) | 4.53 [2.55, 8.03] |
| 1.2.2 Group focused | 25 | 1532 | Odds Ratio (IV, Random, 95% CI) | 6.25 [4.45, 8.78] |
| 1.3 Subgroup analysis: remission of primary anxiety diagnosis post‐treatment (ITT) (amount of therapist contact time) | 39 | Odds Ratio (IV, Random, 95% CI) | Subtotals only | |
| 1.3.1 Therapist contact (< 10 hours) | 6 | 513 | Odds Ratio (IV, Random, 95% CI) | 6.12 [2.08, 18.00] |
| 1.3.2 Therapist contact (≥10 and < 20 hours) | 23 | 1622 | Odds Ratio (IV, Random, 95% CI) | 5.85 [3.95, 8.64] |
| 1.3.3 Therapist contact (≥ 20 hours) | 13 | 562 | Odds Ratio (IV, Random, 95% CI) | 4.44 [2.26, 8.72] |
| 1.4 Subgroup analysis: remission of primary anxiety diagnosis post‐treatment (ITT) (age) | 39 | Odds Ratio (IV, Random, 95% CI) | Subtotals only | |
| 1.4.1 ≤ 12 years | 11 | 789 | Odds Ratio (IV, Random, 95% CI) | 3.93 [2.20, 7.02] |
| 1.4.2 Mixed age range (< 12 and ≥ 12 years) | 21 | 1447 | Odds Ratio (IV, Random, 95% CI) | 6.43 [3.90, 10.58] |
| 1.4.3 ≥ 12 years | 7 | 461 | Odds Ratio (IV, Random, 95% CI) | 5.28 [2.83, 9.86] |
| 1.5 Subgroup analysis: remission of primary anxiety diagnosis post‐treatment (ITT) (ASD vs non‐ASD) | 39 | Odds Ratio (IV, Random, 95% CI) | Subtotals only | |
| 1.5.1 Sample with ASD | 4 | 136 | Odds Ratio (IV, Random, 95% CI) | 1.79 [0.39, 8.16] |
| 1.5.2 Not sample with ASD | 35 | 2561 | Odds Ratio (IV, Random, 95% CI) | 5.88 [4.19, 8.24] |
| 1.6 Remission of primary anxiety diagnosis post‐treatment (completers) | 38 | 2406 | Odds Ratio (IV, Random, 95% CI) | 11.55 [8.41, 15.86] |
| 1.7 Acceptability (number of participants lost to post‐treatment assessment) | 45 | 3158 | Odds Ratio (IV, Random, 95% CI) | 1.09 [0.85, 1.41] |
| 1.8 Remission of all anxiety diagnoses post‐treatment (ITT) | 28 | 2075 | Odds Ratio (IV, Random, 95% CI) | 4.43 [2.89, 6.78] |
| 1.8.1 Child focused | 11 | 564 | Odds Ratio (IV, Random, 95% CI) | 8.52 [2.97, 24.39] |
| 1.8.2 Child and parent | 15 | 916 | Odds Ratio (IV, Random, 95% CI) | 5.19 [3.26, 8.27] |
| 1.8.3 Parent only | 7 | 595 | Odds Ratio (IV, Random, 95% CI) | 1.89 [0.98, 3.65] |
| 1.9 Subgroup analysis: remission of all anxiety diagnoses post‐treatment (ITT) (individual vs group) | 28 | Odds Ratio (IV, Random, 95% CI) | Subtotals only | |
| 1.9.1 Individual focused | 9 | 671 | Odds Ratio (IV, Random, 95% CI) | 3.72 [1.70, 8.12] |
| 1.9.2 Group focused | 20 | 1404 | Odds Ratio (IV, Random, 95% CI) | 4.92 [2.95, 8.20] |
| 1.10 Subgroup analysis: remission of all anxiety diagnoses post‐treatment (ITT) (amount of therapist contact time) | 28 | Odds Ratio (IV, Random, 95% CI) | Subtotals only | |
| 1.10.1 Therapist contact (< 10 hours) | 5 | 461 | Odds Ratio (IV, Random, 95% CI) | 1.42 [0.68, 2.96] |
| 1.10.2 Therapist contact (≥ 10 and < 20 hours) | 17 | 1123 | Odds Ratio (IV, Random, 95% CI) | 6.59 [3.62, 12.01] |
| 1.10.3 Therapist contact (≥ 20 hours) | 9 | 491 | Odds Ratio (IV, Random, 95% CI) | 5.03 [2.55, 9.93] |
| 1.11 Subgroup analysis: remission of all anxiety diagnoses post‐treatment (ITT) (age) | 28 | Odds Ratio (IV, Random, 95% CI) | Subtotals only | |
| 1.11.1 ≤ 12 years | 10 | 950 | Odds Ratio (IV, Random, 95% CI) | 3.59 [1.97, 6.56] |
| 1.11.2 Mixed age range (< 12 years and ≥ 12 years) | 15 | 980 | Odds Ratio (IV, Random, 95% CI) | 4.87 [2.58, 9.21] |
| 1.11.3 ≥ 12 years | 3 | 145 | Odds Ratio (IV, Random, 95% CI) | 8.48 [0.79, 91.08] |
| 1.12 Remission of all anxiety diagnoses post‐treatment (completers) | 27 | 1871 | Odds Ratio (IV, Random, 95% CI) | 9.13 [5.78, 14.41] |
| 1.13 Reduction in anxiety symptoms (child report) post‐treatment | 45 | 2831 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.67 [‐0.88, ‐0.47] |
| 1.13.1 Child focused | 24 | 1239 | Std. Mean Difference (IV, Random, 95% CI) | ‐1.04 [‐1.41, ‐0.67] |
| 1.13.2 Child and parent | 20 | 1285 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.45 [‐0.67, ‐0.23] |
| 1.13.3 Parent only | 5 | 307 | Std. Mean Difference (IV, Random, 95% CI) | 0.04 [‐0.38, 0.46] |
| 1.14 Sensitivity analysis: reduction in anxiety symptoms (child report) post‐treatment (broad anxiety measures) | 38 | 2459 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.41 [‐0.57, ‐0.25] |
| 1.15 Subgroup analysis: reduction in anxiety symptoms (child report) post‐treatment (individual vs group) | 45 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 1.15.1 Individual focused | 21 | 1203 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.39 [‐0.64, ‐0.15] |
| 1.15.2 Group focused | 27 | 1628 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.91 [‐1.22, ‐0.60] |
| 1.16 Subgroup analysis: reduction in anxiety symptoms (child report) post‐treatment (amount of therapist contact time) | 45 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 1.16.1 Therapist contact (< 10 hours) | 9 | 587 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.36 [‐0.75, 0.03] |
| 1.16.2 Therapist contact (≥ 10 and < 20 hours) | 29 | 1840 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.81 [‐1.09, ‐0.52] |
| 1.16.3 Therapist contact (≥ 20 hours) | 10 | 404 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.62 [‐1.06, ‐0.18] |
| 1.17 Subgroup analysis: reduction in anxiety symptoms (child report) post‐treatment (age) | 45 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 1.17.1 ≤ 12 years | 11 | 663 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.23 [‐0.54, 0.08] |
| 1.17.2 Mixed age range (< 12 years and ≥ 12 years) | 28 | 1834 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.62 [‐0.83, ‐0.41] |
| 1.17.3 ≥ 12 years | 6 | 334 | Std. Mean Difference (IV, Random, 95% CI) | ‐1.78 [‐3.01, ‐0.56] |
| 1.18 Subgroup analysis: reduction in anxiety symptoms (child report) post‐treatment (ASD vs non‐ASD) | 45 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 1.18.1 Sample with ASD | 5 | 181 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.61 [‐1.54, 0.33] |
| 1.18.2 Not sample with ASD | 40 | 2650 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.68 [‐0.90, ‐0.47] |
| 1.19 Reduction in anxiety symptoms (parent report) post‐treatment | 35 | 2137 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.70 [‐0.90, ‐0.51] |
| 1.19.1 Child focused | 13 | 734 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.87 [‐1.21, ‐0.53] |
| 1.19.2 Child and parent | 17 | 1031 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.69 [‐0.98, ‐0.39] |
| 1.19.3 Parent only | 5 | 372 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.37 [‐0.77, 0.04] |
| 1.20 Sensitivity analysis: reduction in anxiety symptoms (parent report) post‐treatment (broad anxiety measures only) | 32 | 1952 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.59 [‐0.77, ‐0.41] |
| 1.21 Subgroup analysis: reduction in anxiety symptoms (parent report) post‐treatment (individual vs group) | 35 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 1.21.1 Individual focused | 17 | 858 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.43 [‐0.65, ‐0.21] |
| 1.21.2 Group focused | 21 | 1279 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.92 [‐1.21, ‐0.62] |
| 1.22 Subgroup analysis: reduction in anxiety symptoms (parent report) post‐treatment (amount of therapist contact time) | 35 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 1.22.1 Therapist contact (< 10 hours) | 4 | 336 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.36 [‐0.81, 0.10] |
| 1.22.2 Therapist contact (≥ 10 and < 20 hours) | 22 | 1402 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.66 [‐0.89, ‐0.43] |
| 1.22.3 Therapist contact (≥ 20 hours) | 10 | 399 | Std. Mean Difference (IV, Random, 95% CI) | ‐1.03 [‐1.55, ‐0.52] |
| 1.23 Subgroup analysis: reduction in anxiety symptoms (parent report) post‐treatment (age) | 35 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 1.23.1 ≤ 12 years | 11 | 750 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.40 [‐0.63, ‐0.17] |
| 1.23.2 Mixed age range (< 12 years and ≥ 12 years) | 18 | 1057 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.76 [‐1.04, ‐0.49] |
| 1.23.3 ≥ 12 years | 6 | 330 | Std. Mean Difference (IV, Random, 95% CI) | ‐1.07 [‐1.78, ‐0.37] |
| 1.24 Subgroup analysis: reduction in anxiety symptoms (parent report) post‐treatment (ASD vs non‐ASD) | 35 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 1.24.1 Sample with ASD | 7 | 244 | Std. Mean Difference (IV, Random, 95% CI) | ‐1.12 [‐1.91, ‐0.34] |
| 1.24.2 Not sample with ASD | 28 | 1893 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.63 [‐0.82, ‐0.44] |
| 1.25 Reduction in depressive symptoms post‐treatment | 17 | 1157 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.34 [‐0.51, ‐0.17] |
| 1.26 Improvement in global functioning post‐treatment | 11 | 557 | Std. Mean Difference (IV, Random, 95% CI) | 1.03 [0.68, 1.38] |
| 1.27 Remission of primary anxiety diagnosis at follow‐up (ITT) | 5 | Odds Ratio (IV, Random, 95% CI) | Subtotals only | |
| 1.27.1 Follow‐up (≤ 6 months) | 4 | 153 | Odds Ratio (IV, Random, 95% CI) | 10.94 [2.33, 51.41] |
| 1.27.2 Follow‐up (> 6 and ≤ 12 months) | 3 | 166 | Odds Ratio (IV, Random, 95% CI) | 2.80 [0.24, 33.19] |
| 1.28 Remission of primary anxiety diagnosis at follow‐up (completers) | 5 | Odds Ratio (IV, Random, 95% CI) | Subtotals only | |
| 1.28.1 Follow‐up (≤ 6 months) | 4 | 151 | Odds Ratio (IV, Random, 95% CI) | 11.46 [2.40, 54.67] |
| 1.28.2 Follow‐up (> 6 and ≤ 12 months) | 3 | 161 | Odds Ratio (IV, Random, 95% CI) | 4.04 [0.77, 21.20] |
| 1.29 Remission of all anxiety diagnoses at follow‐up (ITT) | 5 | Odds Ratio (IV, Random, 95% CI) | Subtotals only | |
| 1.29.1 Follow‐up (≤ 6 months) | 3 | 130 | Odds Ratio (IV, Random, 95% CI) | 8.25 [0.69, 98.10] |
| 1.29.2 Follow‐up (> 6 and ≤ 12 months) | 3 | 166 | Odds Ratio (IV, Random, 95% CI) | 3.75 [0.25, 56.88] |
| 1.29.3 Follow‐up (> 12 months) | 2 | 131 | Odds Ratio (IV, Random, 95% CI) | 0.48 [0.17, 1.38] |
| 1.30 Remission of all anxiety diagnoses at follow‐up (completers) | 5 | Odds Ratio (IV, Random, 95% CI) | Subtotals only | |
| 1.30.1 Follow‐up (≤ 6 months) | 3 | 128 | Odds Ratio (IV, Random, 95% CI) | 8.68 [0.72, 104.46] |
| 1.30.2 Follow‐up (> 6 and ≤ 12 months) | 3 | 161 | Odds Ratio (IV, Random, 95% CI) | 5.01 [0.70, 35.87] |
| 1.30.3 Follow‐up (> 12 months) | 2 | 114 | Odds Ratio (IV, Random, 95% CI) | 1.25 [0.36, 4.34] |
| 1.31 Reduction in anxiety symptoms (child report) at follow‐up | 5 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 1.31.1 Follow‐up (≤ 6 months) | 5 | 179 | Std. Mean Difference (IV, Random, 95% CI) | ‐1.92 [‐2.95, ‐0.89] |
| 1.32 Sensitivity analysis: remission of primary anxiety diagnosis post‐treatment (ITT) (only studies where sequence generation is clear) | 20 | 1476 | Odds Ratio (IV, Random, 95% CI) | 4.84 [3.03, 7.73] |
| 1.33 Sensitivity analysis: remission of primary anxiety diagnosis post‐treatment (ITT) (only studies where blind assessors used) | 31 | 2037 | Odds Ratio (IV, Random, 95% CI) | 5.54 [3.76, 8.18] |
Comparison 2. CBT versus treatment as usual.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 2.1 Remission of primary anxiety diagnosis post‐treatment (ITT) | 8 | 487 | Odds Ratio (IV, Random, 95% CI) | 3.19 [0.90, 11.29] |
| 2.1.1 Child focused | 3 | 315 | Odds Ratio (IV, Random, 95% CI) | 0.61 [0.18, 2.01] |
| 2.1.2 Child and parent | 5 | 172 | Odds Ratio (IV, Random, 95% CI) | 8.56 [3.10, 23.66] |
| 2.2 Subgroup analysis: remission of primary anxiety diagnosis post‐treatment (ITT) (ASD vs non‐ASD) | 8 | Odds Ratio (IV, Random, 95% CI) | Subtotals only | |
| 2.2.1 Sample with ASD | 4 | 142 | Odds Ratio (IV, Random, 95% CI) | 11.25 [3.11, 40.79] |
| 2.2.2 Not sample with ASD | 4 | 345 | Odds Ratio (IV, Random, 95% CI) | 1.14 [0.29, 4.47] |
| 2.3 Remission of primary anxiety diagnosis post‐treatment (completers) | 8 | 440 | Odds Ratio (IV, Random, 95% CI) | 4.87 [1.51, 15.72] |
| 2.4 Acceptability (number of participants lost to post‐treatment assessment) | 8 | 441 | Odds Ratio (IV, Random, 95% CI) | 1.37 [0.73, 2.56] |
| 2.5 Remission of all anxiety diagnoses post‐treatment (ITT) | 5 | 203 | Odds Ratio (IV, Random, 95% CI) | 2.74 [1.16, 6.46] |
| 2.6 Remission of all anxiety diagnoses post‐treatment (completers) | 5 | 201 | Odds Ratio (IV, Random, 95% CI) | 2.78 [1.18, 6.55] |
| 2.7 Reduction in anxiety symptoms (child report) post‐treatment | 6 | 214 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.15 [‐0.78, 0.48] |
| 2.8 Sensitivity analysis: reduction in anxiety symptoms (child report) post‐treatment (broad anxiety measures only) | 5 | 187 | Std. Mean Difference (IV, Random, 95% CI) | 0.07 [‐0.54, 0.68] |
| 2.9 Reduction in anxiety symptoms (parent report) post‐treatment | 7 | 228 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.32 [‐0.70, 0.06] |
| 2.10 Sensitivity analysis: reduction in anxiety symptoms (parent report) post‐treatment (broad anxiety measures only) | 6 | 202 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.16 [‐0.44, 0.11] |
Comparison 3. CBT versus attention control.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 3.1 Remission of primary anxiety diagnosis post‐treatment (ITT) | 10 | 822 | Odds Ratio (IV, Random, 95% CI) | 2.28 [1.33, 3.89] |
| 3.1.1 Child focused | 7 | 509 | Odds Ratio (IV, Random, 95% CI) | 3.58 [1.92, 6.65] |
| 3.1.2 Child and parent | 4 | 313 | Odds Ratio (IV, Random, 95% CI) | 1.12 [0.65, 1.92] |
| 3.2 Subgroup analysis: remission of primary anxiety diagnosis post‐treatment (ITT) (individual vs group) | 10 | Odds Ratio (IV, Random, 95% CI) | Subtotals only | |
| 3.2.1 Individual focused | 5 | 469 | Odds Ratio (IV, Random, 95% CI) | 2.04 [1.06, 3.91] |
| 3.2.2 Group focused | 5 | 353 | Odds Ratio (IV, Random, 95% CI) | 3.10 [1.14, 8.45] |
| 3.3 Remission of primary anxiety diagnosis post‐treatment (completers) | 10 | 752 | Odds Ratio (IV, Random, 95% CI) | 3.88 [2.52, 5.97] |
| 3.4 Acceptability (number of participants lost to post‐treatment assessment) | 12 | 797 | Odds Ratio (IV, Random, 95% CI) | 1.00 [0.68, 1.49] |
| 3.5 Remission of all anxiety diagnoses post‐treatment (ITT) | 5 | 378 | Odds Ratio (IV, Random, 95% CI) | 2.75 [1.22, 6.17] |
| 3.6 Remission of all anxiety diagnoses post‐treatment (completers) | 5 | 359 | Odds Ratio (IV, Random, 95% CI) | 3.88 [1.58, 9.51] |
| 3.7 Reduction in anxiety symptoms (child report) post‐treatment | 15 | 978 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.31 [‐0.51, ‐0.11] |
| 3.8 Sensitivity analysis: reduction in anxiety symptoms (child report) post‐treatment (broad anxiety measures only) | 11 | 685 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.18 [‐0.34, ‐0.02] |
| 3.9 Reduction in anxiety symptoms (parent report) post‐treatment | 8 | 638 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.25 [‐0.61, 0.11] |
| 3.10 Sensitivity analysis: reduction in anxiety symptoms (parent report) post‐treatment (broad anxiety measures only) | 4 | 345 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.04 [‐0.26, 0.18] |
| 3.11 Reduction in depressive symptoms post‐treatment | 10 | 613 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.18 [‐0.45, 0.09] |
| 3.12 Remission of primary anxiety diagnosis at follow‐up (ITT) | 4 | Odds Ratio (IV, Random, 95% CI) | Subtotals only | |
| 3.12.1 Follow‐up (≤ 6 months) | 4 | 341 | Odds Ratio (IV, Random, 95% CI) | 3.06 [1.22, 7.65] |
| 3.13 Remission of primary anxiety diagnosis at follow‐up (completers) | 4 | Odds Ratio (IV, Random, 95% CI) | Subtotals only | |
| 3.13.1 Follow‐up (≤ 6 months) | 4 | 302 | Odds Ratio (IV, Random, 95% CI) | 6.52 [2.58, 16.43] |
| 3.14 Remission of all anxiety diagnoses at follow‐up (ITT) | 3 | Odds Ratio (IV, Random, 95% CI) | Subtotals only | |
| 3.14.1 Follow‐up (≤ 6 months) | 3 | 205 | Odds Ratio (IV, Random, 95% CI) | 5.44 [1.00, 29.60] |
| 3.15 Remission of all anxiety diagnoses at follow‐up (completers) | 3 | Odds Ratio (IV, Random, 95% CI) | Subtotals only | |
| 3.15.1 Follow‐up (≤ 6 months) | 3 | 182 | Odds Ratio (IV, Random, 95% CI) | 11.19 [1.94, 64.51] |
| 3.16 Reduction in anxiety symptoms (child report) at follow‐up | 6 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 3.16.1 Follow‐up (≤ 6 months) | 6 | 434 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.44 [‐0.79, ‐0.08] |
| 3.17 Reduction in anxiety symptoms (parent report) at follow‐up | 6 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 3.17.1 Follow‐up (≤ 6 months) | 6 | 434 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.63 [‐1.33, 0.08] |
Comparison 4. CBT versus alternative treatment.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 4.1 Acceptability (number of participants lost to post‐treatment assessment) | 7 | 515 | Odds Ratio (IV, Random, 95% CI) | 1.58 [0.61, 4.13] |
| 4.2 Remission of all anxiety diagnoses post‐treatment (ITT) | 4 | 401 | Odds Ratio (IV, Random, 95% CI) | 0.89 [0.35, 2.23] |
| 4.3 Remission of all anxiety diagnoses post‐treatment (completers) | 4 | 348 | Odds Ratio (IV, Random, 95% CI) | 1.52 [0.70, 3.27] |
| 4.4 Reduction in anxiety symptoms (child report) post‐treatment | 6 | 399 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.09 [‐0.40, 0.21] |
| 4.5 Sensitivity analysis: reduction in anxiety symptoms (child report) post‐treatment (broad anxiety measures only) | 5 | 378 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.00 [‐0.21, 0.20] |
| 4.6 Reduction in anxiety symptoms (parent report) post‐treatment | 6 | 423 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.13 [‐0.33, 0.06] |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Afshari 2014.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: 10‐ to 12‐week treatment, 3‐month follow‐up Number of study centres and location: 1, Iran Study setting: private clinic Date of study: October 2011 to August 2012 |
|
| Participants |
N = 34 (CBT: N = 12; CBT (emotion‐focused): N = 12; no treatment control: N = 10) Mean age (SD): 10.57 (2.27) Age range: 9 to 13 years Inclusion criteria: separation anxiety disorder diagnosis (based on the ADIS‐C/P), not receiving medication or stopped using drugs for at least 1 month before pretest Exclusion criteria: IQ < 80, learning disorders, psychosis, serious mental or physical problems, low interest in continuing the study |
|
| Interventions |
CBT Intervention: Coping Cat Concomitant/excluded medications: no medication or stopped for at least 1 month before pretest Delivery format: child‐only sessions, does not specify if parent sessions included; group format Therapist contact time: 10 hours (10 x 1 hour) Who delivers the intervention: advanced PhD students in psychology CBT (emotion‐focused) Intervention: emotion‐focused CBT (ECBT) (Suveg 2006) Concomitant/excluded medications: no medication or stopped for at least 1 month before pretest Delivery format: child‐only sessions, and 2 parent sessions; group format Therapist contact time: 12 hours (child: 10 x 1; parent: 2 x 1) Who delivers the intervention: advanced PhD students in psychology Wait list/no treatment Intervention: no treatment Concomitant/excluded medications: no medication or stopped for at least 1 month before pretest |
|
| Outcomes |
Reduction in anxiety symptoms (child report) post‐treatment and 3‐month follow‐up: SCARED‐C Reduction in anxiety symptoms (parent report) post‐treatment and 3‐month follow‐up: SCARED‐P |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement Comment: No detail given |
| Allocation concealment (selection bias) | Unclear risk | Judgement Comment: No detail given |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: No detail given but child/parent report questionnaires only |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Judgement Comment: Reason for missing outcome data (low interest in attending sessions) likely to be related to outcome |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes for each measure reported |
| Other source of bias ‐ Therapy integrity | Unclear risk | Judgement Comment: Therapists PhD students. No detail on any attempt to maintain or measure therapy integrity |
| Other bias | Unclear risk | Judgement Comment: Timings for post‐treatment assessment not detailed. Treatment period different for 2 treatment groups |
Arendt 2016.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: non‐controlled 3‐month and 12‐month follow‐up Number of study centres and location: 1, in Denmark Study setting: university research clinic Date of study: October 2011 to August 2012 |
|
| Participants |
N = 109 (CBT: N = 56; waitlist: N = 53) Mean age (SD): 11.78 (2.74) Age range: 7 to 16 Gender: 62 (57%) female Inclusion criteria: primary anxiety disorder diagnosis (based on the ADIS‐C/P) Exclusion criteria: psychosis, untreated attention deficit hyperactivity disorder (ADHD), intellectual disability, and severe behaviour disorders Notes: funded by TrygFonden (grant ID n10691). Authors declare no competing interests |
|
| Interventions |
CBT Intervention: Cool Kids Concomitant/excluded medications: encouraged not to change medication during treatment period Delivery format: child and parent sessions; group Therapist contact time: 20 hours (10 x 2 hours), plus 1‐hour booster Who delivers the intervention: psychologists, plus graduate psychologists as assistants Waitlist/no treatment Intervention: 3‐month waitlist Concomitant/excluded medications: encouraged not to change medication during treatment period |
|
| Outcomes |
Remission of primary anxiety diagnosis post‐treatment: ADIS‐C/P Remission of all anxiety disorder diagnoses post‐treatment: ADIS‐C/P Reduction in anxiety symptoms (child report) post‐treatment: SCAS‐C Reduction in anxiety symptoms (parent report) post‐treatment: SCAS‐P (mother report) Reduction in depressive symptoms post‐treatment: SMFQ‐C |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Judgement Comment: Block randomisation, computer‐generated list. Good detail |
| Allocation concealment (selection bias) | Low risk | Judgement Comment: Sequence list and allocation concealed from researchers and therapists until start of treatment |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: ADIS assessors blind to group and prior diagnosis |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: Missing data reported in consort and have been imputed using appropriate methods. Small amount of missing data |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes for planned measures all reported, and where collected and not reported acknowledged |
| Other source of bias ‐ Therapy integrity | Unclear risk | Judgement Comment: Therapists trained and supervised. No assessment of adherence |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Barrett 1996.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: non‐controlled 6‐month, 12‐month, and 6‐year follow‐up Number of study centres and location: 1, in Australia Study setting: university research clinic |
|
| Participants |
N = 85 (CBT‐child: N = 31; CBT‐family: N = 27; waitlist: N = 27) Mean age (SD): CBT‐child: 9.7 (2.5); CBT‐family: 10.1 (1.9); waitlist: 8.2 (1.9) Age range: 7 to 14 Gender: 34 (43%) female Inclusion criteria: principal diagnosis of overanxious disorder, separation anxiety disorder, or social phobia (based on ADIS‐C/P) Exclusion criteria: intellectual or physical disabilities, anti‐anxiety or depression medication, parents involved in acute marital breakdown |
|
| Interventions |
CBT‐ child Intervention: Coping Koala (adaptation of Coping Cat) Concomitant/excluded medications: anti‐anxiety and depression medication excluded Delivery format: child‐only sessions; individual Therapist contact time: 12 to 16 hours (12 x 60 to 80 minutes) Who delivers the intervention: registered clinical psychologists CBT‐ family Intervention: Coping Koala (adaptation of Coping Cat), plus Family Anxiety Management (FAM) Concomitant/excluded medications: anti‐anxiety and depression medication excluded Delivery format: child‐only sessions, and parent and child sessions (FAM); individual Therapist contact time: 12 to 16 hours (12 x 60 to 80 minutes) Who delivers the intervention: registered clinical psychologists Waitlist/no treatment Intervention: 12‐week waitlist Concomitant/excluded medications: anti‐anxiety and depression medication excluded |
|
| Outcomes |
Remission of all anxiety disorder diagnoses post‐treatment: ADIS‐C/P Reduction in anxiety symptoms (child report) post‐treatment: RCMAS Reduction in depressive symptoms post‐treatment: CDI |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement Comment: Lacks details; randomisation to treatment groups/therapists unclear and refers to "alternating" |
| Allocation concealment (selection bias) | Unclear risk | Judgement Comment: No detail given |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Blinded assessors |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Judgement Comment: Dropouts reported, but number randomised vs completers not clear and not reported for individual measures |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes for all measures reported |
| Other source of bias ‐ Therapy integrity | Low risk | Judgement Comment: Protocol adherence assessed and confirmed for 60% sessions by blind clinician |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Barrett 1998.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: non‐controlled 12‐month follow‐up Number of study centres and location: 1, in Australia Study setting: clinic |
|
| Participants |
N = 60 (CBT‐child: N = 23; CBT‐family: N = 17; waitlist: N = 20) Age range: 7 to 14 Gender: 28 (46.7%) female Inclusion criteria: principal diagnosis of overanxious disorder, separation anxiety disorder, or social phobia (based on ADIS‐C/P) Exclusion criteria: principal diagnosis of simple phobia, intellectual or physical disabilities, currently taking anti‐anxiety or depression medication, parents involved in acute marital breakdown |
|
| Interventions |
CBT‐ child Intervention: Coping Koala (adaptation of Coping Cat) Concomitant/excluded medications: anti‐anxiety and depression medication excluded Delivery format: child‐only sessions; group Therapist contact time: 24 hours (12 x 2 hours) Who delivers the intervention: registered clinical psychologists CBT‐ family Intervention: Coping Koala (adaptation of Coping Cat) and Group Family Anxiety Management Concomitant/excluded medications: anti‐anxiety and depression medication excluded Delivery format: child and parent sessions; group Therapist contact time: 24 hours (12 x 2 hours) Who delivers the intervention: registered clinical psychologists Waitlist/no treatment Intervention: 12‐week waitlist Concomitant/excluded medications: anti‐anxiety and depression medication excluded |
|
| Outcomes | Remission of all anxiety disorder diagnoses post‐treatment: ADIS‐C/P | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement Comment: No detail given. Refers to matching across conditions but does not detail procedure |
| Allocation concealment (selection bias) | Unclear risk | Judgement Comment: No detail given |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Blind assessors |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Judgement Comment: Insufficient detail on completers vs number randomised for each measure or how missing data were managed |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Reported outcomes for all measures |
| Other source of bias ‐ Therapy integrity | Low risk | Judgement Comment: Blind clinician assessed therapy integrity of random sessions; trained therapists delivered treatment |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Barrington 2005.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: 12‐month follow‐up Number of study centres and location: Australia Study setting: clinic |
|
| Participants |
N = 54 (CBT: N = 28; TAU: N = 26) Mean age (SD): CBT: 9.8 (2.29); TAU: 10.2 (1.75) Age range: 7 to 14 Gender: 35 (64.8%) female Inclusion criteria: referrals with predominantly anxiety‐related problems (100% primary anxiety disorder diagnosis, based on ADIS‐C/P, parent and child interviewed together) Exclusion criteria: predominant high levels of aggressive behaviour, intellectual disability, focus of court procedures, exposed to recent trauma |
|
| Interventions |
CBT Intervention: based on CBT guidelines and CBT toolkit Delivery format: child‐only sessions and parent‐only/child and parent together sessions; individual Therapist contact time: 12 hours (approximate) Who delivers the intervention: experienced therapists, masters/doctoral level, CBT trained TAU Intervention: variety of treatment modalities, including family therapy, play therapy, supportive psychotherapy, psychodynamic psychotherapy, non‐CBT eclectic approaches Delivery format: child‐only sessions and parent‐only/child and parent together sessions; individual Therapist contact time: 12 hours (approximate) Who delivers the intervention: experienced therapists, masters/doctoral level, CBT trained |
|
| Outcomes |
Remission of all anxiety disorder diagnoses post‐treatment, 6‐month follow‐up and 12‐month follow‐up: ADIS‐C/P (child and parent interviewed together) Reduction in anxiety symptoms (child report) post‐treatment, 6‐month follow‐up and 12‐month follow‐up: RCMAS Reduction in anxiety symptoms (parent report) post‐treatment, 6‐month follow‐up and 12‐month follow‐up: SCAS‐P |
|
| Notes | Number randomised not clear in paper. Report SCAS‐C z score, so prioritise RCMAS | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement Comment: No detail given |
| Allocation concealment (selection bias) | Unclear risk | Judgement Comment: No detail given |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Judgement Comment: No detail given about whether participants were blinded to condition |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Assessor blind to treatment condition and therapist |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Judgement Comment: Missing data for questionnaires detailed, but number randomised vs completers not clear |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes reported for all measures |
| Other source of bias ‐ Therapy integrity | Low risk | Judgement Comment: Adherence monitored and independently assessed |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Berge 2017.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: non‐controlled 12‐month follow‐up Number of study centres and location: 1, in Norway Study setting: odontophobia clinic Date of study: 2013 to 2016 |
|
| Participants |
N = 67 (CBT: N = 34; waitlist: N = 33) Mean age (SD): 12.2 (2.0) Age range: 10 to 16 Gender: 39 (58.2%) female Inclusion criteria: 10 to 16 years, primary diagnosis of intra‐oral injection phobia (I‐OIP) (DSM‐5 criteria, using modified ADIS), other phobias as either secondary diagnoses or co‐primary diagnoses with I‐OIP allowed, willingness to try exposure treatment; willingness to participate in the study for a period of 1 year Exclusion criteria: primary depression, drug or alcohol abuse, intellectual disabilities, psychotic symptoms |
|
| Interventions |
CBT Intervention: One Session Treatment (OST), modified for 5 sessions Concomitant/excluded medications: no detail given Delivery format: child only; individual Therapist contact time: 5 hours (5 x 1 hour) Who delivers the intervention: dentists, trained and accredited in OST Waitlist/no treatment Intervention: 5‐week waitlist Concomitant/excluded medications: no detail given |
|
| Outcomes | Reduction in anxiety symptoms (child report) post‐treatment: Intra Oral Injection Fear Scale (IOIF‐s) | |
| Notes | Anxiety symptoms measure ‐ measure of intra‐oral injection fears | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Judgement Comment: Computer‐generated random number |
| Allocation concealment (selection bias) | Low risk | Judgement Comment: Opaque and sealed envelopes were put in order according to the randomisation |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Outcome assessment questionnaires only |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: Dropouts detailed, and where reasons known this information was provided; missing data for each measure reported |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes for all measures reported |
| Other source of bias ‐ Therapy integrity | Unclear risk | Judgement Comment: Dentists trained and accredited in the OST delivered intervention, but no detail provided on adherence |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Cartwright Hatton 2011.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: 12‐month follow‐up Number of study centres and location: 1, in the UK Study setting: research hospital Date of study: recruitment January 2006 to January 2008 Withdrawals: 1 family randomised to treatment group withdrawn |
|
| Participants |
N = 74 randomised (CBT: N = 38; waitlist: N = 36); NB: N = 70 met diagnostic criteria for an anxiety disorder and included here Mean age: 6.6 years (n = 74) Age range: 2.7 to 9 years (n = 74) Gender: 42 (56.8%) (n = 74) Inclusion criteria: ≥ cut‐off on CBCL Internalising Scale or Preschool Behaviour Checklist Internalising Scale and likely to have an anxiety disorder (NB: only those who met diagnostic criteria for an anxiety disorder based on ADIS‐P are included here) Exclusion criteria: parent/child had moderate‐to‐severe learning difficulties; child had moderate‐to‐severe autistic spectrum disorder |
|
| Interventions |
CBT Intervention: Timid Tiger Concomitant/excluded medications: Delivery format: parent only; group Therapist contact time: 20 hours (10 x 2 hours) Who delivers the intervention: clinical psychologist Waitlist/no treatment Intervention: 10‐week waitlist |
|
| Outcomes |
Remission of primary anxiety disorder diagnosis post‐treatment and 12‐month follow‐up: ADIS‐P Remission of all anxiety disorder diagnoses post‐treatment and 12‐month follow‐up: ADIS‐P |
|
| Notes | Symptom measures ‐ data not available for those who met diagnostic criteria for an anxiety disorder at baseline (N = 70) | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Judgement Comment: Minimisation with random element using 3 factors; planned 1:1 ratio |
| Allocation concealment (selection bias) | Low risk | Judgement Comment: Telephone, with concealed allocation by independent agency |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Assessors blind to group allocation |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: Missing outcome data balanced in numbers across intervention groups, and where possible imputed with appropriate method |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes for all measures reported (with the exception of teacher reports, which is justified) |
| Other source of bias ‐ Therapy integrity | Low risk | Judgement Comment: Therapist qualifications evidenced, and therapy adherence detailed |
| Other bias | Unclear risk | Judgement Comment: Long‐term follow‐up data: 38% controls reported to have received additional intervention vs 7% in the CBT group |
Chalfant 2007.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: treatment period 5.5 months Number of study centres and location: 1, in Australia Study setting: clinic |
|
| Participants |
N = 51 (CBT: N = 32; waitlist: N = 19) Mean age: 10.8 (1.35) (n = 47) Age range: 8 to 13 Gender: 12 (25.5%) (n = 47) Inclusion criteria: documentation of diagnosis of high functioning autistic disorder or Asperger's disorder. Received primary anxiety disorder diagnosis (based on ADIS‐C/P) Exclusion criteria: intellectual delay, physical disability, currently taking anti‐anxiety or anti‐depressant medication, presented with marked externalising difficulties (e.g. conduct disorder or oppositional defiant disorder), parents experiencing acute marital breakdown |
|
| Interventions |
CBT Intervention: adaptation of Cool Kids Concomitant/excluded medications: currently taking anti‐anxiety and anti‐depressant medication excluded Delivery format: child and parent concurrent sessions; group Therapist contact time: 24 hours (12 x 2 hours) Who delivers the intervention: clinical psychologist Waitlist/no treatment Intervention: waitlist, approximately 5.5 months Concomitant/excluded medications: currently taking anti‐anxiety and anti‐depressant medication excluded |
|
| Outcomes |
Remission of all anxiety disorder diagnoses post‐treatment: ADIS‐C/P Reduction in anxiety symptoms (child report) post‐treatment: SCAS‐C Reduction in anxiety symptoms (parent report) post‐treatment: SCAS‐P |
|
| Notes | Total N randomised not clear.
Author confirmed not able to provide additional diagnostic outcome data. Sample with ASD |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement Comment: No detail on sequence generation given |
| Allocation concealment (selection bias) | Unclear risk | Judgement Comment: No detail on allocation given |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Judgement Comment: Clinicians who collected post‐treatment data not blind to study aims. Not specified if blind to intervention group |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Judgement Comment: Detailed number of dropouts, but not clear if dropouts included in analyses. Did not provide n for individual measures or any detail on how missing data were managed |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Data reported for all outcome measures |
| Other source of bias ‐ Therapy integrity | Unclear risk | Judgement Comment: Therapy delivered by clinical psychologists, no other detail on training/supervision or adherence |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Cheung 2016.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: non‐controlled 6‐month follow‐up Number of study centres and location: 1, in Hong Kong Study setting: Clinic‐Child Assessment Service Date of study: 2014 to 2015 |
|
| Participants |
N = 81 (CBT: 22; active control (Attention Bias Modification Training (ABM)): 20; CBT + ABM: 20; waitlist: 19) Mean age: 7.37 Age range: 6 to 12 Gender: 48 (64%) (n = 75) Inclusion criteria: diagnostic criteria for social anxiety disorder (based on ADIS‐P) Exclusion criteria: sensory impairments or other physical disabilities, ASD, received psychotherapy (such as CBT) or medication for anxiety or mood problems within the previous 6 months |
|
| Interventions |
CBT Intervention: adapted version of Coping Cat Delivery format: child‐only sessions, parent join some sessions Therapist contact time: 18 hours (9 x 2 hours) Who delivers the intervention: clinical psychologist Active control (ABM) Intervention: Attention Bias Modification Training (8 sessions computerised ABM training) CBT (CBT+ ABM) Intervention: adapted version of Coping Cat and ABM (8 sessions computerised ABM training) Delivery format: child‐only sessions, parent join some sessions Therapist contact time: 18 hours (9 x 2 hours) Who delivers the intervention: clinical psychologist Waitlist/no treatment Intervention: 2‐month waitlist |
|
| Outcomes |
Reduction in anxiety symptoms (child report) post‐treatment: SCAS‐C Reduction in anxiety symptoms (parent report) post‐treatment: SCAS‐P |
|
| Notes | Comparisons: CBT vs waitlist; CBT + ABM vs active control (ABM) Active control (ABM) = alternative treatment Used post‐treatment diagnostic assessment but did not report remission outcomes Thesis |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement Comment: Computerised random number generator, but unclear allocation of additional children recruited after dropouts from CBT group |
| Allocation concealment (selection bias) | Low risk | Judgement Comment: Computer based, so unlikely to foresee assignment |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Judgement Comment: No detail |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Blind assessors |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Judgement Comment: No ITT analyses reported |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes for relevant measures reported |
| Other source of bias ‐ Therapy integrity | Unclear risk | Judgement Comment: No detail |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Chiu 2013.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: treatment period 3 months. Non‐controlled 1‐year follow‐up Number of study centres and location: 2 schools in the USA Study setting: elementary schools Date of study: recruitment January 2005 to April 2008 |
|
| Participants |
N = 40 (CBT: N = 22; waitlist: N = 18) Mean age: 8.51 (1.74) Age range: 5 to 12 Gender: 18 (45%) female Inclusion criteria: primary diagnosis of separation anxiety disorder, social phobia, or generalised anxiety disorder (DSM–IV) (based on ADIS‐C/P); no psychiatric medication use or stable use of psychiatric medication for at least 1 month and agree to maintain that dose throughout the study Exclusion criteria: child was currently in psychotherapy |
|
| Interventions |
CBT Intervention: Building Confidence Concomitant/excluded medications: no psychiatric medication use or stable use Delivery format: child only, or if parent opted to attend session divided into child only, parent alone, parent and child together; individual Therapist contact time: up to 16 hours (up to 16 x 1 hour) Who delivers the intervention: clinical/educational psychology doctoral students Waitlist/no treatment Intervention: 3‐month waitlist Concomitant/excluded medications: no psychiatric medication use or stable use |
|
| Outcomes |
Remission of all anxiety disorder diagnoses post‐treatment: ADIS‐C/P Reduction in anxiety symptoms (child report) post‐treatment: MASC‐Child report Reduction in anxiety symptoms (parent report) post‐treatment: MASC‐Parent report |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement Comment: Did not detail sequence generation, description of stratification method unclear |
| Allocation concealment (selection bias) | Unclear risk | Judgement Comment: No detail given |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Assessors blind to treatment condition |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: Described method for managing missing data. Small amount of missing data, only 1 dropout |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Data for each measure reported |
| Other source of bias ‐ Therapy integrity | Low risk | Judgement Comment: Trained clinicians, regular supervision. Blind assessors rated random‐selection therapy sessions for fidelity |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Cobham 2017.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: non‐controlled 12‐month follow‐up Number of study centres and location: 1, in Australia Study setting: university clinic |
|
| Participants |
N = 63 (CBT: N = 33; waitlist: N = 30) Mean age: 9.3 (2.0) (n = 60) Age range: 7 to 14 Gender: 30 (49.2%) female Inclusion criteria: child aged 7 to 14 years; child meets diagnostic criteria for a primary DSM‐IV anxiety diagnosis (based on ADIS‐C/P); parent able to attend treatment Exclusion criteria: child currently in psychotherapy |
|
| Interventions |
CBT Intervention: Fear‐less Triple P Concomitant/excluded medications: medication for anxiety excluded Delivery format: parent only; group Therapist contact time: 9 hours (6 x 1.5 hours) Who delivers the intervention: postgraduate clinical psychology interns Waitlist/no treatment Intervention: 6‐week waitlist Concomitant/excluded medications: medication for anxiety excluded |
|
| Outcomes |
Remission of primary anxiety disorder diagnoses post‐treatment: ADIS‐C/P Remission of all anxiety disorder diagnoses post‐treatment: ADIS‐C/P Reduction in anxiety symptoms (child report) post‐treatment: SCAS‐C Reduction in anxiety symptoms (parent report) post‐treatment: SCAS‐P |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Judgement Comment: Computer‐generated, block randomisation |
| Allocation concealment (selection bias) | Low risk | Judgement Comment: Computer generated, so unlikely to foresee assignment |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Assessors blind to treatment condition |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: Attrition/withdrawals detailed, with reasons provided. Few dropouts. Detail related to missing data provided, with evidence missing at random and appropriate imputation methods used |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes reported for all measures |
| Other source of bias ‐ Therapy integrity | Low risk | Judgement Comment: Intervention delivered by trained therapists, weekly supervision. Treatment integrity assessed and confirmed by blind researcher |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Cornacchio 2019.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: non‐controlled school year follow‐up Number of study centres and location: 1, in the USA Study setting: selective mutism treatment centre |
|
| Participants |
N = 29 (CBT: N = 14; waitlist: N = 15) Mean age: 6.6 (1.3) Age range: 5 to 9 Gender: 22 (75.9%) female Inclusion criteria: age 5 to 9, meet DSM–5 criteria for selective mutism (based on ADIS‐P) Exclusion criteria: identified as having any mental health condition more impairing than selective mutism; or they were non‐verbal with both of their parents |
|
| Interventions |
CBT Intervention: intensive group CBT programme centred around graded exposure to verbal communication that draws on parent‐child interaction therapy Concomitant/excluded medications: medication for anxiety excluded Delivery format: child‐only and parent‐only sessions; group Therapist contact time: 30 to 40 hours (5 x 6 to 8 hours, 5 consecutive days) Who delivers the intervention: counsellor and masters‐level therapist Waitlist/no treatment Intervention: 4‐week waitlist, 1‐page psychoeducation information brochure on selective mutism Concomitant/excluded medications: medication for anxiety excluded |
|
| Outcomes |
Remission of primary anxiety disorder diagnoses post‐treatment: ADIS‐P Improvement in global functioning post‐treatment: CGAS |
|
| Notes | Report CBCL‐Anxiety t score | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement Comment: Not detailed |
| Allocation concealment (selection bias) | Unclear risk | Judgement Comment: Not detailed |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Masked assessors |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: Retention detailed, and procedure for managing missing data appropriate |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes reported for relevant measures |
| Other source of bias ‐ Therapy integrity | Low risk | Judgement Comment: Trained staff, and fidelity assessed and reported |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Creswell 2017.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: 6‐month follow‐up Number of study centres and location: 4, in the UK Study setting: CAMHS Date of study: recruitment March 2012 to March 2014 |
|
| Participants |
N = 136 randomised (CBT: N = 68; active control: N = 68) NB: N = 122 met diagnostic criteria for an anxiety disorder and were included here (based on ADIS‐C/P) Age range: 5 to 12 Gender: 63 (51.6%) female (n = 122) Inclusion criteria: child aged 5 to 12 years with anxiety associated with clinical impairment as the primary presenting problem. NB: we only included those who met diagnostic criteria (90% original sample) Exclusion criteria: children prescribed psychotropic medication, and parents or children with little understanding of English or with physical or intellectual impairment (including autism spectrum disorder) that would interfere with their ability to participate in assessments or treatment |
|
| Interventions |
CBT Intervention: parent‐guided CBT Concomitant/excluded medications: not allowed Delivery format: parent only; individual Therapist contact time: 5 hours (5 x 1 hour) (face‐to‐face and telephone sessions) Who delivers the intervention: primary mental health workers Active control Intervention: Solution Focused Therapy Concomitant/excluded medications: not allowed Delivery format: child only, and 1 session parent and child; individual Therapist contact time: 5 hours (5 x 1 hour) Who delivers the intervention: primary mental health workers |
|
| Outcomes |
Remission of primary anxiety disorder diagnosis post‐treatment and 6‐month follow‐up: ADIS‐C/P Remission of all anxiety disorder diagnoses post‐treatment and 6‐month follow‐up: ADIS‐C/P Reduction in anxiety symptoms (child report) post‐treatment and 6‐month follow‐up: SCAS‐C Reduction in anxiety symptoms (parent report) post‐treatment and 6‐month follow‐up: SCAS‐P |
|
| Notes | Active control = alternative treatment | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Judgement Comment: Secure online minimisation tool |
| Allocation concealment (selection bias) | Low risk | Judgement Comment: Allocation sequence was retained on the secure online minimisation program, only accessible to the principal investigator and the clinical supervisor who allocated participants to clinicians |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Research staff who obtained outcome measurements were masked to group allocation |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: Dropouts detailed, and appropriate methods used to manage missing data |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes reported/provided for all measures |
| Other source of bias ‐ Therapy integrity | Low risk | Judgement Comment: Trained, supervised and adherence measured |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Dadds 1997.
| Study characteristics | ||
| Methods |
Study design: cluster‐randomised controlled trial Total duration of study: 6‐, 12‐, and 24‐month follow‐up Number of study centres and location: 8 primary schools in Australia Study setting: primary schools |
|
| Participants |
N = 128 randomised (CBT: N = 61; active control: N = 68) (NB: N = 64 met diagnostic criteria for an anxiety disorder and were included here (based on ADIS‐P)) Age range: 7 to 14 years Inclusion criteria: children met diagnostic criteria for anxiety disorder or features of anxiety disorder. We only included those who met diagnostic criteria (based on ADIS‐P, CSR = 4+) Exclusion criteria: Clinical Severity Rating 6 to 8 |
|
| Interventions |
CBT Intervention: Coping Koala (Australian modification of Coping Cat) Concomitant/excluded medications: Delivery format: child only, parent only; group Therapist contact time: 10 to 23 hours (10 x 1 to 2 hours, plus 3 parent sessions) Who delivers the intervention: clinical psychologists Waitlist/no treatment Intervention: monitoring, no intervention |
|
| Outcomes |
Remission of primary anxiety disorder diagnosis post‐treatment and 6‐, 12‐, and 24‐month follow‐up: ADIS‐P Remission of all anxiety disorder diagnoses post‐treatment and 6‐, 12‐, and 24‐month follow‐up: ADIS‐P Reduction in anxiety symptoms (child report) post‐treatment and 6‐, 12‐, and 24‐month follow‐up: RCMAS |
|
| Notes | Author provided data on outcomes for participants who met diagnostic criteria for an anxiety disorder (CSR 4+) at baseline. Cluster trial ‐ adjustments for analysis as per protocol |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement Comment: Schools matched for size, sociodemographics, and were randomly allocated to condition. No further detail |
| Allocation concealment (selection bias) | Unclear risk | Judgement Comment: No detail |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Blind assessors |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: Author provided data |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes reported/provided |
| Other source of bias ‐ Therapy integrity | Low risk | Judgement Comment: Regular supervision, integrity monitored, and no significant departures from protocol reported |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Flannery Schroeder 2000.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: non‐controlled 3‐month and 1‐year follow‐up Number of study centres and location: 1, in the USA Study setting: university clinic |
|
| Participants |
N = 45 (CBT‐individual: N = 18; CBT‐group: N = 13; waitlist: N = 14) Age range: 8 to 14 years Inclusion criteria: DSM‐IV diagnostic criteria for a childhood anxiety disorder (generalised anxiety disorder, separation anxious disorder, social phobia) (based on ADIS‐C/P) Exclusion criteria: a disabling physical condition, psychotic symptoms or current use of anti‐anxiety or anti‐depressant medication; primary diagnosis of simple phobia |
|
| Interventions |
CBT‐individual Intervention: Coping Cat Concomitant/excluded medications: current use of anti‐anxiety or anti‐depressant medication excluded Delivery format: child‐only sessions, with additional parent meetings; individual Therapist contact time: 15 to 18 hours (18 x 50 to 60 minutes) Who delivers the intervention: trained therapists, doctoral candidates CBT‐group Intervention: Adapted Coping Cat for groups Concomitant/excluded medications: current use of anti‐anxiety or anti‐depressant medication excluded Delivery format: child‐only sessions, with additional parent meetings; group Therapist contact time: 27 hours (18 x 90 minutes) Who delivers the intervention: trained therapists, doctoral candidates Waitlist/no treatment Intervention: 9‐week waitlist Concomitant/excluded medications: current use of anti‐anxiety or anti‐depressant medication excluded |
|
| Outcomes |
Remission of primary anxiety disorder diagnosis post‐treatment: ADIS‐C/P Reduction in anxiety symptoms (child report) post‐treatment: RCMAS Reduction in anxiety symptoms (parent report) post‐treatment: STAIC‐trait (mother report) Reduction in depressive symptoms post‐treatment: CDI |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement Comment: Block randomisation used to assign to group CBT. No detail on sequence generation |
| Allocation concealment (selection bias) | Unclear risk | Judgement Comment: No detail given (only detail on teachers blind to condition) |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Judgement Comment: No detail given regarding whether or not diagnostic assessments were administered by blind assessors |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: Detail on dropouts. Reported ITT similar pattern as completers on continuous measures |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Measures reported |
| Other source of bias ‐ Therapy integrity | Low risk | Judgement Comment: Therapy adherence assessed by independent rater. Therapists trained |
| Other bias | High risk | Judgement Comment: Waitlist duration shorter than treatment |
Fujii 2013.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: 32‐week treatment period Number of study centres and location: 1, in the USA Study setting: clinic |
|
| Participants |
N = 16 (CBT: N = 10; TAU: N = 6) Mean age (SD): 8.80 (1.60), n = 12 Age range: 7 to 11 Gender: 3 (25%) female (n = 12) Inclusion criteria: research criteria for ASD and at least 1 anxiety disorder, CSR 5+ (based on ADIS‐C/P) Exclusion criteria: verbal IQ < 70, primary diagnosis other than anxiety |
|
| Interventions |
CBT Intervention: Building Confidence CBT Program Concomitant/excluded medications: psychiatric medication, if used, was maintained at a stable dose for at least 1 month prior to intake and throughout the duration of the trial Delivery format: child and parent (part of each session individually, and part together); individual Therapist contact time: 48 hours (32 x 90 minutes) Who delivers the intervention: graduate/postdocs in psychology or psychiatry TAU Intervention: free to seek any kind of treatment for period of 16 weeks Concomitant/excluded medications: psychiatric medication, if used, was maintained at a stable dose for at least 1 month prior to intake. Allowed to alter medication during TAU period, as long as stable for at least 1 month prior to post‐assessment |
|
| Outcomes | Remission of primary anxiety disorder diagnosis post‐treatment: ADIS‐C/P | |
| Notes | Sample with ASD | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement Comment: Blocked randomised by sex and age. No detail on sequence generation |
| Allocation concealment (selection bias) | Unclear risk | Judgement Comment: No detail given |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: All assessments were conducted by independent evaluators blind |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: Attrition detailed, data reported |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Reported diagnostic outcomes. No mention of other measures (but reasonable given small sample, population) |
| Other source of bias ‐ Therapy integrity | Low risk | Judgement Comment: Trained and supervisors therapists. Adherence assessed and reported |
| Other bias | High risk | Judgement Comment: TAU period shorter than treatment period |
Gallagher 2004.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: 3‐week follow‐up (3 weeks after end of treatment) Number of study centres and location: 1 in the USA Study setting: clinic |
|
| Participants |
N = 23 (CBT: N = 12; waitlist: N = 11) Age range: 8 to 11 Gender: 12 (52.2%) female Inclusion criteria: meet diagnostic criteria for social phobia (based on ADIS‐C/P) Exclusion criteria: Attention Deficit Hyperactivity Disorder, conduct disorder, Oppositional Defiant Disorder, bipolar, suicidal ideation, mental retardation |
|
| Interventions |
CBT Intervention: brief group intervention for preadolescents with social phobia Delivery format: child only (plus initial child + parent session); group Therapist contact time: 9 hours (3 x 180 minutes) Who delivers the intervention: primary investigator and graduate students Waitlist/no treatment Intervention: 6‐week waitlist |
|
| Outcomes |
Remission of primary anxiety disorder diagnosis post‐treatment: ADIS‐P Reduction in anxiety symptoms (child report) post‐treatment: RCMAS Reduction in depressive symptoms post‐treatment: CDI |
|
| Notes | Report parent and child ADIS data separately; given age of sample, use ADIS‐P data here | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement Comment: No detail given on sequence generation |
| Allocation concealment (selection bias) | Unclear risk | Judgement Comment: Separation of therapists from initial screening, but allocation concealment not detailed |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Procedure somewhat unclear, but sufficient detail to determine post‐treatment assessments carried out by blind assessors |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Judgement Comment: N given for diagnostic outcomes, but attrition not specified. Refer to missing parent data, but not detailed by group |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Report outcomes for measures |
| Other source of bias ‐ Therapy integrity | Low risk | Judgement Comment: Treatment administered by doctoral students and author of manual. Adherence assessed and reported |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Ginsburg 2002.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Number of study centres and location: 1, in the USA Study setting: urban high school |
|
| Participants |
N = 12 (CBT: N = 6; active control: N = 6) Mean age (SD): 15.6 Age range: 14 to 17 Inclusion criteria: DSM‐IV criteria for a primary (i.e. most severe) anxiety diagnosis (excluding Obsessive Compulsive Disorder and Post Traumatic Stress Disorder), with CSR ≥ 4 (based on ADIS‐C); not currently participating in psychiatric or psychosocial treatment aimed at reducing anxiety symptoms Exclusion criteria: psychiatric condition contradicting study treatment (e.g. suicidal intent) or needed more immediate or alternative treatment |
|
| Interventions |
CBT Intervention: modified version of group CBT manual (Silverman 1999b) Concomitant/excluded medications: currently participating in any psychiatric treatment excluded Delivery format: child only; group Therapist contact time: 7.5 hours (10 x 45 minutes) Who delivers the intervention: 2 advanced graduate students trained in CBT Active control Intervention: attention‐support control. Sharing and discussing experiences related to anxiety. Avoided components of CBT Concomitant/excluded medications: currently participating in any psychiatric treatment excluded Delivery format: child only; group Therapist contact time: 7.5 hours (10 x 45 minutes) |
|
| Outcomes |
Remission of primary anxiety disorder diagnosis post‐treatment: ADIS‐C Remission of all anxiety disorder diagnoses post‐treatment: ADIS‐C Reduction in anxiety symptoms (child report) post‐treatment: SCARED‐C |
|
| Notes | Active control = attention control | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Judgement Comment: Used random number table |
| Allocation concealment (selection bias) | Unclear risk | Judgement Comment: No detail given |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Judgement Comment: No detail given about blinding participants |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: ADIS assessors unaware of treatment condition |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: Attrition reported and similar across groups, and reason reported where available ("no longer need group") |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes reported for all relevant included measures |
| Other source of bias ‐ Therapy integrity | Low risk | Judgement Comment: Therapists trained and adherence monitored and approach justified |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Ginsburg 2012.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: 1‐month follow‐up Number of study centres and location: 14 schools in the USA Study setting: school‐based mental health clinics |
|
| Participants |
N = 32 (CBT: N = 17; TAU: N = 15) Mean age (SD): CBT: 11.12 (2.75); TAU: 9.33 (2.06) Age range: 7 to 17 Gender: CBT: 12 (70.6%) female; TAU: 8 (53.3%) female Inclusion criteria: age 7 to 17, presence of GAD, social anxiety disorder, separation anxiety disorder, specific phobia, or anxiety disorder not otherwise stated (based on ADIS‐C/P), no medical or psychiatric conditions contraindicating study intervention, not currently receiving anxiety treatment Exclusion criteria: failed a previous trial of CBT for anxiety |
|
| Interventions |
CBT Intervention: modular CBT adapted from CBT manuals Concomitant/excluded medications: stable medication for another psychiatric disorder allowed Delivery format: child only, encouraged to involve parents in at least 3 sessions; individual Therapist contact time: 6 hours (8 x 45 minutes over 12 weeks) Who delivers the intervention: novice CBT school‐based clinicians TAU Intervention: therapeutic intervention that did not include CBT strategies. Therapy represented usual care for that therapist (e.g. art, play, or supportive therapy), and provided with attention control manual to use if they desired Concomitant/excluded medications: stable medication for another psychiatric disorder allowed Delivery format: child only, encouraged to involve parents in at least 3 sessions; individual Therapist contact time: 6 hours (8 x 45 minutes over 12 weeks) Who delivers the intervention: novice CBT school‐based clinician |
|
| Outcomes |
Reduction in anxiety symptoms (child report) post‐treatment and follow‐up (≤ 6 months): SCARED‐C Reduction in anxiety symptoms (parent report) post‐treatment and follow‐up (≤ 6 months): SCARED‐P |
|
| Notes | Post‐treatment diagnostic assessment included, but did not report required remission outcomes. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Judgement Comment: Sequence online and separate for each clinician |
| Allocation concealment (selection bias) | Low risk | Judgement Comment: Use website to generate number, so unlikely to foresee assignment |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Judgement Comment: No detail given |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Independent assessors, scores reviewed by senior clinician blind to condition |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: Attrition detailed, appropriate imputation for dealing with missing data. 11% outcome data missing |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes reported |
| Other source of bias ‐ Therapy integrity | Unclear risk | Judgement Comment: Adherence assessed and reported; there was some evidence that TAU participants received elements of CBT, which could potentially have influenced outcomes |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Ginsburg 2019a.
| Study characteristics | ||
| Methods |
Study design: cluster‐randomised controlled trial Total duration of study: 1‐year follow‐up Number of study centres and location: USA Study setting: schools Date of study: 2012 to 2017 |
|
| Participants |
N = 216 (CBT: 148; TAU: 68) Mean age (SD): 10.87 (3.27) Age range: 6 to 18 Gender: 48.6% female Inclusion criteria: age 6 to 18, met DSM‐IV diagnostic criteria for primary anxiety disorder (based on ADIS‐C/P) Excluded criteria: medical or psychiatric condition contraindicating study treatment (e.g. suicidality) and needed immediate or alternative treatment, were receiving psychosocial treatment for anxiety and/or were in the custody of state social services |
|
| Interventions |
CBT Intervention: modular CBT. Adapted from empirically supported manuals. Included: psychoeducation, exposure, rewards, cognitive restructuring, problem solving, somatic/relaxation skills, relapse prevention, optional parental psychoeducation module Concomitant/excluded medications: stable dose allowed Delivery format: child only, optional parent; individual Therapist contact time: 6 to 8 hours (12 x 30 to 40 minutes) Who delivers the intervention: school‐based clinicians TAU Intervention: therapeutic strategies clinicians would typically provide (e.g. supportive therapy) Concomitant/excluded medications: stable dose allowed Delivery format: child only; individual Therapist contact time: 6 to 8 hours (12 x 30 to 40 minutes) Who delivers the intervention: school‐based clinicians |
|
| Outcomes | Remission of primary anxiety disorder diagnosis post‐treatment and 12‐month follow‐up: ADIS‐C/P | |
| Notes | SCARED‐C, SCARED‐P, CGAS reported but no SDs Cluster trial ‐ reported data adjusted as per protocol |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement Comment: Web‐based randomisation plan generator, but change in randomisation ratios post onset |
| Allocation concealment (selection bias) | Low risk | Judgement Comment: Web based, so unlikely to foresee assignment |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Judgement Comment: Not specified |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Blind assessors |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: Attrition reported and appropriate method for managing missing data |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes reported |
| Other source of bias ‐ Therapy integrity | Low risk | Judgement Comment: Adherence measured |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Hancock 2018.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: 3‐month follow‐up for treatment groups only Number of study centres and location: 1 in Australia Study setting: university hospital |
|
| Participants |
N = 193 (CBT (Acceptance and Commitment Therapy): N = 68; CBT: N = 63; waitlist: N = 62) Mean age (SD): 11.2 (2.76) Age range: 7 to 17 Gender: 111 (58%) female Inclusion criteria: DSM‐IV anxiety disorder (based on ADIS‐C/P), age 7 to 17 Exclusion criteria: non‐English speaker, complex mental health problems (e.g. psychotic symptoms, major depression primary disorder) or medical conditions, attention deficit disorder with hyperactivity that was not well controlled, taking psychotropic medication for less than 2 months, post‐traumatic stress disorder (due to specialised treatment required), or academically more than 1 grade behind peers |
|
| Interventions |
CBT (ACT) Intervention: ACT programme. Included mindfulness, psychoeducation, cognitive defusion, exposure, cognitive coping, problem solving, social skills Concomitant/excluded medications: medication‐free or stabilised on anti‐depressants for at least 2 months Delivery format: child and parent; group Therapist contact time: 15 hours (10 x 90 minutes) Who delivers the intervention: clinical psychologists CBT (Cool Kids/Chilled) Intervention: Cool Kids/Chilled programme for children and adolescents Concomitant/excluded medications: medication‐free or stabilised on anti‐depressants for at least 2 months Delivery format: child and parent; group Therapist contact time: 15 hours (10 x 90 minutes) Who delivers the intervention: clinical psychologists Waitlist Intervention: 10 weeks waitlist Concomitant/excluded medications: medication‐free or stabilised on anti‐depressants for at least 2 months |
|
| Outcomes | Reduction in anxiety symptoms (child report) post‐treatment: MASC‐C | |
| Notes | Use post‐treatment diagnostic assessment, but did not report remission outcomes | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Judgement Comment: Clear details of sequence allocation |
| Allocation concealment (selection bias) | Low risk | Judgement Comment: Participants’ enrolment into the study was conducted by an intake officer. They were subsequently assessed by researchers masked to the treatment condition, with both parties informed of the group allocation after assessment. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Blind assessors and subset interviews rated by clinicians blind to original diagnosis and group |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: Attrition detailed and reasons provided. Some of reasons for attrition were potentially related to group allocation, but appropriate imputation methods were used to manage missing data (ITT analyses undertaken). |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes for planned relevant measures reported. Some measures reported elsewhere. |
| Other source of bias ‐ Therapy integrity | Low risk | Judgement Comment: Therapist competence and adherence assessed and reported |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Herbert 2009.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: 6‐month follow‐up Number of study centres and location: 1 in the USA Study setting: university clinic |
|
| Participants |
N = 73 (CBT‐group: N = 23; CBT‐individual: N = 24; control: N = 26) Mean age (SD): CBT‐group: 14.6 (2.8); CBT‐individual: 14.3 (2.1); control: 15.1 (1.4) Age range: 12 to 17 Gender: 42 (57.5%) female Inclusion criteria: primary social anxiety disorder, generalised subtype (based on ADIS‐C); aged 12 to 17; literacy in English Excluded criteria: history of mental retardation, pervasive developmental disorder, organic mental disorder, bipolar disorder, a psychotic disorder, or borderline or schizotypal personality disorder, imminent suicidal risk, substance abuse or dependence within the past year, or a previous trial of behaviour or CBT for social anxiety disorder |
|
| Interventions |
CBT (group) Intervention: psychoeducation, breathing retraining, cognitive restructuring, simulated and in vivo exposure to phobic stimuli, and social skills training Concomitant/excluded medications: stabilised (at least 3 months with no change in medication or dosage) allowed Delivery format: child only; group Therapist contact time: 24 hours (12 x 2 hours) Who delivers the intervention: advanced doctoral candidates in clinical psychology CBT (individual) Intervention: same content as group CBT Concomitant/excluded medications: stabilised (at least 3 months with no change in medication or dosage) allowed Delivery format: child only; individual Therapist contact time: 12 hours (12 x 1 hour) Who delivers the intervention: advanced doctoral candidates in clinical psychology Active control Intervention: psychoeducational supportive therapy. Discussions around various topics relevant to social anxiety disorder. Therapists offered support but did not provide specific advice, teach skills, problem‐solve, or assign exposure exercises. Concomitant/excluded medications: stabilised (at least 3 months with no change in medication or dosage) allowed Delivery format: child only; group Therapist contact time: 24 hours (12 x 2 hours) Who delivers the intervention: advanced doctoral candidates in clinical psychology |
|
| Outcomes |
Reduction in anxiety symptoms (child report) post‐treatment and follow‐up (6 months): SPAI‐C Reduction in anxiety symptoms (parent report) post‐treatment and follow‐up (6 months): SAS‐P |
|
| Notes | Post‐treatment diagnostic assessment used but required remission outcomes not reported. Active control = attention control |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Judgement Comment: Block randomisation |
| Allocation concealment (selection bias) | Unclear risk | Judgement Comment: No detail |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Judgement Comment: No detail |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Blind outcome assessment |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: Attrition detailed, differences between completers and dropouts examined and reported; details for managing missing data reported |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes for planned measures reported |
| Other source of bias ‐ Therapy integrity | Low risk | Judgement Comment: Trained therapists, regular supervisor to monitor adherence, measures of fidelity given |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Hirshfeld Becker 2010.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: 1‐year non‐controlled follow‐up Number of study centres and location: 1 in the USA Study setting: research clinic Date of study: February 2001 to January 2004 |
|
| Participants |
N = 64 (CBT: N = 34; waitlist: N = 30) Mean age (SD): 5.4 (1.0) Age range: 4 to 7 Gender: 34 (53%) female Inclusion criteria: current DSM‐IV anxiety disorder (based on K‐SADS) Exclusion criteria: active psychosis, suicidality, or substance abuse in a parent; mental retardation in the child; current psychiatric treatment or past CBT; if a consensus of 2 senior clinicians judged the child to be too unco‐operative or distractible to take part in the trial or too severely symptomatic to wait 6 months to receive treatment, based on suicidal ideation, serious impairment in eating or sleeping habits, severe social isolation, severe impairment in school function or attendance, or severe OCD |
|
| Interventions |
CBT Intervention: Being Brave: A Program for Coping with Anxiety for Young Children and Their Parents. Loosely modelled after the manualised Coping Cat programme Concomitant/excluded medications: Delivery format: parent only, and child and parent sessions; individual Therapist contact time: up to 20 sessions over 6 months Who delivers the intervention: psychologists and postdoctoral fellow Waitlist/no treatment Intervention: 6‐month waitlist |
|
| Outcomes |
Remission of primary anxiety disorder diagnosis post‐treatment: K‐SADS‐E Remission of all anxiety disorder diagnoses post‐treatment: K‐SADS‐E |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Judgement Comment: Block randomisation; the allocation sequences were generated in advance for the 2 cells (presence or absence of parental anxiety disorders) by the study co‐ordinator |
| Allocation concealment (selection bias) | Low risk | Judgement Comment: Concealed in a computer file from all other staff (including the clinicians who enrolled the participants, the assessors and clinicians who conducted the assessments, and the clinicians who determined the eligibility of each child) |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Blind assessors |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: Attrition fully reported, and for all measures. Quite high level of missing data for CBCL‐I, which is potentially related to outcome but not used here |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes reported for all measures |
| Other source of bias ‐ Therapy integrity | Unclear risk | Judgement Comment: Intervention delivered by psychologists/postdoctoral fellow, but no detail given on assessment of adherence and competence |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Holmes 2014.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: non‐controlled 3‐month follow‐up Number of study centres and location: 1 in Australia |
|
| Participants |
N = 42 (CBT: N = 20; waitlist: N = 22) Mean age (SD): 9.64 (1.41) Age range: 7 to 12 Gender: 28 (66.7%) female Inclusion criteria: aged 7 to 12, primary diagnosis GAD (based on ADIS‐C/P) Exclusion criteria: pervasive developmental disorder, intellectual handicap or learning disability, behavioural problems more impairing than anxiety, substance abuse, self‐harm or suicidal ideation; currently receiving psychological assistance or medical treatment |
|
| Interventions |
CBT Intervention: No Worries ‐ target intolerance of uncertainty, negative beliefs about worry, negative problem orientation, cognitive avoidance Delivery format: child and parent; group Therapist contact time: 15 hours (10 x 90 minutes) Who delivers the intervention: postgraduate students receiving advanced clinical training, supervised Waitlist/no treatment Intervention: 12‐week waitlist |
|
| Outcomes |
Remission of primary anxiety disorder diagnosis post‐treatment: ADIS‐C/P Reduction in anxiety symptoms (child report) post‐treatment: SCAS‐C Reduction in anxiety symptoms (parent report) post‐treatment: SCAS‐P Improvement in global functioning post‐treatment: CGAS |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Judgement Comment: Computer‐generated, blocked randomisation list |
| Allocation concealment (selection bias) | Low risk | Judgement Comment: Computer generated, so unlikely to foresee assignment |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Assessors blind to both experimental condition and client history |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: Dropouts and reasons for them detailed and clear. Completer analysis reported, and compared to ITT. |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes for all measures reported. |
| Other source of bias ‐ Therapy integrity | Low risk | Judgement Comment: Adherence rated and reported; delivered by provisionally registered psychologists, with regular supervision |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Hudson 2009.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: 3‐month follow‐up Number of study centres and location: 1 in Australia Study setting: research clinic |
|
| Participants |
N = 112 (CBT: N = 60; active control: N = 52) Mean age (SD): CBT: 10.2 (2.4) (n = 51); active control: 0.2 (2.7) (n = 44) Age range: 7 to 16 Gender: CBT: 37.3% female (n = 51); active control: 52.3% female (n = 44) Inclusion criteria: primary anxiety disorder (based on ADIS‐C/P) Exclusion criteria: mental retardation, psychoses, and concurrent psychological treatment |
|
| Interventions |
CBT Intervention: Cool Kids Concomitant/excluded medications: allowed if stable Delivery format: child and parent; group Therapist contact time: 20 hours (10 x 2 hours) Who delivers the intervention: clinical psychologists or postgraduate students Active control Intervention: group support and attention. Aim to provide supportive environment, activities to help express and understand emotions and build relationships between and within families. Therapists instructed not to provide CBT interpretations or strategies. Concomitant/excluded medications: allowed if stable Delivery format: child and parent; group Therapist contact time: 20 hours (10 x 2 hours) Who delivers the intervention: clinical psychologists or postgraduate students |
|
| Outcomes |
Remission of primary anxiety disorder diagnosis post‐treatment and 3‐month follow‐up: ADIS‐C/P Remission of all anxiety disorder diagnoses post‐treatment and 3‐month follow‐up: ADIS‐C/P Reduction in anxiety symptoms (child report) post‐treatment and 3‐month follow‐up: SCAS‐C Reduction in anxiety symptoms (parent report‐mother) post‐treatment and 3‐month follow‐up: SCAS‐P |
|
| Notes | Active control = attention control | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Judgement Comment: Used a schedule from a random number generator to assign each group |
| Allocation concealment (selection bias) | Unclear risk | Judgement Comment: Performed by principal investigator. No detail on attempt to conceal allocation |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Appropriate methods to conceal differences between control and CBT; participants told 1 treatment new to the clinic, once assignment informed about their condition |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Judgement Comment: Reliability of ADIS outcomes assessed, but no detail on blinding of assessors/double raters |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: Attrition detailed. Appropriate methods for handling missing data. Completer analyses reported, and ITT also performed for comparison. |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes for all measures reported |
| Other source of bias ‐ Therapy integrity | Low risk | Judgement Comment: Therapists qualified and supervised. Therapy adherence assessed and reported. Detailed procedure for managing 1 instance of protocol breach |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Ingul 2013.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: non‐controlled 12‐month follow‐up Number of study centres and location: Norway Study setting: recruitment through school screening |
|
| Participants |
N = 128 (CBT‐individual: N = 36; CBT‐group: N = 58; active control: N = 34) Mean age (SD): 14.5 (1.01) (n = 57) Age range: 13 to 16 Gender: 32 (56.1%) female (n = 57) Inclusion criteria: primary problem social phobia diagnosis (based on ADIS‐C) Exclusion criteria: mental retardation or psychosis; being treated elsewhere for mental health conditions |
|
| Interventions |
CBT‐individual Intervention: Clark and Wells manual, adapted for adolescents Delivery format: child only; individual Therapist contact time: 10 hours (12 x 50 minutes) Who delivers the intervention: clinical psychologist and co‐therapists CBT‐group Intervention: based on CAT Project Manual for CBT of Anxious Adolescents, with some play elements from SET‐C Delivery format: child only; group Therapist contact time: 15 hours (10 x 90 minutes) Who delivers the intervention: clinical psychologist and co‐therapists Active control Intervention: attentional placebo. No active components in CBT. Social activity, social interaction, and social support Delivery format: child only; group Therapist contact time: 15 hours (10 x 90 minutes) Who delivers the intervention: experienced milieu therapists |
|
| Outcomes |
Reduction in anxiety symptoms (child report) post‐treatment: SCARED‐C Reduction in depressive symptoms post‐treatment: CDI |
|
| Notes | Active control = attention control Follow‐up diagnostic assessment, but only CBT groups |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Judgement Comment: Pre‐assigned random schedule |
| Allocation concealment (selection bias) | Unclear risk | Judgement Comment: State performed at each site, but no further detail |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Judgement Comment: No detail given |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Assessors blind |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Judgement Comment: High dropout rate and large amount of missing data and related to treatment group, although ITT analysis reported to confirm completer analysis |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes for measures reported |
| Other source of bias ‐ Therapy integrity | Unclear risk | Judgement Comment: Therapists appropriately qualified. Adherence and competence assessed and reported in 2 CBT groups, but not the control. |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Ishikawa 2019.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: non‐controlled 3‐ and 6‐month follow‐up Number of study centres and location: Japan Study setting: clinic Date of study: recruitment 2012 to 2015; follow‐up complete 2017 |
|
| Participants |
N = 51 (CBT: N = 26; waitlist: N = 25) Mean age (SD): 10.9 (2.0) Age range: 8 to 15 Gender: 29 (56.9%) female Inclusion criteria: (a) age 7 to 15, (b) attend the programme with their parents, (c) have an anxiety disorder (based on ADIS), (d) did not fulfil criteria for PTSD, disruptive behavioural disorders, substance abuse, mental retardation, pervasive developmental disorder, or a psychotic disorder, and (e) agree to discontinue other forms of therapy for the duration of the study |
|
| Interventions |
CBT Intervention: Japanese Anxiety Children/Adolescents Cognitve Behaviour Therapy Program Concomitant/excluded medications: none currently taking medication Delivery format: child and parent together; individual Therapist contact time: 8 hours (8 x 1 hour) Who delivers the intervention: clinical psychologist Waitlist/no treatment Intervention: 2‐month waitlist Concomitant/excluded medications: none currently taking medication |
|
| Outcomes |
Remission of primary anxiety disorder diagnosis post‐treatment: ADIS‐C/P (parent and child interviewed together) Remission of all anxiety disorder diagnoses post‐treatment: ADIS‐C/P (parent and child interviewed together) Reduction in anxiety symptoms (child report) post‐treatment: SCAS‐C Reduction in anxiety symptoms (parent report) post‐treatment: SCAS‐P Reduction in depressive symptoms post‐treatment: CDI |
|
| Notes | 4 participants met diagnostic criteria for an anxiety disorder, but primary disorder was a depressive disorder. Included in all analyses apart from remission of primary anxiety disorder diagnosis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Judgement Comment: Random number generator |
| Allocation concealment (selection bias) | Low risk | Judgement Comment: Independent person |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Blind assessors |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: Report ITT and completer analyses. Only 1 dropout in each condition |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes for measures reported |
| Other source of bias ‐ Therapy integrity | Low risk | Judgement Comment: Trained therapists. Adherence assessed and reported. |
| Other bias | High risk | Judgement Comment: Difference in timing for post‐assessment for CBT vs waitlist ‐ shorter time period for waitlist (70 days vs 122). Included children with depressive disorders as primary diagnoses |
Kendall 1994.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: non‐controlled long‐term follow‐up Number of study centres and location: 1 in the USA Study setting: university clinic |
|
| Participants |
N = 60 (CBT: N = 30; waitlist: N = 30) Age range: 9 to 13 Gender: 40% female (n = 47) Inclusion criteria: primary anxiety disorder diagnosis (i.e. over‐anxious disorder, separation anxiety disorder, avoidant disorder) based on ADIS‐C/P Exclusion criteria: primary diagnosis of specific phobia, IQ below 80, disabling physical condition, displayed psychotic symptoms, currently using anti‐anxiety medications |
|
| Interventions |
CBT Intervention: Coping Cat Concomitant/excluded medications: anti‐anxiety medication excluded Delivery format: child only; individual Therapist contact time: 13 to 20 hours (16 to 20 x 50‐ to 60‐minute sessions over 16 weeks) Who delivers the intervention: doctoral students Waitlist/no treatment Intervention: 8‐week waitlist Concomitant/excluded medications: anti‐anxiety medication excluded |
|
| Outcomes |
Remission of primary anxiety disorder diagnosis post‐treatment: ADIS‐P Reduction in anxiety symptoms (child report) post‐treatment: RCMAS Reduction in anxiety symptoms (parent report) post‐treatment: STAIC‐trait‐parent Reduction in depressive symptoms post‐treatment: CDI |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement Comment: No detail given |
| Allocation concealment (selection bias) | Unclear risk | Judgement Comment: No detail given |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Judgement Comment: Specify observational data rated by blind assessors, but no detail about diagnostic assessments |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Judgement Comment: Number of dropouts detailed, and dropouts vs remainers compared, but analyses only include completers; insufficient detail on how missing data were managed or comparison with ITT |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes for measures reported |
| Other source of bias ‐ Therapy integrity | Low risk | Judgement Comment: Therapists appropriately qualified, integrity assessed and reported |
| Other bias | High risk | Judgement Comment: Endpoint different for waitlist (8 weeks) and CBT group (16 weeks) |
Kendall 1997.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: non‐controlled long‐term follow‐up Number of study centres and location: 1 in the USA Study setting: university clinic |
|
| Participants |
N = 118 (CBT: N = 69; waitlist: N = 49) Age range: 9 to 13 Gender: 38% female (n = 94) Inclusion criteria: age 9 to 13; primary anxiety disorder (overanxious disorder, separation anxiety disorder, avoidant disorder) based on ADIS, NB: diagnosis based on parent report when discrepancy with child report Exclusion criteria: primary specific phobia diagnosis, psychotic symptoms, taking anti‐anxiety medication |
|
| Interventions |
CBT Intervention: Coping Cat Concomitant/excluded medications: anti‐anxiety medication excluded Delivery format: child‐only sessions and parent meeting; individual Therapist contact time: 18 hours (18 x 1 hour) Who delivers the intervention: doctoral students Waitlist/no treatment Intervention: 8‐week waitlist Concomitant/excluded medications: anti‐anxiety medication excluded |
|
| Outcomes |
Remission of primary anxiety disorder diagnosis post‐treatment: ADIS‐P Reduction in anxiety symptoms (child report) post‐treatment: RCMAS Reduction in anxiety symptoms (parent report) post‐treatment: CBCL‐Anxiety scale (mother) Reduction in depressive symptoms post‐treatment: CDI |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement Comment: No detail given |
| Allocation concealment (selection bias) | Unclear risk | Judgement Comment: No detail given |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Judgement Comment: No detail given |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Judgement Comment: Dropout numbers given and reported that no there was no difference between dropouts and completers on pretreatment characteristics, but reasons for dropouts not reported. No detail on missing data for individual measures or how missing data for questionnaires were managed |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes reported for all measures |
| Other source of bias ‐ Therapy integrity | Low risk | Judgement Comment: Therapists appropriately qualified. Integrity independently assessed. |
| Other bias | High risk | Judgement Comment: Time of endpoint (post‐assessment) differed between waitlist and treatment group |
Kendall 2008.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: non‐controlled long‐term follow‐up Number of study centres and location: 1 in the USA Study setting: university clinic Date of study: referred 2000 to 2006 |
|
| Participants |
N = 161 (CBT‐individual: N = 55; CBT‐family: N = 56; active control: N = 50) Age range: 7 to 14 Gender: 71 (44%) female Inclusion criteria: age 7 to 14; primary anxiety disorder (based on ADIS‐C/P), at least 1 parent speaks English Exclusion criteria: psychotic symptoms, mental retardation, a disabling medical condition, the child’s participation in concurrent treatment, or the child’s taking anti‐anxiety or anti‐depressant medications |
|
| Interventions |
CBT Intervention: Coping Cat Concomitant/excluded medications: anti‐anxiety medication excluded Delivery format: child (14 sessions), parent (2 sessions); individual Therapist contact time: 16 hours (16 x 1 hour) Who delivers the intervention: master’s level therapists with 2 to 3 years of experience at the clinic and doctoral‐level psychologist CBT Intervention: family CBT for anxious children manual (Howard, Chu, Krain, Marrs‐Garcia, & Kendall, 2000) and used the Coping Cat Workbook Concomitant/excluded medications: anti‐anxiety medication excluded Delivery format: child and parent together, 2 sessions child and parent separate; individual Therapist contact time: 16 hours (16 x 1 hour) Who delivers the intervention: master’s level therapists with 2 to 3 years of experience at the CAADC and doctoral‐level psychologist Active control Intervention: manual for family education, support, and attention for anxious children and used a workbook to add child interest/involvement Concomitant/excluded medications: anti‐anxiety medication excluded |
|
| Outcomes |
Remission of primary anxiety disorder diagnosis post‐treatment: ADIS‐C/P Remission of all anxiety disorder diagnoses post‐treatment: ADIS‐C/P Reduction in anxiety symptoms (child report) post‐treatment: MASC‐C Reduction in anxiety symptoms (parent report) post‐treatment: CBCL‐Anxiety scale (mother) Reduction in depressive symptoms post‐treatment: CDI |
|
| Notes | Include 1‐year follow‐up, but control group who still met criteria offered treatment after post‐treatment, so did not include follow‐up here Active control = attention control | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Judgement Comment: The co‐ordinator used a predetermined schedule (random number generated) |
| Allocation concealment (selection bias) | Low risk | Judgement Comment: Key to blind held by co‐ordinator, not primary investigator or therapist, but no further detail given |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Judgement Comment: No detail given regarding blinding of participants |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Independent assessors and families asked not to discuss treatment |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: Attrition detailed, and reasons for dropouts given. ITT analysis. Missing data for measures handled appropriately (last observation carried forward). |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes reported for all measures |
| Other source of bias ‐ Therapy integrity | Unclear risk | Judgement Comment: Therapists trained and supervised, and integrity assessed. Evidence of CBT bleeding in control group could have influenced outcomes. |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Kennedy 2009.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: 6 months (post‐treatment assessment) Number of study centres and location: Australia Study setting: university |
|
| Participants |
N = 71 (CBT: N = 35; waitlist: N = 36) Mean age (SD): 47.07 months (7.05 months) Age range: 36 to 58 months Gender: CBT: 58% female; waitlist: 51% female Inclusion criteria: child aged 36 to 58 months, high on a laboratory measure of behavioural inhibition (BI), at least 1 parent met DSM‐IV criteria for diagnosis of an anxiety disorder (NB: not inclusion criteria, but all children meet diagnostic criteria for anxiety disorder based on ADIS‐P) Exclusion criteria: diagnosed developmental disorder or a severe language delay in the child, or parents who were unable to complete questionnaires in English |
|
| Interventions |
CBT Intervention: parent intervention ‐ modified Cool Kids Program Delivery format: parent only; group Therapist contact time: 12 hours (8 x 90 minutes) Who delivers the intervention: clinical psychologist Waitlist/no treatment Intervention: 6‐month waitlist |
|
| Outcomes |
Remission of all anxiety disorder diagnoses post‐treatment: ADIS‐P Reduction in anxiety symptoms (parent report) post‐treatment: PAS‐R (mother report) |
|
| Notes | Post‐treatment assessment point is 6 months. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Judgement Comment: Toss of coin |
| Allocation concealment (selection bias) | Unclear risk | Judgement Comment: No detail given |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Judgement Comment: ADIS assessors trained, and reliability assessed, but no detail as to whether blind or not |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: Attrition detailed, and although reasons not given, small numbers and across both groups |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes reported for all measures |
| Other source of bias ‐ Therapy integrity | Unclear risk | Judgement Comment: Therapy delivered by qualified and experienced therapist, but integrity not assessed/reported |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Khanna 2010.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Study setting: university Date of study: 2006 to 2008 |
|
| Participants |
N = 49 randomised (CBT: N = 17; computerised CBT: 16; active control: N = 16) (NB: N = 33 included here) Age range: 7 to 13 Inclusion criteria: primary anxiety disorder (separation anxiety, social phobia, GAD, specific phobia, or panic disorder) (based on ADIS‐parent and child interviewed together) Exclusion criteria: IQ < 80, psychotic symptoms, use of anti‐anxiety or depression medication or ongoing psychotherapy |
|
| Interventions |
CBT Intervention: individual CBT ‐ Coping Cat Concomitant/excluded medications: use of anti‐anxiety or depression medication not allowed Delivery format: child only, with parent included in 2 sessions; individual Therapist contact time: 10 hours (12 x 50 minutes) Who delivers the intervention: school psychologists, psychology doctoral candidates, clinical psychologist Active control Intervention: computer‐assisted education support & attention. Education, support, and attention manual (as in Kendal and colleagues, 2008) and child use of computer age‐appropriate games Concomitant/excluded medications: use of anti‐anxiety or depression medication not allowed Delivery format: child only; individual Therapist contact time: 10 hours (12 x 30 minutes of support, 20 minutes child use computer) Who delivers the intervention: school psychologists, psychology doctoral candidates, clinical psychologist |
|
| Outcomes |
Remission of primary anxiety disorder diagnosis post‐treatment: ADIS (parent and child interviewed together) Reduction in anxiety symptoms (child report) post‐treatment: MASC‐C Reduction in depressive symptoms post‐treatment: CDI Improvement in global functioning post‐treatment: CGAS |
|
| Notes | Did not include "Camp Cope‐A lot" arm (computer‐assisted CBT) Active control = attention control |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Judgement Comment: Random number‐generating program |
| Allocation concealment (selection bias) | Low risk | Judgement Comment: Computer generated, so unlikely to foresee assignment |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Judgement Comment: No evidence of blinding participants in individual CBT vs control, but as control computer program potentially not feasible |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Assessors blind to treatment condition |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: Attrition detailed and ITT analysis reported, with appropriate imputation for missing data. 2 participants in control group withdrawn due to worsening of symptoms. |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes reported |
| Other source of bias ‐ Therapy integrity | Low risk | Judgement Comment: Therapist trained and supervised. Adherence assessed and reported. |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Kidd 2018.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: non‐controlled 6‐month follow‐up Number of study centres and location: 1 in Australia Study setting: university clinic |
|
| Participants |
N = 49 (CBT: N = 26; waitlist: N = 23) Mean age (SD): 14.23 (1.76) Age range: 12 to 18 Gender: 9 (18.4%) female Inclusion criteria: meet diagnostic criteria for an anxiety disorder, with CSR 4+ (based on ADIS‐P); able to demonstrate a clinical diagnosis of ASD, Asperger’s disorder, or pervasive developmental disorder – not otherwise specified (PDD‐NOS); aged 12 to 18; verbal IQ above 70; ability to read English; not taking any psychotropic medication or taking a stable dose of psychiatric medication and, if taking medication, agreement for this to be maintained throughout the study Exclusion criteria: participated in psychotherapy, social skills training, or behavioural intervention over the course of the study; the family were attending child‐related health professional services or parenting classes; taking psychiatric medication or changed his or her dosage during the intervention period; family was not able to participate in the intervention program |
|
| Interventions |
CBT Intervention: Cool Kids, ASD adaptation Concomitant/excluded medications: stable dose, and maintain stable dose during study allowed Delivery format: combination of child alone, parent alone, and child and parent together; group Therapist contact time: 24 hours (12 x 2 hours) Who delivers the intervention: psychology graduate trainee Master's or PhD students Waitlist/no treatment Intervention: 4.5‐month waitlist Concomitant/excluded medications: stable dose, and maintain stable dose during study allowed |
|
| Outcomes |
Remission of primary anxiety disorder diagnosis post‐treatment: ADIS‐P Reduction in anxiety symptoms (child report) post‐treatment: SCAS‐C Reduction in anxiety symptoms (parent report) post‐treatment: SCAS‐P Reduction in depressive symptoms post‐treatment: SMFQ‐C |
|
| Notes | Sample with ASD | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Judgement Comment: Randomisation software |
| Allocation concealment (selection bias) | Low risk | Judgement Comment: Computer generated, so unlikely to foresee assignment |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Blind assessors |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment:Missing data detailed and managed appropriately |
| Selective reporting (reporting bias) | Low risk | Judgement Comment:Outcomes reported for all measures |
| Other source of bias ‐ Therapy integrity | Low risk | Judgement Comment: Independent integrity assessment |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Last 1998.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Study setting: university clinic Date of study: September 1993 through April 1995 |
|
| Participants |
N = 56 (CBT: N = 32; active control: N = 24) Mean age (SD): CBT: 11.67 (3.00); active control: 12.40 (2.79) Age range: 6 to 17 Gender: CBT: 13 (56%) female; active control: 15 (62%) female Inclusion criteria: (1) anxiety‐based school refusal; (2) current enrolment in elementary, middle, or high school; (3) current DSM‐lll‐R anxiety disorder diagnosis (based on K‐SADS‐P); (4) at least 10% absenteeism from classes for at least 1 month before intake; (5) no current diagnosis of major depression; and (6) no current use of psychiatric medication |
|
| Interventions |
CBT Intervention: modified adult treatment for treatment of anxiety‐based school refusal. In vivo exposure and coping self statements Concomitant/excluded medications: psychiatric medication excluded Delivery format: child and parent; individual Therapist contact time: 12 hours (12 x 1 hour) Who delivers the intervention: Therapist. Involvement of school‐based contact Active control Intervention: educational support therapy ‐ modification of control therapy used previously: educational presentations and supportive psychotherapy Concomitant/excluded medications: psychiatric medication excluded Delivery format: child only?; individual Therapist contact time: 12 hours (12 x 1 hour) Who delivers the intervention: Therapist. Involvement of school‐based contact |
|
| Outcomes |
Remission of primary anxiety disorder diagnosis post‐treatment: K‐SADS (parent and child, abbreviated form) Reduction in anxiety symptoms (child report) post‐treatment: STAIC‐modified Reduction in depressive symptoms post‐treatment: CDI |
|
| Notes | Active control = attention control | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement Comment: No detail given |
| Allocation concealment (selection bias) | Unclear risk | Judgement Comment: No detail given |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Judgement Comment: No detail given |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Judgement Comment: Assessor blind to initial diagnosis, but no detail given regarding whether blind to condition |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Judgement Comment: Attrition reported, but relatively high dropout rate and greater in CBT group, with only completer analysis reported |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes reported |
| Other source of bias ‐ Therapy integrity | Low risk | Judgement Comment: Treatment fidelity assessed and reported as highly credible |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Lau 2010.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: non‐controlled 3‐ and 6‐month follow‐up Number of study centres and location: 1 in Hong Kong Study setting: community clinic |
|
| Participants |
N = 45 randomised (NB: we only include those who met diagnostic criteria for an anxiety disorder at baseline: N = 38; CBT: N = 21; waitlist: N = 17) Age range: 6 to 11 Inclusion criteria: diagnosed with anxiety problems/disorders (we only include participants that meet diagnostic criteria based on K‐SADS) Exclusion criteria: only specific phobia, severe hyperactivity symptoms |
|
| Interventions |
CBT Intervention: Anxiety Group treatment programme ‐ adaptation of Coping Cat Delivery format: child, with parents invited to observe and meet with co‐therapists at the beginning of some sessions; group Therapist contact time: 18 hours (9 x 2 hours) Waitlist/no treatment Intervention: 13‐week waitlist |
|
| Outcomes |
Remission of primary anxiety disorder diagnosis post‐treatment: K‐SADS Reduction in anxiety symptoms (child report) post‐treatment: SCAS‐C (modified, only 4 subscales) Reduction in anxiety symptoms (parent report) post‐treatment: SCAS‐P (modified, only 4 subscales) |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement Comment: No detail given |
| Allocation concealment (selection bias) | Unclear risk | Judgement Comment: No detail given |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Independent coder blind to treatment condition rated subset of interviews |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment:No missing data |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Report outcomes for all measures |
| Other source of bias ‐ Therapy integrity | Low risk | Judgement Comment: Trained therapists, adherence assessed and reported |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Lau 2017.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: 6 months (post‐treatment assessment); non‐controlled 12‐month follow‐up Number of study centres and location: 1 in Australia Study setting: recruited through child care centres and preschools; intervention delivery in university setting |
|
| Participants |
N = 72 (CBT: N = 39; waitlist: N = 33) Mean age (SD): 52.1 months Age range: 36 to 65 months Gender: 34 (47.2%) female Inclusion criteria: (1) age 36 to 66 months at the time of recruitment; (2) minimum of 30 (1.15 SD above the norm) on the child's score of social approach on the Short Temperament Scale for Children; (3) a minimum of 30 on at least 1 parent’s self‐reported scores on the Depression Anxiety Stress Scales; (4) no known diagnosis of any severe developmental disorders; and (5) parents who were able to complete questionnaires in English (NB: all children met diagnostic criteria for an anxiety disorder (based on ADIS‐P), but this was not an inclusion criterion) |
|
| Interventions |
CBT Intervention: parent and child intervention. Parent: Cool Little Kids. Child: Social Skills Facilitated Play programme Delivery format: parent sessions and child sessions; group Therapist contact time: 18 hours total (6 x 90 minutes ‐ parent; 6 x 90 minutes ‐ child) Who delivers the intervention: clinical psychologist (parent), graduate or final‐year students (child) Waitlist/no treatment Intervention: 6‐month waitlist |
|
| Outcomes |
Remission of all anxiety disorder diagnoses post‐treatment: ADIS‐P Reduction in anxiety symptoms (parent report‐mother) post‐treatment: Preschool Anxiety Scale‐Revised (PAS‐R) ‐ mother report |
|
| Notes | Post‐treatment assessment point 6 months | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Judgement Comment: Coin toss |
| Allocation concealment (selection bias) | Low risk | Judgement Comment: A coin toss by a research assistant who was blind to baseline assessment details was used to allocate families to the 2 conditions |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Interviewers blind to treatment condition |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: Dropouts and missing questionnaire data detailed. Only 1 dropout. Used appropriate imputation to manage missing item data. Mother report low rate missing data |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Report all outcomes |
| Other source of bias ‐ Therapy integrity | Unclear risk | Judgement Comment: Therapist qualifications detailed, but no further detail given on assessing/monitoring competence/adherence |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Lebowitz 2019.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Number of study centres and location: 1 in the USA Study setting: clinic |
|
| Participants |
N = 124 (CBT: N = 60; control: N = 64) Mean age (SD): 9.4 (2.41) Age range: 7 to 12 Gender: 66 (53%) female Inclusion criteria: primary DSM‐5 anxiety disorder diagnosis (based on ADIS‐C/P); aged 7 to 14 years; residing with mother at least 50% of the time; fluent in English; medication‐free or on a stable dose of anti‐depressant or stimulant when child and parent agreed to refrain from changes during the study period; parental informed permission and consent; child assent Exclusion criteria: drug or alcohol abuse; psychotic symptoms; autism spectrum disorder; any comorbid disorder more impairing than the most severe anxiety disorder; concurrent psychotherapy or medication, apart from stable dose of anti‐depressant or stimulant; serious suicidal intent or risk |
|
| Interventions |
CBT Intervention: manual used in Silverman 2009. Psychoeducation, exposure hierarchy, cognitive restructuring Concomitant/excluded medications: stable dose of anti‐depressant or stimulant allowed Delivery format: child only (NB: therapist met with parent to provide information on child's therapy); individual Therapist contact time: 12 hours total (12 x 1 hour) Who delivers the intervention: doctoral‐ and postdoctoral‐level psychology students Active control Intervention: SPACE (Supportive Parenting for Anxious Childhood Emotions) manual. Family modifications mapped out and target accommodation selected for modification, modules for problem‐solving difficulties related to child's responses to reduced accommodation Concomitant/excluded medications: stable dose of anti‐depressant or stimulant allowed Delivery format: parent only; individual Therapist contact time: 12 hours total (12 x 1 hour) Who delivers the intervention: doctoral‐ and postdoctoral‐level psychology students |
|
| Outcomes |
Remission of all anxiety disorder diagnoses post‐treatment: ADIS‐C/P Reduction in anxiety symptoms (child report) post‐treatment: SCARED‐C Reduction in anxiety symptoms (parent report) post‐treatment: SCARED‐P |
|
| Notes | Active control = alternative treatment | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Judgement Comment: Computerised randomisation algorithm |
| Allocation concealment (selection bias) | Low risk | Judgement Comment: Computer generated, so unlikely to foresee assignment |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Independent evaluators masked to treatment assignment |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: Focus on completer analysis justified. Report remission rates, comparison between completers and non‐completers and missing data bias |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes reported for all measures |
| Other source of bias ‐ Therapy integrity | Low risk | Judgement Comment: Trained therapists, regular supervision, fidelity checks |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Leutgeb 2012.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Number of study centres and location: 1 in Austria Study setting: university |
|
| Participants |
N = 30 (CBT: N = 16; waitlist: N = 14) Mean age (SD): CBT: 137.3 (15) months; waitlist: 138.5 (21.0) months Age range: 8 to 14 Gender: 100% female Inclusion criteria: aged 8 to 14, spider phobia (based on DIPS‐K), non‐medicated, right‐handed, female Exclusion criteria: any other mental disorder |
|
| Interventions |
CBT Intervention: Single Session CBT (OST) Concomitant/excluded medications: not allowed Delivery format: child only; individual Therapist contact time: 4 hours total Waitlist/no treatment Intervention: 1‐week waitlist Concomitant/excluded medications: not allowed |
|
| Outcomes | Reduction in anxiety symptoms (child report) post‐treatment: STAIC‐C (trait) | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement Comment: Not detailed |
| Allocation concealment (selection bias) | Unclear risk | Judgement Comment: Not detailed |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Not detailed, but no post‐treatment diagnostic assessment used |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: No missing data |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Relevant outcomes reported |
| Other source of bias ‐ Therapy integrity | Unclear risk | Judgement Comment: No detail given |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Masia Warner 2005.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: non‐controlled 9‐month follow‐up Number of study centres and location: 2 schools in the USA Study setting: schools |
|
| Participants |
N = 42 (CBT: N = 21; waitlist: N = 21) Mean age (SD): 14.8 (.81) (n = 35) Age range: 13 to 17 (n = 35) Gender: 26 (74.3%) female (n = 35) Inclusion criteria: met diagnostic criteria for DSM‐IV social anxiety disorder (based on ADIS‐C/P) Exclusion criteria: diagnosis of substance use disorder, oppositional defiant disorder, conduct disorder, or major depression that was of greater severity than social phobia; experiencing psychotic symptoms or current suicidal or homicidal thoughts; or had a current major life event requiring immediate attention (e.g. a parent dying) |
|
| Interventions |
CBT Intervention: SASS (Skills for Social and Academic Success) Concomitant/excluded medications: current pharmacological treatment excluded Delivery format: child sessions, plus parent meetings; group plus individual meetings Therapist contact time: 17.5 hours total (12 x 40 min ‐ group, 2 x 15 min ‐ individual, 4 x 90 min ‐ group social events, 2 x 45 min ‐ parent, 2 x 45 min ‐ teachers) Who delivers the intervention: clinical psychologist and clinical psychology graduate student Waitlist/no treatment Intervention: waitlist Concomitant/excluded medications: current pharmacological treatment excluded |
|
| Outcomes |
Remission of primary anxiety disorder diagnosis post‐treatment: ADIS‐C/P Reduction in anxiety symptoms (child report) post‐treatment: SPAI‐C (child) Reduction in anxiety symptoms (parent report) post‐treatment: SAS‐A (parent) Reduction in depressive symptoms post‐treatment: CDI Improvement in global functioning post‐treatment: CGAS |
|
| Notes | Anxiety symptom measures are social anxiety symptom measures. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement Comment: No detail given |
| Allocation concealment (selection bias) | Unclear risk | Judgement Comment: No detail given |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Independent blind assessors |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: Dropouts detailed. Report running completer and ITT analyses, and no differences in results |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes reported for all measures |
| Other source of bias ‐ Therapy integrity | Unclear risk | Judgement Comment: Qualified therapists, but no detail provided on assessment of competence or adherence |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Masia Warner 2007.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: 6‐month follow‐up Number of study centres and location: 2 schools in the USA Study setting: schools Withdrawals: 1 participant died after allocation and is not included in number randomised |
|
| Participants |
N = 36 (CBT: N = 19; active control: N = 17) Mean age (SD): 15.1 (0.6) Age range: 14 to 16 Gender: 30 (83.3%) female Inclusion criteria: primary social anxiety disorder (based on ADIS‐C/P) Excluded criteria: 1) current psychological or psychopharmacological treatment, 2) current diagnosis of substance use or conduct disorder, 3) concurrent mental disorder of greater severity than social phobia, and 4) psychotic symptoms or current suicidal or homicidal ideation |
|
| Interventions |
CBT Intervention: Skills for Academic and Social Success (SASS) Concomitant/excluded medications: current psychopharmacological treatment excluded Delivery format: child‐only sessions, plus parent sessions; group, plus 4 individual Therapist contact time: 17.5 hours total (12 x 40 min ‐ group, 2 x 15 min ‐ individual, 4 x 90 min ‐ group social events, 2 x 45 min ‐ parent, 2 x 45 min teachers) Who delivers the intervention: clinical psychologists and clinical psychology graduate Active control Intervention: identical professional attention and format as SASS. Psychoeducation or general relaxation techniques, support targeting social anxiety symptoms Concomitant/excluded medications: current psychopharmacological treatment excluded Delivery format: child‐only sessions, plus parent sessions; group, plus 4 individual Therapist contact time: 17.5 hours total (12 x 40 min ‐ group, 2 x 15 min ‐ individual, 4 x 90 min ‐ group social events, 2 x 45 min ‐ parent, 2 x 45 min ‐ teachers) Who delivers the intervention: clinical psychologists and clinical psychology graduates |
|
| Outcomes |
Remission of primary anxiety disorder diagnosis post‐treatment and 6‐month follow‐up: ADIS‐C/P Remission of all anxiety disorder diagnoses post‐treatment and 6‐month follow‐up: ADIS‐C/P Reduction in anxiety symptoms (child report) post‐treatment and 6‐month follow‐up: SPAI‐C Reduction in anxiety symptoms (parent report) post‐treatment and 6‐month follow‐up: SAS‐A Reduction in depressive symptoms post‐treatment: BDI‐II Improvement in global functioning post‐treatment: CGAS |
|
| Notes | Remission data reported in Warwick 2016. Anxiety symptom measures are social anxiety symptom measures. Active control = attention control |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement Comment: No detail given |
| Allocation concealment (selection bias) | Unclear risk | Judgement Comment: No detail given |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Judgement Comment: Students did not know students in other condition to prevent contamination, but no detail provided regarding whether participants were blind to receiving 'intervention' or 'control' |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Independent blind assessors |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: Dropouts detailed, completer and ITT analyses reported, with appropriate imputation |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes reported for all measures |
| Other source of bias ‐ Therapy integrity | Low risk | Judgement Comment: Qualified therapists. Measures to ensure treatment integrity |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Masia Warner 2011.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: non‐controlled 3‐month follow‐up Number of study centres and location: USA Study setting: paediatric primary care and speciality physicians |
|
| Participants |
N = 40 (CBT: N = 20; waitlist: N = 20) Mean age (SD): 12.4 (2.6) Age range: 8 to 16 Gender: 26 (65%) female Inclusion criteria: age 8 to 16 with functional physical complaints (primarily gastrointestinal symptoms) and a principal anxiety disorder (based on ADIS‐C/P), psychiatric medication allowed if receiving for 6 months and stable during intervention phase |
|
| Interventions |
CBT Intervention: TAPS (Treatment of Anxiety and Physical Symptoms). Jointly addresses anxiety and physical symptoms through identifying contexts where symptoms occur and interact Concomitant/excluded medications: children receiving psychiatric medication for more than 6 months and stable medication during intervention phase allowed Delivery format: child‐only sessions, and parent meetings; individual Therapist contact time: 11 to 14 hours (12 x 45 to 60 minutes (child), 3 x 45 minutes (parent)) Who delivers the intervention: PhD level clinical psychologists trained in CBT Waitlist/no treatment Intervention: 8‐week waitlist Concomitant/excluded medications: children receiving psychiatric medication for more than 6 months and stable medication during intervention phase allowed |
|
| Outcomes |
Remission of primary anxiety disorder diagnosis post‐treatment: ADIS‐C/P Improvement in global functioning post‐treatment: CGAS |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Judgement Comment: Table of random numbers |
| Allocation concealment (selection bias) | Unclear risk | Judgement Comment: Predetermined, but no further detail given |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Blind assessors |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: 1 dropout in control group. n reported for outcomes. |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes reported for all measures |
| Other source of bias ‐ Therapy integrity | Unclear risk | Judgement Comment: Therapist clinical psychologist with training in CBT, no detail given regarding supervision or adherence |
| Other bias | High risk | Judgement Comment: Timing post‐treatment assessment differs across groups |
Masia Warner 2016.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: recruitment over 3 academic years. 5 months follow‐up Number of study centres and location: 3 schools in the USA Study setting: schools Withdrawals: 2 removed (in P‐SASS) ‐ irregular school attendance, medical emergency (NB: relate to inclusion criteria, so not included in number randomised) |
|
| Participants |
N = 136 (CBT (C‐SASS): N = 46; CBT (P‐SASS): N = 47; active control: N = 43) Mean age (SD): 15.42 (0.81) Age range: 13 to 17 Gender: 92 (67.7%) female Inclusion criteria: diagnosis of social anxiety disorder (based on ADIS‐C/P); if other disorders present, SAD had to be of equal or greater severity Exclusion criteria: require immediate care, unreliable school attendance, receiving CBT |
|
| Interventions |
CBT (C‐SASS) Intervention: Skills for Academic and Social Success delivered by school counsellors (C‐SASS) Concomitant/excluded medications: anxiety medication allowed if stable Delivery format: child‐only sessions, plus 2 parent sessions; group, plus 2 brief individual Therapist contact time: 16 hours ‐ 12 x 40 minutes (group), 2 x 15 minutes (individual), 2 x 45 minutes (parent), 4 x 90 minutes social activities Who delivers the intervention: Master's‐level school counsellors CBT (P‐SASS) Intervention: Skills for Academic and Social Success delivered by psychologists (P‐SASS) Concomitant/excluded medications: anxiety medication allowed if stable Delivery format: child‐only sessions, plus 2 parent sessions; group, plus 2 brief individual Therapist contact time: 16 hours ‐ 12 x 40 minutes (group), 2 x 15 minutes (individual), 2 x 45 minutes (parent), 4 x 90 minutes social activities Who delivers the intervention: doctoral‐level clinical psychologists Active control Intervention: Skills for Life ‐ non‐specific counselling programme Concomitant/excluded medications: anxiety medication allowed if stable Delivery format: child‐only sessions, plus 1 parent session; group, plus 1 brief individual Therapist contact time: 9 hours (12 x 40 minutes (group), 1 x 15 minutes (individual), 1 x 45 minutes (parent)) Who delivers the intervention: Master's‐level counsellors |
|
| Outcomes |
Remission of primary anxiety disorder diagnosis post‐treatment and 5‐month follow‐up: ADIS‐C/P Reduction in anxiety symptoms (child report) post‐treatment and 5‐month follow‐up: SPAI‐C Reduction in anxiety symptoms (parent report) post‐treatment and 5‐month follow‐up: SPAI‐P |
|
| Notes | Active control = attention control Social anxiety symptom measures | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Judgement Comment: Independent randomisation |
| Allocation concealment (selection bias) | Low risk | Judgement Comment: Independent |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Judgement Comment: No detail given |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Blinded independent assessors |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: Dropouts detailed across groups, and examined differences between dropouts and completers, and completer analysis vs ITT |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes reported for all measures |
| Other source of bias ‐ Therapy integrity | Low risk | Judgement Comment: Therapist qualifications detailed, and treatment adherence assessed and reported (NB: contamination in 42% of control sessions, but with 1 exception was mild, so assume low risk of bias) |
| Other bias | Unclear risk | Judgement Comment: Amount of therapist contact time and social events not equal across conditions |
McConachie 2014.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: assessed 3 months (post‐treatment), 6 months, and 9 months Number of study centres and location: the UK Study setting: referrals from CAMHS teams in England |
|
| Participants |
N = 32 (CBT: N = 17; waitlist: N = 15) Mean age (SD): CBT: 11.7 (1.4); waitlist: 11.8 (1.3) Age range: 9 to 13 Gender: CBT: 2 (11.8%); waitlist: 2 (13.3) Inclusion criteria: child had a confirmed diagnosis of ASD, met criteria for at least 1 anxiety disorder (based on ADIS‐P), aged 9 years to 13 years 11 months with intellectual ability in the average range (full scale IQ > 69). Parent(s) also had to be willing to attend group therapy in parallel with their child. Exclusion criteria: children with untreated ADHD or oppositional behaviour that was considered likely to disrupt a small‐group setting |
|
| Interventions |
CBT Intervention: Exploring Feelings, with minor adjustments for UK setting Concomitant/excluded medications: clinician asked to avoid alteration in medication Delivery format: child and parent separate sessions; group Therapist contact time: 28 hours total (7 x 2 hours ‐ child; 7 x 2 hours ‐ parent), parent and child sessions run same time Who delivers the intervention: trainee psychologists, no prior CBT qualification Waitlist/no treatment Intervention: delayed treatment, 9 months wait (assessment 3 months, 6 months, 9 months) Concomitant/excluded medications: clinician asked to avoid alteration in medication |
|
| Outcomes |
Remission of primary anxiety disorder diagnosis post‐treatment: ADIS‐P Remission of all anxiety disorder diagnoses post‐treatment: ADIS‐P Reduction in anxiety symptoms (child report) post‐treatment: SCAS‐C Reduction in anxiety symptoms (parent report) post‐treatment: SCAS‐P |
|
| Notes | 6‐ and 9‐month follow‐up anxiety symptoms outcomes reported, but only change scores. Sample with ASD | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Judgement Comment: Random permuted blocks of variable length (www.randomization.com) |
| Allocation concealment (selection bias) | Low risk | Judgement Comment: Measures to ensure concealed allocation |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Blind assessors |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: Attrition detailed. Only 1 dropout. Use last observation carried forward for this case for questionnaires |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes reported for all measures |
| Other source of bias ‐ Therapy integrity | Low risk | Judgement Comment: Therapists trained and supervised, and fidelity assessed and reported |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
McNally Keehn 2013.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: non‐controlled 2‐month follow‐up Number of study centres and location: 1 in the USA Study setting: university clinic Date of study: June to September 2009; post‐ and follow‐up assessments completed by April 2010 |
|
| Participants |
N = 22 (CBT: N = 12; waitlist: N = 10) Mean age (SD): 11.26 (1.53) Age range: 8 to 14 Gender: 1 (4.5%) female Inclusion criteria: a) diagnosis of ASD based on the Autism Diagnostic Observation Schedule (ADOS), Autism Diagnostic Interview‐Revised (ADI‐R), and expert clinical judgement based on DSM‐IV criteria, (b) diagnosis of separation anxiety disorder, social phobia, or GAD (based on ADIS‐P), c) IQ > 70, d) age 7 to 14, and e) English as the primary language |
|
| Interventions |
CBT Intervention: Modified Coping Cat to accommodate learning styles of ASD Concomitant/excluded medications: usual medication allowed Delivery format: child sessions, plus 2 parent sessions; individual Therapist contact time: 16 to 24 hours (16 x 60 to 90 minutes) Who delivers the intervention: lead author Waitlist/no treatment Intervention: 16‐week waitlist Concomitant/excluded medications: usual medication allowed |
|
| Outcomes |
Remission of primary anxiety disorder diagnosis post‐treatment: ADIS‐P Reduction in anxiety symptoms (child report) post‐treatment: SCAS‐C Reduction in anxiety symptoms (parent report) post‐treatment: SCAS‐P |
|
| Notes | Author provided data on remission for separation anxiety disorder, social phobia, and GAD, not able to use. Sample with ASD |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Judgement Comment: Block randomised, stratified |
| Allocation concealment (selection bias) | Unclear risk | Judgement Comment: No detail given |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Blind assessors |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: Detailed no dropouts to post‐treatment |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes reported for all measures |
| Other source of bias ‐ Therapy integrity | Low risk | Judgement Comment: Adherence rated and reported |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Melfsen 2011.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: 10‐month follow‐up for treatment group (6 months post‐treatment) Number of study centres and location: 1 in Germany Study setting: clinic Date of study: recruitment 2004 to 2006 |
|
| Participants |
N = 44 (CBT: N = 21; waitlist: N = 23) Mean age (SD): CBT: 10.60 (1.64); waitlist: 10.76 (1.90) Age range: 8 to 14 Gender: 21 (47.8%) female Inclusion criteria: a) DSM‐IV criteria for social phobia (based on DIPS‐K), (b) child experienced social phobia for at least 6 months, (c) social phobia was considered to be the child’s main current problem, (d) child age 8 to 13 years, (e) child and parent agreed not to start any additional treatment during the trial Exclusion criteria: psychotic symptoms, current suicidal or self‐harming behaviour, or current involvement in other psychosocial or psychopharmacological treatment for phobia and anxiety problems |
|
| Interventions |
CBT Intervention: psychoeducation, cognitive restructuring, behavioural experiments, relapse Concomitant/excluded medications: psychopharmacological treatment not allowed Delivery format: child and parent sessions; individual Therapist contact time: 20 hours (20 x 50 minutes, 4 x parent sessions) Who delivers the intervention: advanced doctoral‐level graduate students Waitlist/no treatment Intervention: 4‐month waitlist Concomitant/excluded medications: psychopharmacological treatment not allowed |
|
| Outcomes |
Remission of primary anxiety disorder diagnosis post‐treatment: DIPS‐K Remission of all anxiety disorder diagnoses post‐treatment: DIPS‐K Reduction in anxiety symptoms (child report) post‐treatment: SPAIK‐C Reduction in depressive symptoms post‐treatment: CDI Improvement in global functioning post‐treatment: K‐GAS |
|
| Notes | Refer to follow‐up but do not report follow‐up data | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Judgement Comment: Web‐based computerised randomisation plan generator |
| Allocation concealment (selection bias) | Low risk | Judgement Comment: Independent research assistant placed participants on randomisation list in next available slot |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Assessor not blind, but video recordings of assessments viewed and rated by blind expert |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: Attrition detailed and use appropriate imputation, and report ITT |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Relevant outcomes reported. Not report follow up data for intervention group, but the follow‐up h as no comparison group so would not be eligible for inclusion here |
| Other source of bias ‐ Therapy integrity | Low risk | Judgement Comment: Therapy delivered by advanced doctoral graduates, adherence assessed |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Muris 2002.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Number of study centres and location: 2 primary schools in the Netherlands Study setting: primary schools |
|
| Participants |
N = 20 (CBT: N = 10; control: N = 10) (NB: study also includes 10 participants (not randomly) assigned to no treatment control, not included here) Mean age (SD): 10 (0.8) Age range: 9 to 12 Gender: 13 (65%) female Inclusion criteria: elevated RCADS score; generalised anxiety disorder, separation anxiety disorder, or social phobia diagnosis (based on DISC) |
|
| Interventions |
CBT Intervention: Coping Koala Delivery format: child only; group Therapist contact time: 6 hours (12 x 30 minutes) Who delivers the intervention: clinical psychology student Active control Intervention: Emotional Disclosure Delivery format: child only; group Therapist contact time: 6 hours (12 x 30 minutes) Who delivers the intervention: clinical psychology student |
|
| Outcomes |
Reduction in anxiety symptoms (child report) post‐treatment: RCADS‐C Anxiety Scale Reduction in depressive symptoms post‐treatment: RCADS‐C‐Depression Scale |
|
| Notes | Participants randomised to CBT vs active control. Study also includes no treatment control, but non‐randomised allocation so not included here. Active control = attention control |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement Comment: No detail given |
| Allocation concealment (selection bias) | Unclear risk | Judgement Comment: No detail given |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Judgement Comment: No detail given |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Questionnaires administered by psychologist not involved in treatment |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: Reports no dropouts |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes reported for measures |
| Other source of bias ‐ Therapy integrity | Unclear risk | Judgement Comment: Therapist supervised, but no detail given on maintaining adherence |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Murphy 2017.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: 12‐week follow‐up Number of study centres and location: 3 CAMHS clinics in the UK Study setting: clinics Date of study: recruitment April 2011 to April 2013 |
|
| Participants |
N = 36 (CBT: N = 17; active control: N = 19) Mean age (SD): CBT: 14.94 (1.63); active control: 15.56 (1.91) Age range: 12 to 18 Gender: 14 (38.9%) female Inclusion criteria: ASD and anxiety disorder diagnoses (separation anxiety, social anxiety, specific phobia, and/or generalised anxiety) based on ADOS, ADI‐R, ADIS‐C/P); attend mainstream school Exclusion criteria: primary diagnosis OCD, agoraphobia with/without panic disorder, PTSD, psychosis, depression, substance abuse; receipt of current psychological therapy from another source |
|
| Interventions |
CBT Intervention: Multimodal Anxiety and Social Skill Intervention for adolescents with ASD (MASSI). CBT for anxiety, plus strategies targeting social skills deficits Concomitant/excluded medications: not alter medication doses during intervention Delivery format: child only, parents included at end of all sessions; individual and group Therapist contact time: 10 hours (plus group sessions) (12 x 50 minutes individual sessions) Who delivers the intervention: NHS clinicians Active control Intervention: counselling offered in the NHS dealt with anxiety as and when the client raised it, in a supportive manner, but with no focus on physical symptoms or cognitions Concomitant/excluded medications: not alter medication doses during intervention Delivery format: child only, parents included at end of all sessions; individual and group Therapist contact time: 10 hours (plus group sessions) (12 x 50 minutes individual sessions) Who delivers the intervention: NHS clinicians |
|
| Outcomes | Reduction in anxiety symptoms (parent report) post‐treatment and follow‐up (< 6 months): CASI‐ASD Anxiety Scale | |
| Notes | Diagnostic assessment post‐treatment but not required remission data Sample with ASD Active control = alternative treatment (counselling) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Judgement Comment: Predetermined random sequence by an independent statistician |
| Allocation concealment (selection bias) | Low risk | Judgement Comment: Randomisation was managed by a statistician unconnected with the study who prepared sequentially numbered envelopes containing allocation status |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Judgement Comment: No detail given regarding blinding of participants |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Blind assessors |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: Attrition detailed. ITT analyses reported, and method for managing missing data. |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes reported |
| Other source of bias ‐ Therapy integrity | Low risk | Judgement Comment: Qualified therapists. Fidelity assessed and reported. |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
O'Brien 2007.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: 10 weeks; end of 10 weeks TAU group offered CBT Number of study centres and location: 1 in Ireland Study setting: clinic |
|
| Participants |
N = 14 (CBT: N = 7; TAU: N = 7) Mean age (SD): CBT: 13.8 (0.5); TAU: 12.5 (1.0) Age range: 7 to 15 Gender: 7 (50%) female Inclusion criteria: diagnosis of DSM‐IV‐R anxiety disorder (based on ADIS) Exclusion criteria: children with intellectual disabilities, pervasive developmental disorder, or recent history of psychotic symptoms |
|
| Interventions |
CBT Intervention: group CBT: Friends for Youth Concomitant/excluded medications: stable dose allowed Delivery format: child sessions and parent sessions; group Therapist contact time: 19.5 hours (10 x 90 minutes ‐ child; 3 x 90 minutes ‐ parent) Who delivers the intervention: mental health professionals, and supervised by main author TAU Intervention: 10 weeks TAU. Received maximum of 4 reviews with primary clinician ‐ review of progress, medication, and supportive approach Concomitant/excluded medications: stable dose allowed Delivery format: individual Therapist contact time: maximum of 4 sessions Who delivers the intervention: primary clinician |
|
| Outcomes | Reduction in depressive symptoms post‐treatment: CDI | |
| Notes | Anxiety symptoms outcomes only reported after both groups received CBT intervention. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement Comment: Sequence generation lacks detail, and unclear how age managed in the process |
| Allocation concealment (selection bias) | Unclear risk | Judgement Comment: Refers to person doing randomisation being blind, but further detail is lacking |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Not detailed, but no post‐treatment diagnostic assessment |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: Data reported |
| Selective reporting (reporting bias) | Unclear risk | Judgement Comment: Did not report outcomes for all measures at post‐assessment separately for 2 groups |
| Other source of bias ‐ Therapy integrity | Low risk | Judgement Comment: Experienced supervisors. Sessions recorded to monitor and ensure adherence, although lacking detail on how adherence was assessed |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Olivares 2005.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: 6‐month follow‐up Number of study centres and location: Spain Study setting: schools (screening) |
|
| Participants |
N = 34 (CBT: N = 17; waitlist: N = 17) Mean age (SD): 15.03 (0.86) Age range: 14 to 17 Gender: 60% female Inclusion criteria: diagnosis of social phobia (based on ADIS‐C) |
|
| Interventions |
CBT Intervention: IAFS (multicomponent programme: Intervention in Adolescents with Social Phobia) Delivery format: child only; group Therapist contact time: 18 hours (12 x 90 minutes) Waitlist/no treatment Intervention: waitlist |
|
| Outcomes |
Remission of primary anxiety disorder diagnosis post‐treatment and 6‐month follow‐up: ADIS‐C Remission of all anxiety disorder diagnoses post‐treatment and 6‐month follow‐up: ADIS‐C Reduction in anxiety symptoms (child report) post‐treatment and 6‐month follow‐up: SPAI‐C |
|
| Notes | Anxiety symptoms measure ‐ social anxiety symptoms | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement Comment: No detail given |
| Allocation concealment (selection bias) | Unclear risk | Judgement Comment: No detail given |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Independent assessor carried out diagnostic interview and evaluation |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: No missing data |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes reported for all measures |
| Other source of bias ‐ Therapy integrity | Unclear risk | Judgement Comment: Lacks detail |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Olivares 2014.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Number of study centres and location: 9 high schools in Spain Study setting: schools |
|
| Participants |
N = 117 (CBT (expert): N = 39; CBT (inexperienced): N = 39; waitlist: N = 39) Mean age (SD): 15.42 (0.97) Age range: 14 to 17 Gender: 61.8% female Inclusion criteria: generalised social phobia (based on ADIS‐C) Exclusion criteria: depression, borderline personality disorder, narcissistic disorder, paranoid disorder, long history of substance abuse, aggressive behaviour, missing 3 consecutive treatment sessions, and have not previously received psychological treatment |
|
| Interventions |
CBT (expert) Intervention: IAFS (multicomponent programme: Intervention in Adolescents with Social Phobia) Delivery format: child only; group Therapist contact time: 18 hours (12 x 90 minutes) Who delivers the intervention: clinical psychologists (degree in psychology) with more than 2 years' experience treating individual cases and applying psychological treatment to groups with social anxiety CBT (inexperienced) Intervention: IAFS (multicomponent programme: Intervention in Adolescents with Social Phobia) Delivery format: child only; group Therapist contact time: 18 hours (12 x 90 minutes) Who delivers the intervention: psychologists (degree in psychology) with no experience in applying psychological treatment Waitlist/no treatment Intervention: waitlist |
|
| Outcomes |
Remission of primary anxiety disorder diagnosis post‐treatment: ADIS‐C Reduction in anxiety symptoms (child report) post‐treatment: SAS‐A Reduction in anxiety symptoms (parent report) post‐treatment: SAS‐P |
|
| Notes | Anxiety symptoms measures ‐ social anxiety symptoms | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement Comment: No detail given |
| Allocation concealment (selection bias) | Unclear risk | Judgement Comment: No detail given |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Judgement Comment: Evaluators trained, and therapist competence masked, but does not specify if blind to waitlist vs treatment |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Judgement Comment: Attrition given, but only reports completer analyses. No mention of how missing item data were managed |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes reported for all measures |
| Other source of bias ‐ Therapy integrity | Low risk | Judgement Comment: Fidelity measured |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Olivares 2019.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: non‐controlled follow‐up Number of study centres and location: 7 schools in Spain Study setting: high schools |
|
| Participants |
N = 108 randomised (CBT‐IAFS: N = 36; CBT‐IAFS without social skills training: N = 36; waitlist: N = 36) Mean age: 15.4 (1.11) Age range: 14 to 17 Gender: 63% female Inclusion criteria: met diagnostic criteria for generalised social phobia (based on ADIS‐C) Exclusion criteria: no written parental consent, met diagnostic criteria for severe psychopathology (e.g. depression or narcissistic disorder), long history of substance abuse, aggressive behaviour, missing 3 consecutive treatment sessions, and have not previously received psychological or psychiatric treatment |
|
| Interventions |
CBT Intervention: IAFS (Intervention in Adolescents with Social Phobia) Delivery format: child only; group Therapist contact time: 18 hours (12 x 90 minutes) Who delivers the intervention: psychology graduates CBT Intervention: IAFS without social skills training Delivery format: child only; group Therapist contact time: 18 hours (12 x 90 minutes) Who delivers the intervention: psychology graduates Waitlist/no treatment Intervention: waitlist |
|
| Outcomes | Remission of primary anxiety disorder diagnosis post‐treatment: ADIS‐C | |
| Notes | Symptom measures only reported pre‐post change. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement Comment: No detail |
| Allocation concealment (selection bias) | Unclear risk | Judgement Comment: No detail |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Independent assessors |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Judgement Comment: High number of dropouts in 1 CBT group |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes reported for relevant measure |
| Other source of bias ‐ Therapy integrity | Unclear risk | Judgement Comment: Experienced therapists, no further detail |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Ollendick 2009.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: 6‐month follow‐up Number of study centres and location: 2; Sweden and the USA Study setting: clinics Date of study: 2001 to 2006 |
|
| Participants |
N = 196 (CBT: N = 85; active control: N = 70; waitlist: N = 41) Mean age (SD): Virginia site: 10.9 (1.7); Stockholm site: 11.1 (1.9) Age range: 7 to 16 Gender: 106 (43.3%) Inclusion criteria: age 7 to 16; specific phobia diagnosis, present for 6 months with CSR 4+ (based on ADIS‐C/P); discontinue other psychotherapy or anti‐anxiety medication for duration of study Exclusion criteria: primary major depression, pervasive developmental disorder, drug or alcohol abuse, psychotic symptoms |
|
| Interventions |
CBT Intervention: One Session Treatment (OST) (follow Ost, but flexibly implemented) Concomitant/excluded medications: anti‐anxiety treatment not allowed Delivery format: child only; individual Therapist contact time: 3 hours 45 minutes (pretreatment interview 45 minutes, treatment 3 hours) Who delivers the intervention: clinicians with at minimum a Master's degree, trained Active control Intervention: education support therapy Concomitant/excluded medications: anti‐anxiety treatment not allowed Delivery format: child only; individual Therapist contact time: 3 hours Who delivers the intervention: clinicians with at minimum a Master's degree, trained Waitlist/no treatment Intervention: 4‐week waitlist Concomitant/excluded medications: anti‐anxiety treatment not allowed |
|
| Outcomes |
Remission of primary anxiety disorder diagnosis post‐treatment: ADIS‐C/P (mini version to assess pretreatment diagnoses) Reduction in anxiety symptoms (child report) post‐treatment: MASC‐C Reduction in depressive symptoms post‐treatment: CDI |
|
| Notes | Author confirmed diagnosis free = free from primary disorder Reported no adverse events during treatment Active control = attention control Symptom measures reported for each site separately. Follow‐up includes waitlist participants re‐randomised to OST vs active control CBT vs waitlist and CBT vs active control (did not divide CBT group as included in separate comparisons) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Judgement Comment: Computerised randomisation procedures or random number generators |
| Allocation concealment (selection bias) | Low risk | Judgement Comment: Randomisation assignments were kept in opaque envelopes that remained unopened until the time of assignment |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Judgement Comment: Did not specify whether participants were blind to 'active' vs 'control' treatment |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Blind assessors |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: No dropouts |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes reported for all measures |
| Other source of bias ‐ Therapy integrity | Low risk | Judgement Comment: Therapists trained, supervised, and adherence and competence monitored |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Ost 2001.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Number of study centres and location: Sweden Study setting: referrals from child psychiatric services and school services |
|
| Participants |
N = 60 (CBT (child): N = 21; CBT (child + parent) N = 20; waitlist: N = 19) Mean age (SD): 11.7 (2.8) Age range: 7 to 17 Gender: 37 (61%) female Inclusion criteria: aged 7 to 17, primary specific phobia, with CSR 4+ and present for minimum of 1 year (based on ADIS‐C/P), be motivated for treatment Exclusion criteria: primary depression, drug or substance abuse, developmental disorder, psychotic symptoms |
|
| Interventions |
CBT (child) Intervention: One Session Treatment (OST), adjusted to developmental age Delivery format: child only; individual Therapist contact time: 3 hours 45 minutes (pretreatment interview ‐ 45 minutes, treatment ‐ 3 hours) Who delivers the intervention: experienced clinical psychologist, experienced in treating specific phobias with CBT CBT (child + parent) Intervention: One Session Treatment (OST), adjusted to developmental age. Same as child condition, only parent present too Delivery format: child and parent; individual Therapist contact time: 3 hours 45 minutes (pretreatment interview ‐ 45 minutes, treatment ‐ 3 hours) Who delivers the intervention: experienced clinical psychologist, experienced in treating specific phobias with CBT Waitlist/no treatment Intervention: 4‐week waitlist |
|
| Outcomes |
Remission of primary anxiety disorder diagnosis post‐treatment: ADIS‐C/P (mini version to assess pretreatment diagnoses) Reduction in anxiety symptoms (child report) post‐treatment: RCMAS Reduction in depressive symptoms post‐treatment: CDI |
|
| Notes | Author provided remission of all diagnoses for those with pretreatment diagnoses only. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement Comment: No detail given |
| Allocation concealment (selection bias) | Unclear risk | Judgement Comment: No detail given |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Assessors blind to condition |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: Not clear if there were dropouts/missing data/approach to managing missing data, but author provided data |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes reported for measures |
| Other source of bias ‐ Therapy integrity | Unclear risk | Judgement Comment: Experienced therapists, but no detail given on assessing adherence |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Perrin 2019.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: 10‐week treatment period; 3‐month non‐controlled follow‐up Number of study centres and location: referrals from 11 sites in 1 NHS Trust in the UK Study setting: referral from CAMHS services and specialist anxiety clinician at NHS Trust |
|
| Participants |
N = 40 (CBT: N = 20; waitlist: N = 20) Mean age (SD): CBT: 13.2 (2.4); waitlist: 13.6 (2.8) Age range: 10 to 18 Gender: 25 (62.5%) female Inclusion criteria: (1) aged 10 to 18 years; (2) referred for treatment of anxiety; (3) a current, primary diagnosis of DSM‐IV GAD (Based on ADIS‐C/P); (4) no other psychiatric problems in need of more urgent treatment (including self‐injurious thoughts/behaviours or substance use/abuse); (5) no concurrent psychological or pharmacological treatment for any disorder; and (6) the absence of moderate to severe learning difficulties as evidenced in the medical or school records or as reported by the referrer/parent at the pretrial screening |
|
| Interventions |
CBT Intervention: child‐friendly adaptation of CBT for GAD approach Concomitant/excluded medications: concurrent pharmacological treatment for any disorder not allowed Delivery format: child only, parent invited to join for 1 session and to join end of sessions; individual Therapist contact time: 10 sessions Who delivers the intervention: doctoral‐level clinical psychologists Waitlist Intervention: 10‐week waitlist Concomitant/excluded medications: concurrent pharmacological treatment for any disorder not allowed |
|
| Outcomes |
Remission of primary anxiety disorder diagnosis post‐treatment: ADIS‐C/P Remission of all anxiety disorder diagnoses post‐treatment: ADIS‐C/P Reduction in anxiety symptoms (child report) post‐treatment: SCARED‐C Reduction in anxiety symptoms (parent report) post‐treatment: SCARED‐P Reduction in depressive symptoms post‐treatment: MFQ‐C Improvement in global functioning post‐treatment: CGAS |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Judgement Comment: Online random allocation program |
| Allocation concealment (selection bias) | Low risk | Judgement Comment: Online random allocation program created by CTU, allocation after initial assessment |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Independent blind assessors |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: Attrition low and detailed. Report ITT |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes reported for all measures |
| Other source of bias ‐ Therapy integrity | Low risk | Judgement Comment: Trained and supervisor therapist. Adherence assessed |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Pincus 2010.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Number of study centres and location: 1 in the USA Study setting: university research clinic |
|
| Participants |
N = 26 (CBT: N = 13; active control: N = 13) Mean age (SD): 15.75 (1.10) Age range: 14 to 17 Gender: 19 (73.1%) female Inclusion criteria: panic disorder diagnosis, with or without agoraphobia, CSR 4+ (based on ADIS‐C/P) |
|
| Interventions |
CBT Intervention: Panic Treatment Programme (PCT‐A) downward extension of Panic Control Treatment Concomitant/excluded medications: stabilisation period prior to assessment required Delivery format: child sessions, with parent included in some sessions; individual Therapist contact time: 9 hours (11 x 50 minutes) Active control Intervention: attention control. 8‐week self‐monitoring, meet with therapist every other week to discuss self‐monitoring panic and anxiety Concomitant/excluded medications: stabilisation period prior to assessment required Delivery format: child only; individual Therapist contact time: 2 hours (4 x 30 minutes) |
|
| Outcomes |
Reduction in anxiety symptoms (child report) post‐treatment: MASC‐C Reduction in depressive symptoms post‐treatment: CDI |
|
| Notes | Use mini‐ADIS post‐treatment. Remission outcomes not reported/provided. Active control = attention control |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement Comment: No detail given |
| Allocation concealment (selection bias) | Unclear risk | Judgement Comment: No detail given |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Judgement Comment: Not specified |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Judgement Comment: Attrition and how missing data managed detailed, but high rate of missing data (24% for questionnaires) |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes reported |
| Other source of bias ‐ Therapy integrity | Low risk | Judgement Comment: Adherence assessed by independent raters and reported |
| Other bias | High risk | Judgement Comment: Time point for post‐treatment assessment varies across conditions |
Rapee 2005.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: 11‐year follow‐up Number of study centres and location: Australia Study setting: screening in 95 preschools |
|
| Participants |
N = 146 randomised (NB: we included N = 111 who met diagnostic criteria for an anxiety disorder at baseline. CBT: N = 60; no intervention: N = 51) Mean age (SD): CBT: 47.23 (5.08); no intervention: 45.71 (4.15) Age range: 36 to 62 months Gender: 64 (57.7%) female Inclusion criteria: inhibited children (score > 1.5 SD above mean) and met for behavioural inhibition on the lab assessment. We only included children who met diagnostic criteria in the review. |
|
| Interventions |
CBT Intervention: parent education. Nature of anxiety, parent management, exposure, cognitive restructuring for parent, apply cognitive principles with child Delivery format: parent only, group Therapist contact time: 9 hours (6 x 90 minutes) Who delivers the intervention: clinical psychologist No treatment Intervention: monitor condition. No intervention |
|
| Outcomes |
Remission of all anxiety disorder diagnoses post‐treatment: ADIS‐P Reduction in anxiety symptoms (parent report) post‐treatment: Preschool Anxiety Scale |
|
| Notes | We only included children who met diagnostic criteria for an anxiety disorder at baseline. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement Comment: No detail given |
| Allocation concealment (selection bias) | Unclear risk | Judgement Comment: No detail given |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Blind assessors |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: Author provided data |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes reported/provided |
| Other source of bias ‐ Therapy integrity | Unclear risk | Judgement Comment: Experienced therapist delivered intervention. No further detail |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Rapee 2006.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Number of study centres and location: 1 in Australia Study setting: university clinic Date of study: recruitment 1999 to 2002 |
|
| Participants |
N = 267 randomised (NB: we included N = 177, randomised to CBT: N = 90; waitlist: N = 87) Mean age (SD): CBT: 113.7 months (20.4); waitlist: 114.1 months (19.1) Age range: 6 to 12 Gender: CBT: 52.3% female; waitlist: 29.9% female Inclusion criteria: year 1 to 6 at school (age 6 to 12), primary anxiety disorder (based on ADIS‐C/P), parent able to read standard English newspaper |
|
| Interventions |
CBT Intervention: Cool Kids Concomitant/excluded medications: stable dose for month before allowed Delivery format: child and parent sessions, group Therapist contact time: 18 hours (9 x 2 hours) Who delivers the intervention: graduate students in clinical psychology Waitlist/no treatment Intervention: 3‐month waitlist Concomitant/excluded medications: stable dose for month before allowed |
|
| Outcomes |
Remission of primary anxiety disorder diagnosis post‐treatment: ADIS‐C/P Remission of all anxiety disorder diagnoses post‐treatment: ADIS‐C/P Reduction in anxiety symptoms (child report) post‐treatment: SCAS‐C Reduction in anxiety symptoms (parent report) post‐treatment: SCAS‐P |
|
| Notes | Trial included "bibliotherapy" arm (parent‐only condition with no face‐to‐face contact, so not included). Report no adverse events during treatment |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Judgement Comment: Block randomisation, random number schedule |
| Allocation concealment (selection bias) | Low risk | Judgement Comment: Random number schedule known only to study co‐ordinator |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Blind to treatment condition |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: Dropouts detailed. ITT and completer analysis provided, including appropriate method for imputing missing data. |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes reported for all measures |
| Other source of bias ‐ Therapy integrity | Unclear risk | Judgement Comment: Experienced therapist. No detail on adherence |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Reaven 2012.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: 4‐month intervention period Number of study centres and location: 1 in the USA Study setting: research clinic |
|
| Participants |
N = 50 (CBT: N = 24; TAU: N = 26) Mean age (SD): CBT: 125.75 months (21.47); TAU: 125.00 months (20.45) Age range: 7 to 14 Gender: 48 (96%) female Inclusion criteria: age 7 to 14; diagnosis of an ASD (determined by expert clinical psychologists based upon review of a recent ADOS and the Social Communication Questionnaire); speaking in full, complex sentences, and as reflected in recent standardised cognitive assessment, and clinically significant symptoms of anxiety (NB: include ADIS‐P and participants met diagnostic criteria) Excluded criteria: primary psychiatric symptoms reflective of another condition such as depression or psychosis; child does not demonstrate “group readiness” in the first 3 sessions of Facing Your Fears; 1 parent could not commit to attending 80% of sessions |
|
| Interventions |
CBT Intervention: Facing Your Fears. Adapted CBT programme for children with ASD Concomitant/excluded medications: medications allowed Delivery format: child and parent together, group Therapist contact time: 18 hours (12 x 90 minutes) Who delivers the intervention: clinical psychologist and co‐therapists TAU Intervention: maintained current interventions and allowed to pursue new interventions for 4 months Concomitant/excluded medications: medications allowed |
|
| Outcomes |
Remission of primary anxiety disorder diagnosis post‐treatment: ADIS‐P Remission of all anxiety disorder diagnoses post‐treatment: ADIS‐P |
|
| Notes | Use data published in Warwick 2016 review Sample with ASD |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Judgement Comment: Computer generated |
| Allocation concealment (selection bias) | Low risk | Judgement Comment: Computer generated, so unlikely to foresee assignment |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Blind assessors |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: Attrition detailed, report ITT. Diagnostic outcomes only relevant outcome |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes reported/available for relevant measure |
| Other source of bias ‐ Therapy integrity | Low risk | Judgement Comment: Trained therapists, regular supervision, adherence assessed and reported |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Reigada 2015.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: 3‐month follow‐up Number of study centres and location: 1 in the USA Study setting: university clinic |
|
| Participants |
N = 22 (CBT: N = 11; active control: N = 11) Mean age (SD): 13.2 (2.1) Age range: 9 to 17 Gender: 13 (59.1%) female Inclusion criteria: confirmed inflammatory bowel disease (IBD) diagnosis and met diagnostic criteria for a DSM‐IV anxiety disorder (based on ADIS‐C/P) Exclusion criteria: current suicidal thoughts requiring immediate clinical attention; current use of a psychotropic medication prescribed within the last 2 months; current substance use disorder, conduct disorder, or pervasive developmental disorder; schizophrenia or other psychosis; a history of or current bipolar disorder; or a principal diagnosis of post‐traumatic stress disorder |
|
| Interventions |
CBT Intervention: Treatment of Anxiety and Physical symptoms related to IBD (TAPS + IBD) Concomitant/excluded medications: current use of a psychotropic medication prescribed within the last 2 months excluded Delivery format: child sessions and 3 parent sessions; individual Therapist contact time: 16 hours (13 x 1 hour; 3 x 1‐hour parent sessions) Who delivers the intervention: clinical psychology doctoral students Active control Intervention: non‐directive supportive therapy. Offered social and emotional support through the use of non‐directive techniques (e.g. reflection, summarisation), empathetic communication, and supportive statements Concomitant/excluded medications: current use of a psychotropic medication prescribed within the last 2 months excluded Delivery format: child sessions and parent sessions; individual Therapist contact time: 16 hours (13 x 1 hour; 3 x 1‐hour parent sessions) Who delivers the intervention: clinical psychology doctoral students |
|
| Outcomes |
Remission of primary anxiety disorder diagnosis post‐treatment and 3‐month follow‐up: ADIS‐C/P Remission of all anxiety disorder diagnoses post‐treatment and 3‐month follow‐up: ADIS‐C/P Reduction in anxiety symptoms (child report) post‐treatment and 3‐month follow‐up: IBD‐Specific Anxiety Scale |
|
| Notes | Anxiety symptom measure measure of anxiety related to IBD symptoms Active control = alternative treatment |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Judgement Comment: Random number charts |
| Allocation concealment (selection bias) | Unclear risk | Judgement Comment: No detail given |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Judgement Comment: No detail on participant blinding |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Blind independent evaluators |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: Attrition and missing data detailed. Detailed method of managing missing data to report ITT analyses |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes reported for all measures |
| Other source of bias ‐ Therapy integrity | Low risk | Judgement Comment: Therapists trained and supervised. Adherence and contamination in control assessed and reported |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Rosa Alcazar 2009.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: 6‐ and 12‐month follow‐up Number of study centres and location: Spain Study setting: schools (screening) |
|
| Participants |
N = 77 (CBT: N = 20; active control (psychoeducation): N = 19; active control: N = 18; waitlist: N = 20) Mean age (SD): 14.87 (0.80) Age range: 14 to 17 Gender: 75% female Inclusion criteria: generalised social phobia diagnosis (based on ADIS‐C), parental consent |
|
| Interventions |
CBT Intervention: IAFS (Intervención en Adolescentes con Fobia Social) Delivery format: child only; group Therapist contact time: 18 hours (12 x 90 minutes) Who delivers the intervention: therapists Active control Intervention: psychoeducation Delivery format: child only; group Therapist contact time: 18 hours (12 x 90 minutes) Who delivers the intervention: therapists Active control Intervention: health education Concomitant/excluded medications: Delivery format: child only; group Therapist contact time: 18 hours (12 x 90 minutes) Who delivers the intervention: therapists Waitlist/no treatment Intervention: waitlist |
|
| Outcomes |
Remission of primary anxiety disorder diagnosis post‐treatment, 6‐month and 12‐month follow‐up: ADIS‐C Remission of all anxiety disorder diagnoses post‐treatment, 6‐month and 12‐month follow‐up: ADIS‐C Reduction in anxiety symptoms (child report) post‐treatment, 6‐month and 12‐month follow‐up: SPAIC Reduction in anxiety symptoms (parent report) post‐treatment, 6‐month and 12‐month follow‐up: SAS‐P |
|
| Notes | Active controls = attention controls Comparisons: CBT (split CBT group) vs active control, CBT (split CBT group) vs active control, CBT (total CBT group) vs waitlist Anxiety symptoms measures social anxiety symptom measures |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement Comment: Lack of detail |
| Allocation concealment (selection bias) | Unclear risk | Judgement Comment: No detail |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Judgement Comment: No detail |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Judgement Comment: Lack of detail |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: Author provided data |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes reported/provided for all relevant measures |
| Other source of bias ‐ Therapy integrity | Unclear risk | Judgement Comment: Lack of detail |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Salari 2018.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Number of study centres and location: 1 in Iran Study setting: university‐affiliated outpatient clinic |
|
| Participants |
N = 42 (CBT: N = 20; waitlist: N = 22) Mean age (SD): CBT: 8.5 (2.5); waitlist: 8.1 (1.9) Age range: 6 to 12 Gender: CBT: 47.4% female; waitlist: 21.4% female Inclusion criteria: DSM‐IV criteria for primary diagnosis of GAD, separation anxiety disorder, social phobia, or specific phobia (based on K‐SADS), 1 SSRI (Selective Serotonin Reuptake Inhibitor) medicine at a stable dose for at least 8 weeks before baseline Excluded criteria: 1) diagnosed as major psychiatric/neurologic disorders; 2) change in medication during the study; 3) parents missed more than 2 of 6 sessions of treatment |
|
| Interventions |
CBT Intervention: parent training ‐ group CBT "Friends for life" (parent‐training element, translated version) Concomitant/excluded medications: a stable dose of SSRI for at least 8 weeks before baseline allowed Delivery format: parent only; group Therapist contact time: 12 hours (6 x 2 hours) Who delivers the intervention child psychiatrist and co‐led by a fellow of child psychiatry Waitlist/no treatment Intervention: 6‐week waitlist Concomitant/excluded medications: a stable dose of SSRI for at least 8 weeks before baseline |
|
| Outcomes |
Reduction in anxiety symptoms (child report) post‐treatment: RCMAS Reduction in depressive symptoms post‐treatment: CDI Improvement in global functioning post‐treatment: CGAS |
|
| Notes | Author confirmed no diagnostic assessment post‐treatment. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement Comment: No information provided |
| Allocation concealment (selection bias) | Unclear risk | Judgement Comment: No information provided |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: No information provided, but no post‐treatment diagnostic assessment used |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: Did not include participants who missed more than 2 sessions, which is a potential source of bias. 25% dropout in CBT group, but author provided data |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Did not report diagnostic outcomes, but author confirmed no diagnostic assessment post‐treatment |
| Other source of bias ‐ Therapy integrity | Unclear risk | Judgement Comment: Treatment delivery by psychiatrist. Refer to adherence ratings, but no further detail reported |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Salum 2018.
| Study characteristics | ||
| Methods |
Study design: factorial randomised controlled trial Number of study centres and location: Brazil Date of study: recruitment from July 2011 to September 2012 Withdrawals: N = 96 originally randomised, but 17 withdrew before first session and were not aware of allocation ‐ not included |
|
| Participants |
N = 79 (CBT + Attention Bias Modification N = 21; CBT + Attention Control Training: N = 21; active control therapy + Attention Bias Modification: N = 17; active control therapy + Attention Control Training: N = 20) Age range: 7 to 11 Inclusion criteria: primary diagnosis of generalised anxiety disorder, separation anxiety disorder, or social anxiety disorder (based on K‐SADS) Exclusion criteria: (i) other psychiatric disorder judged by the clinician to cause more impairment or distress than GAD, separation anxiety disorder, or social anxiety disorder; (ii) any history of mental health treatment; (iii) IQ lower than 70 |
|
| Interventions |
CBT (CBT + Attention Bias Modification) Intervention: Friends for Life (group CBT) + Attention Bias Modification (160 trials) Delivery format: child and parent sessions; group Therapist contact time: 15 hours (10 x 90 minutes) Who delivers the intervention: trained psychologists CBT (CBT + Attention Control Training) Intervention: Friends for Life (group CBT) + Attention Control Training (160 trials) Delivery format: child and parent sessions; group Therapist contact time: 15 hours (10 x 90 minutes) Who delivers the intervention: trained psychologists Active control (control therapy + Attention Bias Modification) Intervention: control therapy ‐ educational tasks and psychoeducation + Attention Bias Modification (160 trials) Delivery format: child and parent sessions; group Therapist contact time: 15 hours (10 x 90 minutes) Who delivers the intervention: trained psychologists Active control (control therapy + Attention Control Training) Intervention: control therapy ‐ educational tasks and psychoeducation + Attention Control Training (160 trials) Delivery format: child and parent sessions; group Therapist contact time: 15 hours (10 x 90 minutes) Who delivers the intervention: trained psychologists |
|
| Outcomes |
Reduction in anxiety symptoms (child report) post‐treatment: SCAS‐C Reduction in anxiety symptoms (parent report) post‐treatment: SCAS‐P Reduction in depressive symptoms post‐treatment: CDI |
|
| Notes | Comparisons:
Active control therapy + Attention Bias Modification = alternative treatment Active control therapy + Attention Control Training = attention control |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Judgement Comment: Computer‐generated numbers used to allocate participants to each group |
| Allocation concealment (selection bias) | Low risk | Quote: "Allocation to groups was concealed, so therapists did not know the participant’s group allocation until the delivery of the first therapy session." Judgement Comment: Independent |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Participants and investigators were blind |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Independent assessors |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Judgement Comment: Attrition detailed, and ITT reported. However, there was a large number of dropouts (23/79), and dropouts were related to CBT + Attention Bias Modification. |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes reported |
| Other source of bias ‐ Therapy integrity | Low risk | Judgement Comment: Trained therapists. Fidelity monitored in supervision. |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Sanchez Garcia 2009.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Number of study centres and location: screening in 17 schools in Spain Study setting: schools Withdrawals: 7 excluded because they failed to attend 3 consecutive sessions (NB: group not reported) |
|
| Participants |
N = 82 (included here: N = 53, randomised to: CBT: N = 28; waitlist: N = 25) Age range: 10 to 14 Inclusion criteria: generalised social phobia diagnosis (based on ADIS‐C) Exclusion criteria: failed to attend 3 consecutive treatment sessions |
|
| Interventions |
CBT Intervention: Intervention in Adolescents with Social Phobia (IAFS), version for 10‐ to 14‐year‐olds. Education, training in social skills, exposure, cognitive restructuring Delivery format: child only; group Therapist contact time: 18 hours (12 x 90 minutes) Waitlist/no treatment Intervention: waitlist |
|
| Outcomes |
Remission of primary anxiety disorder diagnosis post‐treatment: ADIS‐C Remission of all anxiety disorder diagnoses post‐treatment: ADIS‐C Reduction in anxiety symptoms (child report) post‐treatment: SPAI ‐C |
|
| Notes | Study includes third arm (IAFS without cognitive restructuring) not used in the review. Anxiety symptoms measure = social anxiety symptoms measure |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement Comment: No information given |
| Allocation concealment (selection bias) | Unclear risk | Judgement Comment: No information given |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Judgement Comment: No information given |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Judgement Comment: Dropouts (beyond those excluded) and missing data not detailed |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Author provided diagnostic outcomes data |
| Other source of bias ‐ Therapy integrity | Unclear risk | Judgement Comment: No information given |
| Other bias | Unclear risk | Judgement Comment: Participants who missed treatment sessions were excluded |
Santucci 2013.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Number of study centres and location: USA Study setting: university research clinic (conducted over 3 consecutive summers) |
|
| Participants |
N = 29 (CBT: N = 15; waitlist: N = 14) Mean age (SD): 9.18 (1.58) Age range: 7 to 12 Gender: 100% female Inclusion criteria: diagnosis of separation anxiety disorder (based on ADIS‐C/P); female Exclusion criteria: bipolar or psychotic disorder; anxiety or mood symptoms were primarily due to a medical/physical condition |
|
| Interventions |
CBT Intervention: Child Anxiety Multi‐Day Program (CMAP) for SAD. Psychoeducation, somatic anxiety management, cognitive restructuring, problem solving, graduated exposure. Conducted over 7 days, cumulating in sleepover. Parent sessions incorporate "Building confidence" Concomitant/excluded medications: consistent dose of psychotropic medication allowed Delivery format: child sessions and parent sessions; parent present in some of child sessions; group Therapist contact time: 38 hours (4 x 5 hours; 1 x 3 hours; 1 x 15 hours (sleepover)) Who delivers the intervention: treatment developers and doctoral/PhD candidate assistants Waitlist/no treatment Intervention: 8‐week waitlist Concomitant/excluded medications: consistent dose of psychotropic medication allowed |
|
| Outcomes |
Remission of primary anxiety disorder diagnosis post‐treatment: ADIS‐C/P Reduction in anxiety symptoms (child report) post‐treatment: SCAS‐C Reduction in anxiety symptoms (parent report) post‐treatment: SCAS‐P Improvement in global functioning post‐treatment: CGAS |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement Comment: No information given |
| Allocation concealment (selection bias) | Unclear risk | Judgement Comment: No information given |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Independent assessors |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: Attrition detailed. Small amount of missing data, and method for imputing data for missing values detailed and appropriate |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes reported |
| Other source of bias ‐ Therapy integrity | Unclear risk | Judgement Comment: Therapists trained, and supervision used to monitor/review protocol, but no specific detail on adherence |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Schneider 2011.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Number of study centres and location: 1 in Germany Study setting: university clinic Date of study: 2004 to 2009 |
|
| Participants |
N = 43 (CBT: N = 21; waitlist: N = 22) Mean age (SD): CBT: 6.29 (1.01); waitlist: 6.18 (0.73) Age range: 5 to 7 Gender: 25 (58.1%) female Inclusion criteria: primary diagnosis of separation anxiety disorder according to the DSM‐IV‐TR (based on Kinder‐DIPS); knowledge of the local language; age 5 to 7 years; written parental informed consent and verbal child assent Exclusion criteria: taking psychotropic medication |
|
| Interventions |
CBT Intervention: Separation Anxiety Family Therapy (TAFF) ‐ disorder‐specific CBT Concomitant/excluded medications: psychotropic medication excluded Delivery format: child‐only sessions, parent‐only sessions, and family sessions; individual Therapist contact time: 13 hours, 20 min (4 x 50 min ‐ child, 4 x 50 min ‐ parent, 8 x 50 min ‐ family/parent) over 12 weeks Who delivers the intervention: child psychiatrist and co‐led by a fellow of child psychiatry Waitlist/no treatment Intervention: 12‐week waitlist Concomitant/excluded medications: psychotropic medication excluded |
|
| Outcomes |
Remission of primary anxiety disorder diagnosis post‐treatment: ADIS‐C/P Reduction in anxiety symptoms (child report) post‐treatment: RCMAS‐C Reduction in anxiety symptoms (parent‐mother report) post‐treatment: RCMAS‐P |
|
| Notes | Diagnostic post‐treatment assessment = 4‐week follow‐up assessment | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Judgement Comment: Randomisation conducted by statistician using a computerised permuted block design |
| Allocation concealment (selection bias) | Low risk | Judgement Comment: Assignments concealed until the time of group assignment |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Blind assessors |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: Attrition detailed and clear. Appropriate methods used for managing missing data. |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes reported |
| Other source of bias ‐ Therapy integrity | Low risk | Judgement Comment: Therapists trained and supervised. Adherence assessed and reported. |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Sciberras 2018.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: 5 months Number of study centres and location: 1 in Australia Study setting: Attention Deficit Hyperactivity Disorder (ADHD) assessment clinic |
|
| Participants |
N = 12 (CBT: N = 6; usual care: N = 6) Mean age (SD): CBT: 10.4 (1.3); usual care: 11.6 (0.6) Age range: 8 to 12 Gender: 1 (8.3%) female Inclusion criteria: meet criteria for ADHD and generalised, social, or separation anxiety disorder (based on ADIS‐P); 8 to 12 years of age Exclusion criteria: receiving specialist help to manage anxiety |
|
| Interventions |
CBT Intervention: Cool Kids CBT; adaptations to make acceptable for children with ADHD Concomitant/excluded medications: medication for anxiety allowed if stable dose for 6 weeks prior to enrolment Delivery format: child and parent together and child and parent alone; individual Therapist contact time: 10 hours (8 x 1 hour, 2 x 1 hour) Who delivers the intervention: trained facilitators TAU Intervention: continued to receive treatment as usual for ADHD Concomitant/excluded medications: medication for anxiety allowed if stable dose for 6 weeks prior to enrolment |
|
| Outcomes |
Remission of all anxiety disorder diagnoses post‐treatment: ADIS‐P Reduction in anxiety symptoms (child report) post‐treatment: SCAS‐C Reduction in anxiety symptoms (parent report) post‐treatment: SCAS‐P |
|
| Notes | Post‐treatment assessment = 5 months postrandomisation, approximately 6 weeks post‐treatment | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Judgement Comment: An independent statistician generated a randomisation schedule using a computerised random number sequence |
| Allocation concealment (selection bias) | Low risk | Judgement Comment: Independent statistician. Allocation was concealed from families and researchers using sealed, opaque envelopes until parent consent was obtained. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Blind assessors |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: No dropouts |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes reported for all measures |
| Other source of bias ‐ Therapy integrity | Unclear risk | Judgement Comment: Trained facilitators delivered treatment. No further details |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Shahnavaz 2016.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: 1‐year follow‐up Number of study centres and location: 2 in Sweden Study setting: dental clinics Date of study: recruitment January 2013 to March 2014 |
|
| Participants |
N = 30 (CBT: N = 13; TAU: N = 17) Mean age (SD): 10 (3.1) Age range: 7 to 18 Gender: 22 (73.3%) female Inclusion criteria: 1) patient and all primary caregivers agreed to participate; 2) patient had a principal diagnosis of specific phobia (dental anxiety or intraoral injection phobia) according to the DSM‐IV‐TR (adapted DAWBA); 3) no other psychiatric or developmentally related diagnoses considered to be the primary diagnosis, 4) patient was not receiving concurrent psychological treatments and did not have appointments for psychological examination elsewhere; and 5) patient needed dental care but not emergency care; and practical requirements |
|
| Interventions |
CBT Intervention: manual developed by research team. Behavioural analyses, psychoeducation, parent education, exposure to dental procedures both in vivo and in films, relaxation techniques, procedural pain management information, and cognitive restructuring Delivery format: child and parent; individual Therapist contact time: 10 hours (10 x 1 hour) Who delivers the intervention: psychologists, CBT training TAU Intervention: tell‐show‐do, distraction, premedication with midazolam, nitrous oxide sedation, general anaesthesia |
|
| Outcomes |
Remission of primary anxiety disorder diagnosis post‐treatment and 12‐month follow‐up: adapted DAWBA Reduction in anxiety symptoms (child report) post‐treatment and 12‐month follow‐up: Child Survey Fear Schedule: Dental Subscale Reduction in anxiety symptoms (parent report) post‐treatment and 12‐month follow‐up: Child Survey Fear Schedule: Dental Subscale |
|
| Notes | Anxiety symptoms measure dental phobia symptoms measure No adverse events reported in CBT group. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Judgement Comment: True randomisation list, generated at www.random.org |
| Allocation concealment (selection bias) | Low risk | Judgement Comment: External person. Allocation after eligibility assessed, agreed to be included |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Blind assessors |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: Attrition detailed and reasons provided for small number of dropouts. Outcomes reported for completers |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes reported |
| Other source of bias ‐ Therapy integrity | Low risk | Judgement Comment: Trained therapists with regular supervision where adherence and competence monitored |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Sharma 2017.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Number of study centres and location: 1 in India Study setting: university clinic |
|
| Participants |
N = 63 randomised (NB: N = 61 aged 10 to 18 included here: CBT: N = 30; TAU: N = 31) Age range: 10 to 18 Inclusion criteria: aged 10 to 19 (NB: 19‐year‐olds not included in analysis in review); current ICD diagnosis of anxiety disorder (mini‐KID); current International Headache Society diagnosis of primary headaches; basic reading and writing; no significant medication change in last 4 weeks; no history of organic disorder; willingness to be randomised Exclusion criteria: depression excluded on basis CDI |
|
| Interventions |
CBT Intervention: transdiagnostic CBT Delivery format: child only; group Therapist contact time: 24 hours (12 x 2 hours) TAU Intervention: continued receiving TAU ‐ pharmacotherapy, visit psychiatrist for medication review |
|
| Outcomes |
Remission of primary anxiety disorder diagnosis post‐treatment: mini‐KID Remission of all anxiety disorder diagnoses post‐treatment: mini‐KID Reduction in anxiety symptoms (child report) post‐treatment: STAIC‐trait Improvement in global functioning post‐treatment: CGAS |
|
| Notes | Author provided data on under 19s. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Judgement Comment: Computer‐generated list |
| Allocation concealment (selection bias) | Low risk | Judgement Comment: Computer generated, so unlikely to foresee assignment |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Judgement Comment: Not detailed |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: Data presented |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes reported/provided |
| Other source of bias ‐ Therapy integrity | Unclear risk | Judgement Comment: Review of treatment content by committee, but no further detail |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Shortt 2001.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: non‐controlled 12‐month follow‐up Number of study centres and location: 1 in Australia Study setting: university clinic |
|
| Participants |
N = 71 (CBT: N = 54; waitlist: N = 17) Mean age (SD): CBT: 7.83 (1.33); waitlist: 7.88 (1.32) Age range: 6 to 10 Gender: CBT: 57% female; waitlist: 65% female Inclusion criteria: a principal diagnosis of Generalised Anxiety Disorder, Separation Anxiety Disorder, or Social Phobia (determined using the DISCAP) Exclusion criteria: all children with intellectual or severe physical impairment, or who were currently involved in psychosocial or psychopharmacological interventions |
|
| Interventions |
CBT Intervention: FRIENDS. Children work through workbook, parents booklet with parent strategies Concomitant/excluded medications: medications not allowed Delivery format: child‐only and parent‐only sessions, with parent and child together for some sessions; group Therapist contact time: 15 hours (10 x 1 hour (child sessions), 10 x 30 min (parent sessions)) Who delivers the intervention: clinical doctoral candidates Waitlist/no treatment Intervention: 10‐week waitlist Concomitant/excluded medications: medications not allowed |
|
| Outcomes |
Remission of all anxiety disorder diagnoses post‐treatment: DISCAP Reduction in anxiety symptoms (child report) post‐treatment: RCMAS |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement Comment: 3:1 ratio, but no further detail |
| Allocation concealment (selection bias) | Unclear risk | Judgement Comment: No detail |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Blind assessors |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: Attrition reported. Completer and ITT analyses for diagnostic outcomes. Missing data managed appropriately. |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes for relevant measures reported |
| Other source of bias ‐ Therapy integrity | Low risk | Judgement Comment: Integrity assessed and reported |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Silk 2018.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: 12‐month follow‐up Number of study centres and location: 1 in the USA |
|
| Participants |
N = 133 (CBT: N = 90; active control: N = 43) Mean age (SD): CBT: 10.943 (1.395); waitlist: 10.981 (1.633) Age range: 9 to 14 Gender: CBT: 50 (55.6%) female; active control: 24 (55.8%) female Inclusion criteria: meet criteria for current Generalised Anxiety Disorder, Separation Anxiety Disorder, and/or Social Anxiety Disorder (Based on K‐SADS) Exclusion criteria: IQ below 70, psychoactive medications; acute suicidality or risk for harm to self or others; presence of metal objects in the body; current primary diagnosis of major depressive disorder, OCD, PTSD, conduct disorder, substance abuse or dependence, or ADHD. Anxious youth were also excluded if they had evidence of an autism spectrum disorder or a lifetime diagnosis of bipolar disorder, psychotic depression, schizophrenia, or schizoaffective disorder. |
|
| Interventions |
CBT Intervention: Coping Cat. Anxiety management sessions; exposure sessions Concomitant/excluded medications: psychoactive medication not allowed Delivery format: child only; 2 parent sessions; individual Therapist contact time: 16 sessions Who delivers the intervention: Master's and doctoral‐level therapists Active control Intervention: Child Centred Therapy (CCT). Manualised non‐directive, supportive psychotherapy based on humanistic principles such as unconditional positive regard, empathy, and therapist genuineness Concomitant/excluded medications: psychoactive medication not allowed Delivery format: child only; 2 parent sessions; individual Therapist contact time: 16 sessions Who delivers the intervention: Master's and doctoral‐level therapists |
|
| Outcomes |
Remission of all anxiety disorder diagnoses post‐treatment and 12‐month follow‐up: K‐SADS Reduction in anxiety symptoms (child report) post‐treatment and 12‐month follow‐up: SCARED‐C Reduction in anxiety symptoms (parent report) post‐treatment and 12‐month follow‐up: SCARED‐P |
|
| Notes | Active control = alternative treatment | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement Comment: No detail |
| Allocation concealment (selection bias) | Unclear risk | Judgement Comment: No detail |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Judgement Comment: No detail blinding of participants |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Independent evaluators |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: Attrition detailed, and missing data managed appropriately |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes reported for all measures |
| Other source of bias ‐ Therapy integrity | Low risk | Judgement Comment: Trained therapists, and integrity assessed and reported |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Silverman 1999a.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: 12‐month follow‐up Number of study centres and location: 1 in the USA Study setting: university clinic |
|
| Participants |
N = 104 randomised (NB: N = 64 included here, randomised to: CBT: N = 41; active control: N = 23) Mean age (SD): CBT: 10.3 (2.6); active control: 9.7 (2.9) Age range: 6 to 16 Gender: CBT: 20 (48.8%) female; active control: 14 (60.9%) female Inclusion criteria: primary phobic disorder (simple phobia‐majority; social phobia or agoraphobia) (ADIS‐C/P) Exclusion criteria: pervasive developmental disorders, psychotic symptoms, current involvement in psychosocial or psychopharmacological treatment |
|
| Interventions |
CBT Intervention: exposure + self control. Faciliate graded exposure, using cognitive self‐control procedures. Taught cognitive strategies and devised fear hierarchy, perform in‐ and out‐of‐session exposure Concomitant/excluded medications: psychopharmacological treatment not allowed Delivery format: child sessions and parent sessions, and part of session together; individual Therapist contact time: 13 hours 20 min (10 x 80 min) Who delivers the intervention: postdoctoral fellows Active control Intervention: educational support. Education about phobias and treatment. No information on therapeutic strategies or implementing these Concomitant/excluded medications: psychopharmacological treatment not allowed Delivery format: child sessions and parent sessions, and part of session together; individual Therapist contact time: 13 hours 20 min (10 x 80 min) Who delivers the intervention: postdoctoral fellows |
|
| Outcomes |
Remission of primary anxiety disorder diagnosis post‐treatment: ADIS‐C/P Reduction in anxiety symptoms (child report) post‐treatment and 6‐month and 12‐month follow‐up: RCMAS‐C Reduction in anxiety symptoms (parent report) post‐treatment and 6‐month and 12‐month follow‐up: RCMAS‐P Reduction in depressive symptoms post‐treatment: CDI |
|
| Notes | Study includes Contingency Management condition ‐ behavioural intervention not included here. Active control = attention control | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement Comment: Not detailed |
| Allocation concealment (selection bias) | Unclear risk | Judgement Comment: Not detailed |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Judgement Comment: Not detailed |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Judgement Comment: Not detailed |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Judgement Comment: Overall attrition detailed. Missing data for measures and procedure for managing missing data not detailed. It appears that completer analysis was reported only. |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes reported |
| Other source of bias ‐ Therapy integrity | Low risk | Judgement Comment: Therapists trained and supervised. Integrity assessed. |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Silverman 1999b.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: non‐controlled 12‐month follow‐up Number of study centres and location: 1 in the USA Study setting: university clinic |
|
| Participants |
N = 56 (CBT: N = 37; waitlist: N = 19) Mean age (SD): 9.96 Age range: 6 to 16 Gender: CBT: 17 (46%) female; waitlist 5 (26%) female Inclusion criteria: primary diagnosis of social phobia, overanxious disorder, or GAD (based on ADIS‐C/P) Exclusion criteria: pervasive developmental disorder, psychotic symptoms, current psychological or psychopharmacological treatment |
|
| Interventions |
CBT Intervention: group CBT ‐ parent and child. Contigency management, exposure, child self‐talk Concomitant/excluded medications: psychopharmacological treatment not allowed Delivery format: child sessions and parent sessions, and parent joined child sessions; group Therapist contact time: ? sessions 40 minutes each + 15 minutes together Who delivers the intervention: psychologist and doctoral student Waitlist/no treatment Intervention: 8‐ to 10‐week waitlist Concomitant/excluded medications: psychopharmacological treatment not allowed |
|
| Outcomes |
Remission of primary anxiety disorder diagnosis post‐treatment: ADIS‐C/P Reduction in anxiety symptoms (child report) post‐treatment: RCMAS‐C Reduction in anxiety symptoms (parent report) post‐treatment: RCMAS‐P Reduction in depressive symptoms post‐treatment: CDI |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement Comment: Not detailed |
| Allocation concealment (selection bias) | Unclear risk | Judgement Comment: Not detailed |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Subsample rated by independent evaluators, although blinding of assessors not specified |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Judgement Comment: Attrition detailed. 27% dropout. Completers compared to non‐completers on baseline characteristics. It appears that only completer analysis was reported, and does not specify comparison to ITT. |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes reported |
| Other source of bias ‐ Therapy integrity | Low risk | Judgement Comment: Integrity assessed and reported |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Simon 2011.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: 24‐month follow‐up Number of study centres and location: the Netherlands Study setting: primary schools (screening) |
|
| Participants |
N = 412 randomised (NB: N = 75 included here, CBT (parent): N = 27; CBT (child): N = 18; no treatment: N = 30) Mean age (SD): CBT (parent): 9.67 (1.04); CBT (child): 9.61 (1.15); no treatment: 10.10 (1.27) Age range: 8 to 13 Gender: 33 (44% female) Inclusion criteria: score top 15% on SCARED‐71 in screening (NB: we only included those who met diagnostic criteria for an anxiety disorder based on ADIS‐C/P in the review) |
|
| Interventions |
CBT (parent) Intervention: parent‐focused CBT Delivery format: parent only; group (and telephone) Therapist contact time: 5 hours 45 minutes (3 x 90 minutes (group); 5 x 15 minutes (telephone)) Who delivers the intervention: psychology graduates CBT (child) Intervention: child‐focused CBT Delivery format: child only; group Therapist contact time: 12 hours (8 x 90 minutes) Who delivers the intervention: psychology graduates Waitlist/no treatment Intervention: no intervention |
|
| Outcomes |
Remission of all anxiety disorder diagnoses post‐treatment and 24‐month follow‐up: ADIS‐C/P Reduction in anxiety symptoms (child report) post‐treatment and 24‐month follow‐up: SCARED‐C |
|
| Notes | We only included participants who met diagnostic criteria for anxiety disorder at baseline. Post‐treament assessment = 12 months |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement Comment: Not detailed |
| Allocation concealment (selection bias) | Unclear risk | Judgement Comment: Not detailed |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Judgement Comment: Not detailed |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: Detail provided on missing data |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Data on outcomes provided by author |
| Other source of bias ‐ Therapy integrity | Low risk | Judgement Comment: Trained and supervised, integrity assessed and reported |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Smith 2014.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: non‐controlled 3‐month follow‐up Number of study centres and location: 1 in the USA Study setting: university clinic |
|
| Participants |
N = 31 (CBT: N = 18; waitlist: N = 13) Mean age (SD): 9.80 (1.78) Age range: 7 to 13 Gender: 12 (38.7%) Inclusion criteria: met DSM‐IV diagnostic criteria for 1 or more of the following: separation anxiety disorder, social anxiety disorder, specific phobia, and/or generalised anxiety disorder Exclusion criteria: comorbid pervasive developmental disorder, traumatic brain injury, organic brain damage, psychotic symptoms, or engagement in concurrent psychotherapy for anxiety |
|
| Interventions |
CBT Intervention: individualised parent intervention. Includes psychoeducation and strategies for responding adaptively to child anxiety, and demonstrates CBT techniques for parents to teach their children Concomitant/excluded medications: concurrent pharmacological treatment for anxiety required stable dosages 1 month prior to and throughout participation Delivery format: parent only; individual Therapist contact time: 10 hours (10 x 1 hour) Who delivers the intervention: advanced doctoral psychology student Waitlist Intervention: 10‐week waitlist Concomitant/excluded medications: concurrent pharmacological treatment for anxiety required stable dosages 1 month prior to and throughout participation |
|
| Outcomes |
Reduction in anxiety symptoms (child report) post‐treatment: MASC‐C Reduction in anxiety symptoms (parent report) post‐treatment: MASC‐P |
|
| Notes | Post‐treatment diagnostic assessment used, but required outcomes not reported. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement Comment: Not detailed |
| Allocation concealment (selection bias) | Unclear risk | Judgement Comment: Not detailed |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Blind assessors |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Judgement Comment: High rate of missing questionnaire data |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes for measures reported |
| Other source of bias ‐ Therapy integrity | Low risk | Judgement Comment: Trained therapists. Regular supervision, fidelity monitored |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Southam Gerow 2010.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Number of study centres and location: USA Study setting: recruited from 6 mental health clinics |
|
| Participants |
N = 48 (CBT: N = 24; TAU: N = 24) Mean age (SD): 10.9 (2.1) Age range: 8 to 15 Gender: 56.2% female Inclusion criteria: primary diagnosis of GAD, separation anxiety disorder, social phobia, specific phobia (based on DISC); anxiety the treatment priority Exclusion criteria: a) pervasive developmental disorder, (b) a psychotic disorder, or (c) mental retardation |
|
| Interventions |
CBT Intervention: Coping Cat Concomitant/excluded medications: medication use was tracked during treatment Delivery format: child only; individual Therapist contact time: 16 to 20 sessions Who delivers the intervention: social workers/doctoral‐level psychologists/Master's‐level psychologists/other (e.g. marriage and family therapists) TAU Intervention: usual care. Therapists used treatment procedures regularly used and believed to be effective in clinical practice. Concomitant/excluded medications: medication use was tracked during treatment Delivery format: child only; individual Who delivers the intervention: social workers/doctoral‐level psychologists/Master's‐level psychologists/other (e.g. marriage and family therapists) |
|
| Outcomes |
Remission of primary anxiety disorder diagnosis post‐treatment: DISC Reduction in anxiety symptoms (child report) post‐treatment: STAIC‐Trait Reduction in anxiety symptoms (parent report) post‐treatment: STAIC‐Trait |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Judgement Comment: Block randomised |
| Allocation concealment (selection bias) | Unclear risk | Judgement Comment: No detail given |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Judgement Comment: No detail given |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Blind assessors |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: Attrition fully described. Appropriate method used for managing missing data ‐ diagnostic outcomes report for completers and using ITT, and explored if any differences between those with and without missing data. |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes for measures reported |
| Other source of bias ‐ Therapy integrity | Low risk | Judgement Comment: Therapists trained and supervised. Adherence assessed. |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Spence 2000.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: non‐controlled 6‐ and 12‐month follow‐up Number of study centres and location: 1 in Australia Study setting: university clinic |
|
| Participants |
N = 51 (CBT (child + parent): N = 17; CBT (child only): N = 19; waitlist: N = 15) Mean age (SD): CBT (child + parent): 10.94 (1.92), n = 17; CBT (child only): 11 (2.45), n = 19; waitlist: 9.93 (1.77), n = 14 Age range: 7 to 14 Gender: CBT (child + parent): 7 (41.2%) female, n = 17; CBT (child only): 9 (47.4%), n = 19; waitlist: 3 (21.4%) female, n = 14 Inclusion criteria: social phobia principal diagnosis (based on ADIS‐C/P) Exclusion criteria: not report any avoidance or worry related to any social situation on the SWQ‐PU, severe learning difficulty, medication for a psychological disorder |
|
| Interventions |
CBT (child + parent) Intervention: social skills training, relaxation techniques, social problem‐solving, positive self‐instruction, cognitive challenging and graded exposure. Parent observes child sessions and attends parent training sessions. Concomitant/excluded medications: medications excluded Delivery format: child‐only sessions (parent observes), plus parent‐only sessions; group Therapist contact time: 24 hours (child: 12 x 1 hour + 12 x 30 min; parents: 6 hours) Who delivers the intervention: psychologists CBT (child only) Intervention: social skills training, relaxation techniques, social problem‐solving, positive self‐instruction, cognitive challenging and graded exposure Concomitant/excluded medications: medications excluded Delivery format: child only; group Therapist contact time: 18 hours (12 x 1 hour + 12 x 30 min) Who delivers the intervention: psychologists Waitlist/no treatment Intervention: 12‐week waitlist Concomitant/excluded medications: medications excluded |
|
| Outcomes |
Remission of primary anxiety disorder diagnosis post‐treatment: ADIS‐C/P Remission of all anxiety disorder diagnosis post‐treatment: ADIS‐C/P Reduction in anxiety symptoms (child report) post‐treatment: RCMAS |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement Comment: No detail given |
| Allocation concealment (selection bias) | Unclear risk | Judgement Comment: No detail given |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Blind assessor not specified for post‐treatment, but independent rater assessed subset of interviews |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: Data provided by author |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes for all measures reported |
| Other source of bias ‐ Therapy integrity | Unclear risk | Judgement Comment: Qualified therapists, but no further detail on assessing/monitoring adherence/competence |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Spence 2006.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: 12‐month non‐controlled follow‐up Number of study centres and location: 1 in Australia Study setting: university clinic |
|
| Participants |
N = 72 randomised (NB: N = 45 included here, randomised to CBT: N = 22; waitlist: N = 23) Mean age (SD): CBT: 10.26 (2.05); waitlist: 9.70 (1.73) Age range: 7 to 14 Gender: CBT: 40.90% female; waitlist: 43.50% female Inclusion criteria: primary diagnosis of an anxiety disorder (based on ADIS‐P), aged 7 to 14, ability to read and write English, and access to internet at home Exclusion criteria: no significant differences in demographic or clinical variables |
|
| Interventions |
CBT Intervention: clinic group. Components included identifying physiological symptoms of anxiety; progressive muscle relaxation, guided imagery, and deep breathing; coping self‐talk and cognitive restructuring; graded exposure; problem solving; and self‐evaluation and reward. Parent component included psychoeducation about (a) child anxiety, (b) contingency management, and (c) ways of assisting their child with relaxation training, cognitive restructuring, graded exposure, and problem solving. Concomitant/excluded medications: not allowed Delivery format: child only and parent only; group Therapist contact time: 16 hours (10 x 1 hour (child), 6 x 1 hour (parent)) Who delivers the intervention: psychologists Waitlist/no treatment Intervention: 10‐week waitlist Concomitant/excluded medications: not allowed |
|
| Outcomes |
Remission of primary anxiety disorder diagnosis post‐treatment: ADIS‐P Remission of all anxiety disorder diagnosis post‐treatment: ADIS‐P Reduction in anxiety symptoms (child report) post‐treatment: SCAS‐C Reduction in anxiety symptoms (child report) post‐treatment: SCAS‐P |
|
| Notes | Study included "NET" condition (online delivery) which we did not include in the review. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Judgement Comment: A coin was tossed |
| Allocation concealment (selection bias) | Unclear risk | Judgement Comment: Assigned in advance, but no further detail provided, e.g. if independent |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Judgement Comment: Interrater reliability assessed, with rater blind to original diagnoses, but does not specify if assessors were blind to condition |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: Report ITT and completer analyses. Attrition detailed. |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes reported |
| Other source of bias ‐ Therapy integrity | Low risk | Judgement Comment: Independent assessment of integrity |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Spence 2011.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: 12‐month non‐controlled follow‐up Number of study centres and location: 3 in Australia Study setting: 3 university clinics |
|
| Participants |
N = 115 randomised (NB: N = 71 included here: CBT: N = 44; waitlist: N = 27) Age range: 12 to 18 Inclusion criteria: primary diagnosis of separation anxiety disorder, social phobia, GAD, or specific phobia (ADIS‐C/P); aged 12 to 18; access to computer and internet at home; able to read and write English at age‐appropriate level Exclusion criteria: primary diagnosis of panic disorder, OCD, PTSD, mood disorder with CSR 6+, pervasive developmental disorder, learning disorder, significant behavioural, substance abuse, suicidal ideation or current self‐harm |
|
| Interventions |
CBT Intervention: BRAVE CLINIC. Manualised individual CBT for adolescent anxiety, adapted from child version (equivalent to online programme in content, number, and length sessions) Delivery format: child only and parent only; individual Therapist contact time: 15 hours (10 x 1 hour (child), 5 x 1 hour (parent)) Who delivers the intervention: psychologists Waitlist/no treatment Intervention: 12‐week waitlist |
|
| Outcomes |
Remission of primary anxiety disorder diagnosis post‐treatment: ADIS‐P Remission of all anxiety disorder diagnosis post‐treatment: ADIS‐P Reduction in anxiety symptoms (child report) post‐treatment: SCAS‐C Reduction in anxiety symptoms (child report) post‐treatment: SCAS‐P Improvement in global functioning post‐treatment: CGAS |
|
| Notes | Study included "NET" condition (online CBT) which we did not include in the review. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Judgement Comment: Computer‐generated sequence |
| Allocation concealment (selection bias) | Low risk | Judgement Comment: In advance, implemented by independent researcher |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Blind assessors |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: Attrition reported. Reported completer and ITT analyses for diagnostic outcomes, and ITT for continuous. Examined and reported impact of missing data |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes reported |
| Other source of bias ‐ Therapy integrity | Low risk | Judgement Comment: Trained therapists, regular supervision, fidelity assessed and reported |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Storch 2013.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: non‐controlled 3‐month follow‐up Number of study centres and location: 1 in the USA Study setting: university clinic |
|
| Participants |
N = 45 (CBT: N = 24: TAU: N = 21) Mean age (SD): 8.89 (13.4) Age range: 7 to 11 Gender: 9 (20%) female Inclusion criteria: diagnosis of autistic disorder, Asperger’s syndrome, or pervasive developmental disorder–not otherwise specified; primary diagnosis of separation anxiety disorder, social phobia, generalised anxiety disorder, or obsessive‐compulsive disorder (based on ADIS‐C/P) Exclusion criteria: full‐scale or verbal comprehension IQ less than 70 on a standardised test; concurrent participation in psychosocial interventions (excluding occupational/speech therapy, and social skills training groups that did not include homework and were less than 90 minutes per week, given that treatment efficacy for anxiety was limited, and parents are often reluctant to give up services); active suicidality or engagement in suicidal behaviours within 6 months before enrolment; or bipolar or psychotic disorder |
|
| Interventions |
CBT Intervention: Behavioral Interventions for Anxiety in Children with Autism (BIACA) Concomitant/excluded medications: stable dose before screening allowed Delivery format: child only and parent only; individual Therapist contact time: 16 to 24 hours (16 x 60 to 90 minutes) Who delivers the intervention: doctoral students or postdoctoral fellows in clinical or school psychology TAU Intervention: free to begin, continue, change, or refrain from any psychosocial or pharmacological treatment Concomitant/excluded medications: any allowed |
|
| Outcomes |
Remission of primary anxiety disorder diagnosis post‐treatment: ADIS‐C/P Remission of all anxiety disorder diagnosis post‐treatment: ADIS‐C/P Reduction in anxiety symptoms (parent report) post‐treatment: MASC‐P |
|
| Notes | Sample with ASD Remission for all anxiety diagnoses reported in Warwick 2016. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Judgement Comment: Computer‐generated algorithm |
| Allocation concealment (selection bias) | Low risk | Judgement Comment: Computer generated, so unlikely to foresee assignment |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Blind assessors |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: Attrition and missing data detailed. Small amount of missing data, and appropriate methods used to manage missing data |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes reported |
| Other source of bias ‐ Therapy integrity | Low risk | Judgement Comment: Therapists trained. Fidelity assessed and reported. |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Storch 2015.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: 1‐month non‐controlled follow‐up Number of study centres and location: 1 in the USA Study setting: university clinic |
|
| Participants |
N = 31 (CBT: N = 16: TAU: N = 15) Mean age (SD): 12.74 (1.34) Age range: 12 to 16 Gender: 6 (19.4%) female Inclusion criteria: met criteria for (1) a diagnosis of autism, Asperger’s syndrome, or Pervasive Developmental Disorder– Not Otherwise Specified ; (2) a co‐occurring anxiety diagnosis of separation anxiety disorder, generalised anxiety disorder, Obsessive Compulsive Disorder, or social phobia (based on ADIS‐C/P); (3) a score of 13 on the Pediatric Anxiety Rating Scale (PARS); and (4) an IQ 80 evaluated by the Wechsler Abbreviated Scale of Intelligence or review of standardised testing occurring in the prior 2 years Exclusion criteria: (1) initiation of new medications within 6 weeks (anti‐psychotics, Attention Deficit Hyperactivity Disorder medications) or 12 weeks (anti‐depressants) before study enrolment; (2) concurrent participation in psychotherapy, social skills training over 90 min per week, or other programmatic behavioural interventions (e.g. applied behavioural analysis); (3) active suicidality; (4) lifetime history of mania, psychosis, or substance abuse |
|
| Interventions |
CBT Intervention: developmentally modified version of the Behavioral Interventions for Anxiety in Children with Autism (BIACA) treatment manual. A minimum of 3 sessions were spent developing coping skills (e.g. behavioural activation, cognitive restructuring) with at least 8 sessions of exposure therapy. Concomitant/excluded medications: any stable medication allowed Delivery format: child sessions, with parent included in most sessions; individual Therapist contact time: 16 to 24 hours (16 x 60 to 90 minutes) Who delivers the intervention: postdoctoral fellows or doctoral students in clinical or school psychology with at least 1 year of experience in CBT for childhood anxiety TAU Intervention: participants could seek any psychosocial or pharmacological treatment that they chose, or not seek treatment, for 16 weeks Concomitant/excluded medications: continued with pre‐existing medications or therapy or were able to initiate dosage changes or new medications with the prescribing provider |
|
| Outcomes |
Remission of primary anxiety disorder diagnosis post‐treatment: ADIS‐C/P Remission of all anxiety disorder diagnoses post‐treatment: ADIS‐C/P Reduction in anxiety symptoms (parent report) post‐treatment: MASC‐P |
|
| Notes | Remission from all anxiety disorders diagnoses provided in Warwick 2016. Sample with ASD |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Judgement Comment: Computer generated |
| Allocation concealment (selection bias) | Low risk | Judgement Comment: Computer generated, so unlikely to foresee assignment |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Blind assessors |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: No dropouts to post‐treatment assessment. Missing data managed appropriately. |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes reported/available |
| Other source of bias ‐ Therapy integrity | Low risk | Judgement Comment: Therapists trained and supervised, and adherence rated and reported |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Thirlwall 2013.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: non‐controlled 6‐month follow‐up and 3‐ to 5‐year follow‐up Number of study centres and location: 1 in the UK Study setting: university and NHS clinic Date of study: recruitment April 2008 to December 2010 |
|
| Participants |
N = 194 (CBT (full): N = 64: CBT (brief): N = 61; waitlist: N = 69) Age range: 7 to 12 Gender: CBT (full): 30 (46.9%) female; CBT (brief): 30 (49.2%) female; waitlist: 34 (49.3%) female Inclusion criteria: age 7 to 12, primary diagnosis of GAD, social phobia, separation anxiety disorder, panic disorder/agoraphobia, or specific phobia (based on ADIS‐C/P), no significant physical or intellectual impairment, if prescription of psychotropic medication, stable dose (parent and child), primary carer not have current anxiety disorder or other serious mental health disorder, parent not have significant intellectual impairment |
|
| Interventions |
CBT (full) Intervention: guided parent‐delivered CBT treatment. Parents given self‐help book and receive full guidance, some face‐to‐face and some on phone. Concomitant/excluded medications: stable dose allowed Delivery format: parent only; individual Therapist contact time: 5 hours 20 minutes Who delivers the intervention: some clinical experience or novice (some experience delivering CBT or working with clinical populations) CBT (brief) Intervention: guided parent‐delivered CBT treatment. Parents given self‐help book and receive brief guidance, some face‐to‐face and some on phone. Concomitant/excluded medications: stable dose allowed Delivery format: parent only; individual Therapist contact time: 2 hours 40 minutes Who delivers the intervention: some clinical experience or novice (some experience delivering CBT or working with clinical populations) Waitlist/no treatment Intervention: 12‐week waitlist Concomitant/excluded medications: stable dose allowed |
|
| Outcomes |
Remission of primary anxiety disorder diagnosis post‐treatment: ADIS‐C/P Remission of all anxiety disorder diagnoses post‐treatment: ADIS‐C/P Reduction in anxiety symptoms (child report) post‐treatment: SCAS‐C Reduction in anxiety symptoms (parent report) post‐treatment: SCAS‐P Reduction in depressive symptoms post treatment: SMFQ‐child |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Judgement Comment: Centralised telephone randomisation service at the Centre for Statistics in Medicine, University of Oxford |
| Allocation concealment (selection bias) | Low risk | Judgement Comment: Centralised |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Blind assessors |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: Attrition and missing data detailed. Sensitivity analyses used to examine impact of missing data. |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes reported for all measures |
| Other source of bias ‐ Therapy integrity | Low risk | Judgement Comment: Therapists attend training and regular supervision. Adherence assessed and reported. |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Villabo 2018.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: 2‐year non‐controlled follow‐up Number of study centres and location: 5 clinics in Norway Study setting: community clinics Date of study: recruitment September 2008 through October 2011 |
|
| Participants |
N = 165 (CBT (individual CBT): N = 55: CBT ( group CBT): N = 55; waitlist: N = 55) Mean age (SD): 10.46 (1.49) Age range: 7 to 13 Gender: CBT (ICBT): 24 (43.6%) female; CBT (GCBT): 25 (45.5%) female; waitlist: 26 (47.3%) female Inclusion criteria: age 7 to 13, primary diagnosis of SAD, GAD, or social anxiety disorder (based on ADIS‐C/P), significant functional impairment, IQ 70+, 1 parent + proficient in Norwegian Exclusion criteria: (a) a mental health disorder with a higher treatment priority, (b) pervasive developmental disorder(s), (c) psychosis, or (d) current use of anxiolytic medication |
|
| Interventions |
CBT (individual CBT) Intervention: Norwegian translation of Coping Cat Concomitant/excluded medications: current use of anxiolytic medication not allowed Delivery format: child only, and 2 parent only; individual Therapist contact time: 14 sessions Who delivers the intervention: community therapists (psychologists, social workers, psychiatry residents) CBT (group CBT) Intervention: Norwegian translation of Coping Cat Concomitant/excluded medications: current use of anxiolytic medication not allowed Delivery format: child only, and 2 parent only; group Therapist contact time: 14 sessions Who delivers the intervention: community therapists (psychologists, social workers, psychiatry residents) Waitlist/no treatment Intervention: 12‐week waitlist Concomitant/excluded medications: current use of anxiolytic medication not allowed |
|
| Outcomes |
Remission of primary anxiety disorder diagnosis post‐treatment: ADIS‐C/P Remission of all anxiety disorder diagnoses post‐treatment: ADIS‐C/P Reduction in anxiety symptoms (child report) post‐treatment: MASC‐C Reduction in anxiety symptoms (parent report) post‐treatment: MASC‐P Improvement in global functioning post‐treatment: CGAS |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Judgement Comment: Computer‐generated permuted blocking procedure |
| Allocation concealment (selection bias) | Low risk | Judgement Comment: Computer generated, so unlikely to foresee assignment |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Blind assessors |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: Attrition reported. Appropriate methods used to manage missing data. |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes reported for all measures |
| Other source of bias ‐ Therapy integrity | Low risk | Judgement Comment: Therapists with a range of experience. Adherence assessed and reported. |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Walkup 2008.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: long‐term follow‐up (6 years) to date Number of study centres and location: 6 in the USA Study setting: university clinics Date of study: 2002 to 2007 |
|
| Participants |
N = 488 (CBT alone: N = 139: CBT + sertraline: N = 140; sertraline alone: N = 133; drug placebo: N = 76) Mean age (SD): CBT alone: 10.5 (2.9); CBT + sertraline: 10.7 (2.8); sertraline alone: 10.8 (2.8); drug placebo: 10.6 (2.8) Age range: 7 to 17 Gender: CBT alone: 72 (51.8%) female; CBT + sertraline: 72 (51.4%) female; sertraline alone: 61 (45.9%) female; drug placebo: 37 (48.7%) female Inclusion criteria: aged 7 to 17, primary diagnosis of separation or generalised or social phobia, substantial impairment (based on ADIS‐C/P), IQ 80+ Exclusion criteria: unstable medical condition, were refusing to attend school because of anxiety, or had tried but had no response to 2 adequate trials of SSRIs or an adequate trial of CBT. Girls who were pregnant or sexually active and were not using an effective method of birth control were also excluded. Children who were receiving psychoactive medications other than stable doses of stimulants and who had psychiatric diagnoses that made participation in the study clinically inappropriate (i.e. current major depressive or substance use disorder; unmedicated ADHD, combined type; or a lifetime history of bipolar, psychotic, or pervasive developmental disorders) or who presented an acute risk to themselves or others were also excluded. |
|
| Interventions |
CBT alone Intervention: based on Coping Cat Concomitant/excluded medications: receiving psychoactive medications other than stable doses of stimulants excluded Delivery format: child only, parent check‐in, and 2 parent only Therapist contact time: 14 hours (14 x 1 hour) Who delivers the intervention: experienced psychotherapists certified in the Coping Cat protocol CBT + sertraline Intervention: based on Coping Cat + sertraline (Zoloft) Concomitant/excluded medications: receiving psychoactive medications other than stable doses of stimulants excluded Delivery format: child only, parent check‐in, and 2 parent only Therapist contact time: 18 to 22 hours: 14 hours (14 x 1 hour) + 4 to 8 hours (8 x 30 to 60 minutes) Who delivers the intervention: experienced psychotherapists certified in the Coping Cat protocol. Psychiatrists and nurse clinicians with experience in medicating children with anxiety disorders Sertraline alone Intervention: sertraline (Zoloft) Concomitant/excluded medications: receiving psychoactive medications other than stable doses of stimulants excluded Therapist contact time: 4 to 8 hours (8 x 30 to 60 minutes) Who delivers the intervention: psychiatrists and nurse clinicians with experience in medicating children with anxiety disorders Drug placebo Intervention: drug placebo Concomitant/excluded medications: receiving psychoactive medications other than stable doses of stimulants excluded Therapist contact time: 4 to 8 hours (8 x 30 to 60 minutes) Who delivers the intervention: psychiatrists and nurse clinicians with experience in medicating children with anxiety disorders |
|
| Outcomes |
Reduction in anxiety symptoms (child report) post‐treatment and 36‐week follow‐up: MASC‐C Reduction in anxiety symptoms (parent report) post‐treatment and 36‐week follow‐up: MASC‐P Improvement in global functioning post‐treatment: CGAS Reduction in depressive symptoms post‐treatment: MFQ‐C |
|
| Notes | Adverse events reported. Long‐term remission outcomes reported elsewhere. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Judgement Comment: Computer generated |
| Allocation concealment (selection bias) | Low risk | Judgement Comment: Managed central pharmacy |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Drug placebo kept secret from participants |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Independent blind assessors |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: Dropouts clear, and procedures for managing clear and robust |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes reported for all measures |
| Other source of bias ‐ Therapy integrity | Low risk | Judgement Comment: Experienced therapists. Regular supervision. Fidelity assessed. |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Waters 2009.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Number of study centres and location: 1 in Australia Study setting: university clinic |
|
| Participants |
N = 80 (CBT (parent + child): N = 31; CBT (parent only): 38; waitlist: N = 11) Mean age (SD): CBT (parent + child): 6.89 (1.2); CBT (parent only): 6.68 (1.20); waitlist: 6.68 (1.20) Age range: 4 to 8 Gender: CBT (parent + child): 17 (54.8%) female; CBT (parent only): 20 (64.5%) female; waitlist: 5 (45.5%) female Inclusion criteria: specific phobia, social phobia, GAD, and/or separation anxiety disorder diagnosis (based on ADIS‐P) Exclusion criteria: comorbid externalising disorder, pervasive developmental disorder, organic brain damage, or psychosis. Children involved in psychological or pharmacological treatment for anxiety disorders were excluded. |
|
| Interventions |
CBT (parent + child) Intervention: Take Action. Children: psychoeducation, training in relaxation, identifying anxious self‐talk, coping strategies, exposure, problem solving, social skills. Parent sessions: provided with child workbook, cover: psychoeducation, parent strategies for managing anxiety, coverage of take action steps children complete each week, positive parent coping, communication and problem‐solving skills Concomitant/excluded medications: not allowed Delivery format: child sessions and parent sessions; group Therapist contact time: 20 hours (10 x 1 hour (child); 10 x 1 hour (parent)) Who delivers the intervention: psychologists trained in CBT for child anxiety CBT (parent only) Intervention: same as parent sessions in parent + child above Concomitant/excluded medications: not allowed Delivery format: parent sessions; group Therapist contact time: 10 hours (10 x 1 hour (parent)) Who delivers the intervention: psychologists trained in CBT for child anxiety Waitlist/no treatment Intervention: approximately 10‐week wait Concomitant/excluded medications: not allowed |
|
| Outcomes |
Remission of primary anxiety disorder diagnosis post‐treatment: ADIS‐P Remission of all anxiety disorder diagnoses post‐treatment: ADIS‐P |
|
| Notes | Anxiety symptoms measure not reported for waitlist, so not able to use in review. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement Comment: No detail given |
| Allocation concealment (selection bias) | Unclear risk | Judgement Comment: No detail given |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Blind ADIS assessors |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: Report dropouts. High number of dropouts, but report completer analyses and ITT and same conclusions |
| Selective reporting (reporting bias) | Unclear risk | Judgement Comment: Did not report parent‐reported child anxiety symptoms for waitlist |
| Other source of bias ‐ Therapy integrity | Low risk | Judgement Comment: Trained therapists, regular supervision. Therapist checklist used to maintain integrity. |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Wergeland 2014.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Total duration of study: non‐controlled 1‐year follow‐up Number of study centres and location: 7 public child and adolescent mental health outpatient clinics in Norway Study setting: CAMHS clinics Date of study: 2008 to 2010 |
|
| Participants |
N = 182 (CBT (iCBT): N = 77; CBT (GCBT): N = 67; waitlist: N = 38) Mean age (SD): 11.5 (2.1) Age range: 8 to 15 Gender: 96 (52.7%) female Inclusion criteria: principal anxiety disorder SAD, SOP, GAD (based on ADIS‐C/P) Exclusion criteria: pervasive developmental disorder, psychotic disorder, and/or mental retardation |
|
| Interventions |
CBT (iCBT) Intervention: individual CBT ‐ Friends Concomitant/excluded medications: stable dose allowed Delivery format: child only, child + parent for 2 sessions and part of 8 sessions; individual Therapist contact time: 10 hours (10 x 1 hour) Who delivers the intervention: clinical psychologists, clinical pedagogues, clinical social worker CBT (GCBT) Intervention: group CBT ‐ Friends Concomitant/excluded medications: stable dose allowed Delivery format: child only, child + parent for 2 sessions and part of 8 sessions; group Therapist contact time: 15 hours (10 x 90 minutes) Who delivers the intervention: clinical psychologists, clinical pedagogues, clinical social worker Waitlist/no treatment Intervention: 10‐week waitlist Concomitant/excluded medications: stable dose allowed |
|
| Outcomes |
Remission of primary anxiety disorder diagnosis post‐treatment: ADIS‐C/P Reduction in anxiety symptoms (child report) post‐treatment: SCAS‐C Reduction in anxiety symptoms (parent report) post‐treatment: SCAS‐P Reduction in depressive symptoms post‐treatment: MFQ‐child |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement Comment: Block randomisation, no further detail |
| Allocation concealment (selection bias) | Unclear risk | Judgement Comment: Block randomisation, no further detail |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Judgement Comment: Assessor not blind to treatment approach |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: Appropriate methods used for managing missing data. Report ITT, and also conducted completer analyses |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes reported |
| Other source of bias ‐ Therapy integrity | Low risk | Judgement Comment: Adherence and competence assessed and reported |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
White 2013.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Number of study centres and location: 1 in the USA Study setting: university clinic Date of study: recruitment October 2008 to October 2010 |
|
| Participants |
N = 30 (CBT: N = 15; waitlist: N = 15) Mean age (SD): 15 years Age range: 12 to 17 Gender: 7 (23%) female Inclusion criteria: age 12 to 17, ASD diagnosis supported by ADOS, meet criteria for social phobia GAD, specific phobia, or separation anxiety disorder (based on ADIS‐C/P) Exclusion criteria: primary OCD, panic disorder, or panic disorder with agoraphobia or serious behaviour problems |
|
| Interventions |
CBT Intervention: Multimodal Anxiety and Social Skills Intervention (MASSI). Individual, group, and parent education. Select appropriate modules from manual Concomitant/excluded medications: concomitant psychiatric medication was permitted if the dose was stable for at least 4 weeks with no planned changes for the duration of the randomised trial Delivery format: child only, parent attend for part of session; individual and group Therapist contact time: 21 to 23 hours (13 x 60 to 70 minutes (individual), 7 x 75 minutes (group)) Who delivers the intervention: principal investigator and doctoral students Waitlist/no treatment Intervention: 14‐week waitlist Concomitant/excluded medications: concomitant psychiatric medication was permitted if the dose was stable for at least 4 weeks with no planned changes for the duration of the trial |
|
| Outcomes |
Reduction in anxiety symptoms (parent report) post‐treatment: CASI‐Anxiety Scale Improvement in global functioning post‐treatment: DD‐CGAS |
|
| Notes | Sample with ASD | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Judgement Comment: Names drawn from a box |
| Allocation concealment (selection bias) | Low risk | Judgement Comment: Done by person unaffiliated with study. Baseline measures complete prior to allocation |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Blind assessors for appropriate measures |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: Use appropriate methods for managing missing data |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes reported |
| Other source of bias ‐ Therapy integrity | Low risk | Judgement Comment: Trained and supervised therapists. Sessions recorded and reviewed. Fidelity assessed independently. |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Wood 2009.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Number of study centres and location: 1 in the USA |
|
| Participants |
N = 40 (CBT: N = 17; waitlist: N = 23) Mean age (SD): CBT: 9.18 (1.42); waitlist: 9.22 (1.57) Gender: CBT: 5 (29%) female; waitlist: 8 (35%) female Inclusion criteria: 1) autism/Asperger's or Pervasive Developmental Disorder – Not Otherwise Specified (PDD‐NOA) diagnosis; 2) separation anxiety disorder, social phobia, or OCD (based on ADIS‐C/P); 3) no psychiatric medication or stable dose for at least 1 month and maintained throughout study Exclusion criteria: GAD diagnosis only, IQ less than 70, current psychotherapy or social skills training, family therapy, or parent coaching |
|
| Interventions |
CBT Intervention: Building confidence CBT Concomitant/excluded medications: stable dose allowed Delivery format: child only, and parent/family with child; individual Therapist contact time: 24 hours (16 x 90 minutes) Who delivers the intervention: doctoral students Waitlist/no treatment Intervention: 3‐month waitlist Concomitant/excluded medications: stable dose allowed |
|
| Outcomes |
Reduction in anxiety symptoms (child report) post‐treatment: MASC‐C Reduction in anxiety symptoms (parent report) post‐treatment: MASC‐P |
|
| Notes | Only report remission from 4 entry diagnoses Sample with ASD |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Judgement Comment: Computer randomisation program |
| Allocation concealment (selection bias) | Low risk | Judgement Comment: Concealed from investigators |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Blinded assessors |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: Dropouts reported. ITT and completer analyses reported |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes for planned measures reported |
| Other source of bias ‐ Therapy integrity | Low risk | Judgement Comment: Therapists trained and supervised and adherence measures |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
Wood 2015.
| Study characteristics | ||
| Methods |
Study design: randomised controlled trial Number of study centres and location: 2 in the USA Study setting: 2 university clinics |
|
| Participants |
N = 33 (CBT: N = 19; waitlist: N = 14) Mean age (SD): CBT: 12.3 (1.14); waitlist: 12.2 (0.98) Age range: 11 to 15 Gender: CBT: 6 (32%) female; waitlist: 4 (29%) female Inclusion criteria: criteria for ASD and 1 anxiety disorder (based on ADIS‐C/P) Exclusion criteria: receiving CBT, social skills training with homework or applied behavioural analysis, had initiated an anti‐depressant or anti‐psychotic within 12 or 6 weeks, respectively, prior to treatment, suicide risk, bipolar, schizophrenia, or substance abuse |
|
| Interventions |
CBT Intervention: Behavioral Interventions for Anxiety in Children with Autism (BIACA) Concomitant/excluded medications: stable dose allowed Delivery format: child only, parent only, altogether; individual Therapist contact time: 24 hours (16 x 90 minutes) Who delivers the intervention: postdoctoral clinical fellow or doctoral students Waitlist/no treatment Intervention: 16‐week waitlist Concomitant/excluded medications: stable dose allowed |
|
| Outcomes |
Remission of primary anxiety disorder diagnosis post‐treatment: ADIS‐C/P Reduction in anxiety symptoms (parent report) post‐treatment: MASC‐P |
|
| Notes | Sample with ASD | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Judgement Comment: Computer randomisation |
| Allocation concealment (selection bias) | Low risk | Judgement Comment: Concealed from investigators |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Judgement Comment: Even though blinding was not possible, we judged that it was unlikely this led to a departure from the intended intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement Comment: Independent evaluators |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement Comment: Dropouts detailed. Imputed missing data, but small amount of missing data |
| Selective reporting (reporting bias) | Low risk | Judgement Comment: Outcomes reported for all measures |
| Other source of bias ‐ Therapy integrity | Low risk | Judgement Comment: Trained, supervised, adherence rated and reported |
| Other bias | Low risk | Judgement Comment: The study appears to be free of other sources of bias |
ADI‐R: Autism Diagnostic Interview‐Revised ADIS‐C/P: Anxiety Disorder Interview Schedule for Children‐Child and Parent interviews ADOS: Autism Diagnostic Observation Schedule ASD: Autism Spectrum Disorder BDI‐II: Beck Depression Inventory‐II CAMHS: Child and Adolescent Mental Health Services CASI: Child and Adolescent Symptom Inventory CBCL: Child Behaviour Checklist CBT: cognitive behaviour therapy CDI: Children's Depression Inventory CGAS: Children's Global Assessment Scale CSR: Clinical Severity Rating CTU: Clinical Trials Unit DAWBA: Development and Wellbeing Assessment DD‐CGAS: Developmental Disabled Children’s Global Assessment Scale DIPS‐K: Diagnostischen Interviews bei psychischen Störungen im Kindes‐ und Jugendalter DISC: Diagnostic Interview Schedule for Children DISCAP: Diagnostic Interview Schedule for Children, Adolescents, and Parents DSM‐IV: Diagnostic and Statistical Manual of Mental Disorders‐4th edition DSM‐5: Diagnostic and Statistical Manual of Mental Disorders‐5th edition ICD: International Classification of Disease IQ: intelligence quotient ITT: intention‐to‐treat K‐GAS: Children's Global Assessment Scale (German Version) K‐SADS: Kiddie Schedule for Affective Disorders and Schizophrenia MASC‐C/P: Multidimensional Anxiety Scale for Children‐Child/Parent report MFQ‐C: Mood and Feelings Questionnaire‐Child report MINI‐KID: Mini International Neuropsychiatric Interview for Children and Adolescents PAS‐R: Preschool Anxiety Scale‐Revised RCADS: Revised Children’s Anxiety and Depression Scale RCMAS: Revised Children's Manifest Anxiety Scale SAS‐A: Social Anxiety Scale for Adolescents SAS‐C/P: Social Anxiety Scale for Children‐Child/Parent report SET‐C: Social Effectiveness Therapy for Children SCAS‐C/P: Spence Children's Anxiety Scale‐Child/Parent report SCARED‐C/P: Screen for Child Anxiety Related Emotional Disorders‐Child/Parent report SD: standard deviation SMFQ‐C: Short Mood and Feelings Questionnaire‐Child report SPAI‐C: Social Phobia and Anxiety Inventory for Children SPAIK‐C: Social Phobia and Anxiety Inventory for Children (German Version) STAIC: State‐Trait Anxiety Inventory for Children TAU: treatment as usual
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Asbrand | Data not analysable |
| Asbrand 2019 | Data not analysable |
| Baer 2005 | Data not analysable |
| Beidel 2000 | Not manualised/modular CBT |
| Beidel 2007 | Not manualised/modular CBT |
| Bergman 2013 | Not manualised/modular CBT |
| Bernstein 2005 | Participants did not all meet diagnostic criteria for an anxiety disorder. |
| Bodden 2008a | Not an RCT |
| Clementi 2019 | No non‐CBT control/comparator |
| Cobham 2012 | Not an RCT |
| Cotton 2019 | Not manualised/modular CBT |
| Ebrahiminejad 2016 | Not manualised/modular CBT |
| Flatt 2010 | Data not analysable |
| Gil Bernal 2009 | No baseline structured diagnostic assessment/participants did not meet diagnostic criteria for anxiety disorder |
| Ginsburg 2019b | Participants did not all meet diagnostic criteria for an anxiety disorder. |
| Hayward 2000 | Not an RCT |
| Jansen 2012 | No baseline structured diagnostic assessment/participants did not meet diagnostic criteria for anxiety disorder |
| Kerns 2016 | No baseline structured diagnostic assessment/participants did not meet diagnostic criteria for anxiety disorder |
| Kujawa 2019 | Not an RCT |
| Lyneham 2006 | No direct contact with parent/child/not face‐to‐face |
| Mendlowitz 1999 | Not an RCT |
| Nauta 2003 | Not an RCT |
| NCT00576719 | Data not analysable |
| Oerbeck 2014 | Not manualised/modular CBT |
| Ollendick 2018 | Not manualised/modular CBT |
| Ost 2015 | Not manualised/modular CBT |
| Ozyurt 2018 | Not manualised/modular CBT |
| Pereira 2014 | Participants did not all meet diagnostic criteria for an anxiety disorder. |
| Rudy 2017 | Not manualised/modular CBT |
| Salzer 2018 | Adults (≥ 19 years) (includes 20‐year‐olds) |
| Sevi Tok 2016 | No baseline structured diagnostic assessment/participants did not meet diagnostic criteria for anxiety disorder |
| Storch 2019 | Not manualised/modular CBT |
| Sung 2011 | No baseline structured diagnostic assessment/participants did not meet diagnostic criteria for anxiety disorder |
| Weisz 2012 | Participants did not all meet diagnostic criteria for an anxiety disorder. |
CBT: cognitive behavioural therapy RCT: randomised controlled trial
Characteristics of studies awaiting classification [ordered by study ID]
ACTRN12613000217707.
| Methods | RCT |
| Participants | Inclusion criteria: age 12 to 19, clinical levels of anxiety acquired brain injury |
| Interventions | CBT |
| Outcomes | Primary: SCAS, SCARED, ADIS |
| Notes |
ACTRN12615000730505.
| Methods | RCT. CBT vs waitlist |
| Participants | Inclusion criteria: anxiety disorder, sleep problems Age: 13 to 17 |
| Interventions | Cognitive behaviour therapy for adolescents with anxiety and sleep‐related problems |
| Outcomes | Primary: ADIS (anxiety). Insomnia (Insomnia Severity Index) |
| Notes | Status: not yet recruiting |
ACTRN12619000619145.
| Methods | RCT |
| Participants | Target: N = 80 Inclusion criteria: age 10 to 14; diagnosed with diabetes, clinical or subclinical anxiety |
| Interventions | CBT Waitlist |
| Outcomes | Primary: YAM‐5 |
| Notes | Not yet recruiting |
DRKS00012823.
| Methods | RCT |
| Participants | Target: N = 420 Inclusion criteria: depressive disorder or anxiety disorder; age 6 to 18 |
| Interventions | CBT Psychodynamic psychotherapy |
| Outcomes | Primary: number of psychiatric diagnoses |
| Notes |
IRCT20181006041250N.
| Methods | RCT |
| Participants | Inclusion criteria: female; age 8 to 12; anxiety symptoms (SCAS cut‐off), mild to moderate anxiety disorder not requiring drug therapy |
| Interventions | CBT: group, based on Coping Cat Control: group, storytelling |
| Outcomes | SCAS, SDQ, CDI |
| Notes | Complete |
ISRCTN59518816.
| Methods | RCT |
| Participants | Target: N = 228 Inclusion criteria: aged 8 to 12; Attention Deficit Hyperactivity Disorder; anxiety disorder (generalised anxiety disorder, social anxiety disorder, separation anxiety disorder) |
| Interventions | CBT Treatment As Usual |
| Outcomes | Remission of anxiety disorder (GAD, social anxiety disorder, separation anxiety disorder) |
| Notes | Complete |
JPRN‐UMIN000008724.
| Methods | RCT |
| Participants | Inclusion criteria: age 7 to 18; anxiety disorder (based on ADIS); discontinue other psychotherapy for the trial |
| Interventions | CBT Control (no treatment) |
| Outcomes | Primary: ADIS |
| Notes |
JPRN‐UMIN000032275.
| Methods | RCT |
| Participants | Inclusion criteria: age 9 to 15; clinical or subclinical diagnosis of anxiety disorder or depressive disorder |
| Interventions | CBT Control: no treatment |
| Outcomes | Primary: ADIS |
| Notes |
JPRN‐UMIN000033218.
| Methods | RCT |
| Participants | Target: N = 60 Inclusion criteria: age 10 to 16; IQ in average range; Autism Spectrum Disorder diagnosis; clinical level of anxiety (semi‐structured interview) |
| Interventions | CBT Active control |
| Outcomes | Primary: anxiety symptoms |
| Notes | No longer recruiting |
NCT02810171.
| Methods | RCT |
| Participants | Target: N = 280 Inclusion: age 7 to 17; clinically significant anxiety as determined by structured clinical interview; anxiety primary concern |
| Interventions | CBT Relaxation Therapy |
| Outcomes | Primary: brain function/structure Secondary: Pediatric Anxiety Rating Scale |
| Notes | Started December 2016 |
NCT02977962.
| Methods | RCT |
| Participants | Target: N = 44 Inclusion criteria: age 16 to 21; ASD; diagnosis of 1 of the following anxiety disorders: separation anxiety disorder, specific phobia, panic disorder, generalised anxiety disorder, social phobia, or obsessive compulsive disorder, and minimum score of 14 on the Hamilton Anxiety Scale |
| Interventions | CBT TAU |
| Outcomes | Primary: Hamilton Anxiety Scale (change from baseline) |
| Notes | Not all participants would be eligible. |
NCT03412227.
| Methods | RCT |
| Participants | Target: N = 200 Inclusion criteria: age 9 to 17; primary DSM‐5 anxiety disorder or depressive disorder |
| Interventions | Individual Behavioral Activation Therapy (IBAT) The PASCET Program for Youth Depressive Disorders Coping Cat (CBT) Waitlist |
| Outcomes | Primary: Clinical Global Impression Severity (CGIS) scale (change) |
| Notes |
NCT03899948.
| Methods | RCT |
| Participants | Target N = 135 Inclusion criteria: attend elementary school, elevated anxiety symptoms and Clinical Severity Rating 3+ on ADIS |
| Interventions | Teacher Anxiety Program for Elementary Students (TAPES) Teacher Anxiety Training (TAT) |
| Outcomes | Secondary: change on modified ADIS |
| Notes | Anxiety diagnosis not required. |
ADIS: Anxiety Disorder Interview Schedule for Children CBT: cognitive behavioural therapy CDI: Children's Depression Inventory IQ: intelligence quotient RCT: randomised controlled trial SCARED: Screen for Child Anxiety Related Emotional Disorders SCAS: Spence Children's Anxiety Scale SDQ: Strengths and Difficulties Questionnaire YAM‐5: Youth Anxiety Scale for DSM‐5
Characteristics of ongoing studies [ordered by study ID]
ACTRN12616001552471.
| Study name | Effectiveness of school group‐based acceptance and commitment therapy for children with anxiety: a randomised controlled trial |
| Methods | RCT |
| Participants | Target N = 130 Inclusion criteria: 1. Aged between 7 and 17 years. 2. Meet criteria for a primary diagnosis of an anxiety disorder. 3. Available/able to attend The Children’s Hospital at Westmead for pretreatment, immediate post‐treatment, and 6‐month post‐treatment assessments as well as attending a minimum of 80% of therapy sessions. 4. Have a parent/caregiver who is willing to attend and participate in the assessment as well as 2 parent sessions |
| Interventions | Proactive (Acceptance and Commitment Therapy group‐based manualised therapy programme delivered by school counsellors) vs waitlist (10 weeks) |
| Outcomes | Primary outcomes: Change in score on the Pediatric Anxiety Rating Scale (PARS) ‐ clinician, child, and parent rated (pre‐, post‐treatment and 6 months post‐treatment) Change in the Spence Anxiety Scale for Children (SCAS) ‐ child and parent rated (pre‐, post‐treatment and 6 months post‐treatment) |
| Starting date | 28 September 2016 |
| Contact information | Dr Karen Hancock SCHN, CHW Department of Psychological Medicine Locked Bag 4001 Westmead NSW 2145 Australia karen.hancock@health.nsw.gov.au |
| Notes | www.who.int/trialsearch/Trial2.aspx?TrialID=ACTRN12616001552471 anzctr.org.au/ACTRN12616001552471.aspx |
NCT02725619.
| Study name | Neural mechanisms of CBT for anxiety in children with autism: randomized controlled trial |
| Methods | RCT |
| Participants | Target N = 150 Inclusion criteria: aged 8 to 14; diagnosis of autism spectrum disorder; diagnosis of anxiety disorder and clinically significant level of anxiety; full‐scale IQ and verbal IQ > 70; unmedicated or on stable medication with no planned changes for duration of study; able to meet MRI safety (e.g. no metal medical implants) and data quality requirements (e.g. able to keep head still during scanning) |
| Interventions | CBT vs Psychoeducation and Supportive Therapy (PST) |
| Outcomes | Primary outcomes: Pediatric Anxiety Rating Scale (PARS) (change from baseline ‐ midpoint; change from baseline ‐ endpoint) Clinical Global Impression‐Improvement (CGI‐I) scale (change from baseline ‐ midpoint; change from baseline ‐ endpoint) Blood oxygenation level dependent signal (BOLD) during down‐regulation versus passive viewing of affective images (change from baseline ‐ midpoint; change from baseline ‐ endpoint) |
| Starting date | April 2016 |
| Contact information | Denis Sukhodolsky Yale Child Study Center New Haven, Connecticut, USA denis.sukhodolsky@yale.edu |
| Notes | clinicaltrials.gov/show/nct02725619 |
NCT02908321.
| Study name | Cognitive behavioural therapy for anxiety disorder in children with co‐morbid autism spectrum disorder |
| Methods | RCT |
| Participants | Target N = 50 Inclusion criteria: aged 7 to 14; diagnosed with Autism Spectrum Disorder and experiencing anxiety symptoms impairing their quality of life Exclusion criteria: IQ under 70; not meeting diagnostic criteria for primary anxiety diagnosis on ADIS; active psychosis; untreated Attention Deficit Hyperactivity Disorder; families not able to follow programme |
| Interventions | CBT (Cool Kids ASD) vs waitlist |
| Outcomes | Primary outcomes: ADIS (baseline, 14 weeks, 3 months) |
| Starting date | August 2016 |
| Contact information | Tina R Kilburn Centre for Child and Adolescent Psychiatry Risskov, Region Of Midtjylland, Denmark, 8240 tinakilb@rm.dk |
| Notes | clinicaltrials.gov/show/nct02908321 |
NCT03279471.
| Study name | Specifying and treating the anxiety phenotype in autism spectrum disorder |
| Methods | RCT |
| Participants | Target N = 132 Inclusion criteria: age 8 to 14; meets criteria for a diagnosis of ASD; clinically significant anxiety symptoms (minimum score of 8 on the Pediatric Anxiety Rating Scale); clinically significant anxiety symptoms as defined by qualifying for a diagnosis on 1 or more non‐phobia items on the ADIS; full‐scale and verbal comprehension IQ greater than 50; anxiety symptoms are considered the primary mental health problem (i.e. most impairing/distressing); stable medication, non‐psychotherapy and psychosocial regimen |
| Interventions | CBT vs drug (sertraline) vs pill placebo |
| Outcomes | Primary outcome: change in Pediatric Anxiety Rating Scale (pretreatment, post‐treatment, 3‐month follow‐up) |
| Starting date | 1 November 2017 |
| Contact information | Brianna Health, PhD UC Davis MIND Institute Sacramento, California, USA, 95817 bheath@ucdavis.edu |
| Notes | clinicaltrials.gov/ct2/show/nct03279471 |
NCT03585010.
| Study name | Brain response associated with parent‐based treatment for childhood anxiety disorders |
| Methods | RCT |
| Participants | Target N = 226 Inclusion criteria: prepubertal; clinical diagnosis of primary anxiety disorder; must not have another mental illness more impairing than the most impairing anxiety disorder; IQ of at least 80 |
| Interventions | Supportive Parenting for Anxious Child Emotions vs CBT vs parent educational support |
| Outcomes | Primary outcome: Pediatric Anxiety Rating Scale (PARS) (12 weeks) Secondary outcome: Multidimensional Anxiety Scale for Children (MASC) parent and child report (12 weeks) |
| Starting date | 1 September 2018 |
| Contact information | Eli R Lebowitz, PhD Yale University Child Study Center New Haven, Connecticut, USA, 06519 eli.lebowitz@yale.edu |
| Notes | clinicaltrials.gov/ct2/show/NCT03585010 |
ADIS: Anxiety Disorder Interview Schedule for Children CBT: cognitive behavioural therapy IQ: intelligence quotient MRI: magnetic resonance imaging RCT: randomised controlled trial
Differences between protocol and review
The criteria used to assess the eligibility of studies for inclusion in this review differed from previous versions of this review (e.g. this review included parent‐delivered CBT). We therefore used updated search strategies (see Appendix 2; Appendix 3).
We removed the 'active control' comparison, dividing this into two separate comparisons: attention controls and alternative treatments.
As there were a large number of eligible studies (> 80), we only included studies that met the defined eligibility criteria and reported (or the author provided) data on at least one of the specified primary or secondary outcomes.
We removed the requirement for therapists to receive regular supervision. Supervision arrangements varied widely across studies and were not always specified, even where it was suspected to be in place. Rather than specifying supervision as a requirement, we assessed therapy integrity (including therapist competence and adherence) as part of the 'Risk of bias' assessment in all included studies.
In the protocol, we specified that participants meet diagnostic criteria for an anxiety disorder. In the review, we clarified that these baseline diagnoses were made by reliable and valid structured interviews for Diagnostic and Statistical Manual of Mental Disorders (DSM) or International Classification of Diseases (ICD) child and adolescent anxiety disorders (to be consistent with measures required for diagnostic outcomes).
Where broad anxiety symptom measures and disorder‐specific symptom measures were reported, we prioritised broad anxiety symptom measures. We also conducted sensitivity analyses for child‐ and parent‐reported anxiety symptom measures, removing studies that only reported disorder‐specific symptom measures.
Child Behaviour Checklist ‐ Internalising Scale was not included as an anxiety symptom measure, as it is not designed to assess only anxiety symptoms.
Subgroup analyses.
We undertook subgroup analyses for the primary outcome (remission of primary anxiety disorder) across comparisons. For the main comparison with the largest number of studies (CBT versus waitlist/no treatment), we also undertook subgroup analyses for the most frequently reported secondary anxiety symptom outcomes (remission of all anxiety diagnoses post‐treatment, and reduction in child‐ and parent‐reported anxiety symptoms post‐treatment).
CBT interventions were delivered either individually or in a group format, and also varied in terms of the amount of parental involvement (child‐focused, child and parent, parent‐only). We therefore undertook separate subgroup analyses to examine the differences between individual versus group formats, and child‐focused, child‐and‐parent, and parent‐only formats. We also provided a more detailed description of 'child‐focused' and 'child‐and‐parent' interventions than was given in the protocol.
In order to examine the differences between interventions with varying amount of therapist contact time, we planned to use four subgroups; however, we collapsed two of these subgroups due to the small number of studies with < 10 hours therapist contact time. We therefore examined differences between < 10 hours, ≥ 10 hours and < 20 hours, and ≥ 20 hours.
In order to evaluate differences between different ages, we undertook subgroup analyses to examine differences between studies with participants ≤ 12 years, ≥ 12 years, and mixed age range including participants < 12 and participants ≥ 12 years.
As the above subgroup analyses were conducted, meta‐regression analyses were not required.
In order to ensure that subgroup analyses were meaningful, we only undertook these analyses where data were available from at least three studies for each subgroup.
We made minor changes to the Background to reflect up‐to‐date evidence and to ensure that the order in which relevant issues/objectives/results were presented was as consistent as possible throughout the review.
Contributions of authors
Anthony James and Tessa Reardon reviewed all papers; Angela Soler reviewed papers in Spanish; and Georgina James and Cathy Creswell reviewed papers where there was any disagreement. Anthony James and Tessa Reardon extracted study data, contacted study authors, and assessed risk of bias, and were responsible for statistical analyses. Anthony James, Tessa Reardon, and Cathy Creswell were jointly responsible for interpreting the data and analyses and drafting the text of the review. All authors contributed to revising and finalising the text.
Sources of support
Internal sources
Oxford Healthcare NHS Foundation Trust, UK
Oxford University Department of Psychiatry, Warneford Hospital, Oxford, UK
External sources
-
National Institute for Health Research (NIHR) Research Professorship, UK
Cathy Creswell and Tessa Reardon are funded by an NIHR Research Professorship to Cathy Creswell (NIHR‐RP‐2014‐04‐018). This study presents independent research partly funded by the NIHR.
Declarations of interest
Anthony James: nothing to declare Tessa Reardon was funded by a National Institute for Health Research (NIHR) Research Professorship to Cathy Creswell. This study presents independent research partly funded by the NIHR. Angela Soler: nothing to declare Georgina James: nothing to declare Cathy Creswell was funded by an NIHR Research Professorship. This study presents independent research partly funded by the NIHR.
New
References
References to studies included in this review
Afshari 2014 {published data only (unpublished sought but not used)}
- Afshari A, Neshat-Doost HT, Maracy M, Ahmady MK, Amiri S. The effective comparison between emotion-focused cognitive behavioral group therapy and cognitive behavioral group therapy in children with separation anxiety disorder. Journal of Research in Medical Sciences 2014;19(3):221-7. [PMC free article] [PubMed] [Google Scholar]
Arendt 2016 {published data only (unpublished sought but not used)}
- Arendt K, Thastum M, Hougaard E. Efficacy of a Danish version of the Cool Kids program: a randomized wait-list controlled trial. Acta Psychiatrica Scandinavica 2016;133(2):109-21. [DOI: 10.1111/acps.12448] [DOI] [PubMed] [Google Scholar]
Barrett 1996 {published data only (unpublished sought but not used)}
- Barrett PM, Dadds MR, Rapee RM. Family treatment of childhood anxiety: a controlled trial. Journal of Consulting and Clinical Psychology 1996;64(2):333-42. [DOI] [PubMed] [Google Scholar]
Barrett 1998 {published data only (unpublished sought but not used)}
- Barrett PM. Evaluation of cognitive-behavioral group treatments for childhood anxiety disorders. Journal of Clinical Child Psychology 1998;27(4):459-68. [DOI: 10.1207/s15374424jccp2704_10] [DOI] [PubMed] [Google Scholar]
Barrington 2005 {published data only (unpublished sought but not used)}
- Barrington J, Prior M, Richardson M, Allen K. Effectiveness of CBT versus standard treatment for childhood anxiety disorders in a community clinic setting. Behaviour Change 2005;22(1):29-43. [DOI: 10.1375/bech.22.1.29.66786] [DOI] [Google Scholar]
Berge 2017 {published data only}
- *.Berge KG, Agdal ML, Vika M, Skeie MS. Treatment of intra-oral injection phobia: a randomized delayed intervention controlled trial among Norwegian 10- to 16-year-olds. Acta Odontologica Scandinavica 2017;75(4):294-301. [DOI: 10.1080/00016357.2017.1297849] [DOI] [PubMed] [Google Scholar]
- NCT02083432. Cognitive behavioural treatment of intra-oral Injection-phobia in 10-16 year old children and adolescents. clinicaltrials.gov/show/nct02083432 (first received 11 March 2014).
Cartwright Hatton 2011 {published data only (unpublished sought but not used)}
- Cartwright-Hatton S, McNally D, Field AP, Rust S, Laskey B, Dixon B, et al. A new parenting-based group intervention for young anxious children: results of a randomized controlled trial. Journal of the American Academy of Child and Adolescent Psychiatry 2011;50(3):242-51. [10.1016/j.jaac.2010.12.015 ] [DOI] [PubMed] [Google Scholar]
Chalfant 2007 {published data only (unpublished sought but not used)}
- Chalfant AM, Rapee R, Carroll L. Treating anxiety disorders in children with high functioning autism spectrum disorders: a controlled trial. Journal of Autism and Developmental Disorders 2007;37(10):1842-57. [DOI: 10.1007/s10803-006-0318-4] [DOI] [PubMed] [Google Scholar]
Cheung 2016 {published data only}
- Cheung MC. Effectiveness of Attention Bias Modification Treatment for Children With Social Anxiety Problem [Thesis]. Pokfulam, Hong Kong: The University of Hong Kong, 2016. [hub.hku.hk/handle/10722/239961] [Google Scholar]
Chiu 2013 {published data only (unpublished sought but not used)}
- *.Chiu AW, Langer DA, McLeod BD, Har K, Drahota A, Galla BM, et al. Effectiveness of modular CBT for child anxiety in elementary schools. School Psychology Quarterly 2013;28(2):141-53. [DOI: 10.1037/spq0000017] [DOI] [PMC free article] [PubMed] [Google Scholar]
- NCT00569829. Modular cognitive behavioral therapy for the treatment of child anxiety disorders in elementary school settings. clinicaltrials.gov/show/nct00569829 (first received 7 December 2007).
Cobham 2017 {published data only}
- Cobham VE, Filus A, Sanders MR. Working with parents to treat anxiety-disordered children: a proof of concept RCT evaluating Fear-less Triple P. Behaviour Research and Therapy 2017;95:128-38. [DOI: 10.1016/j.brat.2017.06.004] [DOI] [PubMed] [Google Scholar]
Cornacchio 2019 {published data only (unpublished sought but not used)}
- *.Cornacchio D, Furr JM, Sanchez AL, Hong N, Feinberg LK, Tenenbaum R, et al. Intensive group behavioral treatment (IGBT) for children with selective mutism: a preliminary randomized clinical trial. Journal of Consulting and Clinical Psychology 2019;87(8):720-33. [DOI: 10.1037/ccp0000422] [DOI] [PMC free article] [PubMed] [Google Scholar]
- NCT03612102. Evaluating intensive group behavioral treatment for children with selective mutism. clinicaltrials.gov/show/nct03612102 (first received 2 August 2018).
Creswell 2017 {published and unpublished data}
- *.Creswell C, Violato M, Fairbanks H, White E, Parkinson M, Abitabile G, et al. Clinical outcomes and cost-effectiveness of brief guided parent-delivered cognitive behavioural therapy and solution-focused brief therapy for treatment of childhood anxiety disorders: a randomised controlled trial. Lancet Psychiatry 2017;4(7):529-39. [DOI: 10.1016/S2215-0366(17)30149-9] [DOI] [PMC free article] [PubMed] [Google Scholar]
- ISRCTN07627865. Guided self-help for childhood anxiety problems: a comparison with usual care. www.isrctn.com/ISRCTN07627865 (first received 13 March 2012).
Dadds 1997 {published and unpublished data}
- Dadds MR, Holland DE, Laurens KR, Mullins M, Barrett PM, Spence SH. Early intervention and prevention of anxiety disorders in children: results at 2-year follow-up. Journal of Consulting and Clinical Psychology 1999;67(1):145-50. [DOI] [PubMed] [Google Scholar]
- *.Dadds MR, Spence SH, Holland DE, Barrett PM, Laurens KR. Prevention and early intervention for anxiety disorders: a controlled trial. Journal of Consulting and Clinical Psychology 1997;65(4):627-35. [DOI] [PubMed] [Google Scholar]
Flannery Schroeder 2000 {published data only (unpublished sought but not used)}
- *.Flannery-Schroeder EC, Kendall PC. Group and individual cognitive-behavioral treatments for youth with anxiety disorders: a randomized clinical trial. Cognitive Therapy and Research 2000;24(3):251-78. [DOI: 10.1023/A:1005500219286] [DOI] [Google Scholar]
Fujii 2013 {published data only (unpublished sought but not used)}
- Fujii C, Renno P, McLeod BD, Lin CE, Decker K, Zielinski K, et al. Intensive cognitive behavioral therapy for anxiety disorders in school-aged children with autism: a preliminary comparison with treatment-as-usual. School Mental Health 2013;5(1):25-37. [DOI: 10.1007/s12310-012-9090-0] [DOI] [Google Scholar]
Gallagher 2004 {published data only (unpublished sought but not used)}
- *.Gallagher HM, Rabian BA, McCloskey MS. A brief group cognitive-behavioral intervention for social phobia in childhood. Journal of Anxiety Disorders 2004;18(4):459-79. [DOI: 10.1016/S0887-6185(03)00027-6] [DOI] [PubMed] [Google Scholar]
Ginsburg 2002 {published data only}
- Ginsburg GS, Drake KL. School-based treatment for anxious African-American adolescents: a controlled pilot study. Journal of the American Academy of Child and Adolescent Psychiatry 2002;41(7):768-75. [DOI: 10.1097/00004583-200207000-00007] [DOI] [PubMed] [Google Scholar]
Ginsburg 2012 {published data only (unpublished sought but not used)}
- *.Ginsburg GS, Becker KD, Drazdowski TK, Tein J. Treating anxiety disorders in inner city schools: results from a pilot randomized controlled trial comparing CBT and usual care. Child and Youth Care Forum 2012;41(1):1-19. [DOI: 10.1007/s10566-011-9156-4 ] [DOI] [PMC free article] [PubMed] [Google Scholar]
- NCT00536094. School-based treatment for anxious children. clinicaltrials.gov/show/nct00536094 (first received 27 September 2007).
Ginsburg 2019a {published data only (unpublished sought but not used)}
- *.Ginsburg GS, Pella JE, Pikulski PJ, Tein JY, Drake KL. School-Based Treatment for Anxiety Research Study (STARS): a randomized controlled effectiveness trial. Journal of Abnormal Child Psychology 2019;48(3):407-17. [10.1007/s10802-019-00596-5 ] [DOI] [PubMed] [Google Scholar]
- NCT01761396. School-based Treatment of Anxiety Research Study (STARS). clinicaltrials.gov/show/nct01761396 (first received 4 January 2013).
Hancock 2018 {published data only (unpublished sought but not used)}
- ACTRN12611001280998. Efficacy of acceptance-mindfulness therapy in children with anxiety: a controlled trial. www.who.int/trialsearch/Trial2.aspx?TrialID=ACTRN12611001280998 (first received 13 December 2011).
- *.Hancock KM, Swain J, Hainsworth CJ, Dixon AL, Koo S, Munro K. Acceptance and commitment therapy versus cognitive behavior therapy for children with anxiety: outcomes of a randomized controlled trial. Journal of Clinical Child and Adolescent Psychology 2018;47(2):296-311. [DOI: 10.1080/15374416.2015.1110822] [DOI] [PubMed] [Google Scholar]
- Swain J, Hancock K, Dixon A, Koo S, Bowman J. Acceptance and commitment therapy for anxious children and adolescents: study protocol for a randomized controlled trial. Trials 2013;14:140. [DOI: 10.1186/1745-6215-14-140] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Swain J, Hancock K, Hainsworth C, Bowman J. Mechanisms of change: exploratory outcomes from a randomised controlled trial of acceptance and commitment therapy for anxious adolescents. Journal of Contextual Behavioral Science 2015;4(1):56-67. [DOI: 10.1016/j.jcbs.2014.09.001] [DOI] [Google Scholar]
Herbert 2009 {published data only (unpublished sought but not used)}
- Herbert JD, Gaudiano BA, Rheingold AA, Moitra E, Myers VH, Dalrymple KL, et al. Cognitive behavior therapy for generalized social anxiety disorder in adolescents: a randomized controlled trial. Journal of Anxiety Disorders 2009;23(2):167-77. [DOI: 10.1016/j.janxdis.2008.06.004] [DOI] [PMC free article] [PubMed] [Google Scholar]
Hirshfeld Becker 2010 {published and unpublished data}
- *.Hirshfeld-Becker DR, Masek B, Henin A, Blakely LR, Pollock-Wurman RA, McQuade J, et al. Cognitive behavioural therapy for 4- to 7-year old children with anxiety disorders: a randomized clinical trial. Journal of Consulting and Clinical Psychology 2010;78(4):498-510. [DOI: 10.1037/a0019055] [DOI] [PubMed] [Google Scholar]
- NCT00865306. Early intervention for children at risk for anxiety. clinicaltrials.gov/show/nct00865306 (first received 19 March 2009).
Holmes 2014 {published data only (unpublished sought but not used)}
- Holmes MC, Donovan CL, Farrell LJ, March S. The efficacy of a group-based, disorder-specific treatment program for childhood GAD - a randomized controlled trial. Behaviour Research and Therapy 2014;61:122-35. [DOI: 10.1016/j.brat.2014.08.002] [DOI] [PubMed] [Google Scholar]
Hudson 2009 {published data only}
- Hudson JL, Rapee RM, Deveney C, Schniering CA, Lyneham HJ, Bovopoulos N. Cognitive-behavioral treatment versus an active control for children and adolescents with anxiety disorders: a randomized trial. Journal of the American Academy of Child and Adolescent Psychiatry 2009;48(5):533-44. [DOI: 10.1097/CHI.0b013e31819c2401] [DOI] [PubMed] [Google Scholar]
Ingul 2013 {published data only}
- Ingul JM, Aune T, Nordahl HM. A randomized controlled trial of individual cognitive therapy, group cognitive behaviour therapy and attentional placebo for adolescent social phobia. Psychotherapy and Psychosomatics 2013;83(1):54-61. [DOI: 10.1159/000354672] [DOI] [PubMed] [Google Scholar]
Ishikawa 2019 {published data only}
- Ishikawa S, Kikuta K, Sakai M, Mitamura T, Motomura N, Hudson JL. A randomized controlled trial of a bidirectional cultural adaptation of cognitive behavior therapy for children and adolescents with anxiety disorders. Behaviour Research and Therapy 2019;120:103432. [DOI: 10.1016/j.brat.2019.103432] [DOI] [PubMed] [Google Scholar]
Kendall 1994 {published and unpublished data}
- Kendall PC. Treating anxiety disorders in youth: results of a randomized clinical trial. Journal of Consulting and Clinical Psychology 1994;62(1):100-10. [DOI] [PubMed] [Google Scholar]
Kendall 1997 {published data only (unpublished sought but not used)}
- Kendall PC, Flannery-Schroeder E, Panichelli-Mindel SM, Southam-Gerow M, Henin A, Warman M. Therapy for youths with anxiety disorders: a second randomized clinical trial. Journal of Consulting and Clinical Psychology 1997;65(3):366-80. [DOI] [PubMed] [Google Scholar]
Kendall 2008 {published and unpublished data}
- *.Kendall PC, Hudson JL, Gosch E, Flannery-Schroeder E, Suveg C. Cognitive-behavioral therapy for anxiety disordered youth: a randomized clinical trial evaluating child and family modalities. Journal of Consulting and Clinical Psychology 2008;76(2):282-97. [DOI: 10.1037/0022-006X.76.2.282] [DOI] [PubMed] [Google Scholar]
- NCT00081406. Individual and family therapy for children with anxiety disorders. clinicaltrials.gov/show/nct00081406 (first received 12 April 2004).
- Suveg CH, Hudson JL, Brewer G, Flannery-Schroeder E, Gosch E, Kendall PC. Cognitive-behavioral therapy for anxiety-disordered youth: secondary outcomes from a randomized clinical trial evaluating child and family modalities. Journal of Anxiety Disorders 2009;23(3):341-9. [DOI: 10.1016/j.janxdis.2009.01.003] [DOI] [PubMed] [Google Scholar]
Kennedy 2009 {published data only (unpublished sought but not used)}
- Kennedy SJ, Rapee RM, Edwards SL. A selective intervention program for inhibited preschool-aged children of parents with an anxiety disorder: effects on current anxiety disorders and temperament. Journal of the American Academy of Child and Adolescent Psychiatry 2009;48(6):602-9. [DOI: 10.1097/CHI.0b013e31819f6fa9] [DOI] [PubMed] [Google Scholar]
Khanna 2010 {published data only (unpublished sought but not used)}
- Khanna MS, Kendall PC. Computer-assisted cognitive behavioral therapy for child anxiety: results of a randomized clinical trial. Journal of Consulting and Clinical Psychology 2010;78(5):737-45. [DOI: 10.1037/a0019739] [DOI] [PubMed] [Google Scholar]
Kidd 2018 {published data only}
- ACTRN12610001014044. Assessing the efficacy and social validity of a manualised, family-based group Cognitive Behavioural Therapy for adolescents with high-functioning autism and comorbid anxiety disorder. www.who.int/trialsearch/Trial2.aspx?TrialID=ACTRN12610001014044 (first received 19 November 2010).
- *.Kidd TC. Treating Anxiety in Adolescents With Autism Spectrum Disorder Using Group Cognitive Behaviour Therapy: A Randomised Controlled Trial [Doctoral thesis]. Perth, Western Australia: Curtin University, 2018. [hdl.handle.net/20.500.11937/73526] [Google Scholar]
Last 1998 {published data only}
- Last CG, Hansen C, Franco N. Cognitive-behavioral treatment of school phobia. Journal of the American Academy of Child and Adolescent Psychiatry 1998;37(4):404-11. [DOI: 10.1097/00004583-199804000-00018] [DOI] [PubMed] [Google Scholar]
Lau 2010 {published and unpublished data}
- Lau WY, Chan CK, Li JC, Au TK. Effectiveness of group cognitive-behavioral treatment for childhood anxiety in community clinics. Behaviour Research and Therapy 2010;48(11):1067-77. [DOI: 10.1016/j.brat.2010.07.007] [DOI] [PubMed] [Google Scholar]
Lau 2017 {published data only (unpublished sought but not used)}
- Lau EX, Rapee RM, Coplan RJ. Combining child social skills training with a parent early intervention program for inhibited preschool children. Journal of Anxiety Disorders 2017;51:32-8. [DOI: 10.1016/j.janxdis.2017.08.007] [DOI] [PubMed] [Google Scholar]
Lebowitz 2019 {published data only (unpublished sought but not used)}
- *.Lebowitz ER, Marin C, Martino A, Shimshoni Y, Silverman WK. Parent-based treatment as efficacious as cognitive-behavioral therapy for childhood anxiety: a randomized noninferiority study of supportive parenting for anxious childhood emotions. Journal of the American Academy of Child and Adolescent Psychiatry 2019 Mar 7 [Epub ahead of print]. [DOI: 10.1016/j.jaac.2019.02.014] [DOI] [PMC free article] [PubMed]
- Lebowitz ER, Marin C, Martino A, Shimshoni Y, Silverman WK. Parent-based treatment as efficacious as cognitive-behavioral therapy for childhood anxiety: a randomized noninferiority study of supportive parenting for anxious childhood emotions. Journal of the American Academy of Child and Adolescent Psychiatry 2020;59(3):362-72. [DOI: 10.1016/j.jaac.2019.02.014] [DOI] [PMC free article] [PubMed] [Google Scholar]
- NCT02310152. Explanatory clinical trial of a novel parent intervention for childhood anxiety (SPACE). clinicaltrials.gov/show/nct02310152 (first received 5 December 2014).
Leutgeb 2012 {published data only}
- Leutgeb V, Schienle A. Changes in facial electromyographic activity in spider-phobic girls after psychotherapy. Journal of Psychiatric Research 2012;46(6):805-10. [DOI: 10.1016/j.jpsychires.2012.02.017] [DOI] [PMC free article] [PubMed] [Google Scholar]
Masia Warner 2005 {published data only (unpublished sought but not used)}
- Masia Warner C, Klein RG, Dent HC, Fisher PH, Alvir J, Albano AM, et al. School-based intervention for adolescents with social anxiety disorder: results of a controlled study. Journal of Abnormal Child Psychology 2005;33(6):707-22. [DOI: 10.1007/s10802-005-7649-z] [DOI] [PubMed] [Google Scholar]
Masia Warner 2007 {published data only}
- Masia Warner C, Fisher PH, Shrout PE, Rathor S, Klein RG. Treating adolescents with social anxiety disorder in school: an attention control trial. Journal of Child Psychology and Psychiatry and Allied Disciplines 2007;48(7):676-86. [DOI: 10.1111/j.1469-7610.2007.01737.x] [DOI] [PubMed] [Google Scholar]
Masia Warner 2011 {published data only (unpublished sought but not used)}
- Masia Warner C, Colognori D, Kim RE, Reigada LC, Klein RG, Browner-Elhanan KJ, et al. Cognitive-behavioral treatment of persistent functional somatic complaints and pediatric anxiety: an initial controlled trial. Depression and Anxiety 2011;28(7):551-9. [DOI: 10.1002/da.20821] [DOI] [PMC free article] [PubMed] [Google Scholar]
Masia Warner 2016 {published data only (unpublished sought but not used)}
- *.Masia Warner C, Colognori D, Brice C, Herzig K, Mufson L, Lynch C, et al. Can school counselors deliver cognitive-behavioral treatment for social anxiety effectively? A randomized controlled trial. Journal of Child Psychology and Psychiatry and Allied Disciplines 2016;57(11):1229-38. [DOI: 10.1111/jcpp.12550] [DOI] [PubMed] [Google Scholar]
- NCT01320800. CBT for social anxiety disorder delivered by school counselors. clinicaltrials.gov/show/nct01320800 (first received 22 March 2011).
McConachie 2014 {published data only}
- ISRCTN11219568. Effective therapy for anxiety in young people with autism spectrum disorder. www.isrctn.com/ISRCTN11219568 (first received 12 May 2010).
- *.McConachie H, McLaughlin E, Grahame V, Taylor H, Honey E, Tavernor L, et al. Group therapy for anxiety in children with autism spectrum disorder. Autism 2014;18(6):723-32. [DOI: 10.1177/1362361313488839] [DOI] [PubMed] [Google Scholar]
McNally Keehn 2013 {published data only (unpublished sought but not used)}
- McNally Keehn RH, Lincoln AJ, Brown MZ, Chavira DA. The Coping Cat program for children with anxiety and autism spectrum disorder: a pilot randomized controlled trial. Journal of Autism and Developmental Disorders 2013;43(1):57-67. [DOI: 10.1007/s10803-012-1541-9] [DOI] [PMC free article] [PubMed] [Google Scholar]
Melfsen 2011 {published and unpublished data}
- Melfsen S, Kuhnemund M, Schwieger J, Warnke A, Stadler C, Poustka F, et al. Cognitive behavioral therapy of socially phobic children focusing on cognition: a randomised wait-list control study. Child and Adolescent Psychiatry and Mental Health 2011;5:ArtID2. [DOI: 10.1186/1753-2000-5-5] [DOI] [PMC free article] [PubMed] [Google Scholar]
Muris 2002 {published data only}
- Muris P, Meesters C, Melick M. Treatment of childhood anxiety disorders: a preliminary comparison between cognitive-behavioral group therapy and a psychological placebo intervention. Journal of Behavior Therapy and Experimental Psychiatry 2002;33(3-4):143-58. [DOI] [PubMed] [Google Scholar]
Murphy 2017 {published data only (unpublished sought but not used)}
- Murphy SM, Chowdhury U, White SW, Reynolds L, Donald L, Gahan H, et al. Cognitive behaviour therapy versus a counselling intervention for anxiety in young people with high-functioning autism spectrum disorders: a pilot randomised controlled trial. Journal of Autism and Developmental Disorders 2017;47(11):3446-57. [DOI: 10.1007/s10803-017-3252-8] [DOI] [PMC free article] [PubMed] [Google Scholar]
O'Brien 2007 {published data only (unpublished sought but not used)}
- O'Brien F, Olden N, Migone M, Dooley B, Atkins L, Ganter K, et al. Group cognitive behavioural therapy for children with anxiety disorder - an evaluation of the 'Friends for Youth' programme. Irish Journal of Psychological Medicine 2007;24(1):5-12. [DOI] [PubMed] [Google Scholar]
Olivares 2005 {published and unpublished data}
- Olivares J, Rosa-Alcazar AI, Piqueras JA. Early detection and treatment of adolescents with generalized social phobia. Psicothema 2005;17(1):1-8. [Google Scholar]
Olivares 2014 {published data only}
- Olivares J, Olivares-Olivares PJ, Rosa-Alcazar AI, Montesinos L, Macia D. The contribution of the therapist's competence in the treatment of adolescents with generalized social phobia. Psicothema 2014;26(4):483-9. [DOI] [PubMed] [Google Scholar]
Olivares 2019 {published data only}
- Olivares-Olivares PJ, Ortiz-González PF, Olivares J. Role of social skills training in adolescents with social anxiety disorder. International Journal of Clinical and Health Psychology 2019;19(1):41-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
Ollendick 2009 {published data only}
- Ollendick TH, Ost LG, Reuterskiold L, Costa N, Cederlund R, Sirbu C, et al. One-session treatment of specific phobias in youth: a randomized clinical trial in the United States and Sweden. Journal of Consulting and Clinical Psychology 2009;77(3):504-16. [DOI: 10.1037/a0015158] [DOI] [PubMed] [Google Scholar]
Ost 2001 {published and unpublished data}
- Ost LG, Svensson L, Hellstrom K, Lindwall R. One-session treatment of specific phobias in youths: a randomized clinical trial. Journal of Consulting and Clinical Psychology 2001;69(5):814-24. [DOI: 10.1037/0022-006X.69.5.814] [DOI] [PubMed] [Google Scholar]
Perrin 2019 {published data only}
- ISRCTN50951795. Cognitive therapy for generalised anxiety in youth. www.isrctn.com/ISRCTN50951795 (first received 30 June 2010).
- *.Perrin S, Bevan D, Payne S, Bolton D. GAD-specific cognitive behavioral treatment for children and adolescents: a pilot randomized controlled trial. Cognitive Therapy and Research 2019;43(6):1051-64. [DOI: 10.1007/s10608-019-10020-3] [DOI] [Google Scholar]
Pincus 2010 {published data only (unpublished sought but not used)}
- NCT00705380. Effectiveness of cognitive behavioral therapy with panic control treatment for adolescents with panic disorder. clinicaltrials.gov/show/nct00705380 (first received 25 June 2008).
- *.Pincus DB, May JE, Whitton SW, Mattis SG, Barlow DH. Cognitive-behavioral treatment of panic disorder in adolescence. Journal of Clinical Child and Adolescent Psychology 2010;39(5):638-49. [DOI: 10.1080/15374416.2010.501288] [DOI] [PubMed] [Google Scholar]
Rapee 2005 {published and unpublished data}
- *.Rapee RM, Kennedy S, Ingram M, Edwards S, Sweeney L. Prevention and early intervention of anxiety disorders in inhibited preschool children. Journal of Consulting and Clinical Psychology 2005;73(3):488-97. [DOI: 10.1037/0022-006X.73.3.488] [DOI] [PubMed] [Google Scholar]
- Rapee RM, Kennedy SJ, Ingram M, Edwards SL, Sweeney L. Altering the trajectory of anxiety in at-risk young children. American Journal of Psychiatry 2010;167(12):1518-25. [DOI: 10.1176/appi.ajp.2010.09111619] [DOI] [PubMed] [Google Scholar]
- Rapee RM. The preventative effects of a brief, early intervention for preschool-aged children at risk for internalising: follow-up into middle adolescence. Journal of Child Psychology & Psychiatry 2013;54(7):780-8. [DOI: 10.1111/jcpp.12048] [DOI] [PubMed] [Google Scholar]
Rapee 2006 {published and unpublished data}
- Rapee RM, Abbott MJ, Lyneham HJ. Bibliotherapy for children with anxiety disorders using written materials for parents: a randomized controlled trial. Journal of Consulting and Clinical Psychology 2006;74(3):436-44. [DOI: 10.1037/0022-006X.74.3.436] [DOI] [PubMed] [Google Scholar]
Reaven 2012 {published data only}
- Reaven J, Blakeley-Smith A, Culhane-Shelburne K, Hepburn S. Group cognitive behavior therapy for children with high-functioning autism spectrum disorders and anxiety: a randomized trial. Journal of Child Psychology and Psychiatry and Allied Disciplines 2012;53(4):410-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
Reigada 2015 {published and unpublished data}
- Reigada LC, Polokowski AR, Walder DJ, Szigethy EM, Benkov KJ, Bruzzese JM, et al. Treatment for comorbid pediatric gastrointestinal and anxiety disorders: a pilot study of a flexible health sensitive cognitive-behavioral therapy program. Clinical Practice in Pediatric Psychology 2015;3(4):314-26. [DOI: 10.1037/cpp0000116] [DOI] [Google Scholar]
Rosa Alcazar 2009 {published and unpublished data}
- Rosa-Alcazar AI, Olivares-Olivares PJ, Olivares J. The role of non-specific effects in the psychological treatment of adolescents with social phobia. Anuario de Psicologia 2009;40(1):43-61. [Google Scholar]
Salari 2018 {published and unpublished data}
- NCT01513915. A parent-only group cognitive behavioral intervention for children with anxiety disorders: a control group study. clinicaltrials.gov/show/nct01513915 (first received 20 January 2012).
- *.Salari E, Shahrivar Z, Mahmoudi-Gharaei J, Shirazi E, Sepasi M. Parent-only group cognitive behavioral intervention for children with anxiety disorders: a control group study. Journal of the Canadian Academy of Child and Adolescent Psychiatry 2018;27(2):130-6. [PMC free article] [PubMed] [Google Scholar]
Salum 2018 {published data only}
- NCT01687764. Combination of active or placebo Attentional Bias Modification Treatment (ABMT) to either Cognitive Behavioral Group Therapy (CBGT) or Psychoeducational Control Intervention (PCI) for anxiety disorders in children: a randomized clinical trial. https://www.clinicaltrials.gov/ct2/show/NCT01687764 19 September 2012.
- *.Salum GA, Petersen CS, Jarros RB, Toazza R, DeSousa D, Borba LN, et al. Group cognitive behavioral therapy and attention bias modification for childhood anxiety disorders: a factorial randomized trial of efficacy. Journal of Child and Adolescent Psychopharmacology 2018;28(9):620-30. [DOI: 10.1089/cap.2018.0022] [DOI] [PMC free article] [PubMed] [Google Scholar]
Sanchez Garcia 2009 {published and unpublished data}
- Sanchez-Garcia R, Olivares J. Effectiveness of a program for early detection/intervention in children/adolescents with generalized social phobia. Anales de Psicologia 2009;25(2):241-9. [Google Scholar]
Santucci 2013 {published data only (unpublished sought but not used)}
- Santucci LC, Ehrenreich-May J. A randomized controlled trial of the child anxiety multi-day program (CAMP) for separation anxiety disorder. Child Psychiatry and Human Development 2013;44(3):439-51. [DOI: 10.1007/s10578-012-0338-6] [DOI] [PMC free article] [PubMed] [Google Scholar]
Schneider 2011 {published data only (unpublished sought but not used)}
- Schneider S, Blatter-Meunier J, Herren C, Adornetto C, In-Albon T, Lavallee K. Disorder-specific cognitive-behavioral therapy for separation anxiety disorder in young children: a randomized waiting-list-controlled trial. Psychotherapy and Psychosomatics 2011;80(4):206-15. [DOI: 10.1159/000323444] [DOI] [PubMed] [Google Scholar]
Sciberras 2018 {published data only (unpublished sought but not used)}
- ISRCTN33930984. Does the identification and treatment of comorbid anxiety disorders in children with attention deficit hyperactivity disorder (ADHD) improve outcomes? www.isrctn.com/ISRCTN33930984 (first received 2 October 2013).
- *.Sciberras E, Mulraney M, Anderson V, Rapee RM, Nicholson JM, Efron D, et al. Managing anxiety in children with ADHD using cognitive-behavioral therapy: a pilot randomized controlled trial. Journal of Attention Disorders 2018;22(5):515-20. [DOI: 10.1177/1087054715584054] [DOI] [PubMed] [Google Scholar]
Shahnavaz 2016 {published data only}
- NCT01798355. Children and adolescents with dental anxiety - randomized controlled study of cognitive behavioral therapy. clinicaltrials.gov/show/nct01798355 (first received 25 February 2013).
- *.Shahnavaz S, Hedman E, Grindefjord M, Reuterskiold L, Dahllof G. Cognitive behavioral therapy for children with dental anxiety: a randomized controlled trial. JDR Clinical and Translational Research 2016;1(3):234-43. [DOI: 10.1177/2380084416661473] [DOI] [PMC free article] [PubMed] [Google Scholar]
Sharma 2017 {published and unpublished data}
- Sharma P, Mehta M, Sagar R. Efficacy of transdiagnostic cognitive-behavioral group therapy for anxiety disorders and headache in adolescents. Journal of Anxiety Disorders 2017;46:78-84. [DOI: 10.1016/j.janxdis.2016.11.001] [DOI] [PubMed] [Google Scholar]
Shortt 2001 {published data only}
- Shortt AL, Barrett PM, Fox TL. Evaluating the FRIENDS program: a cognitive-behavioral group treatment for anxious children and their parents. Journal of Clinical Child and Adolescent Psychology 2001;30(4):525-35. [DOI: 10.1207/S15374424JCCP3004_09] [DOI] [PubMed] [Google Scholar]
Silk 2018 {published and unpublished data}
- NCT00774150. Transdisciplinary studies of CBT for anxiety in youth: child anxiety treatment study. clinicaltrials.gov/show/nct00774150 (first received 17 October 2008).
- *.Silk JS, Tan PZ, Ladouceur CD, Meller S, Siegle GJ, McMakin DL, et al. A randomized clinical trial comparing individual cognitive behavioral therapy and child-centered therapy for child anxiety disorders. Journal of Clinical Child and Adolescent Psychology 2018;47(4):542-54. [DOI: 10.1080/15374416.2016.1138408] [DOI] [PMC free article] [PubMed] [Google Scholar]
Silverman 1999a {published data only (unpublished sought but not used)}
- Silverman WK, Kurtines WM, Ginsburg GS, Weems CF, Rabian B, Serafini LT. Contingency management, self-control, and education support in the treatment of childhood phobic disorders: a randomized clinical trial. Journal of Consulting and Clinical Psychology 1999;67(5):675-87. [DOI] [PubMed] [Google Scholar]
Silverman 1999b {published data only (unpublished sought but not used)}
- Silverman WK, Kurtines WM, Ginsburg GS, Weems CF, Lumpkin PW, Carmichael DH. Treating anxiety disorders in children with group cognitive-behavioral therapy: a randomized clinical trial. Journal of Consulting and Clinical Psychology 1999;67(6):995-1003. [DOI] [PubMed] [Google Scholar]
Simon 2011 {published and unpublished data}
- NTR1143. Prevention of childhood anxiety disorders via the parent or via the child? www.who.int/trialsearch/Trial2.aspx?TrialID=NTR1143 (first received 27 November 2007).
- *.Simon E, Bogels SM, Voncken JM. Efficacy of child-focused and parent-focused interventions in a child anxiety prevention study. Journal of Clinical Child and Adolescent Psychology 2011;40(2):204-19. [DOI: 10.1080/15374416.2011.546039] [DOI] [PubMed] [Google Scholar]
Smith 2014 {published data only (unpublished sought but not used)}
- *.Smith AM, Flannery-Schroeder EC, Gorman KS, Cook N. Parent cognitive-behavioral intervention for the treatment of childhood anxiety disorders: a pilot study. Behaviour Research and Therapy 2014;61:156-61. [DOI] [PubMed] [Google Scholar]
- Smith AM. Cognitive-behavioral treatment of childhood anxiety: examining a parent consultation model. Dissertation Abstracts International: Section B: The Sciences and Engineering 2014;74:8-B(E). [Google Scholar]
Southam Gerow 2010 {published data only (unpublished sought but not used)}
- Southam-Gerow MA, Weisz JR, Chu BC, McLeod BD, Gordis EB, Connor-Smith JK. Does cognitive behavioral therapy for youth anxiety outperform usual care in community clinics? An initial effectiveness test. Journal of the American Academy of Child and Adolescent Psychiatry 2010;49(10):1043-52. [DOI: 10.1016/j.jaac.2010.06.009] [DOI] [PMC free article] [PubMed] [Google Scholar]
Spence 2000 {published and unpublished data}
- Spence SH, Donovan C, Brechman-Toussaint M. The treatment of childhood social phobia: the effectiveness of a social skills training-based, cognitive-behavioural intervention, with and without parental involvement. Journal of Child Psychology and Psychiatry and Allied Disciplines 2000;41(6):713-26. [PubMed] [Google Scholar]
Spence 2006 {published data only}
- Spence SH, Holmes JM, March S, Lipp OV. The feasibility and outcome of clinic plus internet delivery of cognitive-behavior therapy for childhood anxiety. Journal of Consulting and Clinical Psychology 2006;74(3):614-21. [DOI: 10.1037/0022-006X.74.3.614] [DOI] [PubMed] [Google Scholar]
Spence 2011 {published data only}
- Spence SH, Donovan CL, March S, Gamble A, Anderson RE, Prosser S, et al. A randomized controlled trial of online versus clinic-based CBT for adolescent anxiety. Journal of Consulting and Clinical Psychology 2011;79(5):629-42. [DOI: 10.1037/a0024512] [DOI] [PubMed] [Google Scholar]
Storch 2013 {published data only}
- NCT01178385. Cognitive-behavioral treatment for anxiety disorders in children with autism spectrum disorders. clinicaltrials.gov/show/nct01178385 (first received 10 August 2010).
- *.Storch EA, Arnold EB, Lewin AB, Nadeau JM, Jones AM, De Nadai AS, et al. The effect of cognitive-behavioral therapy versus treatment as usual for anxiety in children with autism spectrum disorders: a randomized, controlled trial. Journal of the American Academy of Child and Adolescent Psychiatry 2013;52(2):132-42.e2. [DOI: 10.1016/j.jaac.2012.11.007] [DOI] [PubMed] [Google Scholar]
Storch 2015 {published data only}
- NCT01563003. Cognitive behavioral therapy for anxiety disorders in adolescents with autism. clinicaltrials.gov/show/nct01563003 (first received 26 March 2012).
- *.Storch EA, Lewin AB, Collier AB, Arnold E, De Nadai AS, Dane BF, et al. A randomized controlled trial of cognitive-behavioral therapy versus treatment as usual for adolescents with autism spectrum disorders and comorbid anxiety. Depression and Anxiety 2015;32(3):174-81. [DOI: 10.1002/da.22332] [DOI] [PMC free article] [PubMed] [Google Scholar]
Thirlwall 2013 {published data only}
- Thirlwall K, Cooper PJ, Karalus J, Voysey M, Willetts L, Creswell C. Treatment of child anxiety disorders via guided parent-delivered cognitive-behavioural therapy: randomised controlled trial. British Journal of Psychiatry 2013;203(6):436-44. [DOI: 10.1192/bjp.bp.113.126698] [DOI] [PubMed] [Google Scholar]
Villabo 2018 {published data only}
- NCT00735995. Effectiveness of cognitive behavioral therapy (CBT) for child anxiety disorders in community clinics in Norway. clinicaltrials.gov/show/nct00735995 (first received 15 August 2008).
- *.Villabo MA, Narayanan M, Compton SN, Kendall PC, Neumer SP. Cognitive-behavioral therapy for youth anxiety: an effectiveness evaluation in community practice. Journal of Consulting and Clinical Psychology 2018;86(9):751-64. [DOI: 10.1037/ccp0000326] [DOI] [PMC free article] [PubMed] [Google Scholar]
Walkup 2008 {published data only (unpublished sought but not used)}
- Albano AM, Comer JS, Compton SN, Piacentini J, Kendall PC, Birmaher B, et al. Secondary outcomes from the Child/Adolescent Anxiety Multimodal Study: implications for clinical practice. Evidence-Based Practice in Child and Adolescent Mental Health 2018;3(1):30-41. [DOI: 10.1080/23794925.2017.1399485] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Compton SN, Walkup JT, Albano AM, Piacentini JC, Birmaher B, Sherrill JT, et al. Child/Adolescent Anxiety Multimodal Study (CAMS): rationale, design, and methods. Child and Adolescent Psychiatry and Mental Health 2010;4:1. [DOI: 10.1186/1753-2000-4-1] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ginsburg GS, Becker EM, Keeton CP, Sakolsky D, Piacentini J, Albano AM, et al. Naturalistic follow-up of youths treated for pediatric anxiety disorders. JAMA Psychiatry 2014;71(3):310-8. [DOI: 10.1001/jamapsychiatry.2013.4186] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ginsburg GS, Becker-Haimes EM, Keeton C, Kendall PC, Lyengar S, Sakolsky D, et al. Results from the Child/Adolescent Anxiety Multimodal Extended Long-Term Study (CAMELS): primary anxiety outcomes. Journal of the American Academy of Child and Adolescent Psychiatry 2018;57(7):471-80. [DOI: 10.1016/j.jaac.2018.03.017] [DOI] [PubMed] [Google Scholar]
- Ginsburg GS, Kendall PC, Sakolsky D, Compton SN, Piacentini J, Albano AM, et al. Remission after acute treatment in children and adolescents with anxiety disorders: findings from the CAMS. Journal of Consulting and Clinical Psychology 2011;79(6):806-13. [DOI: 10.1037/a0025933] [DOI] [PMC free article] [PubMed] [Google Scholar]
- NCT00052078. Child and Adolescent Anxiety Disorders (CAMS). clinicaltrials.gov/ct2/show/NCT00052078 (first received 23 January 2003).
- Piacentini J, Bennett S, Compton SN, Kendall PC, Birmaher B, Albano AM, et al. 24- and 36-week outcomes for the Child/Adolescent Anxiety Multimodal Study (CAMS). Journal of the American Academy of Child and Adolescent Psychiatry 2014;53(3):297-310. [DOI: 10.1016/j.jaac.2013.11.010] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rynn MA, Walkup JT, Compton SN, Sakolsky DJ, Sherrill JT, Shen S, et al. Child/Adolescent Anxiety Multimodal Study: evaluating safety. Journal of the American Academy of Child and Adolescent Psychiatry 2015;54(3):180-90. [DOI: 10.1016/j.jaac.2014.12.015] [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Walkup JT, Albano AM, Piacentini J, Birmaher B, Compton SN, Sherrill JT, et al. Cognitive behavioural therapy, sertraline or a combination in childhood anxiety. New England Journal of Medicine 2008;359(26):2753-66. [DOI: 10.1056/NEJMoa0804633] [DOI] [PMC free article] [PubMed] [Google Scholar]
Waters 2009 {published data only}
- Waters AM, Ford LA, Wharton TA, Cobham VE. Cognitive-behavioural therapy for young children with anxiety disorders: comparison of a child + parent condition versus a parent only condition. Behaviour Research and Therapy 2009;47(8):654-62. [DOI: 10.1016/j.brat.2009.04.008] [DOI] [PubMed] [Google Scholar]
Wergeland 2014 {published and unpublished data}
- NCT00586586. Effectiveness study of CBT for anxiety in children. clinicaltrials.gov/show/nct00586586 (first received 4 January 2008).
- *.Wergeland GJ, Fjermestad KW, Marin CE, Haugland BS, Bjaastad JF, Oeding K, et al. An effectiveness study of individual vs. group cognitive behavioral therapy for anxiety disorders in youth. Behaviour Research and Therapy 2014;57:1‐12. [DOI: 10.1016/j.brat.2014.03.007] [DOI] [PubMed] [Google Scholar]
White 2013 {published data only}
- NCT00926471. Social skills and anxiety reduction treatment for children and adolescents with autism spectrum disorders. clinicaltrials.gov/show/nct00926471 (first received 23 June 2009).
- *.White SW, Ollendick T, Albano AM, Oswald D, Johnson C, Southam-Gerow MA, et al. Randomized controlled trial: Multimodal Anxiety and Social Skill Intervention for adolescents with autism spectrum disorder. Journal of Autism and Developmental Disorders 2013;43(2):382-94. [DOI: 10.1007/s10803-012-1577-x] [DOI] [PMC free article] [PubMed] [Google Scholar]
Wood 2009 {published data only (unpublished sought but not used)}
- Wood JJ, Drahota A, Sze K, Har K, Chiu A, Langer DA. Cognitive behavioral therapy for anxiety in children with autism spectrum disorders: a randomized, controlled trial. Journal of Child Psychology and Psychiatry and Allied Disciplines 2009;50(3):224-34. [DOI: 10.1111/j.1469-7610.2008.01948.x] [DOI] [PMC free article] [PubMed] [Google Scholar]
Wood 2015 {published data only (unpublished sought but not used)}
- NCT01177969. CBT for anxiety disorders in autism: adapting treatment for adolescents. clinicaltrials.gov/ct2/show/nct01177969 (first received 9 August 2010).
- *.Wood JJ, Ehrenreich-May J, Alessandri M, Fujii C, Renno P, Laugeson E, et al. Cognitive behavioral therapy for early adolescents with autism spectrum disorders and clinical anxiety: a randomized, controlled trial. Behavior Therapy 2015;46(1):7-19. [DOI: 10.1016/j.beth.2014.01.002] [DOI] [PMC free article] [PubMed] [Google Scholar]
References to studies excluded from this review
Asbrand {unpublished data only}
- Asbrand J. Exposure-based cognitive behavior therapy for children and adolescents with social anxiety disorder: a randomized controlled group treatment trial. Manuscript provided by author (on 21 May 2019).
Asbrand 2019 {published data only}
- Asbrand J, Heinrichs N, Nitschke K, Wolf OT, Schmidtendorf S, Tuschen-Caffier B. Repeated stress leads to enhanced cortisol stress response in child social anxiety disorder but this effect can be prevented with CBT. Psychoneuroendocrinology 2019;109:104352. [DOI: 10.1016/j.psyneuen.2019.06.003] [DOI] [PubMed] [Google Scholar]
- Asbrand J, Heinrichs N, Schmidtendorf S, Nitschke K, Tuschen-Caffier B. Experience versus report: where are changes seen after exposure-based cognitive-behavioral therapy? A randomized controlled group treatment of childhood social anxiety disorder. Child Psychiatry and Human Development 2020;51(3):427-41. [DOI: 10.1007/s10578-019-00954-w] [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Asbrand J, Schmitz J, Kramer M, Nitschke K, Heinrichs N, Tuschen-Caffier B. Effects of group-based CBT on post-event processing in children with social anxiety disorder following an experimental social stressor. Journal of Abnormal Child Psychology 2019;47(12):1945-56. [DOI: 10.1007/s10802-019-00558-x] [DOI] [PubMed] [Google Scholar]
Baer 2005 {published data only}
- Baer S, Garland EJ. Pilot study of community-based cognitive behavioral group therapy for adolescents with social phobia. Journal of the American Academy of Child and Adolescent Psychiatry 2005;44(3):258-64. [DOI: 10.1097/00004583-200503000-00010] [DOI] [PubMed] [Google Scholar]
Beidel 2000 {published data only}
- Beidel DC, Turner SM, Morris TL. Behavioral treatment of childhood social phobia. Journal of Consulting and Clinical Psychology 2000;68(6):1072-80. [PubMed] [Google Scholar]
- Beidel DC, Turner SM, Young B, Paulson A. Social effectiveness therapy for children: three-year follow-up. Journal of Consulting and Clinical Psychology 2005;73(4):721-5. [DOI] [PubMed] [Google Scholar]
- Beidel DC, Turner SM, Young BJ. Social effectiveness therapy for children: five years later. Behavior Therapy 2006;37(4):416-25. [DOI] [PubMed] [Google Scholar]
Beidel 2007 {published data only}
- *.Beidel DC, Turner SM, Sallee FR, Ammerman RT, Crosby LA, Pathak S. SET-C versus fluoxetine in the treatment of childhood social phobia. Journal of the American Academy of Child and Adolescent Psychiatry 2007;46(12):1622-32. [DOI: 10.1097/chi.0b013e318154bb57] [DOI] [PubMed] [Google Scholar]
- NCT00043537. Treatment of childhood social phobia. clinicaltrials.gov/ct2/show/NCT00043537 (first received 12 August 2002).
Bergman 2013 {published data only}
- Bergman RL, Gonzalez A, Piacentini J, Keller ML. Integrated Behavior Therapy for Selective Mutism: a randomized controlled pilot study. Behaviour Research and Therapy 2013;51(10):680-9. [DOI: 10.1016/j.brat.2013.07.003] [DOI] [PubMed] [Google Scholar]
- NCT00458198. Integrated behavioral therapy for treating children with selective mutism. clinicaltrials.gov/ct2/show/NCT00458198 (first received 9 April 2007).
Bernstein 2005 {published data only (unpublished sought but not used)}
- Bernstein GA, Bernat DH, Victor AM, Layne AE. School-based interventions for anxious children: 3-, 6-, and 12-month follow-ups. Journal of the American Academy of Child and Adolescent Psychiatry 2008;47(9):1039-47. [DOI: 10.1097/CHI.ob013e31817eecco] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bernstein GA, Layne AE, Egan EA, Tennison DM. School-based interventions for anxious children. Journal of the American Academy of Child and Adolescent Psychiatry 2005;44(11):1118-27. [DOI: 10.1097/01.chi.0000177323.40005.a1] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lee SS, Victor AM, James MG, Roach LE, Bernstein GA. School-based interventions for anxious children: long-term follow-up. Child Psychiatry and Human Development 2016;47(2):183-93. [DOI: 10.1007/s10578-015-0555-x] [DOI] [PMC free article] [PubMed] [Google Scholar]
Bodden 2008a {published data only}
- Bodden DH, Bogels SM, Nauta MH, De Haan E, Ringrose J, Appelboom C, et al. Child versus family cognitive-behavioral therapy in clinically anxious youth: an efficacy and partial effectiveness study. Journal of the American Academy of Child and Adolescent Psychiatry 2008;47(12):1384-94. [DOI: 10.1097/CHI.0b013e318189148e] [DOI] [PubMed] [Google Scholar]
- Bodden DHM, Dirksen CD, Bogels SM, Nauta MH, De Haan E, Ringrose J, et al. Costs and cost-effectiveness of family CBT versus individual CBT in clinically anxious children. Clinical Child Psychology and Psychiatry 2008;13(4):543-64. [DOI: 10.1177/1359104508090602] [DOI] [PubMed] [Google Scholar]
Clementi 2019 {published data only}
- Clementi MA. Efficacy of an integrated sleep and anxiety intervention for anxious children: a pilot randomized controlled trial. Dissertation Abstracts International: Section B: The Sciences and Engineering 2019;80:7-B(E). [DOI] [PubMed] [Google Scholar]
Cobham 2012 {published data only}
- Cobham V. Do anxiety-disordered children need to come into the clinic for efficacious treatment? Journal of Consulting and Clinical Psychology 2012;80(3):465-76. [DOI] [PubMed] [Google Scholar]
Cotton 2019 {published data only}
- Cotton S, Kraemer KM, Sears RW, Strawn JR, Wasson RS, McCune N, et al. Mindfulness-based cognitive therapy for children and adolescents with anxiety disorders at-risk for bipolar disorder: a psychoeducation waitlist controlled pilot trial. Early Intervention in Psychiatry 2019;14(2):211-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
Ebrahiminejad 2016 {published data only}
- Ebrahiminejad S, Poursharifi H, Bakhshiour Roodsari A, Zeinodini Z, Noorbakhsh S. The effectiveness of mindfulness-based cognitive therapy on Iranian female adolescents suffering from social anxiety. Iranian Red Crescent Medical Journal 2016;18(11):e25116. [DOI: 10.5812/ircmj.25116] [DOI] [PMC free article] [PubMed] [Google Scholar]
Flatt 2010 {published data only}
- Flatt N, King N. Brief psycho-social interventions in the treatment of specific childhood phobias: a controlled trial and a 1-year follow-up. Behaviour Change 2010;27(3):130-53. [Google Scholar]
Gil Bernal 2009 {published data only}
- Gil-Bernal F, Hernandez-Guzman L. Cognitive-behavioural treatment in Mexican children with social phobia. Anuario de Psicologia 2009;40(1):89-104. [Google Scholar]
Ginsburg 2019b {published data only (unpublished sought but not used)}
Hayward 2000 {published data only}
- Hayward C, Varady S, Albano AM, Thienemann M, Henderson L, Schatzberg AF. Cognitive-behavioral group therapy for social phobia in female adolescents: results of a pilot study. Journal of the American Academy of Child and Adolescent Psychiatry 2000;39(6):721-6. [DOI: 10.1097/00004583-200006000-00010] [DOI] [PubMed] [Google Scholar]
Jansen 2012 {published data only}
- Jansen M, Doorn MM, Lichtwarck-Aschoff A, Kuijpers RC, Theunissen H, Korte M, et al. Effectiveness of a cognitive-behavioral therapy (CBT) manualized program for clinically anxious children: study protocol of a randomized controlled trial. BMC Psychiatry 2012;12(1):16. [DOI: 10.1186/1471-244X-12-16] [DOI] [PMC free article] [PubMed] [Google Scholar]
Kerns 2016 {published data only}
- *.Kerns CM, Wood JJ, Kendall PC, Renno P, Crawford EA, Mercado RJ, et al. The Treatment of Anxiety in Autism Spectrum Disorder (TAASD) study: rationale, design and methods. Journal of Child and Family Studies 2016;25(6):1889-902. [DOI: 10.1007/s10826-016-0372-2] [DOI] [PMC free article] [PubMed] [Google Scholar]
- NCT02028247. Psychotherapy for Anxiety in Children With Autism Spectrum Disorder (TAASD). clinicaltrials.gov/show/NCT02111395 (first received 7 January 2014).
Kujawa 2019 {published data only}
- Kujawa A, Burkhouse KL, Karich SR, Fitzgerald KD, Monk CS, Phan KL. Reduced reward responsiveness predicts change in depressive symptoms in anxious children and adolescents following treatment. Journal of Child and Adolescent Psychopharmacology 2019;29(5):378-85. [DOI] [PMC free article] [PubMed] [Google Scholar]
Lyneham 2006 {published data only}
- Lyneham HJ, Rapee RM. Evaluation of therapist-supported parent-implemented CBT for anxiety disorders in rural children. Behaviour Research and Therapy 2006;44(9):1287-300. [DOI: 10.1016/j.brat.2005.09.009] [DOI] [PubMed] [Google Scholar]
Mendlowitz 1999 {published data only}
- Mendlowitz SL, Manassis K, Bradley S, Scapillato D, Miezitis S, Shaw BF. Cognitive-behavioral group treatments in childhood anxiety disorders: the role of parental involvement. Journal of the American Academy of Child and Adolescent Psychiatry 1999;38(10):1223-9. [DOI] [PubMed] [Google Scholar]
Nauta 2003 {published data only}
- Nauta MH, Scholing A, Emmelkamp PM, Minderaa RB. Cognitive-behavioral therapy for children with anxiety disorders in a clinical setting: no additional effect of a cognitive parent training. Journal of the American Academy of Child and Adolescent Psychiatry 2003;42(11):1270-8. [DOI: 10.1097/01.chi.0000085752.71002.93] [DOI] [PubMed] [Google Scholar]
NCT00576719 {published data only}
- Elkins RM, Gallo KP, Pincus DB, Comer JS. Moderators of intensive cognitive behavioral therapy for adolescent panic disorder: the roles of fear and avoidance. Child and Adolescent Mental Health 2016;21(1):30-6. [DOI: 10.1111/camh.12122] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gallo KP, Chan PT, Buzzella BA, Whitton SW, Pincus DB. The impact of an 8-day intensive treatment for adolescent panic disorder and agoraphobia on comorbid diagnoses. Behavior Therapy 2012;43(1):153-9. [DOI: 10.1016/j.beth.2011.05.002] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gallo KP, Cooper-Vince CE, Hardway CL, Pincus DB, Comer JS. Trajectories of change across outcomes in intensive treatment for adolescent panic disorder and agoraphobia. Journal of Clinical Child and Adolescent Psychology 2014;43(5):742-50. [DOI] [PubMed] [Google Scholar]
- Hardway CL, Pincus DB, Gallo KP, Comer JS. Parental involvement in intensive treatment for adolescent panic disorder and its impact on depression. Journal of Child and Family Studies 2015;24(11):3306-17. [DOI: 10.1007/s10826-015-0133-7] [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.NCT00576719. Effectiveness of intensive cognitive behavioral therapy in treating adolescent panic disorder and agoraphobia. clinicaltrials.gov/show/nct00576719 (first received 19 December 2007).
- Pincus DB, Whitton SW, Gallo KP, Weiner CL, Chow C, Hardway C. Intensive treatment of adolescent panic disorder: results of a randomized controlled trial with short-term maintenance. Citation.
Oerbeck 2014 {published data only}
- Oerbeck B, Overgaard KR, Stein MB, Pripp AH, Kristensen H. Treatment of selective mutism: a 5-year follow-up study. European Child & Adolescent Psychiatry 2018;27(8):997-1009. [DOI: 10.1007/s00787-018-1110-7] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Oerbeck B, Stein MB, Pripp AH, Kristensen H. Selective mutism: follow-up study 1 year after end of treatment. European Child & Adolescent Psychiatry 2015;24(7):757-66. [DOI: 10.1007/s00787-014-0620-1] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Oerbeck B, Stein MB, Wentzel-Larsen T, Langsrud O, Kristensen H. A randomized controlled trial of a home and school-based intervention for selective mutism - defocused communication and behavioural techniques. Child and Adolescent Mental Health 2014;19(3):192-8. [DOI: 10.1111/camh.12045] [DOI] [PubMed] [Google Scholar]
Ollendick 2018 {published data only}
- Ollendick TH, White SW, Richey J, Kim-Spoon J, Ryan SM, Wieckowski AT, et al. Attention bias modification treatment for adolescents with social anxiety disorder. Behavior Therapy 2018;50(1):126-39. [DOI: 10.1016/j.beth.2018.04.002] [DOI] [PMC free article] [PubMed] [Google Scholar]
Ost 2015 {published data only}
- Öst LG, Cederlund R, Reuterskiöld L. Behavioral treatment of social phobia in youth: does parent education training improve the outcome? Behaviour Research and Therapy 2015;67:19-29. [DOI: 10.1016/j.brat.2015.02.001] [DOI] [PubMed] [Google Scholar]
Ozyurt 2018 {published data only}
- Ozyurt G, Gencer O, Ozturk Y, Ozbek A. Is Triple P effective in childhood anxiety disorder? A randomized controlled study. Psychiatry and Clinical Psychopharmacology 2019;29(4):570-8. [DOI: 10.1080/24750573.2018.1483790] [DOI] [Google Scholar]
Pereira 2014 {published data only (unpublished sought but not used)}
- Pereira AI, Marques T, Russo V, Barros L, Barrett P. Effectiveness of the friends for life program in Portuguese schools: study with a sample of highly anxious children. Psychology in the Schools 2014;51(6):647-57. [DOI: 10.1002/pits.21767] [DOI] [Google Scholar]
Rudy 2017 {published data only}
- NCT02051192. A brief behavioral treatment for anxiety in young children. clinicaltrials.gov/ct2/show/NCT02051192 (first received 31 January 2014).
- Rudy BM, Zavrou S, Johnco C, Storch EA, Lewin AB. Parent-led exposure therapy: a pilot study of a brief behavioral treatment for anxiety in young children. Journal of Child and Family Studies 2017;26(9):2475-84. [DOI: 10.1007/s10826-017-0772-y] [DOI] [Google Scholar]
Salzer 2018 {published data only (unpublished sought but not used)}
- Dams J, Kronmüller KT, Leibing E, Steil R, Henningsen P, Leichsenring F, et al. Direct costs of social phobia in adolescents and cost-effectiveness of psychotherapy. Psychiatrische Praxis 2019;46(3):148-55. [DOI: 10.1055/a-0733-4999] [DOI] [PubMed] [Google Scholar]
- ISRCTN22752528. Cognitive therapy (CT-A) versus short-term psychodynamic psychotherapy (STPP-A) for social phobia (SP) in adolescents. www.isrctn.com/ISRCTN22752528 (first received 17 February 2011).
- *.Salzer S, Stefini A, Kronmuller KT, Leibing E, Leichsenring F, Henningsen P, et al. Cognitive-behavioral and psychodynamic therapy in adolescents with social anxiety disorder: a multicenter randomized controlled trial. Psychotherapy and Psychosomatics 2018;87(4):223-33. [DOI: 10.1159/000488990] [DOI] [PubMed] [Google Scholar]
Sevi Tok 2016 {published data only}
- Sevi Tok ES, Arkar H, Bildik T. The effectiveness of cognitive behavioral therapy, medication, or combined treatment for childhood anxiety disorders. Turk Psikiyatri Dergisi [Turkish Journal of Psychiatry] 2016;27(2):1-8. [PubMed] [Google Scholar]
Storch 2019 {published data only}
- NCT01919970. Exposure-focused family-based CBT for youth with ASD and comorbid anxiety. clinicaltrials.gov/ct2/show/NCT01919970 (first received 9 August 2013).
- *.Storch EA, Schneider SC, De Nadai AS, Selles RR, McBride NM, Grebe SC, et al. A pilot study of family-based exposure-focused Treatment for Youth with Autism Spectrum Disorder and Anxiety. Child Psychiatry & Human Development 2019 Sep 6 [Epub ahead of print]. [DOI: 10.1007/s10578-019-00923-3] [DOI] [PubMed]
Sung 2011 {published data only}
- NCT01031511. Effect of cognitive behavioural therapy (CBT) for children with autistic spectrum disorders. clinicaltrials.gov/show/nct01031511 (first received 14 December 2009).
- *.Sung M, Ooi YP, Goh TJ, Pathy P, Fung DS, Ang RP, et al. Effects of cognitive-behavioral therapy on anxiety in children with autism spectrum disorders: a randomized controlled trial. Child Psychiatry and Human Development 2011;42(6):634-49. [DOI: 10.1007/s10578-011-0238-1] [DOI] [PubMed] [Google Scholar]
Weisz 2012 {published data only}
- Chorpita BF, Weisz JR, Daleiden EL, Schoenwald SK, Palinkas LA, Miranda J, et al. Long-term outcomes for the Child STEPs randomized effectiveness trial: a comparison of modular and standard treatment designs with usual care. Journal of Consulting and Clinical Psychology 2013;81(6):999-1009. [DOI: 10.1037/a0034200] [DOI] [PubMed] [Google Scholar]
- NCT01178554. The Clinic Treatment Project (CTP). clinicaltrials.gov/ct2/show/nct01178554 (first received 10 August 2010).
- *.Weisz JR, Chorpita BF, Palinkas LA, Schoenwald SK, Miranda J, Bearman SK, et al. Testing standard and modular designs for psychotherapy treating depression, anxiety, and conduct problems in youth: a randomized effectiveness trial. Archives of General Psychiatry 2012;69(3):274-82. [DOI: 10.1001/archgenpsychiatry.2011.147] [DOI] [PubMed] [Google Scholar]
References to studies awaiting assessment
ACTRN12613000217707 {unpublished data only}
- ACTRN12613000217707. A multi-centre randomised controlled trial of cognitive behavioural therapy for managing anxiety in adolescents with acquired brain injury. www.who.int/trialsearch/Trial2.aspx?TrialID=ACTRN12613000217707 (first received 25 February 2013).
ACTRN12615000730505 {unpublished data only}
- ACTRN12615000730505. Cognitive behaviour therapy for comorbid anxiety and sleep disorders: a randomized controlled trial. www.who.int/trialsearch/Trial2.aspx?TrialID=ACTRN12615000730505 (first received 15 July 2015).
ACTRN12619000619145 {unpublished data only}
- ACTRN12619000619145. SCAN Study - Self Compassion & Cognitive Behavioural Therapy (CBT): Early family intervention for children with Type 1 diabetes experiencing anxiety. www.who.int/trialsearch/Trial2.aspx?TrialID=ACTRN12619000619145 (first received 26 April 2019).
DRKS00012823 {unpublished data only}
- DRKS00012823. Short-term, long-term and cost-effectiveness of treating depression and anxiety disorders in children and adolescents a randomized controlled trial. www.who.int/trialsearch/Trial2.aspx?TrialID=DRKS00012823 (first received 27 September 2017).
IRCT20181006041250N {unpublished data only}
- IRCT20181006041250N1. Effectiveness of coping cat-based cognitive-behavioral therapy (CBT) in group format on treatment of anxiety in children. www.who.int/trialsearch/Trial2.aspx?TrialID=IRCT20181006041250N1 (first received 18 October 2018).
ISRCTN59518816 {unpublished data only}
- ISRCTN59518816. Does the treatment of anxiety in children with ADHD improve outcomes? www.who.int/trialsearch/Trial2.aspx?TrialID=ISRCTN59518816 (first received 29 September 2015).
JPRN‐UMIN000008724 {unpublished data only}
- JPRN-UMIN000008724. Japanese Anxiety Children/Adolescents CBT study. www.who.int/trialsearch/Trial2.aspx?TrialID=JPRN-UMIN000008724 (first received 27 August 2012).
JPRN‐UMIN000032275 {unpublished data only}
- JPRN-UMIN000032275. Transdiagnostic intervention for anxiety and depression in children and adolescents. www.who.int/trialsearch/Trial2.aspx?TrialID=JPRN-UMIN000032275 (first received 19 April 2018).
JPRN‐UMIN000033218 {unpublished data only}
- JPRN-UMIN000033218. The efficacy of group CBT for children with autism spectrum disorder to reduce anxiety symptoms. www.who.int/trialsearch/Trial2.aspx?TrialID=JPRN-UMIN000033218 (first received 1 July 2018).
NCT02810171 {unpublished data only}
- NCT02810171. Dimensional brain behavior predictors of CBT outcomes in pediatric anxiety. clinicaltrials.gov/show/nct02810171 (first received 20 June 2016).
NCT02977962 {unpublished data only}
- NCT02977962. Treatment of anxiety in late adolescents with autism. clinicaltrials.gov/show/nct02977962 (first received 28 November 2016).
NCT03412227 {unpublished data only}
- NCT03412227. Transdiagnostic individual behavioral activation and exposure therapy. clinicaltrials.gov/show/nct03412227 (first received 15 October 2017).
NCT03899948 {unpublished data only}
- NCT03899948. Teacher anxiety program for elementary students. clinicaltrials.gov/show/NCT03899948 (first received 28 March 2019).
References to ongoing studies
ACTRN12616001552471 {published data only}
- ACTRN12616001552471. Effectiveness of school group-based acceptance and commitment therapy for children with anxiety: a randomised controlled trial. www.who.int/trialsearch/Trial2.aspx?TrialID=ACTRN12616001552471 (first received 10 November 2016).
NCT02725619 {published data only}
- NCT02725619. CBT for anxiety in children with autism. clinicaltrials.gov/show/nct02725619 (first received 1 April 2016).
NCT02908321 {published data only}
- Kilburn TR, Sorensen MJ, Thastum M, Rapee RM, Rask CU, Arendt KB, et al. Rationale and design for cognitive behavioral therapy for anxiety disorders in children with autism spectrum disorder: a study protocol of a randomized controlled trial. Trials 2018;19:210. [DOI: 10.1186/s13063-018-2591-x] [DOI] [PMC free article] [PubMed]
- *.NCT02908321. CBT for anxiety disorder in children with co-morbid ASD. clinicaltrials.gov/show/nct02908321 (first received 20 September 2016).
NCT03279471 {published data only}
- NCT03279471. Specifying and treating anxiety in autism research. clinicaltrials.gov/show/nct03279471 (first received 12 September 2017).
NCT03585010 {published data only}
- NCT03585010. Brain response associated with parent-based treatment for childhood anxiety disorders. clinicaltrials.gov/ct2/show/NCT03585010 (first received 12 July 2018).
Additional references
Ale 2015
- Ale CM, McCarthy DM, Rothschild LM, Whiteside SP. Components of cognitive behavioral therapy related to outcome in childhood anxiety disorders. Clinical Child and Family Psychology Review 2015;18(3):240-51. [DOI] [PubMed] [Google Scholar]
Angold 1995
- Angold A, Costello EJ, Messer SC, Pickles A, Winder F, Silver D. The development of a short questionnaire for use in epidemiological studies of depression in children and adolescents. International Journal of Methods in Psychiatric Research 1995;5:237-49. [Google Scholar]
APA 1980
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-III). 3rd edition. Washington, DC: American Psychiatric Association, 1980. [Google Scholar]
APA 1987
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-III-R). 3rd revised edition. Washington, DC: American Psychiatric Association, 1987. [Google Scholar]
APA 1994
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-IV). 4th edition. Washington, DC: American Psychiatric Association, 1994. [Google Scholar]
APA 2000
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-IV-TR). 4th text revision edition. Washington, DC: American Psychiatric Association, 2000. [Google Scholar]
APA 2013
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th edition. Washington, DC: American Psychiatric Association, 2013. [Google Scholar]
Barlow 2010
- Barlow DH. Negative effects from psychological treatments: a perspective. American Psychologist 2010;65(1):13-20. [DOI: 10.1037/a0015643] [DOI] [PubMed] [Google Scholar]
Beck 1996
- Beck A, Steer RA, Brown GK. Beck Depression Inventory Section Edition Manual. San Antonio: The Psychological Corporation, 1996. [Google Scholar]
Beesdo 2009
- Beesdo K, Knappe S, Pine DS. Anxiety and anxiety disorders in children and adolescents: developmental issues and implications for DSM-V. Psychiatric Clinics 2009;32(3):483-524. [DOI] [PMC free article] [PubMed] [Google Scholar]
Beidel 1995
- Beidel DC, Turner SM, Morris TL. A new instrument to assess childhood social anxiety and phobia: the Social Phobia and Anxiety Inventory for Children. Psychological Assessment 1995;10:73-9. [Google Scholar]
Bennett 2016
- Bennett K, Manassis K, Duda S, Bagnell A, Bernstein GA, Garland EJ, et al. Treating child and adolescent anxiety effectively: overview of systematic reviews. Clinical Psychology Review 2016;50:80-94. [DOI] [PubMed] [Google Scholar]
Birmaher 1999
- Birmaher B. Screen for Child Anxiety Related Emotional Disorders (SCARED). Pittsburgh, PA: Western Psychiatric Institute and Clinic, 1999. [Google Scholar]
Bodden 2008b
- Bodden DH, Dirksen CD, Bögels SM. Societal burden of clinically anxious youth referred for treatment: a cost-of-illness study. Journal of Abnormal Child Psychology 2008;36(4):487-97. [DOI] [PMC free article] [PubMed] [Google Scholar]
Bower 2005
- Bower P, Gilbody S. Stepped care in psychological therapies: access, effectiveness and efficiency – narrative literature review. British Journal of Psychiatry 2005;186:11-7. [DOI] [PubMed] [Google Scholar]
Breinholst 2012
- Breinholst S, Esbjorn BH, Reinholdt-Dunne ML, Stallard P. CBT for the treatment of child anxiety disorders: a review of why parental involvement has not enhanced outcomes. Journal of Anxiety Disorders 2012;26(3):416–24. [DOI] [PubMed] [Google Scholar]
Brown 2007
- Brown AM, Deacon BJ, Abramowitz JS, Dammann J, Whiteside SP. Parents' perceptions of pharmacological and cognitive-behavioral treatments for childhood anxiety disorders. Behaviour Research and Therapy 2007;45(4):819-28. [DOI] [PubMed] [Google Scholar]
Cartwright‐Hatton 2004
- Cartwright-Hatton S, Roberts C, Chitsabesan P, Fothergill C, Harrington R. Systematic review of the efficacy of cognitive-behaviour therapies for childhood and adolescent anxiety disorders. British Journal of Clinical Psychology 2004;43:421-36. [DOI] [PubMed] [Google Scholar]
Cartwright‐Hatton 2011
- Cartwright-Hatton S, McNally D, Field AP, Rust S, Laskey B, Dixon C, et al. A new parenting-based group intervention for young anxious children: results of a randomized controlled trial. Journal of the American Academy of Child and Adolescent Psychiatry 2011;50(3):242-51.e6. [DOI] [PubMed] [Google Scholar]
Chatterton 2019
- Chatterton ML, Rapee RM, Catchpool M, Lyneham HJ, Wuthrich V, Hudson JL, et al. Economic evaluation of stepped care for the management of childhood anxiety disorders: results from a randomised trial. Australian and New Zealand Journal of Psychiatry 2019;53:673-82. [DOI] [PubMed] [Google Scholar]
Chorpita 2000
- Chorpita BF, Yim L, Moffitt C, Umemoto LA, Francis SE. Assessment of symptoms of DSM-IV anxiety and depression in children: a revised child anxiety and depression scale. Behaviour Research and Therapy 2000;38(8):835-55. [DOI] [PubMed] [Google Scholar]
Compton 2004
- Compton SN, March JS, Brent D, Albano AM, Weering R, Curry J. Cognitive-behavioral psychotherapy for anxiety and depressive disorders in children and adolescents: an evidence-based medicine review. Journal of the American Academy Child and Adolescent Psychiatry 2004;43:930–59. [DOI] [PubMed] [Google Scholar]
Copeland 2014
- Copeland WE, Angold A, Shanahan L, Costello EJ. Longitudinal patterns of anxiety from childhood to adulthood: the Great Smoky Mountains Study. Journal of the American Academy of Child and Adolescent Psychiatry 2014;53(1):21-33. [DOI] [PMC free article] [PubMed] [Google Scholar]
Covidence [Computer program]
- Covidence. Version Accessed 3 December 2018. Melbourne, Australia: Veritas Health Innovation. Available at covidence.org.
Creswell 2020a
- Creswell C, Nauta M, Hudson J, March S, Reardon T, Arendt K, et al. Recommendations for reporting on treatment trials for child and adolescent anxiety disorders: an international consensus statement. Journal of Child Psychology and Psychiatry 2020 Jul 19 [Epub ahead of print]. [DOI: 10.1111/jcpp.13283] [DOI] [PubMed]
Creswell 2020b
- Creswell C, Waite P, Hudson J. Practitioner Review: Anxiety disorders in children and young people – assessment and treatment. Journal of Child Psychology and Psychiatry 2020;61(6):628-43. [DOI: 10.1111/jcpp.13186] [DOI] [PubMed] [Google Scholar]
Crowe 2017
- Crowe K, McKay D. Efficacy of cognitive-behavioral therapy for childhood anxiety and depression. Journal of Anxiety Disorders 2017;49:76-87. [DOI] [PubMed] [Google Scholar]
Deeks 2017
- Deeks JJ, Higgins JP, Altman DG, editor(s) on behalf of the Cochrane Statistical Methods Group. Chapter 9: Analysing data and undertaking meta-analyses. In: Higgins JPT, Churchill R, Chandler J, Cumpston MS, editor(s). Cochrane Handbook for Systematic Reviews of Interventions version 5.2.0 (updated June 2017). Cochrane, 2017. Available from www.training.cochrane.org/handbook.
Duggan 2014
- Duggan C, Parry G, McMurran M, Davidson K, Dennis J. The recording of adverse events from psychological treatments in clinical trials: evidence from a review of NIHR-funded trials. Trials 2014;15:335. [DOI] [PMC free article] [PubMed] [Google Scholar]
Essau 2003
- Essau CA. Comorbidity of anxiety disorders in adolescents. Depression and Anxiety 2003;18(1):1-6. [DOI: 10.1002/da.10107] [DOI] [PubMed] [Google Scholar]
Essau 2004
- Essau CA, Conradt J, Ederer EM. Anxiety prevention among school children. Versicherungsmedizin 2004;56:123-30. [PubMed] [Google Scholar]
Essau 2014
- Essau CA, Lewinsohn PM, Olaya B, Seeley JR. Anxiety disorders in adolescents and psychosocial outcomes at age 30. Journal of Affective Disorders 2014;163:125-32. [DOI] [PMC free article] [PubMed] [Google Scholar]
Evans 2017
- Evans R, Thirlwall K, Cooper P, Creswell C. Using symptom and interference questionnaires to identify recovery among children with anxiety disorders. Psychological Assessment 2017;29(7):835-43. [DOI] [PMC free article] [PubMed] [Google Scholar]
Fineberg 2013
- Fineberg NA, Haddad PM, Carpenter L, Gannon B, Sharpe R, Young AH, et al. The size, burden and cost of disorders of the brain in the UK. Journal of Psychopharmacology (Oxford, England) 2013;27(9):761-70. [DOI] [PMC free article] [PubMed] [Google Scholar]
Galla 2012
- Galla BM, Wood JJ, Chiu AW, Langer DA, Jacobs J, Ifekwunigwe M, et al. One year follow-up to modular cognitive behavioral therapy for the treatment of pediatric anxiety disorders in an elementary school setting. Child Psychiatry and Human Development 2012;43(2):219-26. [DOI] [PubMed] [Google Scholar]
Gillies 2016
- Gillies D, Maiocchi L, Bhandari AP, Taylor F, Gray C, O'Brien L. Psychological therapies for children and adolescents exposed to trauma. Cochrane Database of Systematic Reviews 2016, Issue 10. Art. No: CD012371. [DOI: 10.1002/14651858.CD012371] [DOI] [PMC free article] [PubMed] [Google Scholar]
Ginsburg 2018
- Ginsburg GS, Becker-Haimes EM, Keeton C, Kendall PC, Lyengar S, Sakolsky D, et al. Results from the Child/Adolescent Anxiety Multimodal Extended Long-Term Study (CAMELS): primary anxiety outcomes. Journal of the American Academy of Child and Adolescent Psychiatry 2018;57(7):471-80. [DOI: 10.1016/j.jaac.2018.03.017] [DOI] [PubMed] [Google Scholar]
GRADEpro GDT [Computer program]
- GRADEpro GDT. Version (accessed 4 October 2018). Hamilton (ON): McMaster University (developed by Evidence Prime). Available at gradepro.org.
Green 2004
- Green H, McGinnity A, Meltzer H, Ford T, Goodman R. Mental health of children and young people in Great Britain, 2004. no-pa.uk/wp-content/uploads/2015/02/Mental-health-of-children.pdf (accessed 4 October 2018).
Health Services Research Unit 2004
- Health Services Research Unit. Database of ICCs: spreadsheet (empirical estimates of ICCs from changing professional practice studies). https://www.abdn.ac.uk/hsru/what-we-do/tools/index.php (accessed 1 September 2020).
Higgins 2003
- Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ 2003;327:557-60. [DOI] [PMC free article] [PubMed] [Google Scholar]
Higgins 2011
- Higgins JP, Deeks JJ, Altman DG, editor(s). Chapter 16: Special topics in statistics. In: Higgins JPT, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Higgins 2017
- Higgins JP, Altman DG, Sterne JA, editor(s). Chapter 8: Assessing risk of bias in included studies. In: Higgins JPT, Churchill R, Chandler J, Cumpston MS, editor(s). Cochrane Handbook for Systematic Reviews of Interventions version 5.2.0 (updated June 2017). Cochrane, 2017. Available from www.training.cochrane.org/handbook.
Hirshfeld‐Becker 2010
- Hirshfeld-Becker DR, Masek B, Henin A, Blakely LR, Pollock-Wurman RA, McQuade J, et al. Cognitive behavioral therapy for 4- to 7-year-old children with anxiety disorders: a randomized clinical trial. Journal of Consulting and Clinical Psychology 2010;78(4):498-510. [DOI] [PubMed] [Google Scholar]
Holland 1995
- Holland D, Dadds M. Diagnostic Interview Schedule for Children, Adolescents and Parents. Brisbane: Griffith University, 1995. [Google Scholar]
Keeton 2013
- Keeton CP, Ginsburg GS, Drake KL, Sakolsky D, Kendall PC, Birmaher B, et al. Benefits of child-focused anxiety treatments for parents and family functioning. Depression and Anxiety 2013;30(9):865-72. [DOI] [PMC free article] [PubMed] [Google Scholar]
Kendall 1993
- Kendall PC. Cognitive-behavioral therapies with youth: guiding theory, current status, and emerging developments. Journal of Consulting and Clinical Psychology 1993;61(2):235-47. [DOI] [PubMed] [Google Scholar]
Kendall 2006
- Kendall PC, Hedtke KA. Cognitive-Behavioral Therapy for Anxious Children: Therapist Manual. 1st edition. Ardmore, PA: Workbook Publishing, 2006. [Google Scholar]
Kendall 2016
- Kendall PC, Cummings CM, Villabo MA, Narayanan MK, Treadwell K, Birmaher B, et al. Mediators of change in the Child/Adolescent Anxiety Multimodal Treatment Study. Journal of Consulting and Clinical Psychology 2016;84(1):1-14. [DOI] [PMC free article] [PubMed] [Google Scholar]
Kovacs 1989
- Kovacs M, Gatsonis C, Paulauskas S, Richards C. Depressive disorders in childhood. IV. A longitudinal study of comorbidity with and the risk for anxiety disorders. Archives of General Psychiatry 1989;46:776-82. [DOI] [PubMed] [Google Scholar]
Kreuze 2018
- Kreuze LJ, Pijnenborg GHM, Jonge YB, Nauta MH. Cognitive-behavior therapy for children and adolescents with anxiety disorders: a meta-analysis of secondary outcomes. Journal of Anxiety Disorders 2018;60:43-57. [DOI] [PubMed] [Google Scholar]
La Greca 1998
- La Greca A. Manual for Social Anxiety Scales for Children and Adolescents. Coral Gables, FL: University of Miami, 1998. [Google Scholar]
Lawrence 2015
- Lawrence D, Johnson S, Hafekost J, Haan KB, Sawyer M, Ainley J, et al. The Mental Health of Children and Adolescents. Report on the Second Australian Child and Adolescent Survey of Mental Health and Wellbeing. www1.health.gov.au/internet/main/publishing.nsf/Content/9DA8CA21306FE6EDCA257E2700016945/$File/child2.pdf (accessed 4 October 2020).
Leyfer 2013
- Leyfer O, Gallo K, Cooper-Vince C, Pincus DB. Patterns and predictors of comorbidity of DSM-IV anxiety disorders in a clinical sample of children and adolescents. Journal of Anxiety Disorders 2013;27(3):306-11. [DOI] [PubMed] [Google Scholar]
March 1997
- March JS, Parker JD, Sullivan K, Stallings P, Conners CK. The Multidimensional Anxiety Scale for Children (MASC): factor structure, reliability, and validity. Journal of the American Academy of Child and Adolescent Psychiatry 1997;36(4):554-65. [DOI] [PubMed] [Google Scholar]
Masia‐Warner 2005
- Masia-Warner C, Klein RG, Dent HC, Fisher PH, Alvir J, Albano AM, et al. School-based intervention for adolescents with social anxiety disorder: results of a controlled study. Journal of Abnormal Child Psychology 2005;33(6):707-22. [DOI] [PubMed] [Google Scholar]
Mavranezouli 2015
- Mavranezouli I, Mayo-Wilson E, Dias S, Kew K, Clark DM, Ades AE, et al. The cost effectiveness of psychological and pharmacological interventions for social anxiety disorder: a model-based economic analysis. PLOS ONE 2015;10(10):e0140704. [DOI: 10.1371/journal.pone.0140704] [DOI] [PMC free article] [PubMed] [Google Scholar]
Merikangas 2011
- Merikangas KR, He JP, Burstein M, Swendsen J, Avenevoli S, Case B, et al. Service utilization for lifetime mental disorders in U.S. adolescents: results of the National Comorbidity Survey-Adolescent Supplement (NCS-A). Journal of the American Academy of Child and Adolescent Psychiatry 2011;50(1):32-45. [DOI] [PMC free article] [PubMed] [Google Scholar]
Moher 2015
- Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, et al, PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Systematic Review 2015;4:1. [DOI: 10.1186/2046-4053-4-1] [DOI] [PMC free article] [PubMed] [Google Scholar]
Monga 2015
- Monga S, Rosenbloom BN, Tanha A, Owens M, Young A. Comparison of child-parent and parent-only cognitive-behavioral therapy programs for anxious children aged 5 to 7 years: short- and long-term outcomes. Journal of the American Academy of Child and Adolescent Psychiatry 2015;54(2):138-46. [DOI] [PubMed] [Google Scholar]
Myers 2002
- Myers K, Winters NC. Ten year review of rating scales II: scales for internalising disorders. Journal of the American Academy of Child and Adolescent Psychiatry 2002;41:634-59. [DOI] [PubMed] [Google Scholar]
NICE 2013
- National Institute for Health and Care Excellence. Social anxiety disorder: recognition, assessment and treatment: Clinical guideline [CG159]. www.nice.org.uk/guidance/cg159 (accessed 4 October 2020).
O'Kearney 2006
- O'Kearney RT, Anstey KJ, Sanden C. Behavioural and cognitive behavioural therapy for obsessive compulsive disorder in children and adolescents. Cochrane Database of Systematic Reviews 2006, Issue 4. Art. No: CD004856. [DOI: 10.1002/14651858.CD004856.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Ollendick 2010
- Ollendick TH, Öst LG, Reuterskiöld L, Costa N. Comorbidity in youth with specific phobias: impact of comorbidity on treatment outcome and the impact of treatment on comorbid disorders. Behaviour Research and Therapy 2010;48(9):827-31. [DOI] [PMC free article] [PubMed] [Google Scholar]
Pennant 2015
- Pennant ME, Loucas CE, Whittington C, Creswell C, Fonagy P, Fuggle P, et al. Computerised therapies for anxiety and depression in children and young people: a systematic review and meta-analysis. Behaviour Research and Therapy 2015;67:1-18. [DOI] [PubMed] [Google Scholar]
Perihan 2019
- Perihan C, Burke M, Bowman-Perrott L, Bicer A, Gallup J, Thompson J, et al. Effects of cognitive behavioral therapy for reducing anxiety in children with high functioning ASD: a systematic review and meta-analysis. Journal of Autism and Developmental Disorders 2019;27:1-5. [DOI: 10.1007/s10803-019-03949-7] [DOI] [PubMed] [Google Scholar]
Peris 2015
- Peris TS, Compton SN, Kendall PC, Birmaher B, Sherrill J, March J, et al. Trajectories of change in youth anxiety during cognitive-behavior therapy. Journal of Consulting and Clinical Psychology 2015;83(2):239-52. [DOI] [PMC free article] [PubMed] [Google Scholar]
Peris 2017
- Peris TS, Caporino NE, O'Rourke S, Kendall PC, Walkup JT, Albano AM, et al. Therapist-reported features of exposure tasks that predict differential treatment outcomes for youth with anxiety. Journal of the American Academy of Child and Adolescent Psychiatry 2017;56(12):1043-52. [DOI] [PMC free article] [PubMed] [Google Scholar]
Peters 2008
- Peters JL, Sutton AJ, Jones DR, Abrams KR, Rushton L. Contour-enhanced meta-analysis funnel plots help distinguish publication bias from other causes of asymmetry. Journal of Clinical Epidemiology 2008;61(10):991-6. [DOI] [PubMed] [Google Scholar]
Pine 2009
- Pine DS, Helfinstein SM, Bar-Haim Y, Nelson E, Fox NA. Challenges in developing novel treatments for childhood disorders: lessons from research on anxiety. Neuropsychopharmacology 2009;34(1):213-28. [DOI] [PMC free article] [PubMed] [Google Scholar]
Polanczyk 2015
- Polanczyk GV, Salum GA, Sugaya LS, Caye A, Rohde LA. Annual research review: a meta-analysis of the worldwide prevalence of mental disorders in children and adolescents. Journal of Child Psychology and Psychiatry and Allied Disciplines 2015;56(3):345-65. [DOI] [PubMed] [Google Scholar]
Rao 1992
- Rao JN, Scott AJ. A simple method for the analysis of clustered binary data. Biometrics 1992;48(2):577-85. [PubMed] [Google Scholar]
Reardon 2017
- Reardon T, Harvey K, Baranowska M, O'Brien D, Smith L, Creswell C. What do parents perceive are the barriers and facilitators to accessing psychological treatment for mental health problems in children and adolescents? A systematic review of qualitative and quantitative studies. European Child & Adolescent Psychiatry 2017;26(6):623-47. [DOI] [PMC free article] [PubMed] [Google Scholar]
Reardon 2020
- Reardon T, Harvey K, Creswell C. Seeking and accessing professional support for child anxiety in a community sample. European Child and Adolescent Psychiatry 2020;29:649-64. [DOI: 10.1007/s00787-019-01388-4] [DOI] [PMC free article] [PubMed] [Google Scholar]
Review Manager 2014 [Computer program]
- Review Manager 5 (RevMan 5). Version 5.3. Copenhagen: Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Reynolds 1985
- Reynolds CR, Richmond BO. Revised Children's Manifest Anxiety Scale (RCAMS) Manual. Los Angeles: Western Psychological Services, 1985. [Google Scholar]
Reynolds 2012
- Reynolds S, Wilson C, Austin J, Hooper L. Effects of psychotherapy for anxiety in children and adolescents: a meta-analytic review. Clinical Psychology Review 2012;32(4):251-62. [DOI] [PubMed] [Google Scholar]
Sanchez‐Garcia 2009
- Sanchez-Garcia R, Olivares J. Effectiveness of a program for early detection/intervention in children/adolescents with generalized social phobia. Anales de Psicologia 2009;25:241-9. [Google Scholar]
Schünemann 2017
- Schünemann HJ, Oxman AD, Vist GE, Higgins JP, Deeks JJ, Glasziou P, et al, on behalf of the Cochrane Applicability and Recommendations Methods Group. Chapter 12: Interpreting results and drawing conclusions. In: Higgins JPT, Churchill R, Chandler J, Cumpston MS, editor(s). Cochrane Handbook for Systematic Reviews of Interventions version 5.2.0 (updated June 2017). Cochrane, 2017. Available from www.training.cochrane.org/handbook.
Seligman 2011
- Seligman L, Ollendick T. Cognitive behavioral therapy for anxiety disorders in youth. Child & Adolescent Psychiatric Clinics of North America 2011;20(2):217-38. [DOI] [PMC free article] [PubMed] [Google Scholar]
Shaffer 1983
- Shaffer D, Gould MS, Brasic J, Ambrosini P, Fisher P, Bird H, et al. A children's global assessment scale (CGAS). Archives of General Psychiatry 1983;40(11):1228-31. [DOI] [PubMed] [Google Scholar]
Silverman 1987
- Silverman WK. Anxiety Disorder Interview for Children (ADIC). New York, NY: Graywind Publications, 1987. [Google Scholar]
Silverman 2008
- Silverman WK, Pina AA, Viswesvaran C. Evidence-based psychosocial treatments for phobic and anxiety disorders in children and adolescents. Journal of Clinical Child and Adolescent Psychology 2008;37:105-30. [DOI] [PubMed] [Google Scholar]
Silverman 2009
- Silverman WK, Kurtines WM, Jaccard J, Pina AA. Directionality of change in youth anxiety treatment involving parents: an initial examination. Journal of Consulting and Clinical Psychology 2009;77:474-85. [DOI] [PMC free article] [PubMed] [Google Scholar]
Southam‐Gerow 2010
- Southam-Gerow MA, Weisz JR, Chu BC, McLeod BD, Gordis EB, Connor-Smith JK. Does cognitive behavioral therapy for youth anxiety outperform usual care in community clinics? An initial effectiveness test. Journal of the American Academy of Child and Adolescent Psychiatry 2010;49(10):1043-52. [DOI] [PMC free article] [PubMed] [Google Scholar]
Spence 1997
- Spence S. Stucture of anxiety symptoms amongst children: a confirmatory factor-analytic study. Journal of Abnormal Psychology 1997;106:280-97. [DOI] [PubMed] [Google Scholar]
Spielberger 1973
- Spielberger C, Edwards C, Montuori J, Lushene R. State-Trait Anxiety Inventory for Children. Palto Alto, CA: Consulting Psychologist Press, 1973. [Google Scholar]
Stata 2012 [Computer program]
- Stata. Version Stata/IC 12.1. College Station, TX: StataCorp, 2012. Available at www.stata.com.
Sterne 2017
- Sterne JA, Egger M, Moher D, Boutron I, editor(s). Chapter 10: Addressing reporting biases. In: Higgins JPT, Churchill R, Chandler J, Cumpston MS, editor(s). Cochrane Handbook for Systematic Reviews of Interventions version 5.2.0 (updated June 2017). Cochrane, 2017. Available from www.training.cochrane.org/handbook.
Suveg 2006
- Suveg C, Kendall PC, Comer JS, Robin J. Emotion-focused cognitive-behavioral therapy for anxious youth: a multiple-baseline evaluation. Journal of Contemporary Psychotherapy 2006;36(2):77-85. [Google Scholar]
Ung 2015
- Ung D, Selles R, Small BJ, Storch EA. A systematic review and meta-analysis of cognitive-behavioral therapy for anxiety in youth with high-functioning autism spectrum disorders. Child Psychiatry and Human Development 2015;46(4):533-47. [DOI] [PubMed] [Google Scholar]
van Steensel 2013
- Steensel F, Bogels S, Perrin S. Anxiety disorders in children and adolescents with autistic spectrum disorders: a meta-analysis. Clinical Child and Family Psychology Review 2011;14:302-17. [DOI] [PMC free article] [PubMed] [Google Scholar]
Waite 2014
- Waite P, Creswell C. Children and adolescents referred for treatment of anxiety disorders: differences in clinical characteristics. Journal of Affective Disorders 2014;167:326-32. [DOI] [PMC free article] [PubMed] [Google Scholar]
Waite 2015
- Waite P, Codd J, Creswell C. Interpretation of ambiguity: differences between children and adolescents with and without an anxiety disorder. Journal of Affective Disorders 2015;188:194-201. [DOI] [PMC free article] [PubMed] [Google Scholar]
Wang 2005
- Wang PS, Berglund P, Olfson M, Pincus HA, Wells KB, Kessler RC. Failure and delay in initial treatment contact after first onset of mental disorders in the National Comorbidity Survey Replication. Archives of General Psychiatry 2005;62(6):603-13. [DOI] [PubMed] [Google Scholar]
Wang 2017
- Wang Z, Whiteside S, Sim L, Farah W, Morrow AS, Alsawas M, et al. Comparative effectiveness and safety of cognitive behavioral therapy and pharmacotherapy for childhood anxiety disorders: a systematic review and meta-analysis. JAMA Pediatrics 2017;171(11):1049-56. [DOI: 10.1001/jamapediatrics.2017.3036] [DOI] [PMC free article] [PubMed] [Google Scholar]
Warner 2011
- Warner CM, Colognori D, Kim RE, Reigada LC, Klein RG, Browner-Elhanan KJ, et al. Cognitive-behavioral treatment of persistent functional somatic complaints and pediatric anxiety: an initial controlled trial. Depression and Anxiety 2011;28(7):551-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
Warwick 2016
- Warwick H, Reardon T, Cooper P, Murayama K, Reynolds S, Wilson C, et al. Complete recovery from anxiety disorders following cognitive behavior therapy in children and adolescents: a meta-analysis. Clinical Psychology Review 2016;52:77-91. [DOI] [PubMed] [Google Scholar]
Whiteside 2015
- Whiteside SP, Ale CM, Young B, Dammann JE, Tiede MS, Biggs BK. The feasibility of improving CBT for childhood anxiety disorders through a dismantling study. Behaviour Research and Therapy 2015;73:83-9. [DOI] [PubMed] [Google Scholar]
WHO 1978
- World Health Organization. The ICD-9 Classification of Mental and Behavioural Disorders: Clinical Description and Diagnostic Guidelines. Geneva: World Health Organization, 1978. [Google Scholar]
WHO 1992
- World Health Organization. The ICD-10 Classification of Mental and Behavioural Disorders: Clinical Description and Diagnostic Guidelines. Geneva: World Health Organization, 1992. [Google Scholar]
Young 2006
- Young BJ, Beidel DC, Turner SM, Ammerman RT, McGraw K, Coaston SC. Pretreatment attrition and childhood social phobia: parental concerns about medication. Journal of Anxiety Disorders 2006;20(8):1133-47. [DOI] [PubMed] [Google Scholar]
Zhou 2019
- Zhou X, Zhang Y, Furukawa TA, Cuijpers P, Pu J, Weisz JR, et al. Different types and acceptability of psychotherapies for acute anxiety disorders in children and adolescents: a network meta-analysis. JAMA Psychiatry 2019;76(1):41-50. [DOI: 10.1001/jamapsychiatry.2018.3070] [DOI] [PMC free article] [PubMed] [Google Scholar]
References to other published versions of this review
James 2005
- James AA, Soler A, Weatherall RR. Cognitive behavioural therapy for anxiety disorders in children and adolescents. Cochrane Database of Systematic Reviews 2005, Issue 4. Art. No: CD004690. [DOI: 10.1002/14651858.CD004690] [DOI] [PubMed] [Google Scholar]
James 2015
- James AC, James G, Cowdrey FA, Soler A, Choke A. Cognitive behavioural therapy for anxiety disorders in children and adolescents. Cochrane Database of Systematic Reviews 2015, Issue 2. Art. No: CD004690. [DOI: 10.1002/14651858.CD004690.pub4] [DOI] [PMC free article] [PubMed] [Google Scholar]
James 2018
- James AC, Reardon T, Soler A, James G, Creswell C. Cognitive behavioural therapy for anxiety disorders in children and adolescents. Cochrane Database of Systematic Reviews 2018, Issue 10. Art. No: CD013162. [DOI: 10.1002/14651858.CD013162] [DOI] [PMC free article] [PubMed] [Google Scholar]